
Abstract
The aim of this study was to analyze the association between risk behaviors and adiposity indicators in adolescents and to discuss some methodological aspects related to this relationship. We evaluated 1,321 adolescents (55.2% female) aged 10–16 years. Relative body fat (%fat) by measurement of triceps and subscapular skinfold thickness and waist circumference (WC) were used as total and central adiposity indicators, respectively. Physical inactivity, time spent in front of the TV, the consumption of soda and/or chocolate, alcohol, and tobacco smoking were analyzed as risk behaviors. Information about the socioeconomic status (categorized into three levels) and nutritional status of the mother (overweight or normal weight) were used as adjustment factors in the analyses of prevalence ratio (PR) of the outcomes and their associated 95% confidence intervals (95% CI). The chi-square test and Poisson regression were used for statistical analyses. Low associations were found between risk behaviors and adiposity indicators. Tobacco smoking was the most positively correlated behavior with adiposity in girls (%fat: PR = 1.61; 95% CI = 1.04–2.47; WC: PR = 1.90; 95% CI = 1.17–3.08) and in adolescents whose mothers were normal weight (%fat: PR = 2.31; 95% CI = 1.33–4.03; WC: PR: 2.31; CI: 1.19–4.46). Additionally, as an important methodological issue, we highlighted the assessment of risk behaviors in adolescents as crucial to producing more robust evidence on the subject. Of the investigated behaviors, we concluded that tobacco smoking is the behavior most associated with adiposity indicators.
Introduction
Among the major public health problems in childhood and adolescence, excess body weight has received great attention in recent decades. This is due to the high prevalence of excess body weight observed in several countries and its negative health consequences (Ebbeling et al., 2002; Ludwig, 2007; Sikorski et al., 2012). To develop actions to improve this situation, studies have tried to identify the main determinants of excess weight in specific pediatric populations (Assunção et al., 2012).
Issues related to lifestyle and the adoption of risk behaviors at early ages, such as low levels of physical activity, a sedentary lifestyle, the consumption of foods with a high energy density and the use of licit and illicit drugs, have been proposed as causes for the current obesity epidemic (Currie et al., 2008). In Brazil, according to data from the National Survey of School Health (BIGS, 2012), which evaluated students in ninth grade, only 30% of them met their recommendations for physical activity, 79% spent more than two hours/day watching TV, 41% ate sweets regularly, 26% consumed alcohol, and 5% were tobacco smokers.
Although studies conducted in developed countries have indicated a causal effect between specific behaviors and adiposity (Boulos et al., 2012; Hancox et al., 2004; Neumark-Sztainer et al., 2012; Ortega et al., 2007), little evidence is available for middle- and low-income countries (Bozza et al., 2014). In order to bring about a discussion on the topic and highlight the problems of decision making based on weak evidence, we analyzed the association between risk behaviors and adiposity indicators in adolescents from Southern Brazil and discussed some methodological issues related to this relationship.
Methods
Sample
A school-based epidemiological study was conducted with 1,321 adolescents aged 10–16 years from public schools in the city of Londrina, in 2011. Located in the north of the state of Paraná, Brazil, Londrina has 515,707 inhabitants (28,822 school children in the age range of interest), a Human Development Index and gross domestic product of .824 and US$ 4,442,229.50, respectively (BIGS, 2013).
The process of sampling was carried out in two stages. All public schools in the city were listed by geographical region (north, south, east, west, and center), and two schools from each region were then randomly selected. Classes from the selected schools were then randomly ordered and five were chosen. All students who studied in the morning or afternoon periods were invited to participate in this study. Schoolchildren were excluded if they frequently used medication, which made their participation impossible, were under treatment for any illness, or who did not return the terms of consent duly signed by their parents or guardians. The sample size was calculated for expected prevalence of metabolic syndrome = 4%, α = .05, error = 2% points; design effect = 2.0, 20% + for losses/refusals. Initially, the sample was composed of 1,395 adolescents. Of these, 74 did not have complete data for the variables of interest. Thus, the final sample consisted of 1,321 adolescents (Table 1). All procedures in this investigation were approved by the Ethics Committee in Research of the Londrina State University.
General characteristics of the sample.

Note: CI: confidence interval; socioeconomic status: highest = A and B classes; middle = C2 class; lowest = C1, D, and E classes; WC: waist circumference.
Considering a statistical power of 80%, confidence interval (CI) of 95%, and the distribution of subjects in the categories of the independent variables, this sample size allowed us to identify prevalence ratios (PRs) of above 1.42 (risk)/.61 (protection), regardless of risk behavior or gender.
