
Abstract
Transition from pediatric to adult health care is a key milestone for children and young people (CYP) with chronic conditions. Family management (FM) and self-management are two important concepts during the process. This study aimed to explore the relationships between FM, self-management and transition readiness, and quality of life (QoL), and identify the potential CYP or family factors influencing the relationships. Data about FM, self-management and transition readiness, QoL, and various contextual factors were collected from 268 caregiver–child pairs. Structural equation modeling was used to examine the relationships between all variables. Results revealed that the easy aspects of FM mediated the relationships between the challenging aspects of FM, self-management and transition readiness, and QoL of CYP. Self-management and transition readiness mediated the relationship between the easy aspects of FM and QoL. Contextual factors indirectly influenced CYP’s transition readiness and QoL through different aspects of FM. The results imply that to ensure the smooth transition from pediatric to adult health care and improve the CYP’s QoL, strengthening CYP’s independence and self-management competencies, combined with the support of the easy aspects of FM, seem to be useful strategies to increase CYP’s readiness for transfer.
Keywords
Introduction
The prevalence of childhood-onset chronic diseases is gradually increasing around the world (Morawska et al., 2015). A recent survey undertaken in the United States revealed that approximately 13–27% of children and young people (CYP) in the country are affected by chronic conditions (Modi et al., 2012). Meanwhile, in China, the prevalence of childhood chronic conditions is also showing an upward trend (Chen and Lin, 2012; Hou and Luo, 2016). Previous studies have analyzed the records of Chinese hospitals and found that common chronic illnesses, such as renal disorders, diabetes, and rheumatic diseases, have become between 1.12 and 2.5 times more prevalent now than 5–10 years ago (Fu et al., 2013; Shen, 2004; The Chinese Society of Pediatric Nephrology, 2004). The fact that 90% of CYP with chronic conditions survive into adulthood (Schwartz et al., 2011) means that it is imperative that health professionals identify methods of increasing CYP’s self-management and transition skills. Furthermore, it has been found that CYP with the above-mentioned chronic diseases have a greater risk of developing cardiovascular disease, the leading cause of mortality worldwide (Hu et al., 2012; Peng and Yan, 2007), and that this risk of terminal damage increases when inadequate self-management practices are applied. Consequently, determining answers to questions such as ‘how do the actions of parents and CYP facilitate or impede CYP’s transition to self-care?’ and ‘what CYP’s factors or family issues related to successful transitions can improve CYP’s quality of life (QoL)?’ represent clinical and research priorities (Fletcher-Johnston et al., 2011).
Family management (FM) relates to the coping styles adopted by families to respond to chronic diseases in CYP, and the type of management applied can affect the functioning of these families and the health of the CYP (Knafl et al., 2012). In an attempt to highlight the issues experienced by such families, as well as to identify areas amenable to clinical-setting based interventions, Knafl et al. (2011) developed six domains of FM: child’s daily life (5 items assessing caregivers’ perceptions of their child and his/her everyday life); condition-management ability (12 items assessing caregivers’ perceptions of the overall ability to manage the child’s condition); condition-management effort (4 items assessing the time and work required to manage the condition); family-life difficulty (14 items assessing caregivers’ perceptions of how having a chronically ill child makes family life difficult); view of condition impact (10 items assessing caregivers’ perceptions of the condition’s impacts on their child’s and family’s future); and parental mutuality (8 items assessing caregivers’ perceptions of satisfaction with how the partners work together to manage the condition). Then, in a related development, Zhang et al. (2013a) tested the cultural applicability of the family-management-style framework by applying it to the Chinese population; further, they also expanded the theoretical frameworks described in previous research by constructing two latent variables for FM: ‘easy aspects of FM’ (indicating easy levels in managing the condition), including child’s daily life, condition-management ability, and parental mutuality, and ‘challenging aspects of FM’ (indicating difficult levels in managing the condition), including condition-management effort, family-life difficulty, and view of condition impact. In China, caregivers were less likely to foster the CYP’s independence or facilitate his/her self-management because they perceived the CYP with chronic disease more vulnerable than healthy children and assumed more family responsibilities for caring for an ill family member than it is in Western families (Yang et al., 2017). Due to Chinese’s value of harmonious attitude, care sharing plays a pivotal role in caring practice. This value helps family members support and work together toward common goals (Guo et al., 2013). Thus, identifying cultural priority domains of FM will help in the development of culturally sensitive, family-centered care aimed at promoting self-management of Chinese CYP with chronic diseases (Guo et al., 2013).
