
Abstract
Childhood chronic illness is a potential source of distress and can be a traumatic experience both for the child and for the family. Several studies highlighted the importance of integrating psychosocial care and standard medical practice in the child’s care. The current pilot study is the first investigation that compared distress in children and their mothers living through a life-threatening illness (cancer) and a non life-threatening (juvenile rheumatoid arthritis) chronic disease. Findings show that there are differences in the psychological functioning in children with respect to age. Moreover, the presence of posttraumatic stress symptoms in mothers of children with cancer seems to be a possible key to understanding the psychological response in this specific population.
Introduction
Chronic childhood illness is a potential source of distress and there is growing recognition that the child’s care must focus not only on medical therapies but also on the psychosocial well-being of patients and their families as a way of integrating psychosocial care and standard medical practice (Cousino and Hazen, 2013). The perception of health and quality of life in children with chronic diseases as well as the impact of the disease and its treatment on other members of their family has become a major focus of research over the past decade (Bruns et al., 2008; Latal and Sennhauser, 2012). Several studies have demonstrated that childhood chronic disease can be a traumatic experience both for the child and for the family (Cousino and Hazen, 2013; Goldbeck, 2006; Jones, 2012; Payot and Barrington, 2011).
The view of childhood cancer as a traumatic event, and the consequent application of a traumatic stress model toward understanding the experiences of children with cancer, has become a major focus of research in pediatric oncology over the past years (Graf et al., 2013; Phipps et al., 2009). Childhood cancer can impact quality of life, mental and physical health, daily living activities, family dynamics, identity formation, parental and sibling roles, as well as sense of meaning (Jones, 2012). It is common for parents to experience significant emotional distress after learning that their child has cancer and for families to go through a period of severe disruption (Weihs and Reiss, 2000). Childhood cancer treatment often requires a dramatic change in the life situation of the family, with emotional reactions including fear, helplessness, disbelief, anger, anxiety, confusion, hope, concern, and shock (Jones, 2012). Most children experiencing significant trauma display disturbances in mood, arousal, and behavior, and many studies have reported on the incidence of posttraumatic stress disorder (PTSD) or subclinical levels of posttraumatic stress symptoms (PTSS) in children with cancer (Phipps et al., 2009; Stuber et al., 2011). Many studies have also shown that the parents (particularly the mothers) and children experience elevated levels of PTSD or PTSS relative to controls or population norms (Axia et al., 2006; Kazak et al., 2005; Stuber et al., 2011). In order to understand the short- and long-term psychological consequences of cancer on the child and the child’s family, the Pediatric Medical Traumatic Stress (PMTS) model has been introduced. The PMTS is defined as ‘a set of psychological and physiological responses of children and their families to pain, injury, serious illness, medical procedures, and invasive or frightening treatment experiences’ (Kazak et al., 2006, pp. 343). In PMTS and PTSS, an individual may not necessarily meet PTSD diagnostic criteria, yet may still suffer from serious distress.
The aim of this pilot study was to increase the knowledge about psychological functioning in children and their mothers living through cancer compared to another chronic and serious disease and to healthy children. For comparison we considered the juvenile rheumatoid arthritis (JRA) chronic disease. In JRA, despite aggressive treatment, daily pain and accompanying impairments in functioning persist for a subset of children (Russo et al., 2012). In this disease, symptoms, physical disabilities, and treatment can place a strain on the child and family. In JRA, family is a target of intervention, both because of the crucial relationship of dependence in developing age and because of the impact of a chronic health condition affecting the child in the family setting in terms of quality of life and well-being (Payot and Barrington, 2011; Rapoff et al., 2003).
The specific aim of this study was to assess the impact of life threatening in psychological functioning response in children and their mothers living through a life-threatening (i.e. cancer) and non life-threatening (i.e. JRA) chronic disease.
