
Abstract
This study aimed to explore the perspectives and experiences of parents caring for an infant with posterior urethral valves (PUVs). Eight parents participated in a semi-structured, individual telephone interview, with qualitative data collected and analysed thematically using NVivo11 software. Two main themes emerged as interconnecting aspects of parents’ experiences: (1) trying to face the challenges and (2) learning to cope. Parents felt challenged by the need to attend to their child’s medical care, while developing a bond with their baby, trying to maintain positivity for their child’s future and managing the impact of the condition on their family. Nevertheless, parents developed strategies to cope with these challenges, such as seeking support, normalizing the experience and focusing on the positives. This preliminary understanding of parents’ experiences provides direction for improving care pathways for infants with PUV and their parents as well as guides further research in this previously unexplored area.
Keywords
Introduction
Diagnosis of a baby with a congenital anomaly can be deeply distressing for parents, who are then often required to attend to their child’s medical needs. While research has described parents’ experiences of raising an infant or child with a congenital anomaly (Marokakis et al., 2016a), very few studies have focused on the experiences of parents of infants with renal disease. A small number of studies have examined the experiences of parents of children with chronic kidney disease (CKD); however, these studies included parents of children with varying causes of CKD, as well as parents of children with markedly impaired glomerular filtration rate, and thus may not reflect the specific experiences of parent of children with congenital anomalies of the kidney and urinary tract (Tong et al., 2010; Wiedebusch et al., 2010). A systematic review by Aldridge (2008) found parents of children with CKD commonly reported increased levels of stress, anxiety and depression compared to parents of healthy children. However, these studies, predominately included parents of school-age children with advanced CKD, therefore, do not provide insight into the potentially unique experiences of parents of infants with a congenital anomaly of the kidney and urinary tract (CAKUT).
Posterior urethral valves (PUVs) is a congenital anomaly of the male urinary tract affecting approximately 1 in 8000 live births (Thakkar et al., 2014). Boys with PUV may experience significant complications requiring ongoing treatment, such as bladder dysfunction, recurrent urinary tract infections (UTIs) and CKD leading to renal failure (Caione and Nappo, 2011; Heikkila et al., 2011; Holmdahl and Sillen, 2005). Clinical management of PUV involves strategies to address any renal impairment and bladder dysfunction. Management of renal impairment includes drug therapy, dietary interventions and, in severe cases, dialysis or kidney transplantation. Surgery is required to ablate urethral valves which can improve urinary flow and reduce the risks of infections and kidney dysfunction. At times, further surgery is undertaken to improve urinary flow. Bladder dysfunction may respond to medication and bladder training; however, boys with severe PUV-related bladder dysfunction may not be able to fully empty their bladder and are often managed by clean intermittent catheterization (CIC). CIC entails penile catheterization several times each day. Parents are taught to do CIC until the boys are old enough to learn themselves.
There is little in the peer-reviewed literature about the impact of PUV on health-related quality of life (QOL) for affected children or their families. Adults with PUV were reported to have reduced QOL, particularly if they had renal impairment or urinary incontinence (Jalkanen et al., 2013). Boys aged 6–16 years with PUV who perform CIC described a feeling that CIC can become an obstacle to ‘normal’ living and may cause anxiety and uncertainty during peer interaction (Hellstrom et al., 2006). In an earlier study, self-reported QOL scores in children undergoing CIC (including a small number of boys with PUV) were comparable to QOL scores in typically developing children; however, parent-proxy QOL scores were lower than scores reported by parents of typically developing children (Alpert et al., 2005). To the best of our knowledge, the experiences and perspectives of parents of infant boys with PUV have not been explored, and the potential impact of the complications and treatments associated with PUV on parents is relatively unknown. Thus, this qualitative study aimed to explore parents’ perspectives and experiences in the context of caring for an infant with PUV.
