
Abstract
Glycemic control and quality of life (QoL) are both considered indicators of health adaptation among adolescents with type 1 diabetes (T1D). The purpose of this study was to construct a path model addressing the influences of individual characteristics, school support, resilience, and self-care behaviors on glycated hemoglobin (HbA1c) and QoL among adolescents with T1D in Taiwan. This was a cross-sectional design study. A structured questionnaire was used to collect information on individual characteristics, school support, resilience, self-care behaviors, and QoL. The latest HbA1c was collected from medical records. Data from 238 adolescents with T1D were analyzed using structural equation modeling to test the hypothesized path model. The findings indicated that self-care behaviors and resilience both directly influenced HbA1c and QoL. School support directly influenced QoL but indirectly influenced HbA1c. We suggest that improving self-care behaviors and resilience could be considered an appropriate intervention for enhancing the health adaptation of adolescents with T1D. Increasing school support might be a strategy to improve QoL among adolescents with T1D.
Introduction
Type 1 diabetes (T1D) is one of the most common chronic diseases in children. The incidence has varied in different countries, ranging from .1/100,000/year in China to 36.5/100,000/year in Finland (The DIAMOND Project Group, 2006). Although the incidence and prevalence of T1D in Asian children are lower than those of Western children, T1D is still an important health issue for Asian children (Maahs et al., 2010). In Taiwan, the newest incidence of T1D was around 5.79/100,000, whereas the prevalence was 0.08% and 0.07% for girls and boys, respectively, under 19 years of age. The prevalence rate increased by 33% for children under 19 years of age (Jiang et al., 2012). Health care for children with T1D is an important health issue in Taiwan.
Adolescents encounter social, academic, and emotional challenges due to their convergence of numerous physical and hormonal changes. These situations impose unique challenges on adolescents with T1D. Adaptation indicates that an individual responds both physiologically and psychologically to the stress of living with a chronic disease. Glycemic control and quality of life (QoL) are considered physical and psychosocial indicators of health adaptation among adolescents with T1D, respectively (Whittemore et al., 2010). Glycated hemoglobin (HbA1c) is an important indicator for glycemic control in children with T1D. ADA (2014a) recommended that the HbA1c level among adolescents aged 13–19 should be lower than 7.5%. The QoL indicates the extent of the disease impact on the well-being of an individual (Cameron, 2003) and is increasingly recognized as one of the crucial psychosocial outcomes of diabetes control. Understanding the factors contributing to HbA1c and QoL is essential for health care providers to improve the health adaptation of adolescents with T1D.
Background
‘Childhood Adaptation Model to Chronic Illness: Diabetes Mellitus’ was proposed to describe factors that influence the health adaptation among adolescents with T1D (Whittemore et al., 2010). In this model, individual characteristics and individual responses directly influence the health adaptation of children with T1D. In previous studies (Lukács et al., 2013; Neylon et al., 2013), individual characteristics including age, gender, socioeconomic status, duration of diabetes, insulin treatment regimen, and frequency of insulin injections have been supported as relating to HbA1c and QoL. Individual responses including stressful life events, social competence, coping behaviors and styles, and self-care behaviors also serve as mediators between individual characteristics and health adaptation.
Self-care behaviors are activities performed by individuals to maintain their health and well-being (Orem, 1971). Adolescents with diabetes must perform demanding self-care behaviors to maintain their glycemic control. Insulin injections, daily blood glucose testing, dietary control, and management of hypo/hyperglycemia are significant components of self-care behaviors for adolescents with T1D (Wysocki et al., 1990). In a systematic review, self-care behaviors have been proved to positively correlate with QoL and negatively correlate with HbA1c, especially for adolescents with T1D (Guo et al., 2011).