Methods
Subjects
We selected a cohort of consecutive patients aged 2–12 years diagnosed with a malignant solid tumor at least two to six months before the recruitment. All patients were hospitalized and currently on chemotherapy treatment. From the initial pool of patients (N = 18), we subsequently excluded children with psychological and behavioral problems prior to the onset of the disease (n = 2). Children with parents diagnosed with psychiatric disorders were also excluded (n = 1). The presence of any psychological and behavioral problems or drug treatment was defined using an anamnestic interview with the mothers.
All the parents of the children who met the criteria agreed to take part in the study. A total of 15 children (females/males (F/M) = 9/6; mean age (SD) = 6.6 (3.2) years; range = 2–11 years) and their mothers (mean age (SD) = 36.5 (5.38) years; range = 29–47 years) met the above-mentioned criteria and were assessed.
Two control groups of children and their mothers matched for sex, age, and socioeconomic status (Hollingshead, 1975) were recruited. The first group consisted of 15 hospitalized patients (F/M = 9/6; mean age (SD) = 6.9 (3.4) years; range = 2–12 years) with JRA. The second group consisted of 15 physically healthy children (F/M = 9/6; mean age (SD) = 6.4 (3.1) years; range = 2–12 years) and their mothers. None of the children recruited had previous psychological or behavioral problems or parents diagnosed with psychiatric disorders or relevant adjustment difficulties toward their children’s diseases.
All patients and their mothers were recruited at the Bambino Gesù Hospital. The healthy children and their mothers were recruited through pediatricians and kindergartens. Table 1 summarizes the sociodemographic description of the study population (see supplementary materials). Local ethics committee approval and written informed consent were obtained before study initiation.
Measures
The assessment procedure, including an anamnestic interview, involved all mothers and was administrated by a licensed psychologist. We asked each mother to consider the past two months for all the instruments. All mothers completed the following measures.
Child behavior checklist
Child Behavior Checklist (CBCL) (Achenbach and Rescorla, 2000, 2001), designed to be completed by parents, is an inventory that evaluates a child’s social and behavior competence. The questionnaires contain items/symptoms of psychopathology. For the following questionnaires, we used the Italian version with Italian normative data (D’Orlando et al., 2010; Frigerio et al., 2006):
The CBCL 1.5–5 (Achenbach and Rescorla, 2000) for children aged two to five years. It provides scores for (a) seven syndrome scales divided into internalizing symptoms (i.e. emotionally reactive, anxious/depressed, somatic complaints, and withdrawn) and externalizing symptoms (i.e. attention problems and aggressive behavior), and Sleep Problems; (b) internalizing problems scale; (c) externalizing problems scale; and (d) total problems scale. The CBCL 6–18 (Achenbach and Rescorla, 2001) for children aged 6–12 years. It provides scores for (a) eight syndrome scales divided into internalizing symptoms (i.e. anxious/depressed, withdrawn/depressed, and somatic complaints), externalizing symptoms (i.e. rule-breaking behavior and aggressive behavior), social problems, thought problems, and attention problems; (b) internalizing problems scale; (c) externalizing problems scale; and (d) total problems scale. Both CBCL/1.5–5 and CBCL 6–18 show good internal consistency (α = .92 and α = .97, respectively) and excellent test–retest reliability (r = .85 and r = .81, respectively) (Achenbach and Rescorla, 2000, 2001).
Adult self-report 18–59
Adult Self-Report (ASR) (Achenbach and Rescorla, 2003) is a self-report in which the subject (i.e. mothers) is rated on various behavioral and emotional problems. It provides scores for eight syndrome scales divided into internalizing (i.e. anxious/depressed, withdrawn, and somatic complaints), externalizing (i.e. aggressive behavior, rule-breaking behavior), intrusive thought problems, and attention problems. This questionnaire was used for describing the mothers’ well-being/ill-health. We used the official Italian translation of the questionnaire (http://www.emedea.it/aseba/strumenti/eta_adulta.php). The ASR shows solid psychometric properties with good internal consistency (α = .83), test–retest reliability (r = .80), and validity (Achenbach and Rescorla, 2003).