Methods
Participants and recruitment strategy
The study was carried out during 2015. Parents of a child born with PUV between 2012 and 2015 were invited to participate. Potential participants were identified from patient databases at a single children’s hospital in Sydney, Australia. Eligible individuals were sent an invitation letter, information sheet, consent form and reply paid envelope. Parents who provided written consent were contacted to arrange a telephone interview. Non-responders were sent a follow-up letter. Individuals who did not respond to this letter were deemed to have declined participation and follow-up ceased. The study was approved by the institutional human research ethics committee (approval: LNR/15/SCHN/173).
Data collection
Consenting parents took part in one individual, semi-structured telephone interview. Each parent was interviewed separately to allow open discussion and expression of individual experiences and viewpoints. Participants were offered telephone interviews for convenience and to maximize the likelihood of study participation. An interview guide consisting open-ended questions was developed to encourage discussion of the following topics: parents’ experiences of their child’s diagnosis, birth and postnatal care; experiences of raising a child with PUV; perceptions of the parent–child relationship; and perceptions of their child’s current physical and emotional well-being. The study was conducted alongside a research protocol investigating parental experiences of antenatal counselling for CAKUT, and the present article focuses on parental experiences from the time of their son’s birth to the time of interview. Interviews were recorded and transcribed verbatim. Details of medical management, including previous surgeries, hospitalizations, UTIs, drug therapy and whether parents were performing CIC, were extracted from patient records. Current renal status was ascertained by collecting the most recent serum creatinine measure.
Data analysis