The synthetic models of FM and self-management suggested that interaction with one another would determine transition readiness, and this can be used to ascertain CYP’s health-care autonomy in regard to illness management (Beacham et al., 2013; Grey et al., 2015).
Along with these models, a variety of studies have also highlighted the role of parent involvement in the transition process. As indicated by Speller-Brown et al. (2015) and Wright et al. (2016), there are strong positive correlations between parents’ involvement in the care process and CYP’s perceptions of their responsibilities in this regard and their overall transition readiness. In particular, specific domains of FM have been recognized as directly affecting the transition readiness or QoL of CYP with chronic diseases; for example, it appears that in families that engage in fewer conflicts, chronically ill CYP enjoy better adjustment (Mitchell et al., 2007). In another study, the mediating role of parental perceptions of CYP’s vulnerability play in the association between chronic illnesses and the CYP’s QoL was investigated (Houtzager et al., 2015). There was also a study which found that caregivers exhibiting high levels of self-efficacy and low levels of condition-management efforts managed their children’s diseases successfully (Lohan et al., 2017). According to theoretical models, parents’ belief is critical in supporting the transition process. The studies of Ersig et al. (2016) and Polfuss et al. (2015) demonstrated that when caregivers have low confidence in CYP’s abilities, or lack confidence in their own ability to manage CYP’s illnesses, and are concurrently concerned about CYP’s negative outcomes, this leads to an adverse transition in terms of the self-management of chronic diseases.
Transition in CYP’s health care generally relates to a gradual shift from pediatric to adult health care (American Academy of Pediatrics, 2002). This process involves multiple steps: Before the ‘transfer’, preparation for the transition should be commenced; during the ‘transfer’, the actual transfer from pediatric to adult care occurs; and after the ‘transfer’, level of adjustment to the new system is evaluated (Stinson et al., 2014). Actually, CYP with chronic diseases were often not well prepared for the transition process (Rutishauser et al., 2011). Most CYP experienced transition as abrupt changes from one environment to another due to age, rather than planned gradual shifts to adult health care. Not involving parents in their child’s transition process and not informing about the changes are common issues with transition. CYP and parents would benefit from the provision of preparatory instruction to support them to better understand the process of navigation from pediatric to adult services (Chu et al., 2015). Logically, transition process is only commenced when it is determined that CYP and their parents are prepared for it; thus, it has been suggested by researchers that transition readiness should be assessed and strengthened in advance of any actual undertakings (Van Staa et al., 2011a). Transition readiness is defined as the process of building CYP’s abilities to involve themselves in their own medical care (Van Staa et al., 2011a). Existing research has found that transition readiness is commonly used (1) as an indicator for beginning, continuing, and finishing the transition process from CYP-centered to adult-oriented health care (Schwartz et al., 2011), (2) as a factor reflecting CYP’s self-management abilities (Cohen et al., 2015), and (3) as a predictor of CYP’s QoL (Speller-Brown et al., 2015). In regard to means of improving transitional care, better preparing CYP for understanding the differences between the pediatric and adult health-care environment, beginning this process at an early stage, involving both CYP and their parents, and focusing on strengthening CYP’s independence have been recommended (Van Staa et al., 2011b). In particular, Cohen et al. (2015) recommended that transition readiness assessments are appropriate for CYP aged eight years and over. Preparing CYP at an early stage may give them more time to think about and decide when they want to leave, to determine what to expect in their new roles, and to learn the skills and knowledge required to manage such a transition. However, it has also been suggested that the age of transition to adult care should be flexible, depending upon the perceived readiness of the CYP and parents (Speller-Brown et al., 2015); in other words, preparedness for transition should be determined first, and then steps should be taken to begin the process. Therefore, there is a need for efficient and accurate assessments of transition readiness. Thus far, studies have identified the CYP’s age, disease variables, and the degree of parent involvement as factors associated with perceptions of increased readiness to undergo transition (Speller-Brown et al., 2015). Recent research concerning the assessment of transition readiness recommended that parental support must be identified and that an attempt be made to design an intervention that is based on reciprocal interactions between CYP and their surrounding environment (Schwartz et al., 2011; Wright et al., 2016).