For adolescents, management of T1D is stressful. Resilience refers to an individual’s capacity to maintain psychological and physical well-being in the face of stressful events (Ahern, 2006). It can be considered a factor of individual responses. Sense of competence, self-esteem, and positive expectations are characteristics of resilience (Fergus and Zimmerman, 2005). Resilience makes challenges become meaningful, thereby enhancing QoL, health-promoting behaviors, and health outcomes (Black and Ford-Gilboe, 2004). Resilience might influence the self-care behaviors of adolescents with T1D. However, the role of resilience on health adaptation of adolescents with T1D has been less addressed by empirical studies.
Adolescents spend a sizable portion of their days in school. School is an important place to support them for the management of their disease. The ADA (2014b) recommended that schools should reasonably accommodate the special needs of students with T1D. Greater flexibility in performing diabetes care at school was related to more effective HbA1c control and better QoL among adolescents with T1D (Wagner et al., 2006). Adolescents who reported being more satisfied with school support had lower levels of HbA1c (Lehmkuhl and Nabors, 2007). School is an external environmental factor. Therefore, school factors might influence health adaption of adolescents with T1D through the mediation of individual responses.
As mentioned above, significant associations were found among individual characteristics, school support, self-care behaviors, resilience, HbA1c level, and QoL among adolescents with T1D. However, the causal path relationships among these variables have been less addressed before, especially for Asian populations. Based on the empirical evidence and Whittemore et al.’s (2010) model, we hypothesized a model that addressed the relationships among individual and school characteristics (school support), individual responses (self-care behaviors and resilience), and health adaptation (HbA1c and QoL) of adolescents with T1D (Figure 1). Because HbA1c reflects the previous three months of glycemic control, we hypothesized that HbA1c influences QoL in this study. The purpose of this study was to test the hypothesized path model.
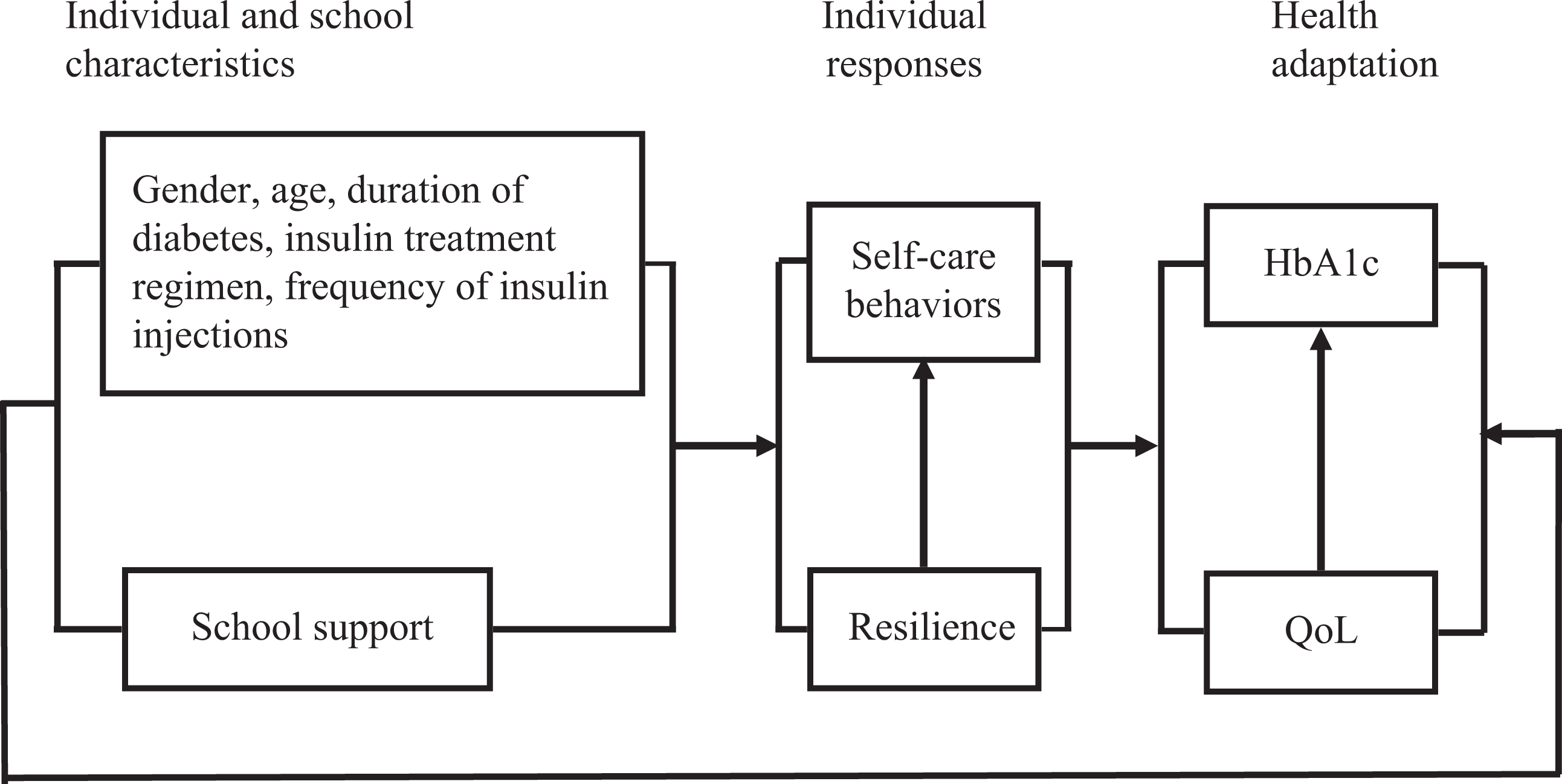
The hypothesized model of health adaptation among adolescents with type 1 diabetes. QoL: quality of life.
Methods
Samples
