
Abstract
Aims:
This study examined associations between mothers’ depressive symptoms and the Turkish heritage vocabulary of their school-age children. We expected that mothers’ depressive symptoms would be associated with lower Turkish vocabulary scores in fourth grade as well as slower growth in vocabulary scores from fourth to sixth grade.
Design:
We collected longitudinal data on 139 mothers of Turkish origin in Germany and their children in fourth, fifth, and sixth grade. Mothers reported on the level of their depressive symptoms, and children were administered a Turkish receptive vocabulary test.
Analysis:
Data were analyzed with growth curve modeling.
Findings and conclusions:
Mothers’ depressive symptoms were not significantly associated with children’s vocabulary in fourth grade. However, mothers’ depressive symptoms did predict slower growth in children’s vocabulary from fourth to sixth grade. The higher a mother’s depressive symptoms score, the slower the growth of her child’s Turkish vocabulary.
Originality:
To our knowledge, this is the first study to examine the association between mothers’ depressive symptoms and their children’s vocabulary development during the school-age years, and the second to examine it for heritage language development.
Significance and implications:
Our findings suggest that mothers’ depressive symptoms may be one risk factor limiting parents in successfully passing on the heritage language to their children, even during school-age. Families as well as medical, psychological, and educational professionals should be made aware of the role of mothers’ depressive symptoms in their children’s language development.
Keywords
Europe’s demographic is undergoing remarkable changes. Many immigrants and refugees are struggling to reach Europe, with the largest proportion of over a million in 2015 heading to Germany (Bundesamt für Migration und Flüchtlinge, 2016). Not only are young men making the arduous and dangerous trek to escape war and persecution, but the number of women and children among immigrants is also rising (Karas, 2016). Once existential needs have been attended to, many families from Syria or Afghanistan will face the challenge of passing on their family language in an environment where they may be their children’s main teacher of that language. Such is the case for families of Turkish origin, Europe’s largest immigrant group with over 2.5 million people of Turkish origin in Germany alone (Crul & Vermeulen, 2003; Statistisches Bundesamt, 2015). Currently, over 8% of fifth graders in Germany have Turkish roots (Olczyk, Seuring, Will, & Zinn, 2016). Thus, more than 1 out of every 12 school-age children in Germany is from a family in which the Turkish language may be used by parents or grandparents. That makes Turkish an important heritage language in Germany and Europe, learned mainly at home from the family.
Drawing on research mostly from North America, there is evidence that maintaining a heritage language may benefit bilingual children in their socio-emotional and cognitive development, their majority language development, and their family relationships (Adesope, Lavin, Thompson, & Ungerleider, 2010; Davison, Hammer, & Lawrence, 2011; Fillmore, 2000; Halle et al., 2014). Furthermore, many Turkish parents are first-generation immigrants, which means that children may need Turkish language skills in order to effectively communicate with their parents. Thus, there is reason to expect that children of Turkish descent may benefit from maintaining the Turkish language. However, in German public schools, the language of instruction is almost exclusively German (Neumann, 2008). Thus, the family is the primary source of Turkish language learning.
Families of Turkish origin in Germany are subject to several adversities which may hamper parents’ success in passing on the heritage language. On average, people of Turkish origin have lower levels of education and higher unemployment rates than non-immigrants, and a full 40% of children of Turkish origin live in families that are at risk of poverty (Autorengruppe Bildungsberichterstattung, 2012; Statistisches Bundesamt, 2015). This financial strain and other experiences related to immigration, such as the loss of support systems, the stress of acculturating into a new society, and discrimination may be risk factors for depression (Bhugra, 2004). There is evidence that mothers’ depression may be connected to language development through the way mothers and children interact and relate to each other (Lovejoy, Graczyk, O’Hare, & Neuman, 2000; Sohr-Preston & Scaramella, 2006). This link may be especially evident when the family is also suffering from economic difficulties (Gelfand & Teti, 1990; Goodman et al., 2011). As of now, most of the knowledge on the relationship between maternal depression and language development is derived from studies on young monolingual children. Possible effects on bilingual children’s heritage language development have been largely neglected. Consequently, we investigate how mothers’ depressive symptoms are related to language development in a low-income population, Turkish immigrant families in Germany. Specifically, we are interested in whether mothers’ depression is connected to growth in their school-age children’s receptive Turkish heritage language vocabulary. We focus on vocabulary as a language domain that is sensitive to environmental effects (Hoff, 2006).
Maternal depression and children’s language outcomes
There is an impressive body of evidence illustrating the implications of mothers’ depressive symptoms for their children. Children of mothers who are depressed or have depressive symptoms have higher rates of unfavorable cognitive, behavioral, and emotional outcomes (Downey & Coyne, 1990; Goodman et al., 2011; Hay et al., 2001; Petterson & Albers, 2001). A smaller number of studies has investigated whether mothers’ depression is specifically connected to young children’s language development. Though there is some mixed evidence (Baydar et al., 2014; Horwitz et al., 2003), several studies show that young children of depressed mothers score lower on receptive and expressive language tests than children of non-depressed mothers (Brennan et al., 2000; Kaplan et al., 2014; NICHD ECCRN, 1999; Stein, Malmberg, Sylva, Barnes, & Leach, 2008). Many of these studies connecting mothers’ depressive symptoms and children’s language development use vocabulary measures as an outcome, as it is an important predictor of reading skills and academic achievement (Prevoo, Malda, Mesman, & van IJzendoorn, 2016). For example, the maximum number of depressive symptoms mothers reported over several years was negatively connected to their five-year-olds’ receptive vocabulary test scores (Brennan et al., 2000). There is also evidence that maternal depression is associated with slower growth in children’s vocabulary. For example, in a study of low-income families, toddlers whose mothers reported a great number of depressive symptoms displayed slower growth in vocabulary production from 1 to 3 years (Pan, Rowe, Singer, & Snow, 2005).