Parenting stress index–short form
Parenting Stress Index–Short Form (PSI-SF) (Abidin, 1995) is a self-report questionnaire designed to quantify parenting stress based on the interrelationship between the child and the parents’ characteristics. The PSI/SF consists of three subscales and a total stress score. The three subscales are parental distress (PD), parent–child dysfunctional interaction, and difficult child. We used the Italian version of the questionnaire and Italian normative data (Guarino et al., 2010). The PSI-SF shows solid psychometric properties with good internal consistency (α = .92), test–retest reliability (r = .70), and validity (Abidin, 1995).
Trauma symptom inventory A
Trauma Symptom Inventory A (TSI-A) (Briere, 1995) is a self-report questionnaire designed to assess PTSS in adults (i.e. mothers). It includes not only symptoms typically associated with PTSD but also those intra- and interpersonal difficulties associated with more chronic psychological trauma. The items are divided into three validity scales (response level, atypical response, and inconsistent response) and eight clinical scales, namely, anxious arousal, depression, anger/irritability, intrusive experiences, defensive avoidance, dissociation, impaired self-reference, and tension reduction behavior. This questionnaire was used for describing the mothers’ well-being/ill-health. We used the Italian version of the questionnaire with Italian normative data (Gambetti et al., 2011). The TSI-A shows solid psychometric properties with good internal consistency (α = .86) and validity (Briere, 1995).
State–Trait anxiety inventory
State–Trait Anxiety Inventory (STAI) (Spielberger, 1983) is a self-report questionnaire assessing anxiety symptoms with regard to both current (state) and personality (trait) anxiety. This questionnaire was used for describing the mothers’ well-being/ill-health. We used the Italian version of the questionnaire and Italian normative data (Pedrabissi and Santiniello, 1989). Several lines of evidence have shown that STAI has an elevated construct and concurrent validity and present high test–retest reliability ranged from .65 to .75. Internal consistency coefficients for the scale have ranged from .86 to .95 (Spielberger, 1983).
Statistical analysis
All statistical analyses were carried out using SPSS 21.0 for Windows (SPSS Inc, Chicago, Illinois, USA). Between-group comparisons of frequencies and means were used for parent (self-report scales), medical (cancer, JRA, and healthy), and child (reports-form scales) variables. Between-group comparisons were performed using ‘multivariate analysis of variance’ (MANOVA) and Scheffè’s post hoc test. All analyses were performed at a significance level of p = .05.
Results
There were no significant differences in age, gender, or socioeconomic status between the cancer group and the control group (JRA and healthy), nor among children or mothers.
Child behavior checklist 1.5–5
MANOVA showed statistical significance, F(8, 8) = 20.98, p < .001, for CBCL 1.5–5 between-group comparison. The univariate effects showed statistical significance in the following scales: total problems, F(2, 17) = 3.82, p < .05; externalizing problems, F(2, 17) = 4.43, p < .05; aggressive behavior, F(2, 17) = 5.83; p < .05. Scheffè’s post hoc analysis revealed that the cancer group reported significantly lower scores than the JRA control group in the total problems scale (p = .05), externalizing problems scale (p = .05), and aggressive behavior scale (p < .01), while no significant differences were found in cancer group with respect to the healthy group (p = n.s.). For each scale, comparisons between control group showed significantly higher scores in the JRA group compared with the healthy group (p < .05). Detailed results of the CBCL 1.5–5 are shown in Figure 1(a) and Table 2 (see supplementary materials).
