
Abstract
Bronchiolitis is the leading cause of morbidity and hospitalization in infants under the age of one year. Supportive treatments and regular assessment remain the mainstay of care for infants admitted to hospital. Nurses play an important role in the assessment of infants with bronchiolitis; however, this is not well described in the literature and consequently little is known about what strategies nurses employ in assessing infants with bronchiolitis. The aim of this study was to explore bronchiolitis assessment in the context of nursing practice. A naturalistic inquiry study was undertaken using think aloud and retrospective probing data collection methods. The results revealed that the information gathered by nurses in their assessment of infants with bronchiolitis was varied and the process of acquiring and evaluating this information was multifaceted and holistic in nature. A close partnership between the nurse and mother was identified, and the mother’s expert knowledge and ability to identify subtle changes in the infant’s clinical condition over time was essential to the assessment process. The assessment partnership with families provides nurses with the most comprehensive and holistic view of the infant’s clinical condition and vital assessment information could be lost if this partnership does not occur.
Introduction
Bronchiolitis, an obstructive lower airway disease of infancy, is the most common cause of hospitalization and the leading cause of morbidity in infants under the age of one year (Shay et al., 1999; Stockman, 2012). Annual hospitalization rates for respiratory syncytial virus associated acute respiratory infections are up to 42.7/1000 children in the first year of life (Bont et al., 2016), with reported substantial increases in admission rates over the last five years (Green et al., 2016).
Many clinical trials have been conducted to evaluate treatments for bronchiolitis and these have been reported in various systematic reviews (Beggs et al., 2014; Enriquez et al., 2012; Farley et al., 2014; Fernandes et al., 2013; Gadomski and Scribani, 2014; Hartling et al., 2011; Liet et al., 2015; Roqué i Figuls et al., 2016; Umoren et al., 2011; Zhang et al., 2013); however, supportive care, along with close and regular nursing assessment, remains the foundations for managing hospitalized infants.
Nursing assessment is a dynamic process that enables the planning of care to be responsive to the patient’s needs and is central to quality and patient safety. Despite strong correlation with in-hospital mortality (Rothman et al., 2012), nursing assessment is poorly defined (Beckwith et al., 2010). While a better articulation of the process is essential, the reality of unpacking tacit knowledge to expose what is seen as intuitive to nursing has not been realized.
The aim of this study was to explore the processes and parameters nurses use to assess infants with bronchiolitis in clinical practice and to answer the following questions:
What kinds of information do nurses gather in order to undertake their assessment of infants with bronchiolitis? How is this information acquired and evaluated in the context of the nursing assessment of infants with bronchiolitis?
Method
Study design and participants
Naturalistic inquiry is a qualitative research methodology underpinned by constructivist beliefs (Lincoln and Guba, 1985). As the study was conducted in the clinical setting, naturalistic inquiry allowed for a holistic approach to investigate the complexity of nursing assessment of infants with bronchiolitis, which combines induction, deduction and analytical reasoning skills.
A purposive sample of 10 registered nurses working in a paediatric ward of a large public metropolitan hospital in New South Wales, Australia, was selected. Participant inclusion criteria include a minimum of three years’ paediatric experience or award of a postgraduate paediatric qualification with at least 12 months’ paediatric experience.
Data collection
After gaining consent from accompanying parents, participants were observed undertaking assessments of infants with bronchiolitis. Data were collected over a period of six months during bronchiolitis season 2011. Concurrent verbal protocol or ‘think aloud’ and retrospective probing were used as data collection methods. Think aloud is a process that links thinking with concurrent perceptions, thus revealing information available to the working memory (Lundgren-Laine and Salantera, 2010), and provides a sequential record of the participant’s thinking and behaviour while completing a specific task (Bucknall and Aitken, 2010). Retrospective probing provides further insight into the assessment process and helps to understand how nurses use information from their assessment of bronchiolitis to make practical decisions about supportive care (Bucknall and Aitken, 2010).