There are several pathways through which mothers’ depression may affect children’s language development. Specifically, depressed mothers tend to interact less with their children; they are more disengaged, inattentive, and less responsive than mothers who are not depressed (Albright & Tamis-LeMonda, 2002; Gelfand & Teti, 1990; Lovejoy et al., 2000; Sohr-Preston & Scaramella, 2006). When they interact with their children, depressed mothers are likely to be more negative and intrusive and less warm and sensitive than non-depressed mothers (Lovejoy et al., 2000; Murray, Fiori-Cowley, Hooper, & Cooper, 1996; NICHD ECCRN, 1999; Sohr-Preston & Scaramella, 2006; Stein et al., 2008). Mothers who are depressed also provide a reduced quantity of verbal input compared with that of well mothers. On average, depressed mothers talk less to their children, respond to them more slowly, ask fewer questions, and read them books less often (Bettes, 1988; Breznitz & Sherman, 1987; Cox, Puckering, Pound, & Mills, 1987; Rowe, Pan, & Ayoub, 2005; Sohr-Preston & Scaramella, 2006). In conclusion, mothers who are depressed may be hampered in providing frequent positive interactions and rich verbal input that promote the language development of their children.
Maternal depression and school-age children
The research connecting mothers’ depression and children’s language skills has almost exclusively focused on young children under the age of six (Brennan et al., 2000; Cox et al., 1987; Kaplan et al., 2014; Murray, 1992; Murray et al., 1996; NICHD ECCRN, 1999; Stein et al., 2008). This raises the questions as to whether maternal depression is connected to language development beyond early childhood.
Two hypotheses are possible. On one hand, the connections between mothers’ depression and the language development of children younger than six may apply similarly to school-age children in that their input is not sufficient and the effects of this accumulate over time. If mothers provide compromised quantity and quality of verbal input and interactions, school-age children have fewer opportunities for building their vocabularies. Furthermore, the effects of less than optimal interactions with a depressed mother may accumulate over time if the symptoms are persistent, thereby slowing older children’s language development. There is some evidence that is concurrent with the idea that depression may affect children’s language development into school-age. First, the effect of mothers’ depressive symptoms on toddlers’ vocabulary found by Pan et al. (2005) increased with the toddlers’ age, meaning that the vocabulary of children of mothers with many and few depressive symptoms differed more over time. Second, drawing on literacy research, there are studies that show effects of depression during school-age. For example, parents’ depression in kindergarten predicted children’s fifth grade reading scores (Bodovski & Youn, 2010). In another study, more persistent maternal depressive symptoms were associated with larger effects on third and fifth grade reading (Claessens, Engel, & Curran, 2015).
On the other hand, it could be hypothesized that mothers’ depression will not affect the vocabulary of school-aged children. One possible reason for this is that school-age children can expand their language skills through their own reading (Nippold, 2006). Another is that for school-age children other adults, peers, and siblings may become more important in shaping their language environment. Older children of depressed mothers may receive much needed opportunities for interactions and verbal exchanges from their social network. Therefore, at least for monolingual children, the effects of maternal depressive symptoms could decrease with age as older children simply spend a large portion of their day with other people, such as peers and teachers. However, for heritage language learners, this would only be the case if the members of the child’s social network actually spoke the heritage language. If there are few heritage speakers in the child’s network, the child may be exposed to very little heritage language input beyond their mothers. Furthermore, the only empirical evidence supporting the idea that mothers’ depression may be less consequential for older children comes from research on non-language outcomes: The association between mothers’ depression and children’s psychological problems is weaker for older than for younger children (Goodman et al., 2011).
Maternal depression and immigrant children learning the heritage language
An estimated two-thirds of the world population is bilingual (Baker & Jones, 1998). Yet, there is a dearth of research studying the connection between mothers’ depression and children’s heritage language in bilingual populations. There are two studies in which bilingual children were included in the larger, mainly monolingual sample. These bilingual children were assessed in their second language, English, but not in their respective heritage languages. Furthermore, no separate analyses were computed for the bilingual subsamples. Instead, bilingual versus monolingual status was only included as a covariate when modeling the connection between mothers’ depression and children’s language outcomes (Horwitz et al., 2003; Stein et al., 2008).
In one study by Cycyk, Bitetti, and Hammer (2015), the focus was specifically on bilingual children, and how mothers’ depressive symptoms are connected to both heritage and majority language skills. This study found that for bilingual Latino children from low-income families, mothers’ depressive symptoms were associated with slower growth of Spanish heritage language vocabulary over 2 years. Interestingly, mothers’ depressive symptoms were not related to English language vocabulary. This finding suggests that mothers’ depressive symptoms may be especially consequential for the heritage language. One reason for this may have been that children may have had fewer interaction partners and learning opportunities for the heritage language than for the majority language, which received more support in daycares and schools. To our knowledge, the study by Cycyk et al. (2015) was the first to examine the connection between mothers’ depression and bilingual children’s heritage language skills. Thus, there is a need for further investigation on whether the connection is also evident for other age and language groups.
The purpose
The purpose of this study was to examine how mothers’ depressive symptoms are related to Turkish heritage language vocabulary development from fourth to sixth grade. Examining this connection is a building block to supporting families in passing on their heritage language, which may benefit the individual child as well as the entire family system (Adesope et al., 2010; Fillmore, 2000; Halle et al., 2014). Based on the extant research, we hypothesized that mothers’ depressive symptoms would be negatively related to children’s Turkish vocabulary in fourth grade. Moreover, we expected mothers’ depressive symptoms to be related to a reduced rate of growth in children’s Turkish vocabulary from fourth to sixth grade.