This was a cross-sectional design study. Adolescents were defined as children aged between 13 and 18 years (National Library of Medicine, 2013). We recruited adolescents who had been diagnosed with T1D for more than one year. The exclusion criteria are as follows: (a) presence of a major psychiatric or neurocognitive disorder that would inhibit the ability to participate or (b) dropped out of or graduated from school. We recruited eligible adolescents from five medical centers in Taiwan by sequential schedule. A trained research assistant approached these eligible adolescents when they visited the outpatient clinics of medical centers. Adolescents signed assent forms before participating in the study. The parents/guardians of adolescents also signed consent forms agreeing the participation of adolescents. At least 200 samples are regarded as sufficient for testing structural equation modeling (SEM) (Kline, 2011), so we approached 246 adolescents with T1D, and 238 of them agreed to participate in the study, with a response rate of 96.7%. Data were collected from February 2010 to March 2011.
Instrument
A structured questionnaire and medical records were used to collect data.
Questionnaire
The contents of the questionnaire are described as follows.
Individual characteristics
Gender, age, duration of diabetes, insulin treatment regimen, and frequency of insulin injections per day were collected.
Self-care behaviors
To prevent overburdening of the participants, a condensed Chinese version scale was developed in this study. Three pediatric endocrine physicians and two nursing researchers were invited to select self-care items that were significant for adolescents with T1D in Taiwan, based on literature reviews (Chang et al., 2007; Harris et al., 2000). The scale included items of administrating insulin (1 item), dietary control (2 items), management of hypoglycemia (1 item) and hyperglycemia (1 item), and blood glucose monitoring (2 items). Each item was scored from 0 points (never) to 4 points (always). The item mean score was calculated by summing the scores of individual items divided by the total number of items. A higher item mean score indicated that the participants had better self-care behaviors. The possible item mean score ranged from 0 to 4.
Adolescent resilience scale
A 12-item Chinese version of the resilience scale was used to measure the awareness of self-esteem, sense of mastery, and positive expectation among adolescents (Chen, 2007). Participants rated each item from 1 point (strongly disagree) to 5 points (strongly agree). A higher item mean score indicated that the participants perceived better resilience. The possible item mean score ranged from 1 to 5.