CYP’s QoL is a multidimensional construct based on subjective perceptions of health status, which is defined as relating to physical, emotional, social, and academic health (Varni et al., 2003). The QoL of CYP with chronic diseases is particularly important as many such CYP will not be cured and these individuals will be required to manage their chronic illness into adulthood. Both Healthy People 2020 (2014), which was implemented in the United States, and Healthy China 2030 Guidelines (National Health and Family Planning Commission of the People’s Republic of China, 2016) identified QoL improvement as a central public health goal. Further, increasing emphasis has been placed on understanding methods of enhancing the QoL of CYP with chronic illnesses. For example, While et al. (2017) compared the QoL of CYP with long-term illnesses before and after they transferred from child to adult health care, and they consequently found that disease category, gender, and maternal factors were predictors of QoL both before and after the transition; meanwhile, other studies have suggested that the transition process itself affects CYP’s QoL (Polfuss et al., 2015; Schwartz et al., 2011).
Considering literature relating to the involvement of parents in the management of CYP with chronic diseases, the relationship chain linking FM, self-management and transition readiness, and QoL have been found in above theories. Further, contextual factors have been found to be related to FM, while different aspects of FM have been identified as having impacts on the self-management and transition readiness of CYP. Moreover, self-management and transition readiness have also been identified as being associated with CYP’s QoL. However, questions concerning how and to what extent these factors cause an influence still require answering. Identifying the mechanisms linking FM, self-management and transition readiness and QoL will lead to a better understanding of how we might facilitate self-management and transition skills in the context of specific FM for CYP with chronic conditions.
Current study
This study used structural equation modeling to explore the interrelationships between the FM, self-management and transition readiness, and QoL of chronically ill CYP. To perform this, we set several related hypotheses:
The hypothesized model is outlined in Figure 1.

The hypothesized structural model based on literature. QoL: quality of life.
Methods
Samples
This is a cross-sectional survey of 268 CYP with chronic conditions and their caregivers. Participants were recruited from two children’s medical centers, and the survey was distributed between June 2016 and March 2017. For the CYP, the inclusion criteria for this study were as follows: (1) aged 8–18 years; (2) diagnosed with one of the following common chronic diseases: diabetes, rheumatic disease, or renal disorder. An additional requirement for the study was the participation of the caregivers who accompanied the CYP to the hospital; however, family members were deemed ineligible if the child had a mental health condition or if they were in a critical condition. Of the 324 eligible caregiver–child pairs approached, 268 (82.7%) agreed to participate and returned valid questionnaires.
Procedure
Ethical approval for this study was acquired from the Research Ethics Committee of the School of Nursing and Public Health, Shanghai Jiao Tong University. Eligible hospitalized caregiver–child dyads were initially identified with the assistance of pediatric nurses; then, the individuals were contacted by two authors in person; these authors explained the purpose of the study and invited them to participate. Once written consent including the reward for participation was obtained from pediatric patients and their primary caregivers, data were collected through the distribution of pen-and-paper-based questionnaires. Each CYP received a gift of ¥30 after they had completed the Self-Management and Transition to Adulthood with Rx=Treatment (STARx) Questionnaire and Pediatric Quality of Life Inventory 4.0 Generic Core Scales (PedsQL 4.0) and their caregiver had completed the demographic questionnaire and Family Management Measure (FaMM) as described in the following.
Measures
Demographic questionnaire
Family characteristics included geographical location, income, number of children, parental education, and employment status. CYP’s characteristics included age, gender, disease category, disease duration, number of days absent from school, and number of medicines used.