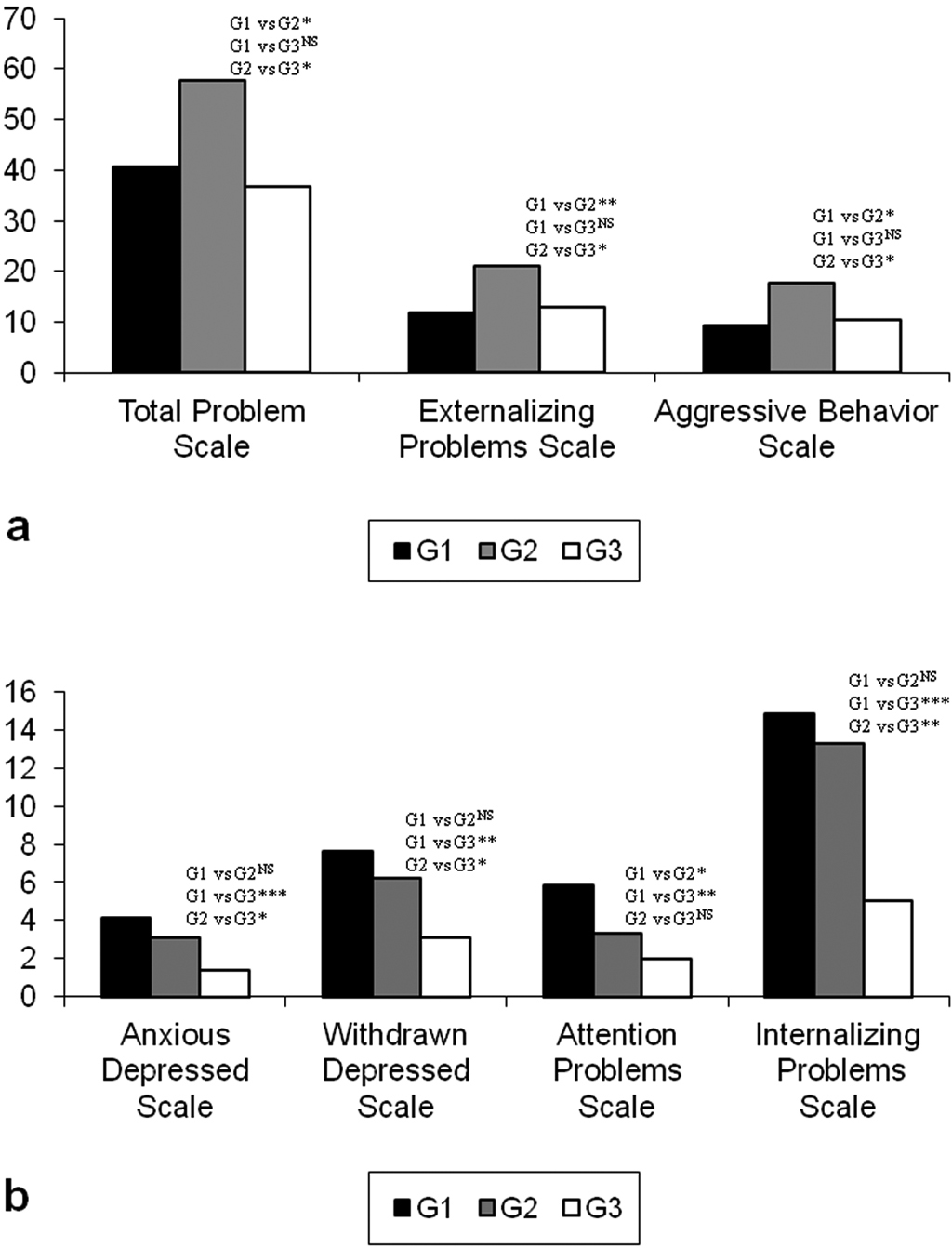
Panel (a) illustrates the scores of total problems, externalizing problems, aggressive behavior scales assessed by CBCL 1.5–5. Panel (b) illustrates the scores of anxious/depressed, withdrawn/depressed, attention problems internalizing problems scales assessed by CBCL 6–18; *p < .05; **p < .01; ***p < .001; NSp: not significant. G1: cancer group; G2: juvenile rheumatoid arthritis group; G3: healthy group; CBCL: Child Behavior Checklist.