School support scale
No known scale has been developed to measure diabetes-specific school support. Accordingly, the authors developed a 5-item school support scale to assess adolescents’ perceptions about the support of meals, materials, and school personnel for their diabetes care in school. Participants responded to each item from 1 point (strongly disagree) to 5 points (strongly agree). A higher item mean score indicated that participants perceived better school support. The possible item mean score ranged from 1 to 5.
Quality of life
A short form of the Chinese version of the Diabetes Quality of Life Youth Scale (C-DQOLY-SF) (Wang et al., 2011) was used to measure the diabetes-specific QoL of adolescents. The C-DQOLY-SF included subscales of life satisfaction (8 items), diabetes impact (9 items), and diabetes-related worry (8 items). The items were rated from 1 point (very dissatisfied) or (all of the time) to 5 points (very satisfied) or (never) according to different subscales. A higher item mean score indicated that participants perceived better QoL. The possible item mean score ranged from 1 to 5.
Medical records
The latest HbA1c data were obtained from the medical records in the hospital for each participant.
Validity and reliability
Seven experts comprising endocrine physicians, nursing professors, and school nurses examined the content validity of the scales used in this study. The experts rated each item from 1 point (not relevant) to 4 points (very relevant). The number of items rated by 3 or 4 was divided by the total number of items, and this was taken to be the content validity index (CVI) of the scale. The CVI for all scales ranged from 0.94 to 1.0. Promax rotation of principal axis factor analysis was performed to examine the construct validity of each scale. The internal consistency of each scale was assessed by Cronbach’s α. Factor analysis and internal consistency were conducted based on the data of all participants in the study. The test–retest reliability was evaluated by administering the questionnaires twice within a two-week interval to 21 adolescents who satisfied the inclusion criteria. The test–retest reliability of each scale was calculated using intraclass correlation coefficients. As shown in Table 1, each scale had acceptable construct validity and reliability.
Summary of the reliability and validity for scales.
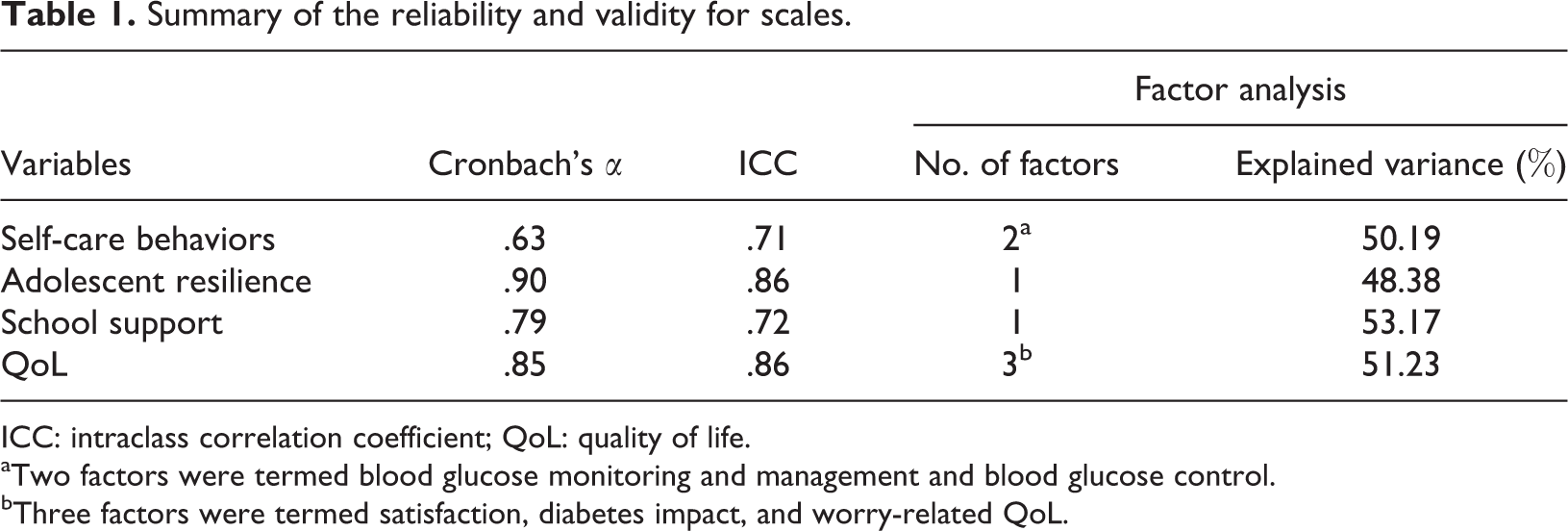
ICC: intraclass correlation coefficient; QoL: quality of life.