Participants wore a lapel microphone attached to a digital recorder during the period of assessment of an infant with bronchiolitis. Field notes were also taken by the researcher for the purpose of contextualizing the think aloud data. Following the think aloud sessions, the audio data was immediately transcribed and questions for retrospective probing formulated. Each of the participants was interviewed within 24 hours of data collection.
Ethical considerations
Ethics approval was sought and obtained through the Human Research Ethics Committees of the Local Health District (1008-293M). Informed consent was sought from the participants and from the parents of those infants who were assessed during the study, following provision of verbal and written information. Participants and parents were advised of their right to withdraw from the study at any time.
Data analysis
Think aloud data, field notes and data from retrospective probing were sorted and categorized using NVivo™ software (version 9; QSR International Pty Ltd, Melbourne). A summative content analysis of the data was undertaken (Hsieh and Shannon, 2005) in order to answer the research question ‘what kinds of information do nurses gather in order to undertake their assessment of infants with bronchiolitis?’ A thematic analysis was conducted according to the method described by Elo and Kyngäs (2008) and concepts were assigned to each identified segment in order to identify and report patterns (themes) in the think aloud data. Data were analysed using a constant comparison method (Lincoln and Guba, 1985). This involved comparing segments in order to identify similarities, differences and emerging themes. The thematic analysis aimed at answering the research question ‘how is information acquired and evaluated in the context of the nursing assessment of infants with bronchiolitis?’
Rigour