Dependent variables
The relative body fat (%fat) and waist circumference (WC) were adopted as indicators of total and central adiposity, respectively. For this, the thickness of the triceps and subscapular skinfolds was measured by an experienced evaluator using a compass of the Lange® brand, suitably calibrated (accuracy = .5 mm), following the recommendations of Harrison et al. (1988). For quality control, the technical error of measurement (TEM) was calculated from measurements duplicated in 90 adolescents (pilot project), who were not included in the sample of this study, but had similar characteristics with regard to age, race, somatic maturation and level of adiposity. The TEMs were 4.8% and 3.5% for subscapular and triceps skinfold thicknesses, respectively. From this information, the %fat was estimated using the equation proposed by Boileau et al. (1985) and the adolescents were categorized dichotomously according to the cutoff proposed by Williams et al. (1992). Additionally, the WC was measured by a single examiner using a metal tape measure of the Sanny® brand with a precision of one millimeter. The recommendations of Katzmarzyk (2004) were adopted both for the measurement itself and for the categorization of the values of WC (normal/high).
Independent variables
Physical inactivity, amount of time spent watching TV, consumption of sodas and/or chocolate, alcohol, and tobacco use were the risk behaviors for the adiposity indicators in this study. This information was obtained through questionnaires administered by an experienced evaluator and assisted by two assessors trained for this purpose. For quality control of the data, the instruments were reapplied (seven-days interval) to 10% of the sample for calculating the intraclass correlation coefficient (ICC, to continuous and ordinal variables) and κ coefficient (to dichotomous variables).
As an indicator of the level of physical activity, playing sports during leisure time was assessed using the questionnaire developed by Baecke et al. (1982) (ICC = .88). Adolescents who reported having engaged in sports activities of moderate to high intensity for at least 240 minutes/week during the previous four months were considered physically active (Fernandes et al., 2012).
The amount of time spent watching TV was calculated by summing the minutes spent during the weekdays and weekends (ICC = .77). Based on the daily weighted average, sedentary behavior was defined as more than four hours/day in front of the TV.
The consumption of sodas and/or chocolate was evaluated by means of one question (ICC = .76) concerning the frequency of consumption (no consumption, one to three days, four to six days, and seven days) during the previous week. The cutoff used for inadequate dietary pattern was the consumption of these foods on four or more days per week. Information about alcohol consumption (κ = .58) and tobacco smoking (κ = .64) was obtained in a dichotomous manner, by indicating frequent use (at least once a week) in the past 30 days.
Confounding variables
For statistical control, in addition to age and sex, socioeconomic status (SES) and the mother’s body mass index (BMImother) were evaluated, by means of a questionnaire filled by the parents or guardians.
While SES was evaluated using the instrument of the Brazilian Association of Research Companies (BARC, 2008), which allows stratification by eight categories (A1, A2, B1, B2, C1, C2, D, and E [lowest]), the BMImother was obtained through the request for self-reported body weight and stature.
Statistical analyses
The statistical sample power was estimated by Epi Info program, version 7. Distribution of relative frequencies and their respective 95% CI, according to sex, were used for the characterization of the sample. Chi-square test of independence was used to check the association between risk behaviors and adiposity indicators (bivariate analysis). Poisson regression was used with robust estimate of variance to obtain the adjusted PRs and their 95% CIs. This method has been used in order to not overestimate the effect measure mainly in high-prevalent outcomes (Barros and Hirakata, 2003). PRs were adjusted by chronological age and SES (stratified by gender analysis) and by chronological age, SES, and sex (stratified by BMImother). After bivariate analyses, independent variables were included in the adjusted multivariate model. All analyses used SPSS 17.0 with a p value below .05 for statistically significant associations.
Results
Crude associations between risk behaviors and adiposity indicators as well as the adjusted PRs (95% CI) are presented in Table 2. In boys, an association was only observed between physical inactivity and total adiposity, and those with insufficient physical activity presented a higher probability of total adiposity (% fat) compared to the more physically active (PR = 1.66, 95% CI: 1.10–2.50; p = .016). Among the girls, dietary pattern and tobacco use were associated with total adiposity. Compared to girls with an adequate diet, those with an inadequate diet were less likely to have higher total adiposity (PR = .76, 95% CI: .59–.98; p = .037). Smoking increased the probability of excess in both central adiposity (PR = 1.90, 95% CI: 1.17–3.08; p = .009) and total adiposity (PR = 1.61, 95% CI: 1.04–2.47; p = .032).
Association between risk behaviors and indicators of adiposity in adolescents.