Qualitative data analysis was informed by the framework of Miles et al. (2014) and involved (1) reading and summarizing the interview transcripts and noting salient themes, (2) first-cycle coding of interview content using codes developed from the noted themes using QSR NVivo11 software, (3) second-cycle coding drawing connections between codes, (4) using visual data displays to synthesize findings and observe patterns in the data and (5) creating themes and subcategories from the synthesized data. Coding and analysis were led by one researcher, with coding reviewed by all investigators. Data derived from medical records were analysed using descriptive statistics and the IBM Statistical Package for the Social Sciences 22.0.
Results
Participant and child characteristics
Eighteen parents of nine boys with PUV were invited to participate (see Figure 1). Eight parents (50% fathers) of four children consented and participated in the telephone interview (response rate: 44%). The sample comprised three couples with a child born with PUV and one couple with a child born with an anterior urethral diverticulum (Adam et al., 2015). The mean age of the children at the time of interview was 26 ± 4.2 months (range: 22–32 months), and the mean interview length was 56.6 ± 15 minutes.
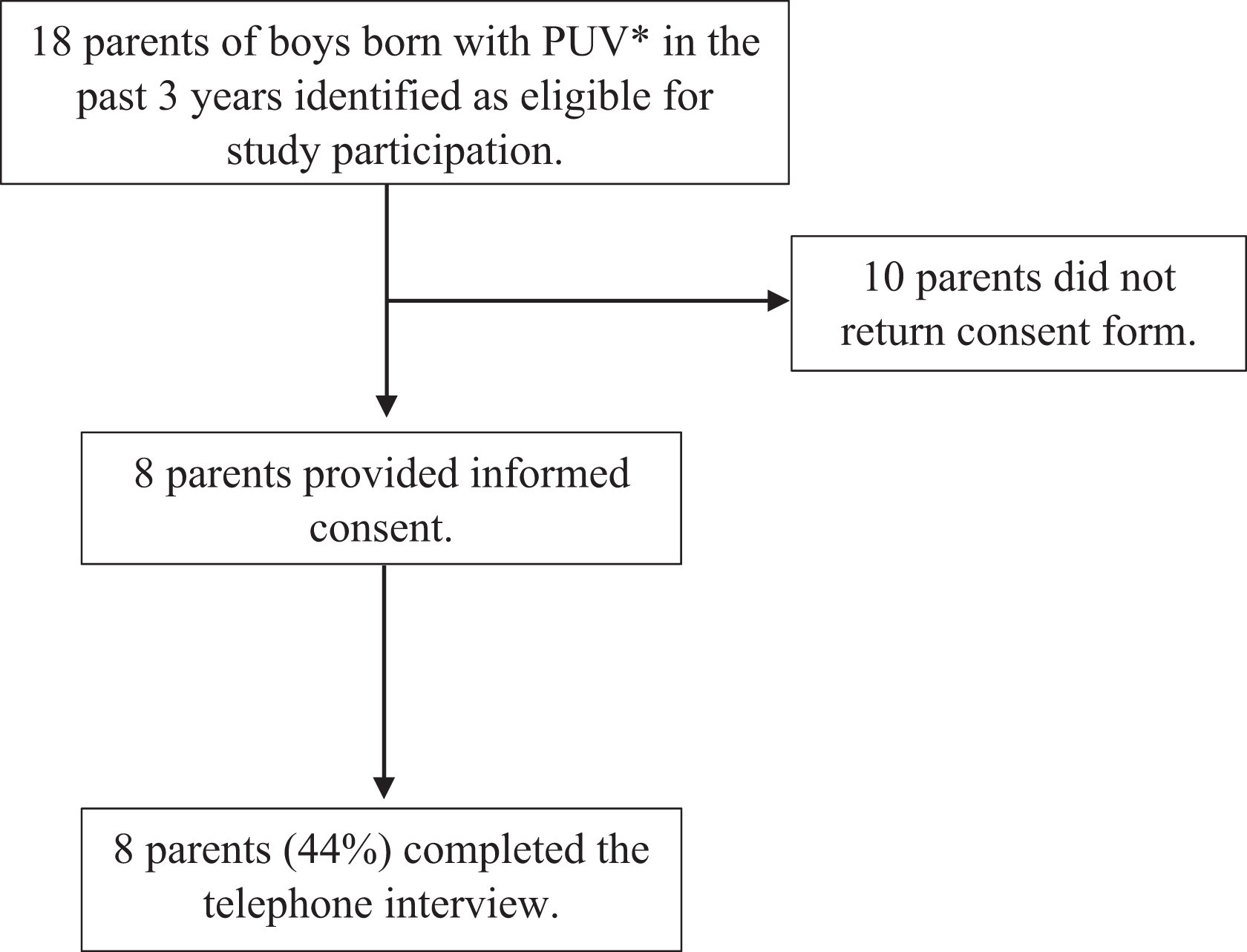
Flowchart summarizing study recruitment and participant response rate. *One boy with anterior urethral diverticulum.
All parents were first informed of their child’s condition during pregnancy following ultrasound screening. All babies were born at full term (range: 37–39 weeks gestation) by vaginal (n = 2) or caesarean delivery (n = 2). All babies required admission into the neonatal intensive care unit (NICU).
The clinical status of the children at the time of interview is shown in Table 1. One child had advanced CKD and the others had relatively normal plasma creatinine. All children had undergone more than one surgical procedure. Three boys had been managed with urinary diversion, one with bilateral pyelostomies and two with vesicostomies. CIC had been commenced in the two boys whose diversions were closed. The child with anterior urethral diverticulum had a vesicostomy at time of interview. The fourth child had mild manifestations, with normal renal function, no UTIs and no significant voiding difficulties.
Clinical characteristics of children at time of interview.