aTwo factors were termed blood glucose monitoring and management and blood glucose control.
bThree factors were termed satisfaction, diabetes impact, and worry-related QoL.
Data analysis
Statistical Package for Social Sciences version 16.0 for Windows was used for descriptive and bivariate correlation analysis. The hypothesized path model was tested using SEM, which was performed by AMOS version 17.0.2. A model was considered to have goodness of fit if the χ 2 was not significant, both the comparative fit index (CFI) and normed fit index (NFI) were greater than .95, and the root mean square error of approximation (RMSEA) values were approximately .06 (Kline, 2011). A p value of less than .05 was considered statistically significant.
Ethical considerations
The study was approved by the institutional review board of each hospital at which the study was conducted. All adolescents and their parents/guardians were informed that their confidentiality and anonymity were guaranteed, and there would be no penalty for declining to participate in the study. Participants retained the rights to withdraw from the study at any time.
Results
Distributions of individual characteristics and their association with HbA1c and QoL
The duration of diabetes ranged from 1 year to 17 years. In terms of frequency of insulin injections per day, 97 participants (40.8%) were ≤2 times, 32 participants (13.4%) were 3 times, and 109 participants (45.8%) were ≥4 times. As shown in Table 2, no significant associations were found between individual characteristics and HbA1c or those between QoL. Age significantly negatively associated with self-care behaviors, school support, and QoL (Table 3).
Summary of individual characteristics and their association with HbA1c and QoL (N = 238).

QoL: quality of life; HbA1c: glycated hemoglobin.
Descriptive and correlation of variables (N = 238).
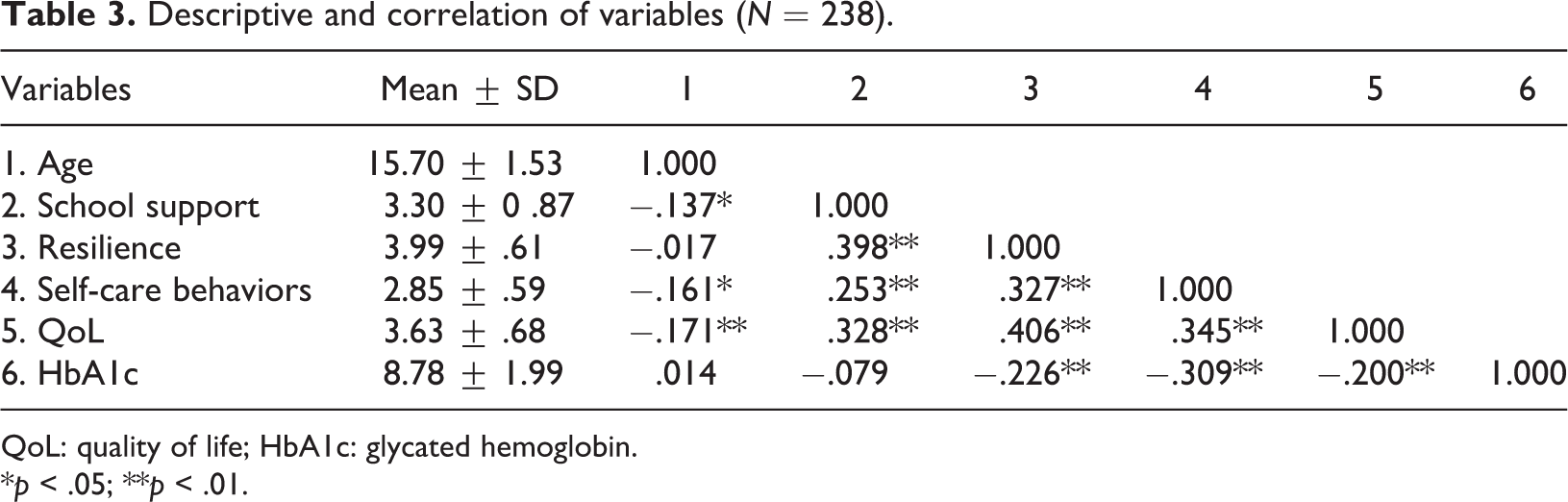
QoL: quality of life; HbA1c: glycated hemoglobin.