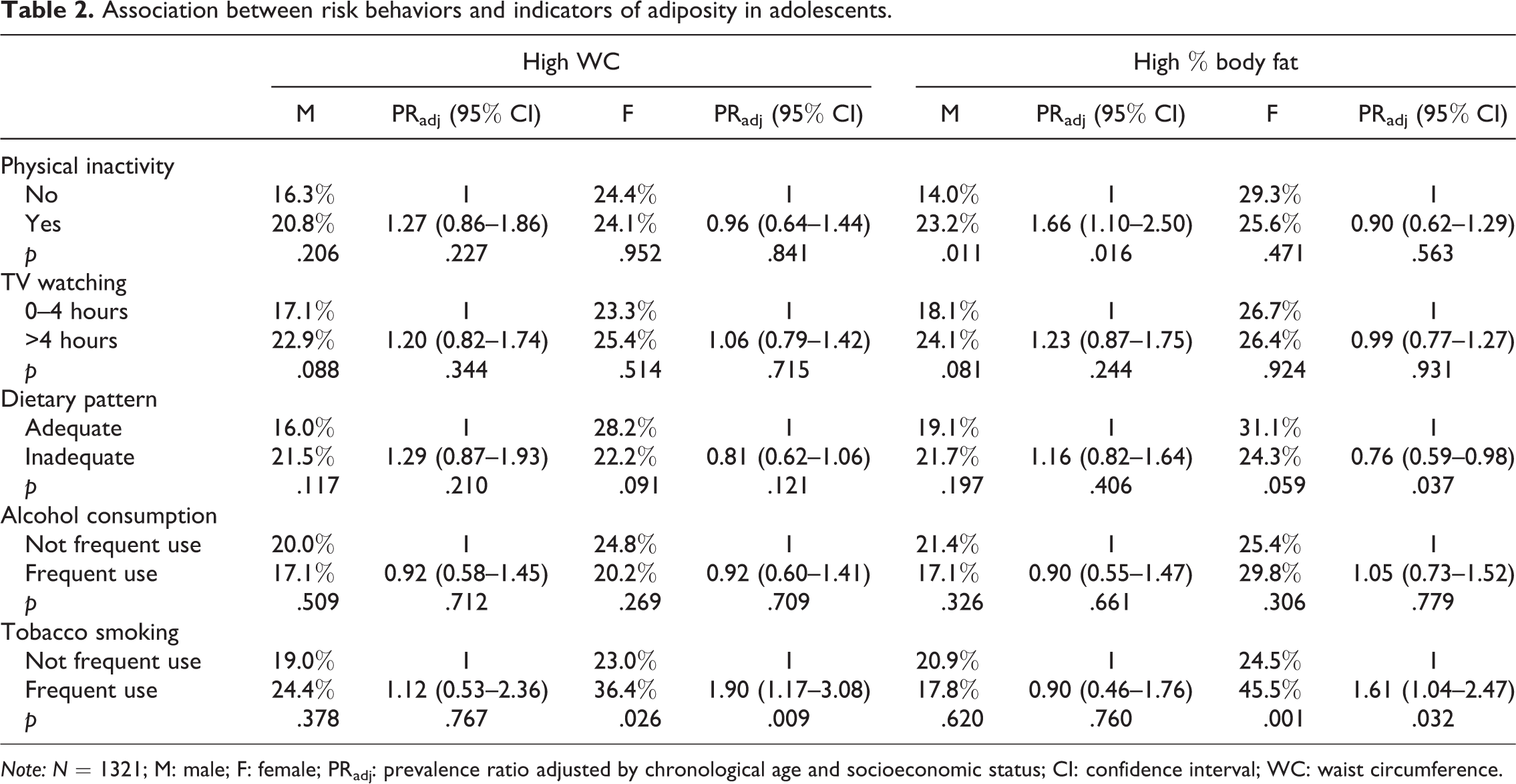
Note: N = 1321; M: male; F: female; PRadj: prevalence ratio adjusted by chronological age and socioeconomic status; CI: confidence interval; WC: waist circumference.
With stratification by BMImother (Table 3), only tobacco use was associated with adiposity indicators. In adolescents whose mothers were of normal weight (BMI < 25 kg/m2), higher central adiposity (PR = 2.31, 95% CI: 1.19–4.46; p = .013) and total adiposity (PR = 2.31, 95% CI: 1.33–4.03; p = .003) were observed among those who reported smoking regularly. However, regardless of sex, chronological age, and SES, adolescents of overweight mothers had a 1.67 (95% CI: 1.27–2.15) and 1.48 (95% CI: 1.15 – 1.88) higher probability of high central and total adiposity (p < .001), respectively, when compared with adolescents of normal weight mothers.
Association between risk behaviors and indicators of adiposity in adolescents according to the BMImother.

Note: N = 1321; BMImother: mother’s body mass index; PRadj: prevalence ratio adjusted by sex, chronological age and socioeconomic status; CI: confidence interval; WC: waist circumference.