Method
Participants
The participants of this study were n = 139 children and their mothers who took part in a larger investigation on positive development of children from Turkish immigrant families in Germany. Data on this community sample were collected in the Ruhr area, which is a highly industrialized area in North-West Germany. For a description of recruitment, see Willard, Agache, Jäkel, Glück, and Leyendecker (2015). For the current study, families were considered eligible if the mother or her parents or grandparents were born in Turkey and if the mother indicated that Turkish, and not Kurdish (a minority language in Turkey) was the family language. Furthermore, the families had to have lived in Germany at least the past 3 years in order to ensure that the children were not monolingual Turkish speakers but had exposure to both Turkish and German. Also, the target child had to be born after 32 weeks gestational age, could not have a referral to a special needs school, and could not currently be living in a foster family.
On average, mothers were 37 years old (SD = 6, range 28–56). The majority of mothers (62%) had primary or lower secondary education. Of the mothers, 72% reported that they were born in Turkey and thus were considered first-generation immigrants. On average, these mothers had immigrated to Germany at the age of 16 years. In this study, 85% of the mothers and children lived in two-parent households. The majority of mothers reported having a low income; 45% of the mothers reported that their net monthly household income was in a bracket below 2000€/month (which is <60% of the median income in Germany for a family with two children), and another 28% reported that their income was between 2000€ and 2500€/month. On average, mothers reported using more Turkish than German with their children. Specifically, 43% of the mothers reported speaking mostly or only Turkish with their children and another 40% reported using equal amounts of Turkish and German. Additional descriptive information on mothers’ background is shown in Table 1.
Mothers’ background characteristics.
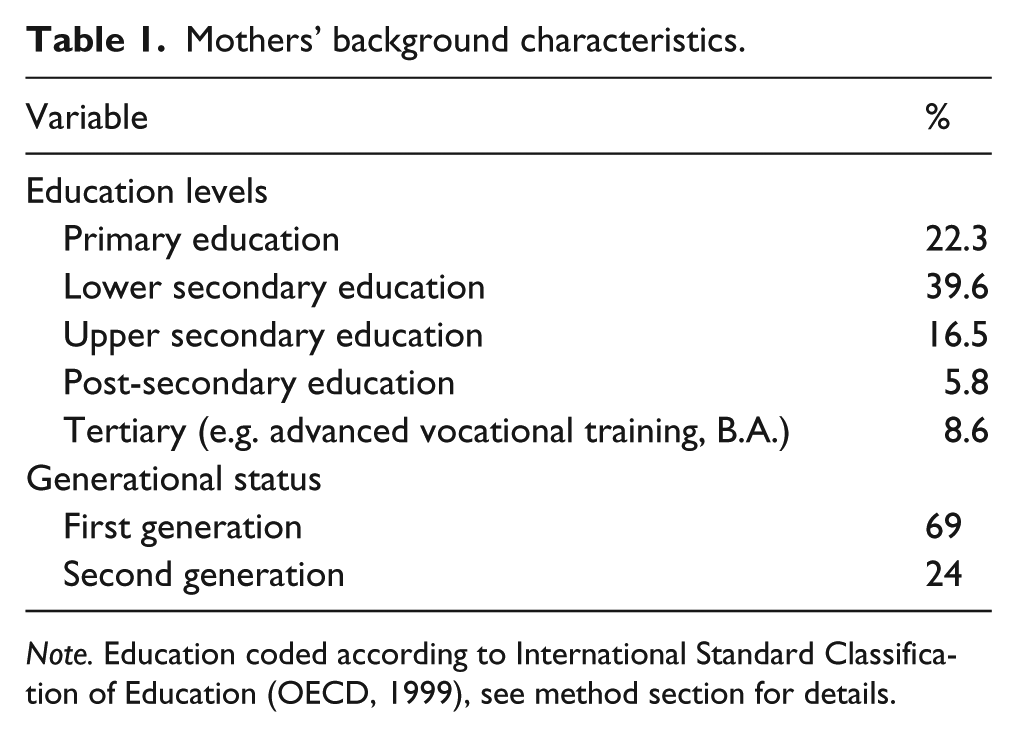
Note. Education coded according to International Standard Classification of Education (OECD, 1999), see method section for details.
At the first assessment, children were in fourth grade, and they were 10 years old on average (M = 10; 5 years, SD = 6 months, range 9;4–12;0 years). Approximately half (53%) of the children were girls. Two of the children immigrated to Germany under the age of three, and the remainder were born in Germany. All children attended schools where German was the language of instruction.
Measures
The measures for the mothers were available in German and Turkish. The measures were translated into Turkish by three teams of bilingual Turkish research assistants involved in the larger study. For each set of items, two separate teams completed a translation, and then differences were discussed with the third team to reach consensus.
Background questionnaire
The background questionnaire for mothers contained questions about the families’ background characteristics such as education, immigration history, and language use. Mothers’ educational levels were coded according to the International Standard Classification of Education (OECD, 1999). Mothers indicated what language they used with the target child on a five-point scale, with the response categories only Turkish, mostly Turkish, both languages equally often, mostly German, and only German. This widely used one-item measure has been shown to explain variance in bilingual children’s language outcomes (Hammer, Davison, Lawrence, & Miccio, 2009).