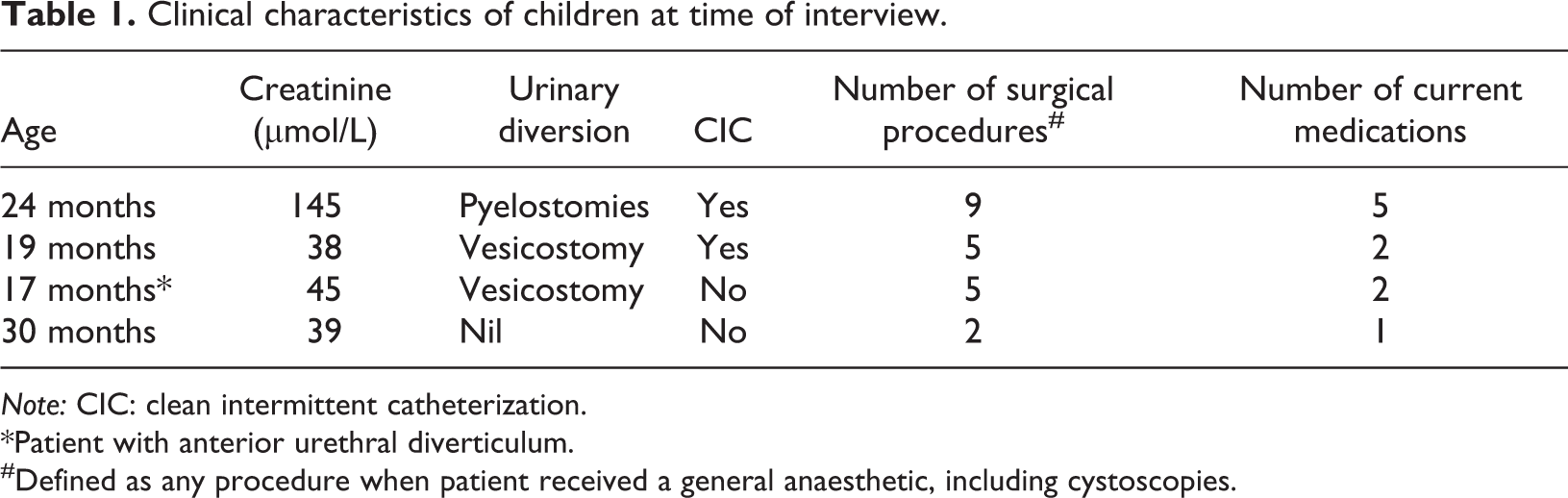
Note: CIC: clean intermittent catheterization.
*Patient with anterior urethral diverticulum.
#Defined as any procedure when patient received a general anaesthetic, including cystoscopies.
All parents reported their child to have ongoing health issues and/or treatment related to the anomaly. Two children had experienced recurrent UTIs. All children were on regular medication and attended regular check-ups.
Parenting experiences
Participants’ experiences of parenting a child with PUV were classified into two main themes, trying to face the challenges and learning to cope, each comprising several subcategories (see Figure 2).
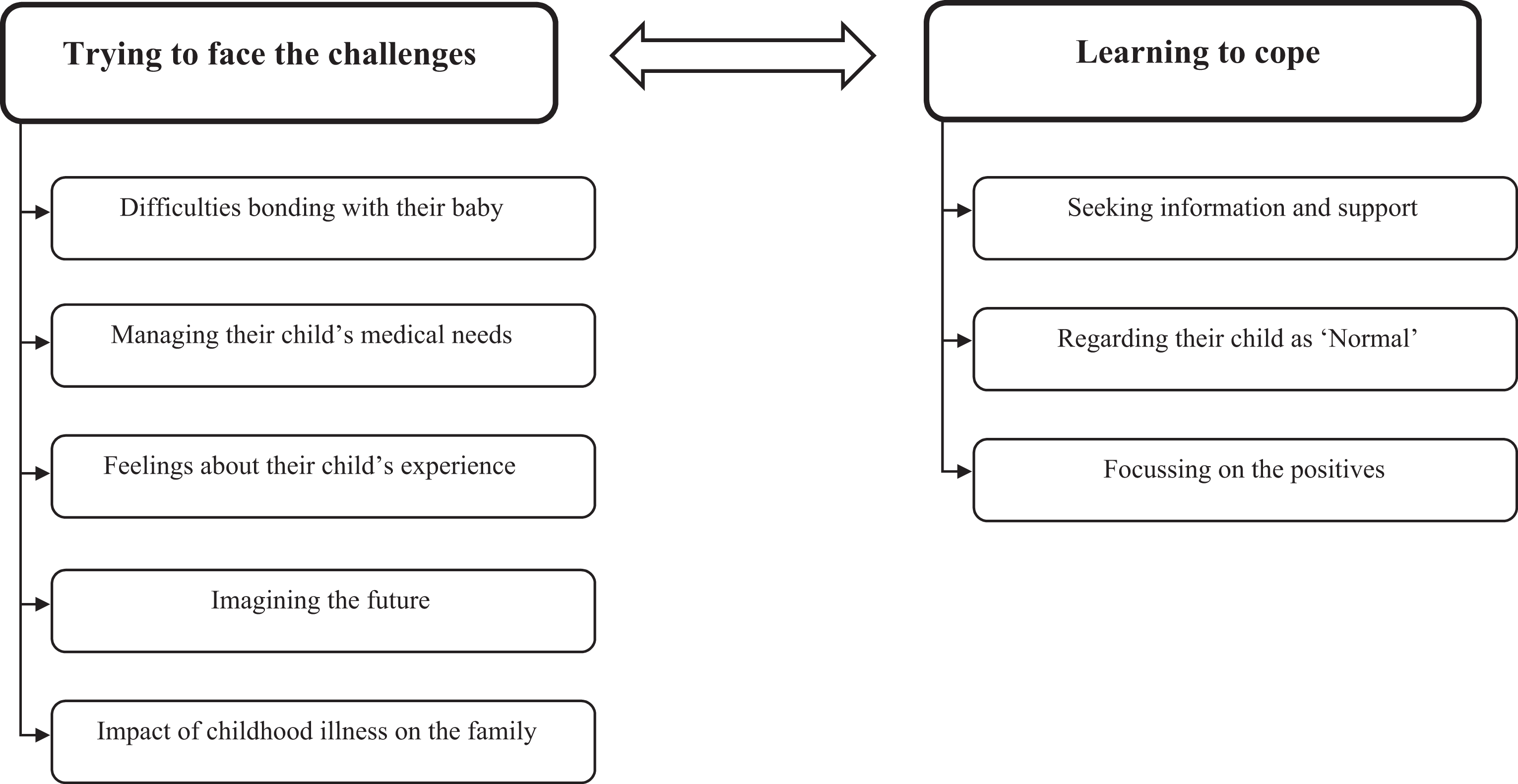
Summary of the overall themes and subcategories reflecting two phases in parents’ experiences. These phases occurred as an interactive process between encountering challenges and developing strategies to deal with these.
Trying to face the challenges
Difficulties bonding with their baby
Although all parents described their current relationship with their child as positive, some parents experienced difficulty in establishing this relationship (n = 3). One couple reflected on the ways the uncertainty regarding their child’s survival disrupted the bonding process and created a tentativeness around bonding: Not that I ever didn’t love him, but that real bonding came with time as opposed to immediately because there was still a part of me holding back for a long time because I didn’t know if I was going to lose him at any point. (Mother, ID011) When I brought him home, I had to say to people, ‘oh he’s three weeks old’ and felt like, he’s really a month old and I didn’t even really know him. (Mother, ID051)
Managing their child’s medical needs
All parents expressed difficulties in managing their child’s health-related needs and medical treatment. Ongoing appointments and hospital visits were perceived as necessary but time-consuming and difficult to manage: It’s just sometimes juggling with his appointments and what-not. That just makes it a little bit difficult. (Mother, ID081) So we’re quite diligent trying to get all of the stuff done that we need to do, but I can imagine if someone wasn’t that organised or that forthright in pushing to get the appointments and things that actually it would be quite complicated. (Father, ID052) …you come out of a meeting and feel really, absolutely heartbroken about maybe what they’ve just said. (Mother, ID051)
Feelings about their child’s experience