*p < .05; **p < .01.
Distributions of school support, self-care behaviors, resilience, HbA1c, QoL, and correlation among them
Distributions of school support, self-care behaviors, resilience, HbA1c, and QoL are shown in Table 3. According to the age-specific control goal recommended by the ADA (2014a), the HbA1c of 54 participants (22.7%) were lower than 7.5%; whereas in 184 participants (77.3%), it was equal to or more than 7.5%. Except for the association between school support and HbA1c, the bivariate associations among school support, resilience, self-care behaviors, HbA1c, and QoL were significant and in expected directions.
Test of the hypothesized model
We did not test the paths between variables that were not significantly associated in bivariate analysis. As shown in Figure 2, age significantly negatively influenced school support, self-care behaviors, and QoL. School support significantly positively influenced on self-care behaviors, resilience, and QoL. Resilience significantly positively influenced self-care behaviors and QoL but significantly negatively influenced HbA1c. Self-care behaviors significantly positively directly influenced QoL but significantly negatively influenced HbA1c. The path from HbA1c to QoL was not significant.
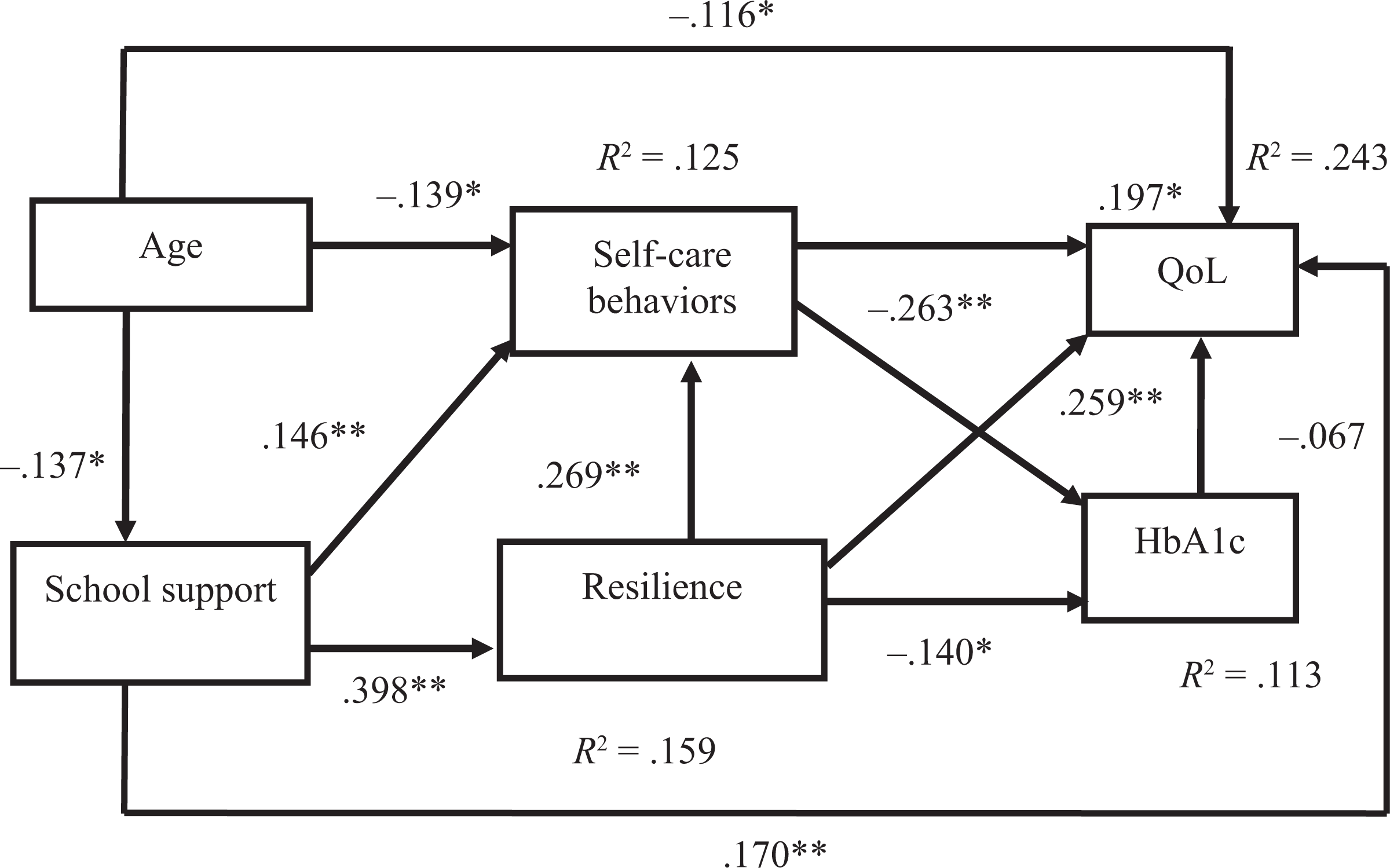
The final model of health adaptation among adolescents with type 1 diabetes. *p < .05; **p < .01. QoL: quality of life.