The rigour of a naturalistic inquiry study relies upon the concept of data trustworthiness and incorporates criteria such as credibility, dependability and confirmability (Lincoln and Guba, 1985). Prolonged engagement and member checks were used as techniques to establish credibility (Lincoln and Guba, 1985). In contrast to quantitative research, where separation is sought to maintain objectivity, naturalistic inquiry sees the researcher and participants as being inseparable and advocates the researcher being an accepted member of a group in order to gain the participants’ trust (prolonged engagement). The researcher had an existing working relationship with the participants and this was seen as being essential to the research process. Each participants was given a copy of the transcribed data, including researcher field notes, to read and confirm as a true representation of their think aloud session (member checks). Dependability was addressed in this study with an inquiry audit where external reviewers acted as ‘inquiry auditors’, scrutinizing the research process throughout (Lincoln and Guba, 1985). A decision trail involving systematic recording of data, process and decisions made at each stage of the study was recorded throughout to establish confirmability (Erlandson et al., 1993).
Findings
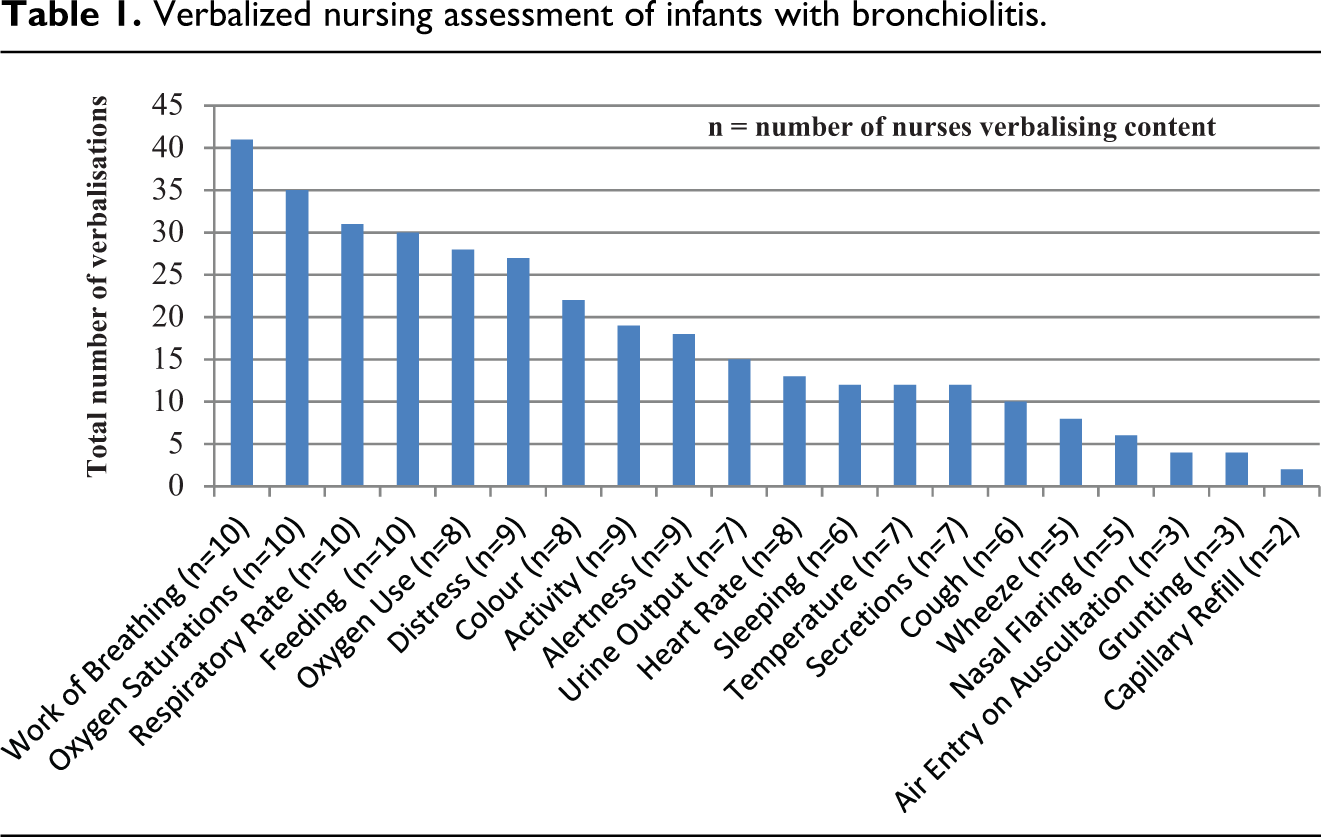
Ten nurses undertook the assessment of 10 infants with bronchiolitis. Infants were aged between 10 days and 12 months and attending parents were all mothers. Through summative analysis, the frequency and the types of assessment information verbalized by the participants were identified (Table 1). In total, 20 separate clinical assessment skills were verbalized. Work of breathing (including chest recession, tracheal tug and head bobbing), oxygen saturation, respiratory rate, and feeding were referred to by all 10 participants. Information on general appearance, including the assessment of distress, colour, activity and alertness, was also frequently verbalized.
Verbalized nursing assessment of infants with bronchiolitis.
Through inductive content analysis, three key themes were identified: understanding the impact of illness, digging deeper and contextual decision-making. The overall complexity and holistic nature of the nursing assessments is conceptualized in the framework shown in Figure 1.