Child behavior checklist 6–18
MANOVA showed statistical significance, F(22, 24) = 3.60, p < .05, for CBCL 6–18 between-group comparison. The univariate effects showed statistical significance in the following scales: anxious/depressed, F(2, 26) = 9.06, p < .001; withdrawn/depressed, F(2, 26) = 6.87, p < .01; attention problems, F(2, 26) = 5.85, p < .01; and internalizing problems, F(2, 26) = 8.70, p < .01. Scheffè’s post hoc analysis revealed that the cancer group reported significantly higher scores than the JRA control group in the attention problems scale (p < .05) but not in the anxious/depressed, withdrawn/depressed, or internalizing problems scales (p = n.s.). However, significant differences in all scales were found in the cancer group with respect to the healthy control group (anxious/depressed scale: p < .001; withdrawn/depressed scale: p < .01; attention problems scale: p < .01, and internalizing problems scale: p < .001). Between control group comparisons showed significantly higher scores in the JRA group compared to the healthy group in the anxious/depressed (p < .05), withdrawn/depressed (p < .05), and internalizing problems (p < .001) scales but not in the attention problems scale (p = n.s.). Detailed results of the CBCL 6–18 are shown in Figure 1(b) and Table 2 (see supplementary materials).
Adult self-report 18–59
MANOVA showed statistical significance, F(20, 66) = 3.27; p < .001, for ASR between-group comparisons. The univariate effects showed statistical significance in the following scales: anxious/depressed, F(2, 44) = 4.06, p < .001, and somatic complaints, F(2, 44) = 8.94, p < .001. Scheffè’s post hoc analysis revealed that the cancer group reported significantly high scores than the control groups (JRA and healthy) for both scales, that is, the anxious/depressed scale (p < .05) and the somatic complaints scale (p < .01). Between control group comparisons showed no significant differences (p = n.s.). Detailed results of the comparisons are shown in Figure 2(a) and Table 3 (see supplementary materials).