Mothers’ depressive symptoms
The Center for Epidemiological Studies Depression Scale 10-item short form (CES-D 10) is a widely used self-report screening measure of depressive symptoms for the general population (Andresen, Malmgren, Carter, & Patrick, 1994; Radloff, 1977). Internal consistency for the Turkish immigrant mothers in our sample was α = .83. The items ask about the frequency of depressive symptoms (e.g. loneliness, restless sleep) during the last week on a four-point scale with 0 = hardly or never (less than once a week), 1 = sometimes or occasionally (1–2 days a week), 2 = frequently or often (3–4 days a week) and 3 = constantly (5–7 days a week). The sum score of item ratings can range from 0 to 30. A score of 10 or higher indicates that a mother may have depressive symptoms (Andresen et al., 1994). As the CES-D 10 is a screening instrument, this does not equal a clinical diagnosis of depression.
Children’s Turkish receptive vocabulary
At the time of testing, no standardized Turkish vocabulary test was available for immigrant school-age children. Thus, the vocabulary test was a research version modeled on the Peabody Picture Vocabulary Test, Fourth Edition (PPVT-4) (Dunn & Dunn, 2007; Glück, 2009). A team of speech-language professionals, including Turkish native speakers, adapted the PPVT-4 items with consideration for cultural differences between the United States and Turkish immigrants in Germany. For example, if the target word was a widely used word in the US context but unfamiliar in the Turkish context, a new target word was selected from one of the three distractors. The test was computer-based, and the format similar to the WWT-6-10 (Glück, 2011). Children were asked to select a color illustration that matched the Turkish target word. The Spearman-Brown split-half reliability (odd versus even items) was .88.
Procedures
Data were collected by trained research assistants during three home visits. Home visits occurred in the spring of each year when the children were in fourth, fifth, and sixth grade. If requested by the mothers or if they had difficulty reading, the measures were read out loud to mothers in the language of their choosing by a Turkish-German bilingual research assistant. The Turkish vocabulary test was administered to the child by a research assistant in a different room. Families received 25€ as compensation and a small toy for the child.
Data analysis
Growth curve modeling of Turkish vocabulary raw scores over the three time points was conducted with the SPSS 22 mixed-models command using maximum likelihood estimation (IBM, 2013). The advantage of growth curve modeling using the long data format is that data can be used even if there are single data points missing, as is common in longitudinal studies. As outlined by Singer and Willett (2003), growth curve modeling was conducted in three stages. At every stage, model fit was evaluated by testing the difference in -2-log-likelihood against a chi-square distribution for nested models, or examining the AIC and BIC for non-nested models.
During the first stage, an unconditional means model with children’s Turkish vocabulary as the outcome was estimated to serve as a baseline for subsequent models. During the second stage, an unconditional growth model including the effect of time on children’s Turkish vocabulary was estimated to examine whether children showed growth in Turkish vocabulary. Time was represented by the age of the child in months at the particular time point. Age in months was centered on the average age at the first time point, 125 months, to ease the interpretation of the intercept. The intercept can then be interpreted as the Turkish vocabulary score of a 125-month-old child in fourth grade. Using age as a time metric accounts for children having somewhat different intervals between time points. Linear and quadratic trajectories were tested, and linear trajectories produced the best model fit. During this stage of modeling it was also determined that adding random effects for children’s age did not improve the model fit.
During the third stage, conditional growth models including mothers’ depressive symptoms (grand mean centered) as a time-varying predictor of children’s Turkish vocabulary were estimated. First, we estimated a conditional growth model containing only the effects of mothers’ depressive symptoms without any covariates. Next, we estimated a final model including mothers’ depressive symptoms controlling for a number of covariates. Several factors that have been found to be connected to heritage language development (Hammer et al., 2009; Place & Hoff, 2011; Willard et al., 2015) were considered. Mothers’ educational level (dichotomized into low = ‘less than upper secondary education’ versus high = ‘at least upper secondary education’), mothers’ generational status (first versus second generation), and children’s gender were considered as time-invariant covariates. Mothers’ language use with the child (grand mean centered to ease interpretation) was considered as a time-varying covariate. In a series of preliminary analyses, we determined that including the following effects on the intercept improved model fit: mothers’ education level, mothers’ generational status, mothers’ language use with their child, and children’s gender. Thus, these effects on the intercept were included in the final model presented in Table 3.
Results
Descriptive results
Descriptive statistics for mothers’ depressive symptoms, children’s Turkish vocabulary, and the time-varying covariate mothers’ language use with the child are displayed in Table 2. At all three time points, the mothers’ mean CES-D score was between 8.0 and 8.7 with a standard deviation of 5.8 or higher. At the first time point, 27% of the mothers had scores above the cutoff that indicated depressive symptoms, at the second 24%, and at the third 32%. These percentages are above the reported rates for depressive symptoms of women in Germany (16% for women of low socioeconomic status; Busch, Maske, Ryl, Schlack, & Hapke, 2013). At all three time points, there was considerable variance in children’s Turkish vocabulary.
Descriptive statistics for children’s Turkish vocabulary, mothers’ depressive symptoms (CES-D 10), and mothers’ language use with the child by time point.