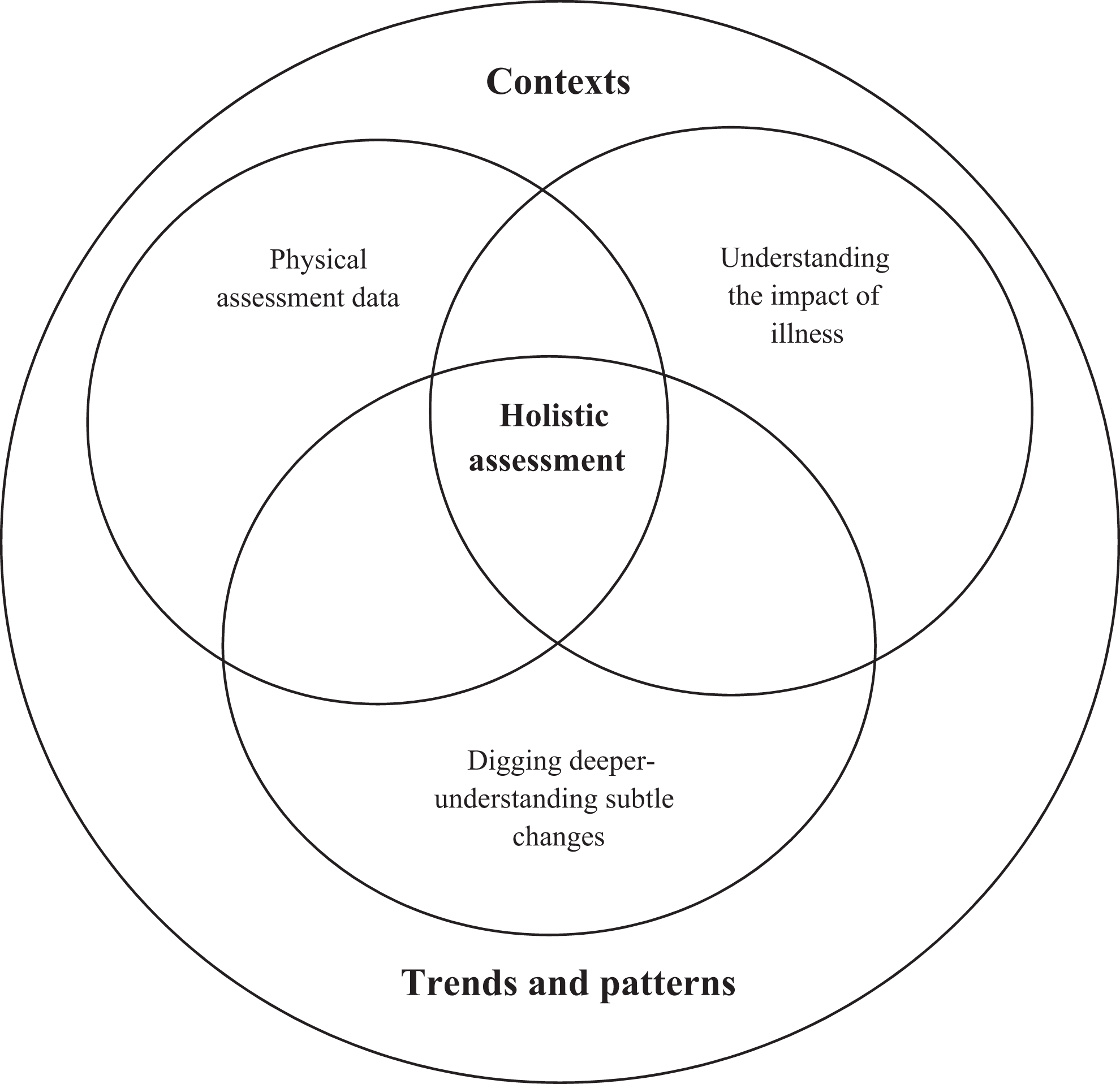
Key themes in the nursing assessment of infants with bronchiolitis.