Some parents described ongoing difficulties in supporting their child during necessary treatment (n = 4), including the various tests, hospital visits, surgical procedures and CIC: At the moment, I don’t tell him we’re going [to the hospital], we just arrive and then I’m holding him down to get blood and holding him down to get a scan. (Mother, ID051) It’s been tough. Seeing your son go through surgery, and being crook, and drugged up, and all this sort of stuff – needles being put in and out; that side has been hard. (Father, ID092) He assumes that it is normal. In time I imagine that will change, when he works out that not everyone does this. (Father, ID012)
Imagining the future
Most parents (n = 6) expressed fear about the possibility of deterioration in their child’s health and QOL: This is something that’s in the back of your mind because you know later on down the track that something will happen. (Father, ID082) I always still think in the back of my head, he might still be on dialysis in a few years. (Mother, ID081) I hope and pray one day he will be able to go to the toilet by himself and not have to catheterise. Likelihood is he could be using a catheter for a long time to come. (Father, ID012) I find that I can’t think about the future because then I get more anxious about it. (Mother, ID011)
Impact of childhood illness on the family
All but one parent perceived their sons’ condition as having significantly affected their family. Two couples felt their focus had shifted to their child with PUV, leaving their other children with less dedicated time and attention. One mother expressed feelings of guilt in spending time away from her children while caring for her baby in the NICU: It was so disturbing and upsetting. I’d never been away ever and then suddenly I was gone for this child I didn’t even know. (Mother, ID051)
Learning to cope
Seeking information and support
Five parents were proactive in seeking support when needed. This involved seeking information and advice from clinical staff, particularly regarding their child’s treatment and prognosis. Most parents also accessed online support groups to obtain information and support from other parents who had experienced similar challenges. Family members and friends were a source of support for most parents. One mother described accessing a community-based service to assist with home duties and caring for her eldest son as needed. Other parents found it difficult to access information due to a lack of time during clinical appointments or difficulty knowing which health professional to approach. Two fathers expressed a need for increased dialogue about their child’s condition:
Sometimes we’ve said maybe we should be trying to book in a separate consultation, just to sit down and talk a bit more about the future and you know. (Father, ID052)