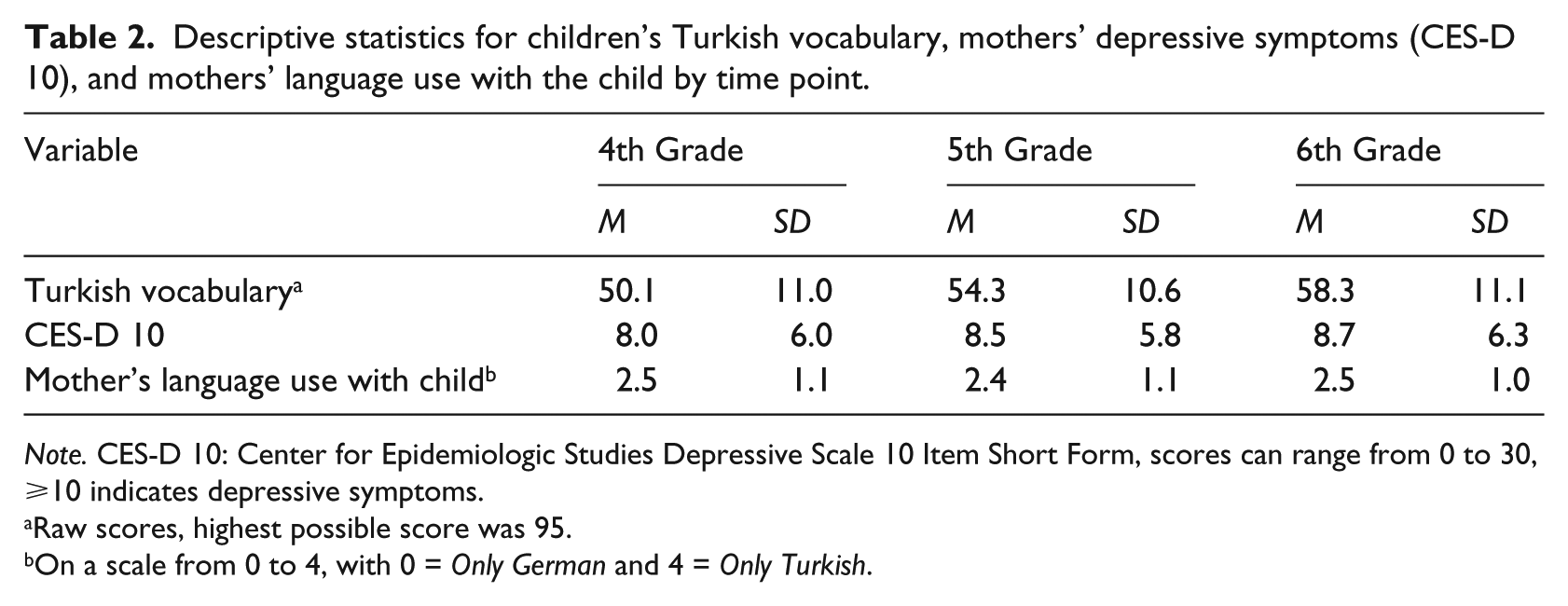
Note. CES-D 10: Center for Epidemiologic Studies Depressive Scale 10 Item Short Form, scores can range from 0 to 30, ⩾10 indicates depressive symptoms.
Raw scores, highest possible score was 95.
On a scale from 0 to 4, with 0 = Only German and 4 = Only Turkish.
Growth curve modeling
The unconditional means model produced an intraclass correlation coefficient of .71. Thus, there was sufficient variance due to interindividual differences in the overall mean Turkish vocabulary score of 51.2 to continue with growth curve modeling.
The unconditional growth model included the effect of children’s age in months (centered on the mean age at the fourth grade home visit), on their Turkish vocabulary. Age in months significantly predicted children’s Turkish vocabulary [γ 10 = 0.36, t (208.5) = 10.9, p ⩽ .001]. On average, children gained almost one point (equaling one word) on the Turkish vocabulary test every 2 months, not accounting for mothers’ depressive symptoms.
The first conditional growth model included the effects of maternal depression on children’s Turkish vocabulary in fourth grade as well as on their Turkish vocabulary growth. The latter effect was represented by the interaction age in months × mothers’ depressive symptoms score. Adding these effects improved model fit compared with the unconditional growth model. Mothers’ depressive symptoms did not significantly predict children’s Turkish vocabulary at the intercept, which was the measurement point in fourth grade when children were approximately 10 years old [γ 01 = 0.08, t (192.8) = 0.7, p = .456]. However, mothers’ depressive symptoms did significantly predict children’s growth in Turkish vocabulary between fourth and sixth grade [γ 11 = −0.01, t (151.2) = −2.2, p = .027]. As the coefficient was negative, this indicated that higher levels of depressive symptoms were connected to slower growth in children’s Turkish vocabulary.
The final conditional growth model included the effects of covariates in addition to those of mothers’ depressive symptoms (Table 3). When including the covariates, the effect of depression on vocabulary growth remained significant (γ 11 = –.02). An increase in mothers’ depression levels was associated with a decrease in the growth rate of children’s Turkish vocabulary. This shows that the effect is robust. When adding the effects of the covariates in the final model, the effect of mothers’ depressive symptoms on the intercept, which represented children’s fourth grade vocabulary, remained non-significant. Importantly, graphically, the children with highly depressed mothers start out at a higher Turkish vocabulary score than the children with less depressed mothers (Figure 1). In the final model, this is determined by a positive parameter estimate for the effect of mothers’ depression on children’s Turkish vocabulary in fourth grade. However, due to a large standard error, this parameter estimate is not significantly different from 0, which is also evidenced by the 95% confidence interval enclosing the value 0. Thus, even though graphically the effect looks quite large, it should not be interpreted as so.
Results of the final conditional growth model predicting children’s Turkish vocabulary.