Understanding the impact of illness
Although physical assessment information was seen as important, participants also sought information to help them understand the impact of the illness on the infant through eliciting the mother’s knowledge. For example, one participant asked ‘How long has he been unwell, mum?…And do you think he is getting better? Is he better today?’ (Nurse B). Participants commonly expressed the need to obtain information from parents even in their absence, for example: I’d ask mum how he was sleeping, if he was sleeping well, if he’s coughing…so yeah, I’d be asking if he’s coughing, whether he’s getting good periods of settled sleep, if he’s more settle being upright or if he’s comfortable lying down.…I’d ask her about his oral intake, is he tolerating his fluids and if he’s had any vomiting post feeds or if he’s finding it hard to feed. (Nurse G)
Impact of the illness on feeding, elimination and sleeping was a key focus of discussion with mothers. In addition to seeking to understand the infant’s illness experience through the mother’s description, the nurses used listening and observation to understand the level of distress experienced by the infants themselves. Distress was identified as the infant’s way of communicating that something was wrong. For example: …but if he’s irritable, not happy it could be a sign that something is wrong, because he can’t tell us that. (Nurse A)
Conversely, the terms ‘happy’ and ‘settled’ were used to describe a settled infant which suggested an improvement in the infant’s clinical condition: …and she’s nice and settled which is considerably better than she was a few days ago when she was very unsettled…she looks lovely. (Nurse F)
In addition to assessing the clinical condition of the infant, nurses extended their assessment to the mother. Assessing the mother’s physical and emotional well-being was described as a barometer of the infant’s clinical condition. One nurse asked ‘So how are you mum? Did you get a good night’s sleep last night?’ and explained later: Well, if mum has had a bad night then the baby has had a bad night, you know? Yeah, yeah.…If mum looks shattered I know she’s been up all night with a sick baby. (Nurse B)
Digging deeper – Identifying subtle changes
The expertise of mothers in assessing their own babies and identifying subtle clinical changes was highly valued by nurses who used this expert knowledge to inform their clinical assessments. The mothers’ intimate knowledge of the infant’s normal behaviour meant that she was more likely to be able to detect subtle changes in clinical condition that might have gone unnoticed by the nurse. As such, the mother’s judgment as to whether the baby was returning to normal patterns and behaviours was commonly sought. Normal patterns related to specific behaviours such as feeding and sleeping, but also encompassed other aspects of behaviour, such as the infant’s general disposition, and was described as the infant ‘getting back to his normal self’.
Mothers were asked about subtle changes regarding their infant’s alertness and responsiveness that perhaps would not have been picked up by the nurse’s observations of these particular signs: She’s alert and responsive to you isn’t she?…looking at the light and…yeah I think she looks great. Good…yes, you said that last night that you noticed that she was a bit more awake. (Nurse F)
By seeking this information, subtle changes in the infant’s condition that may be non-specific, and perhaps not easily picked up by traditional physical assessment, were identified.
Contextual decision-making
After obtaining all of this information (physical signs, clinical observations and the mother’s assessment of their infant), the participants attempted to make contextual sense of it.
Physical information was assessed in the context of expected normal appearance and behaviour relative to the infant’s age and developmental stage, as well as individual norms. Age-related norms were particularly important when it came to assessing respiratory rate and levels of alertness including interest in their surroundings and appropriate interactions. Physical assessment information was rarely considered in isolation but often in the context of other clinical information, such as oxygen saturation recordings and the amount of oxygen being delivered. Assessments of work of breathing and respiratory rates were also often made in the context of the amount of oxygen being delivered. One participant explained: …what time did they turn it [oxygen] off then?…went into room air at 10.30…OK.…Her breathing is probably a little bit faster than it has been but that’s purely because she has to compensate [for not having oxygen on]. (Nurse F)
Others recognizing that a recording of low saturations was not the only indication that oxygen therapy may be required: …so, sometimes the saturations will be OK but they are working hard you know? So that might mean they are compensating…they are working hard but being able to maintain their saturations. So, we might need to give them some oxygen to settle them, give them a hand. Otherwise they are going to get tired. (Nurse A)
Participants also sought to understand physical assessment information in the context of the infant’s general appearance: And you’ve got a little bit of effort there I can see going on, but he’s quite happy with it.…And because he is quite alert and reactive I’m not majorly concerned about him…I don’t think he is acutely unwell. (Nurse D)
Limitations
A purposive sample of 10 registered nurses was recruited to this study. This number was based on data saturation being achieved in similar sample sizes of other studies using this methodology. Data saturation was believed to have been achieved in this study, as constant comparison was used during data analysis and no new themes emerged. However, it is recognized that a larger sample may have produced additional findings.
The participants, when asked about the researcher’s presence during retrospective probing, said that they ‘quickly forgot about them being there’; however, the authors recognize that the effect of an observer in the room may, in some cases, alter the verbalizations of the participants.