Regarding their child as ‘normal’
Seven parents used normalizing as a coping strategy in a number of ways: (1) viewing their child as a ‘normal kid’, (2) accepting challenges as part of the normal routine and (3) hoping for ‘normalcy’ in the future. Viewing their child as a normal kid enabled parents to develop a positive interpretation of their child’s situation without denying the difficulties he may face. This strategy also allowed parents to avoid the perception of having a ‘sick child’ and to perceive their child as separate from the anomaly: He’s just a normal little boy. You wouldn’t know that there was anything wrong with him. He plays with all the other kids, he does all the kid’s things. He wouldn’t know that he’s sick, he would have no idea that he’s got a problem. And a lot of the time my wife and I don’t even think about it. (Father, ID082) And as much as it is normal for most people to clean their teeth, it’s normal for me to put a catheter into [child] and do what needs to be done. It becomes part of life and you just get into a routine and work out what we need to do and just do it. (Father, ID012) Because being a child, being able to have a bath for the first time, is nothing short of amazing, and thinking that he might be able to have a normal-ish life. But it’s still a long shot from perfect. (Mother, ID011) He’s a beautiful kid. He’s really happy-go-lucky. Second child; bit of a risk-taker, bit of a menace at times. But such an outgoing, happy, smiley child. They often say those children that go through the most are happy and most content in life. (Father, ID012) You can sit in the cafeteria and he looks completely normal, and then you see a child who has got no hair and obviously going through cancer, or is really disfigured and you think, my goodness, what am I even worried about? It’s so nothing in the scale of what could have happened or what could happen. (Mother, ID051) Now I don’t think I would change anything. I don’t think I’d even change the condition now because I think it’s really shaped us as a family and I think he is unique in who he is and it’s made us a better family in some way. (Mother, ID051)
Discussion
Raising a child with a congenital anomaly presents unique challenges to parents. To the best of our knowledge, only one published study explores parents’ experiences of raising a child with CAKUT (Marokakis et al., 2016b). The present qualitative study explored parents’ experiences and perspectives in the context of raising a child with PUV. Parents in this study described the hardships they encountered and demonstrated a capacity to respond to these challenges as best they can using the resources available.