Discussion
The main results of this study indicate weak associations between behavioral risk factors and adiposity indicators in adolescents from Southern Brazil when analyzed by sex and BMImother. It is important to highlight that these associations seem to be different to some extent between the sexes and mother’s BMI category. The only behavioral risk factor positively associated with both the adiposity outcomes was tobacco use in girls and adolescents whose BMImother < 25 kg/m2.
Our findings do not corroborate many other studies, especially those that endorse recommendations for the prevention and treatment of obesity (Barlow, 2007; Davis et al., 2007; Spear et al., 2007). To consensually establish causality between behaviors and biological outcomes in young people (short term), some factors should be considered, such as, the experimental design, the method for obtaining the variables, the characteristics of the population and the duration, intensity and frequency of the behaviors.
In this sense, the cross-sectional design adopted in this study is a limitation. Although it is useful to detect disease frequencies and risk factors, as well as to identify population groups that are more affected, this approach does not allow the establishment of temporality between variables. However, short term longitudinal designs should not be encouraged since a large part of the morbidities attributed to lifestyle have a long latency period. Therefore, in order to discuss reverse causality, a characteristic of cross-sectional designs, the stratified analysis of BMImother was performed, hypothesizing that adolescents whose mothers are overweight are more prone to the effects of reverse causality.
The method for obtaining measurements is the second limitation of this study. Information about lifestyle, mainly in middle and low-income countries has been obtained predominantly using questionnaires (Farias Júnior et al., 2010; Hallal et al., 2007). However, particularly in adolescents, data collected from questionnaires should be viewed with caution since many behaviors are susceptible to social approval. In this case, questionnaires were used in the school environment where the presence of peers or uncertainty about the confidentiality of the information to their parents may affect the reporting of the data (Brener et al., 2003). Although we took care of the reproducibility of the questionnaires’ results, the absence of a gold standard method to measure physical activity does not allow us to control the validity. However, it is worth highlighting the methodological care adopted, such as sample selection, quality control of the measures, and statistical power of the analyses, as strengths of this study.
Based on the analyses, we believe that the associations found between physical inactivity, sedentary behavior, and alcohol consumption with adiposity (central and total) did not suffer the effect of reverse causality since no result was significant in the stratified analysis with BMImother. Regarding eating habits, the results seem to be more influenced by sex (girls may have reported their habits distortedly) than mother’s nutritional status (no significant association). The association between adiposity and tobacco use, less reported in the literature and even an inverse determination product, positively observed in girls, remained even in the adolescents whose mothers had BMI < 25 kg/m2. This indicates that, among children whose mothers are overweight, tobacco use was found to have no relationship with adiposity indicators. In this instance, we concluded that the measurement collection may have more influence than the reverse causality.
Others studies conducted in Brazil have also not observed associations between risk behaviors and adiposity indicators in adolescents (Moraes and Falcao, 2013; Silva et al., 2011), corroborating our findings. Further investigations, unpublished because they do not show positive associations, should also be considered. Therefore, we highlight the importance of discussing the methodological problems inherent in cross-sectional designs, in the sense of looking carefully at the observed results and trying to overcome the problems.
A relevant point relates to the detailed characteristics of the selected behaviors, such as the intensity, duration, and frequency of the habit or combinations thereof. Studies have suggested that the relationship between specific behaviors and negative outcomes depends on how this behavior is conducted (Ambrosini et al., 2012; Byun et al., 2012; Ortega et al., 2007) and their combination may soften/potentiate the health risk outcomes (Chaput et al., 2012; Rey-Lopez et al., 2012). Thus, the consideration of habits in isolation may not reflect the true position, creating biased conclusions and negatively influencing the practical applications of the results for public policies.
Finally, we conclude that, among the risk behaviors investigated in this study (physical inactivity, sedentary behavior, inadequate dietary pattern, alcohol, and tobacco use), the latter is the behavior most associated with adiposity indicators in adolescents from Southern Brazil. Based on the foregoing discussion, in studies of this nature, the authors reinforce the need to advance methodological aspects, mainly with regard to research design, methods of measuring behaviors detailed, and grouped analyses of adolescents’ behavioral risks.
Footnotes
Acknowledgments
The authors thank Décio Barbosa, Danielle Venturini, Alessandra Okino, and Jair Oliveira for research support, Mariana Carnelossi and Sandra Kawaguti for acquisition of data, Coordination for the Improvement of Higher Education Personnel (CAPES, Brazil) for scholarships (DRPS, CMT, MBB), and National Council of Scientific and Technological Development (CNPq/Brazil) for funding the project and for scholarship productive research (ERVR and ESC).
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support by National Council of Scientific and Technological Development (CNPq/Brazil) for the research. No financial support was received for authorship and/or publication of this article.