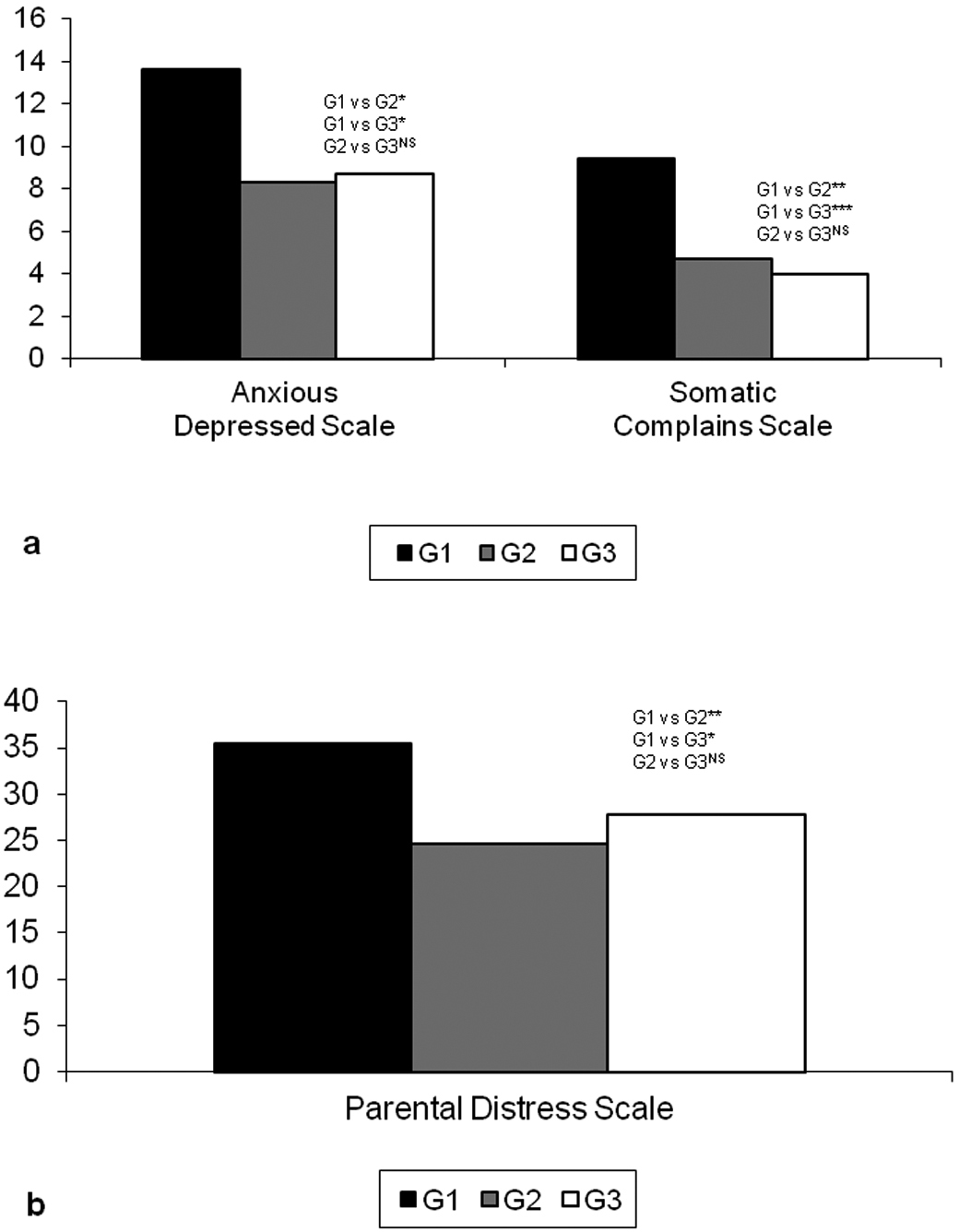
Panel (a) illustrates the scores of anxious/depressed, somatic complaints scales assessed by ASR. Panel (b) illustrates the scores of PD scale assessed by PSI-SF; *p < .05; **p < .01; ***p < .001; NSp: not significant. G1: cancer group; G2: juvenile rheumatoid arthritis group; G3: healthy group; ASR: Adult Self-Report; PD: parental distress; PSI-SF: Parenting Stress Index–Short Form.
Parenting stress index–short form
MANOVA showed statistical significance, F(8, 8) = 20.98; p < .001, for PSI/SF between-group comparisons. The univariate effects showed statistical significance in the PD scale, F(2, 44) = 7.45, p < .01. Scheffè’s post hoc analysis revealed that the cancer group reported significantly higher scores than JRA control group in the PD scale (p < .001). However, significant differences in only the PD scale (p < .05) were found in the cancer group with respect to the healthy control group.
Between control group comparisons showed no significant differences (p = n.s.). Detailed results of the PSI/SF are shown in Figure 2(b) and Table 4 (see supplementary materials).
Trauma symptom inventory A
MANOVA showed statistical significance, F(16, 79) = 10.31, p < .001, for TSI-A between-group comparisons. The univariate effects showed statistical significance in the following scales: intrusive experiences, F(2, 44) = 11.93, p < .001, defensive avoidance, F(2, 44) = 8.52, p < .001, dissociation, F(2, 44) = 19.56, p < 0.001, and tension reduction behavior, F(2, 44) = 53.36, p < 0.001. Scheffè’s post hoc analysis revealed that the cancer group reported significantly higher scores than the control groups (JRA and healthy) for all scales: intrusive experiences (p < .001), defensive avoidance (p < .01), the dissociation (p < .001), and the tension reduction behavior (p < .001). Between control group comparisons showed no significant differences (p = n.s.). Detailed results of the TSI-A are shown in Figure 3(a) and Table 4 (see supplementary materials).