Parents of children with chronic illnesses, including congenital anomalies, are often faced with trying to establish a balance between acting as their child’s ‘medical caregiver’ and enjoying parenthood (Moola, 2012; Rempel et al., 2013; Tong et al., 2010). Parents in this study described the initial challenges associated with developing a loving parent–infant bond as they were driven to meet their infant’s immediate medical needs, as well as dedicate ongoing effort towards day-to-day management of their child’s condition at home. Participants described the need to take charge of their child’s medical care to increase his chance of survival, similar to parents of children with congenital heart disease (Rempel and Harrison, 2007). Therefore, the caregiver role became a dominant aspect of their parenting experience (Tong et al., 2010). In an attempt to protect their parenting role, some participants described incorporating their child’s medical care into their everyday routine, creating some sense of ‘normalcy’ for their child and family (Rempel et al., 2013; Tong et al., 2010).
Imagining their child’s future was a source of emotional pain for parents. Similar to parents of children with other chronic conditions, uncertainty surrounding their child’s prognosis and fears of further deterioration dominated parents’ future projections (Moola, 2012; Rempel et al., 2013). While some children with PUV may progress to renal failure or experience ongoing voiding problems requiring catheterization, others may not (Caione and Nappo, 2011; Heikkila et al., 2011). To cope with this uncertainty, parents remained hopeful their child would have the opportunity to live a ‘normal life’, rather than focusing on disease outcomes. This hope for a ‘normal life’ may act as a protective mechanism for parents to safeguard against anxieties about the future (Rempel and Harrison, 2007).
This process of ‘normalization’ also played a role in the way parents perceived their child. Lee and Rempel (2011) described normalization as both a cognitive process of developing a positive interpretation of their child’s circumstances and a behavioural process of maintaining a normal upbringing. Knafl and Deatrick (1986) suggested this coping response also involved behaving to sustain the impression of ‘normalcy’. Parents in the present study often described their child as a normal kid, creating a representation of their child that was not defined by the anomaly (Lee and Rempel, 2011). This, coupled with parental responsiveness to the needs of their child, safe and predictable caregiving and the development of a loving parent–child bond, may play a role in assisting children with PUV to develop a sense of emotional security in the context of medical illness (Belsky, 1999).
Strengths and limitations
As the first to specifically examine the experiences of parents of infants with PUV, this study has several strengths. The qualitative methodology allowed the experiences of parents to be explored in detail. All interviews were undertaken by a single investigator who had no prior contact with participants, therefore limiting potential researcher bias. Furthermore, mothers and fathers were interviewed separately to ascertain individual views and experiences. The study did, however, have limitations. Despite achieving informational saturation (Miles et al., 2014), the small sample size made drawing comparisons according to parent gender and disease severity difficult and may limit the generalizability of the findings.
Recommendations
This study provides a starting point for future research in this unexplored area. Future studies should include a larger sample and incorporate both qualitative and quantitative methodologies to allow for comparisons according to parent gender and disease severity. In addition, studies should include parents of children of all ages or be longitudinal in design to explore the potential changes in experiences as the child grows older. In terms of clinical practice, this study offers a preliminary understanding of parents’ experiences, which can be used to inform clinical care and support pathways for affected children and their families. Clinicians should remain an accessible source of information and support for parents to assist them in the ongoing management of their child’s health. Ensuring parents are informed of available services as additional avenues for emotional and psychological care is also imperative.
Conclusion
Parents of children with PUV face ongoing medical, psychological and practical challenges as they learn to parent a child with ongoing health concerns. Parents are faced with a need to manage their child’s medical care while coping with uncertainty about their child’s future and minimizing the burden of illness on the child and family. Although parents are able to develop a range of coping responses to this difficult situation, increased access to psychological care and support services may provide further assistance.
Footnotes
Acknowledgements
The authors would like to thank Ms Dianne Swinsburg from the School of Women’s and Children’s Health, UNSW Medicine, the University of New South Wales, the Heart Centre for Children and the Sydney Children’s Hospitals Network for assistance with interview preparation and training.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A/Professor Kasparian is the recipient of a Heart Foundation Future Leader Fellowship (ID 101229).