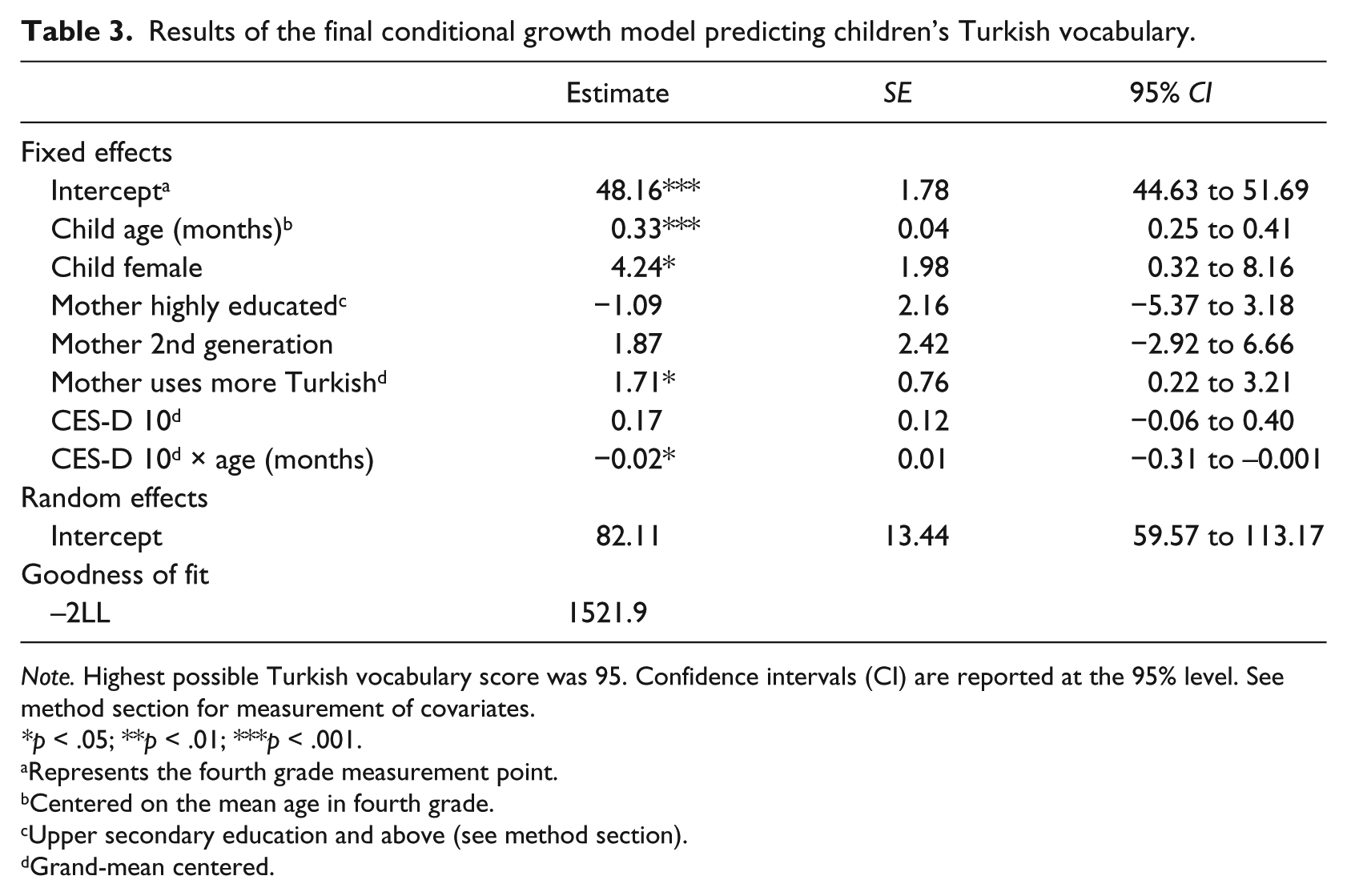
Note. Highest possible Turkish vocabulary score was 95. Confidence intervals (CI) are reported at the 95% level. See method section for measurement of covariates.
*p < .05; **p < .01; ***p < .001.
Represents the fourth grade measurement point.
Centered on the mean age in fourth grade.
Upper secondary education and above (see method section).
Grand-mean centered.
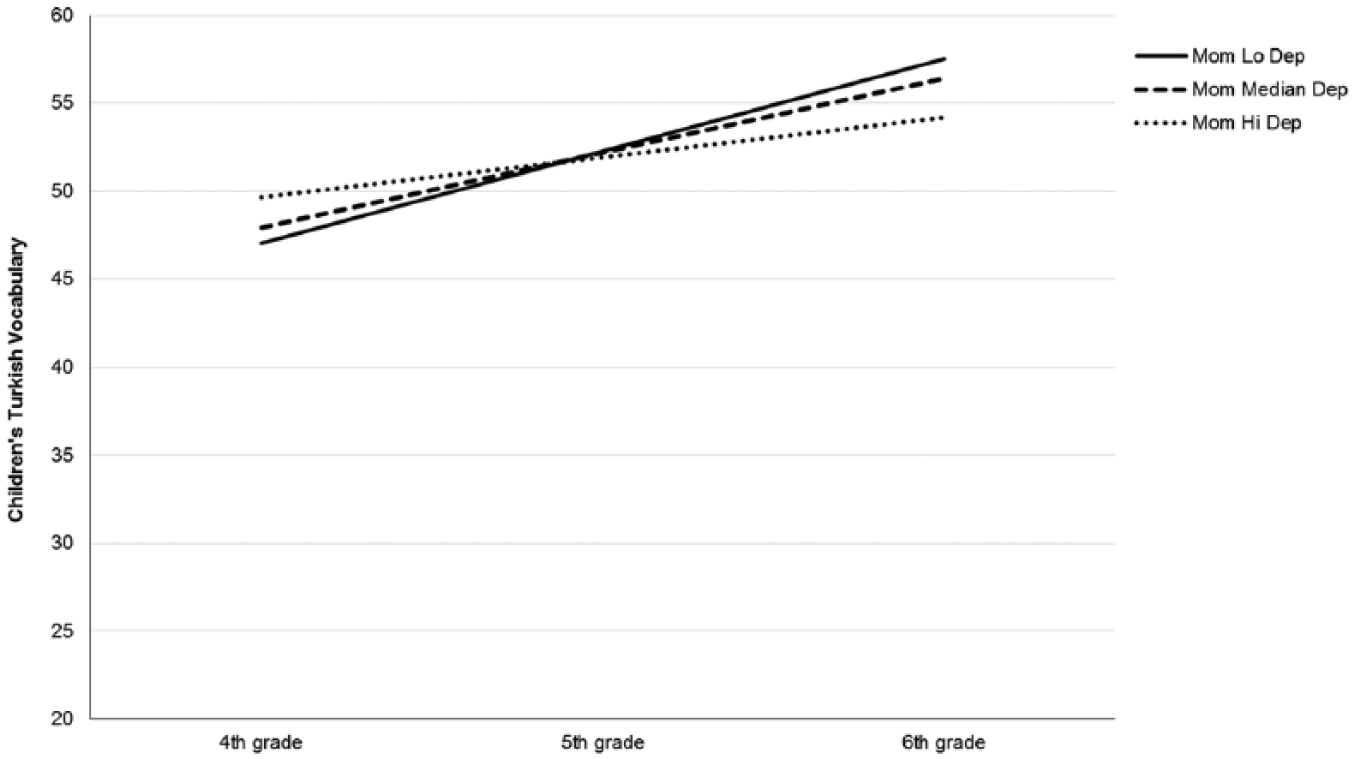
Prototypical growth trajectories showing the effect of mothers’ depressive symptoms on children’s Turkish vocabulary growth and a non-significant effect on the intercept. Mom Lo Dep = estimated Turkish vocabulary score for children whose mothers’ scored at the 10th percentile of depressive symptoms on the Center for Epidemiological Studies Depression Scale (CES-D), equaling a score of 2. Mom Median Dep = estimated Turkish vocabulary score for children whose mothers scored at the 50th percentile, equaling a score of 7. Mom Hi Dep = estimated Turkish vocabulary score for children whose mothers scored at the 90th percentile, equaling a score of 17. Covariates are set to child gender = male, mothers’ education = low, mothers’ generation = 1st generation and mothers’ language use = 2.5 (indicating a use of slightly more Turkish than German).
To illustrate the size of the effect of mothers’ depressive symptoms on Turkish vocabulary growth, consider, as an example, two children with the same age, gender, and fourth grade vocabulary, and their respective mothers with the same education level and generational status but different levels of depressive symptoms. One child has a mother with few depressive symptoms (for example, a score of 2, equaling the 10th percentile) and the other child a mother with many depressive symptoms (for example, a score of 17, equaling the 90th percentile). By sixth grade, the first child would have a predicted Turkish vocabulary score of 57.5, and the second child a score of 54.2, indicating a difference of three correct words on the vocabulary test, which equals about a third of a standard deviation. Figure 1 shows prototypical growth trajectories for children of mothers with low, median, and high levels of depressive symptoms, which were defined as the 10th, 50th, and 90th percentile, respectively.
Discussion
Given the increasing numbers of immigrants to Germany, we focused on the heritage language development of one large immigrant group, children of Turkish descent. Specifically, we were interested in whether mothers’ level of depressive symptoms was associated with their children’s Turkish vocabulary development from fourth to sixth grade. The results showed that contrary to our first hypothesis, mothers’ depressive symptoms were not significantly associated with children’s vocabulary at the study onset in fourth grade. However, in accordance with our second hypothesis, mothers’ depressive symptoms did predict growth in children’s vocabulary from fourth to sixth grade, albeit to a minor degree. More specifically, the higher a mother’s depressive symptoms score, the slower the growth of her child’s Turkish vocabulary.