In terms of indirect effect, school support significantly positively influenced self-care behaviors (β indirect = .107, p < .01) and QoL (β indirect = .161, p < .01), significantly negatively influenced HbA1c (β indirect = −.122, p < .01). Resilience significantly negatively influenced HbA1c (β indirect = −.071, p < .05) but significantly positively influenced QoL (β indirect = .067, p < .05). Age did not significantly influence resilience (β = −.055, p > .05), self-care behaviors (β = −.032, p > .05), HbA1c (β = −.053, p > .05), and QoL (β = −.06, p > .05).
The fit indices of the model were as follows: χ 2 = 1.188, degree of freedom = 3, p = .756, NFI = .993, CFI = 1.000, RMSEA = .001 (95% CI = .000–.076), which indicated that the model fitted the data well. The final model accounted for 11.3% and 25.9% of the total variance of HbA1c and QoL, respectively.
Discussion
In this study, 77.3% of the participants did not satisfy the age-specific HbA1c control goal recommended by ADA (2014a). Studies of Western and Asian adolescents (Hilliard et al. 2013a; Hilmi et al., 2013; Moore et al., 2013) found more than two-thirds of adolescents with T1D did not achieve the recommended goal of HbA1c control. Improving glycemic control among adolescents with T1D should be a global concern of health care providers. The item mean score of QoL (3.63 ± .68) was at a medium to high level, indicating that participants of this study possessed acceptable QoL, which is consistent with a study conducted in the United States (Hilliard et al., 2013b). The path from HbA1c to QoL was not supported in this study. The finding is consistent with a previous study (Ingerski et al., 2010). Health care providers should apply diverse strategies to individually improve HbA1c control or QoL among adolescents with T1D.