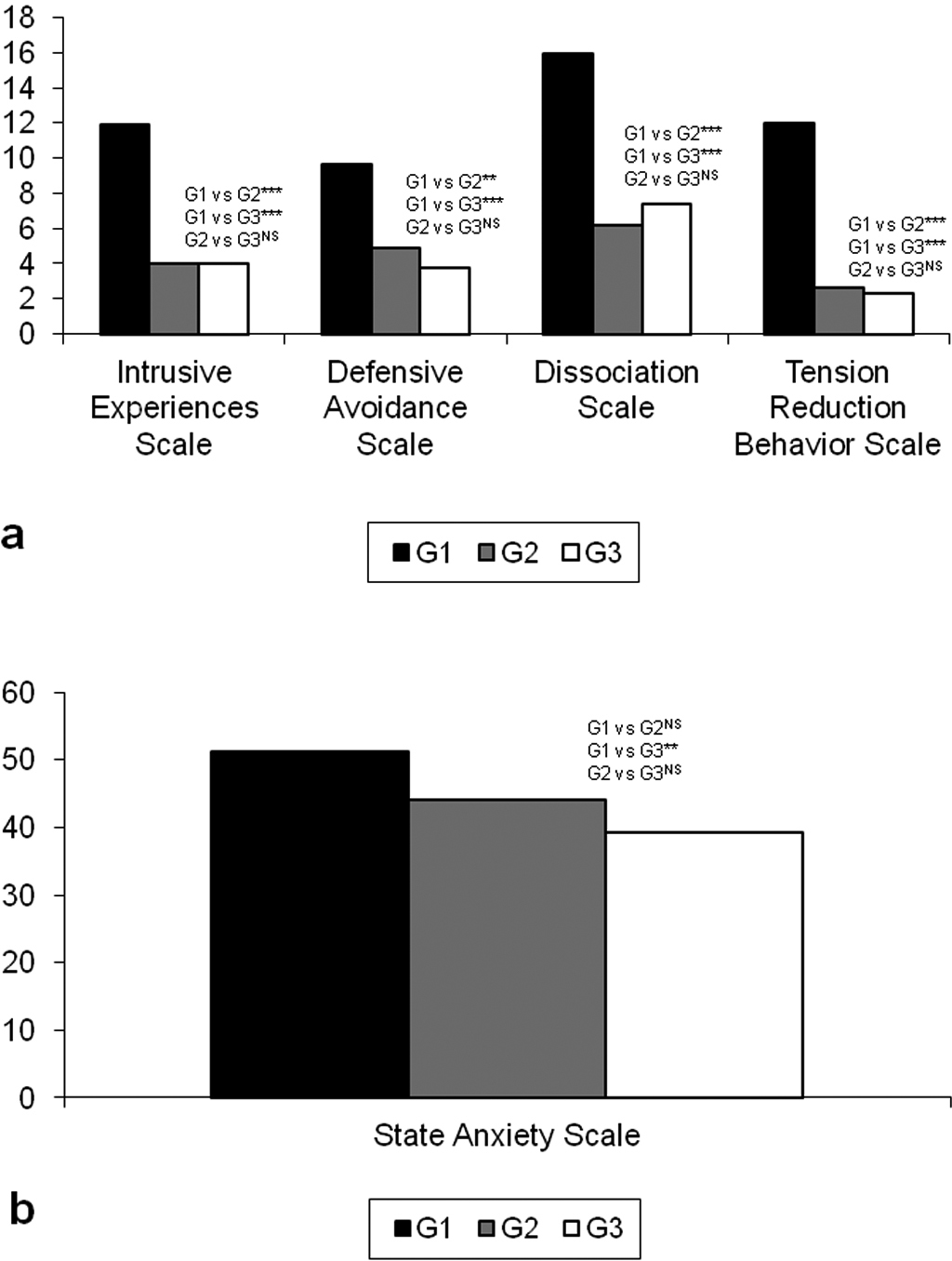
Panel (a) illustrates the scores of intrusive experiences, defensive avoidance, dissociation, tension reduction behavior scales assessed by TSI A. Panel (b) illustrates the scores of state anxiety scale assessed by STAI; *p < .05; **p < .01; ***p < .001; NS: not significant. G1: cancer group; G2: juvenile rheumatoid arthritis group; G3: healthy group; TSI A: Trauma Symptom Inventory A; STAI: State–Trait Anxiety Inventory.