This study is not the first growth curve modeling study to find no evidence of a connection between mothers’ depressive symptoms and children’s vocabulary at the first time point. The same result was obtained in the growth curve models by Pan et al. (2005) and Cycyk et al. (2015). This was the case despite children’s mean age in the three different samples ranging from 1 year to 10 years of age at the first assessment. One reason for this may be that the various modes of measurement were less sensitive to individual differences at the first time point. For example, in the Pan et al. (2015) study, the very young toddlers may have been intimidated by the novel situation. However, this finding may also indicate that mothers’ depressive symptoms are associated with children’s language development over the entire course of childhood, but it may take some prolonged exposure to a mother behaving differently due to depressive symptoms until a child’s language development shows any negative effects. In other words, growing up with a mother with depressive symptoms may be related to experiencing certain types of interactions that have cumulating long-term effects. An isolated period of time during which a mother has depressive symptoms may not have a measurable effect. Indeed, there is evidence that more chronic maternal depression is connected to parenting and child outcomes (NICHD ECCRN, 1999; Petterson & Albers, 2001). However, we do not know at what retrospective time point the mothers in this sample developed depressive symptoms. Unlike the toddlers in the Pan et al. (2005) study, the school-age children in our sample may well have had multiple years of exposure to a mother with depressive symptoms before the study onset. Thus, this result remains somewhat curious and should be further investigated in future studies.
The finding that mothers’ depressive symptoms were associated with slower heritage vocabulary growth concurs with the result by Cycyk et al. (2015) that mothers’ depressive symptoms were associated with slower growth in Latino preschoolers’ Spanish receptive vocabulary. It also is in line with the finding in Pan et al. (2005) that mothers’ depressive symptoms were associated with slower growth in toddlers’ vocabulary production. Together, these three longitudinal growth curve modeling studies suggest that mothers’ depressive symptoms can slow children’s vocabulary development throughout their lives. The larger number of cross-sectional findings points in the same direction (e.g. Brennan et al., 2000; NICHD ECCRN, 1999; Stein et al., 2008).