We found that participants of older age tended to perceive worse school support, worse self-care behaviors, and worse QoL. These results are consistent with previous studies (Abolfotouh et al., 2011; Paris et al., 2009). Health care providers should place more effort on diabetes care of adolescents as they grow up. In this study, self-care behaviors not only positively directly influenced HbA1c and QoL but were also a mediator between school support and HbA1c. Thus, self-care behaviors were particularly important for improving health adaption of adolescents with T1D. Compared with the maximum possible score, the self-care behaviors of participants (2.85 ± .59) were at a medium level in this study. Adolescents tended to pursue identification from peers and independence from parents (Court et al., 2008). Performing self-care behaviors is not the first priority in adolescent life, which might result in poor self-care behaviors. The result echoes the recommendation of the ADA (2014a), which suggested that self-care behaviors should be regularly evaluated in clinical settings for adolescents with T1D. Health care providers should educate adolescents with T1D on the benefits of performing self-care behaviors and emphasize their responsibility in self-care behaviors. In this study, resilience and school support directly influenced self-care behaviors. Improving resilience and/or school support might be appropriate strategies to enhance self-care behaviors of adolescents with T1D.
Resilience not only directly influenced self-care behaviors but directly influenced HbA1c and QoL in this study. The results support the important role of resilience on health adaptation of adolescents with T1D. Resilience emphasizes the strengths and assets of individuals rather than deficits (Padesky and Mooney, 2012). Health care providers can help adolescents with T1D by recognizing their strengths or assets and encouraging them to utilize these strengths and assets to adapt to the negative impact of diabetes on their lives. Quality of schooling can influence the resilience of children (Musick et al., 2008). It is not surprising to find that school support directly influenced resilience in this study.
School support more specifically influenced QoL in this study. Increasing school support could be a strategy to improve QoL. Increasing knowledge of diabetes control for school personnel appears useful to provide a supportive school environment (Wagner and James, 2006). Health care providers can educate school personnel to obtain the knowledge and positive attitude toward caring for adolescents with T1D in school. Health care providers can also cooperate with school personnel to provide a more flexible school schedule that satisfies the special needs of adolescents with T1D in school.
In this study, the explained variances of HbA1c and QoL in the model were only 11.3% and 24.3%, respectively. Psychological and family responses can influence health adaption of adolescents with T1D (Whittemore et al., 2010). To increase the explained variance of HbA1c and QoL, variables of psychological and family responses, such as depression and family conflict which have been found to be negatively associated with HbA1c (Drotar et al., 2013; Neylon et al., 2013), could be included in the model in the future. Scales of self-care behaviors and school support were first developed in this study, however; these two scales demonstrated acceptable validity and reliability. Although the Cronbach’s α of self-care behaviors was .63, it was above acceptable level for a preliminary developed scale (Kline, 2000). In order to more comprehensively capture the construct of self-care behaviors and school support of adolescents with T1D, further studies are required to revise these two scales.
Limitations
There are several limitations in this study. We only recruited 238 participants from Taiwan, which might limit the generalizability of the findings. The power was .60 by post hoc power analysis (Preacher and Coffman, 2006). In the future, we might replicate the study in larger and more diverse populations to generalize the results and improve the power. SEM only provides information to indicate that a hypothesized model failed to be rejected. Longitudinal and experimental designs are needed to further confirm the path relationships among factors supported by the study.
Conclusions and clinical implication
In this study, we applied a model developed from the United States to model the health adaptation of Taiwanese adolescents with T1D. Factors contributing to HbA1c and QoL are similar cross-culturally. Self-care behaviors and resilience are key factors that can simultaneously affect HbA1c and QoL of adolescents with T1D. Improving self-care behaviors and resilience could be considered an appropriate intervention for enhancing the health adaptation of adolescents with T1D. School support more specifically influenced QoL. Increasing school support might be a strategy to improve QoL among adolescents with T1D. The results expand the knowledge of health adaptation among adolescents with T1D.
Footnotes
Acknowledgment
The authors wish to express thanks to Chin-Mi Chen (School of Nursing, National Defense Medical Center, Taiwan) for permission to use the resilience scale.
Conflict of interest
The authors declared no conflicts of interest.
Funding
Study funding was provided by the National Science Council, Taiwan (NSC 98-2314-B-037-047).
Ethical approval
Ethical approval was given by the Kaohsiung Medical University in Taiwan.