State–Trait anxiety inventory
MANOVA showed statistical significance, F(20, 66) = 3.27; p < .001, for STAI between-group comparison. The univariate effects showed statistical significance in the State Anxiety scale, F(2, 44) = 3.70, p <.05. Scheffè’s post hoc analysis revealed that the cancer group did not report significantly higher scores than the JRA control group. However, significant differences were found in the cancer group with respect to the healthy control group (p < 0.01). Between control group comparisons showed no significant differences (p = n.s.). Detailed results of the STAI are shown in Figure 3(b) and Table 4 (see supplementary materials).
Discussion
This pilot study is useful in increasing the knowledge about the psychological functioning of children and their mothers living through a life- and non life-threatening chronic disease. Our investigation focused on the differences in psychological functioning between children with cancer, children with JRA, healthy children, and their mothers.
We found differences in the psychological functioning in the three groups of children. The 6- to -12-year-old children with cancer had more significant internalizing problems and attention problems with respect to healthy children but not to JRA children. Conversely, the two- to -five-year-old children with cancer did not show any significant problems compared to children with JRA and healthy children. However, children with JRA had statistically more problems, particularly externalizing problems, than children with cancer and healthy children. These results are consistent with previous literature highlighting developmental differences in distress response, that is, externalizing problems seem to be a distinctive aspect in younger children and internalizing problems seem to be a distinctive aspect in older children (Scheeringa, 2007). Therefore, it is important to identify phase-specific indicators in order to understand psychological functioning in children through a developmental perspective. Psychological functioning differences between younger and older children could be closely related to lower capacities of younger children to verbally describe internal states (Frigerio et al., 2006; Scheeringa, 2007, 2012). Low levels of emotional problems in younger children with cancer could also be explained by a ‘repressive adaptive style’ (Weinberger, 1990) characterized by high levels of adaptation, high levels of defensiveness (i.e. inhibition of negative affect to avoid threat to idealized self-concept), and reduced levels of anxiety. In fact, some studies assessing psychological symptoms in children with cancer compared with healthy reported no group differences in the levels of depressive symptoms, anxiety, posttraumatic stress, self-esteem, behavioral problems, and somatic distress (Erickson and Steiner, 2001; Phipps, 2007; Williams et al., 2011).
When considering life threatening, our results suggest that the threat to life impacts psychological functioning in younger children but not in older children. It is possible that in older children, the illness severity and the impact of the disease on the quality of life are more relevant than the threat to life. In fact, both cancer and JRA children are characterized by disability, reduction in quality of life, daily activity limitation, impairments in functioning, aggressive treatment, and pain. Future studies comparing childhood cancer, JRA, and other severe chronic diseases in different age ranges could explain these results.
Regarding the mother’s results, we found that mothers of children with cancer had higher levels of both PTSS and parental distress than mothers of children with JRA and mothers of healthy children. This result suggests that life threatening could be an important factor in psychological functioning and emotional and adaptive response in mothers of children with a chronic disease.
This study has some limitations. First, this is a pilot study with a small sample of subjects. Second, we did not consider the possible bias related to using self-report and report-form measures. In particular, the study relied on the mothers as a single informant. Follow-up studies using additional methodological approaches, including the use of multiple informants to assess both child and parent emotional functioning, are recommended. Third, we did not investigate the effect of other variables such as risk, protective, and vulnerability factors (e.g. life background, social support, etc.). Fourth, we did not consider a follow-up off-treatment assessment to monitor long-term psychological sequelae.
In conclusion, this pilot study confirms the importance to consider childhood cancer as a challenging and traumatic experience for patients and their mothers, focusing on psychological functioning and not only on PTSD. Therefore, this pilot study confirms that PTSD seems not to be a very informative model for understanding the responses of children with chronic disease and their mothers. Finally, the current pilot study highlights the importance of life threatening in psychological functioning response in children and their mothers living through a chronic disease.
Future work, including extension of sample size and other chronic disease as a control group, is needed to confirm and/or clarify our results. If confirmed, the results of this pilot study can open a new perspective in formulating family intervention to reduce distress and enhance well-being and/or psychological intervention, focusing on specific response to chronic diseases.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.