However, in both this study and Cycyk et al. (2015), the effect of mothers’ depressive symptoms on children’s language growth was small. A larger effect surfaced in Pan et al. (2005), who assessed word-type production of children interacting with their mothers. While interacting with their mothers, differences between children of depressed and non-depressed mothers may be more pronounced than is observable with a receptive vocabulary test. Word production during an interaction is not purely a measure of expressive vocabulary, but likely to be affected by children’s talkativeness and interaction patterns with their mothers. Moreover, our study covers a narrow range of time from fourth to sixth grade. The gaps in Turkish language vocabulary associated with mothers’ depressive symptoms may continue to widen over time. Yet, the small effect size we found shows that mothers’ level of depressive symptoms is only one of many factors that are connected to children’s language development. In reality, depressive symptoms may occur not as an isolated risk factor but as one among several. Multiple risk factors such as low-income status and immigrant status could have additive effects on vocabulary development or could interact in much more complicated ways. The combined effect of such multiple risks on children’s development may be very powerful (Evans, Li, & Whipple, 2013).
Limitations and future directions
This study has several limitations. First, Turkish vocabulary was assessed with an objective computerized receptive vocabulary test that has not yet been fully validated and standardized for school-age children. The development of language tests for Turkish heritage speakers in Germany is still in the early stages, with some standardized options available only for younger children (e.g. Glück, 2011). The lack of normative data for our receptive Turkish vocabulary test may make the “real life” size of the effect of depressive symptoms harder to gauge. Importantly, though, the presence of normative data is not necessarily the main concern when examining relationships between variables.
Second, a self-report screening questionnaire was used to assess depressive symptoms. Self-reports have been criticized for reflecting general distress instead of depression (Lovejoy et al., 2000; Van Dam & Earleywine, 2011). However, the short and reliable self-report made it possible to study a community sample with varying levels of depressive symptoms. Further reassurance for our use of a self-report comes from a meta-analysis of the relationship between maternal depression and parenting, where the effects were similar for self-reports and diagnostic interviews (Lovejoy et al., 2000).
Third, the scope of this study is limited to examining the effect of mothers’ well-being on children’s Turkish language development. Undoubtedly, fathers’ well-being also plays a role for children’s family life and development (Wilson & Durbin, 2010). Moreover, the presence of well fathers may be able buffer the effects of mothers’ depressive symptoms on children’s language development.
Further longitudinal research needs to examine the connection between mothers’ depressive symptoms and children’s vocabulary development in conjunction with other risk factors. Several other aspects of family characteristics such as poverty, parenting stress or marital discord may be important to consider in more complex models (Downey & Coyne, 1990). In the case of this study, the size of our sample limits the number of covariates that can be included in the statistical models. Larger sample sizes allow disentangling the individual contributions of co-occurring risk factors.
In addition, future studies should also examine whether the causal direction from mothers’ depressive symptoms to child heritage language vocabulary is indeed as theoretically assumed here. There may be reciprocal effects between mothers’ depressive symptoms and children’s heritage language vocabulary. More specifically, having a child with a small heritage language vocabulary may affect parent–child relationships, and those in turn could be connected to mothers’ depressive symptoms (Oh & Fuligni, 2010). A mother may feel that is harder to relate with a school-age child that does not speak the heritage language, and this may be a stressor that plays into her well-being. There is indeed evidence for such reciprocal effects between mother’s depression and child development for non-language outcomes (Elgar, McGrath, Waschbusch, Stewart, & Curtis, 2004). Further research could gain more insight into the direction of effects by longitudinally studying the processes which mediate between mothers’ depressive symptoms and children’s heritage language development, such as the interactions between parents and children.
Practical implications
The relatively high prevalence of depressive symptoms in our sample suggests that medical, psychological, and educational professionals should be observant of signs of depression in Turkish immigrant mothers. Importantly, depressive symptoms may not only be connected to a host of negative outcomes for the mothers themselves, but also for their children and their children’s language development. Not only young but also school-age children may experience such negative effects. This should be further motivation to help mothers access interventions or treatment. Immigrant mothers in Germany are currently underserved in the German health system, particularly regarding mental health (Machleidt, Behrens, Ziegenbein, & Calliess, 2007). As unexpected as it may seem, providing adequate health care to immigrant mothers may help them to provide a stimulating language environment for their children. This is necessary especially when families and particularly mothers are a main source of heritage language learning, as is the case for Turkish families in Germany. Mothers will likely not be aware that their own psychological state is related to their children’s development in so many different ways. If made aware, even those who experience only mild depressive symptoms may appreciate interventions targeting their own well-being.
Conclusion
This study adds to the extant literature by showing that mothers’ depressive symptoms are associated with slower language development in the case of children exposed to two languages—even into the school-age years. Increasing numbers of immigrants in Germany, Europe, and the US make this a noteworthy finding (UN Department of Economic and Social Affairs, 2015).
Currently, there is a strong focus on the amount and quality of language input that children receive in their homes. Beyond the immediate characteristics of language input, the families’ psychological well-being appears to be important for children’s language development. For many parents all over Europe, whether they are passing on Turkish as a heritage language or refugees just beginning to experience the challenges of being their child’s main teacher of their heritage language, this may be important to know.
Footnotes
Acknowledgements
We are very grateful to the participating families.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the NORFACE Era-Net Grant 292 to Birgit Leyendecker, Judi Mesman, and Brit Oppedal, and by a grant from the Ruhr University Research School PLUS, funded by Germany’s Excellence Initiative [DFG GSC 98/3].