Discussion
Careful monitoring of clinical status is seen as key in the management and care of infants hospitalized with bronchiolitis (Zentz, 2011), but there is little written about how this is undertaken and what this information comprises of. This study is the first to describe how nurses assess infants with bronchiolitis.
A variety of information was used to inform the assessment, demonstrating a complex and holistic process that extended beyond pure physical assessment and incorporated an important partnership with parents. These findings are in contrast to previous suggestions that the nursing assessment of infants and children concentrates heavily on the collection of quantitative data (Broom, 2007).
In this study, nursing assessments of infants were holistic in nature and relied upon the collection of both quantitative and qualitative data. Nurses sought to understand the impact of bronchiolitis on the infants by collecting information about feeding and sleeping. This suggests that the recognition of severity of illness is not purely defined through the measurement of clinical signs but also through the effects of the illness on the infant’s ability to function and the burden that the illness places upon the infant’s life.
An important element of the assessments was the nurses attempt to hear the infant’s voice and this was done in two ways. Behaviours such as inconsolability were identified as the infant’s way of communicating that something was wrong. Information regarding the impact of illness – particularly feeding and sleeping – was obtained from mothers. In this way, the nurse participants sought to hear the infant’s voice to understand the impact of the illness using the mother as a ‘proxy’ for the infant. Using parents as a proxy is important in the assessment of an unwell child, as they are recognized as the most knowledgeable about the child’s normal behaviours, temperament and routine activities (Reid et al., 1995).
Nurse’s attempts to identify subtle changes in the infant’s condition, particularly by accessing mother’s knowledge of her infant’s normal behaviour, were a key finding in this study. Although trends in vital signs are recognized as important in detecting deteriorating patients (Churpek et al., 2016), the subtlety of changes in normal behaviour may render them as unrecognizable signs or symptoms by healthcare professionals and consequently could be regarded as insignificant when considering normal variation in standard assessment measures. These subtle changes identified by parents are often based on feelings that the child is ‘not quite right’. The identification of subtle changes requires repeated assessment over a period of time by the same person who knows the patient well; it is suggested that such an approach may be more important in identifying deterioration or improvement than routine physical assessments (Zambas, 2010). The importance of recognizing subtle changes and the role that families can play in this assessment process is starting to be recognized by health professionals and the organizations in which they work. Studies into patient- and family-activated emergency response calls have shown how family members’ recognition of subtle changes in a patient’s condition can be useful in detecting early deterioration in patients and, when incorporated into emergency response systems, result in improved mortality rates (Gerdik et al., 2010), although there seems to be some apprehension from staff in regard to these systems and the implementation of parent-activated response systems is not well reported (Gill et al., 2016).
The concept of using expert maternal knowledge is not new to paediatric health professionals who, for many years, have recognized that ‘the ability to judge what is normal or abnormal for their own child is a skill which parents alone possess’ (Callery, 1997). Although previous studies have suggested the power imbalance between health professionals and mothers results in maternal knowledge not being given as much importance as professional knowledge (Callery, 1997), significant importance was placed on accessing the mother’s knowledge and incorporating it into the nursing assessments in this study. An assessment partnership with parents and families provides nurses with what appears to be the most comprehensive and holistic view of the infant’s clinical condition. Indeed, it seems that vital assessment information could be lost if this partnership does not occur.
Conclusion
The findings of this study indicate that rather than purely collecting physiological data, nursing assessment of infants with bronchiolitis is multifaceted, complex and holistic in nature. Nurses routinely include the observation of behavioural cues in their assessments and include changes in feeding patterns, distress, alertness and activity. It is essential that the importance of this behavioural information in assessing illness severity is recognized and valued. Documentation of assessments should be inclusive of these behavioural cues and be organized such that a longitudinal view can be collected and compared across the trajectory of the illness. This information should be sought from parents or caregivers who are uniquely placed to relay normal patterns of behaviour and health state for their infant. Failure to do so may result in vital assessment information being lost.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Royal North Shore Hospital Nursing and Midwifery Scholarship fund and in particular the generous donation from the Skipper family.