Family management
FM was assessed using the Chinese version of FaMM (Zhang and Wei, 2009), which was in fact a translation of the original FaMM developed by Knafl et al. (2011). The Chinese version of FaMM has been culturally tested in regard to Chinese families (Zhang et al., 2013a) and has been widely used in the Chinese context (Sun et al., 2013; Yang et al., 2017). Specifically, FaMM is a 53-item caregiver-report questionnaire that is scored using a 5-point Likert scale (1 = absolutely disagree to 5 = absolutely agree). FaMM assesses six dimensions of FM (see the ‘Introduction’ section). Cronbach’s alpha for the six scales of the current sample ranged from .45 to .83.
Self-management and transition readiness
Self-management and transition readiness was assessed using the STARx Questionnaire (Ferris et al., 2015). For this survey, the Chinese translation of this tool was applied. To develop this translation, the scale was forward–backward translated, and then, adopting the cross-cultural measurement approach, it was revised in order to enhance its appropriateness for Chinese culture (Waltz et al., 2004). Specifically, the Chinese version of the STARx Questionnaire is an 18-item self-report questionnaire that utilizes a 5-point Likert scale (1 = never to 5 = always). The STARx Questionnaire assesses six dimensions: medication management (four items addressing CYP’s ability to manage his/her medications); provider communication (three items addressing the CYP’s ability to communicate with health providers); engagement during appointments (three items addressing the CYP’s engagement during the appointments with health providers); disease knowledge (three items addressing the CYP’s knowledge of the disease and its management); adult health responsibilities (two items addressing the health responsibilities assumed to the CYP); and resource utilization (three items addressing the resource used by the CYP). Higher scores on the STARx Questionnaire indicates better self-management and transition readiness. The content-validity index was .92. Acceptable reliability was determined in regard to the total scores for self-management and transition readiness (Cronbach’s alpha = .83). Confirmatory factor analysis was performed to test the fit of the same factor structure of the original STARx Questionnaire for the Chinese CYP. More details are presented in Online Supplemental files 1 and 2.
Quality of life
QoL was reported by CYP using the Chinese version of PedsQL 4.0 (Lu et al., 2008). This is a 23-item self-report questionnaire that is scored using a 5-point Likert scale (1 = never to 5 = always). The PedsQL 4.0 assesses four dimensions of QoL: physical functioning (eight items), emotional functioning (five items), social functioning (five items), and school functioning (five items). Higher scores on the PedsQL 4.0 indicate better QoL. Cronbach’s alpha for the current sample was .91.
Data analysis
Descriptive, bivariate correlation and multiple linear regression analyses were performed using SPSS 20.0. In order to examine the relationships between demographic variables, FM, self-management and transition readiness, and QoL, structural equation modeling was conducted using the software LISREL 8.8.
Structural equation modeling is a framework that reflects complex relationships in multivariate data using latent factors, and significantly contextual variables in the multiple regression analysis were included in the structural equation modeling. In our study, structural equation modeling was performed through a two-step approach. First, a confirmatory factor analysis was conducted to examine the measurement model, which revealed the relationship between latent variables and their corresponding observed variables. Then, a structural equation model was prepared to explore the relationships between latent factors and contextual variables. Next, the fit of the models to the current data was appraised using a variety of indices, and this provided a comprehensive evaluation. The chi-square (χ2), root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), comparative fit index (CFI), and normed fit index (NFI) were then used to evaluate the model fit. The χ2 test was nonsignificant, indicating that the model was acceptable (Kellar and Kelvin, 2013); however, multivariate skewness or large samples may result in a large χ2 statistic, which would lead to a significant outcome. Meanwhile, CFI and NFI values greater than .90, RMSEA values close to .06, and an SRMR below .08 indicate a good fitting model (Kellar and Kelvin, 2013). Finally, R 2 values, indicating the amount of variance in the dependent variables that can be explained by the model, were computed using the reduced-form equations in our model.
Results
Preliminary analyses
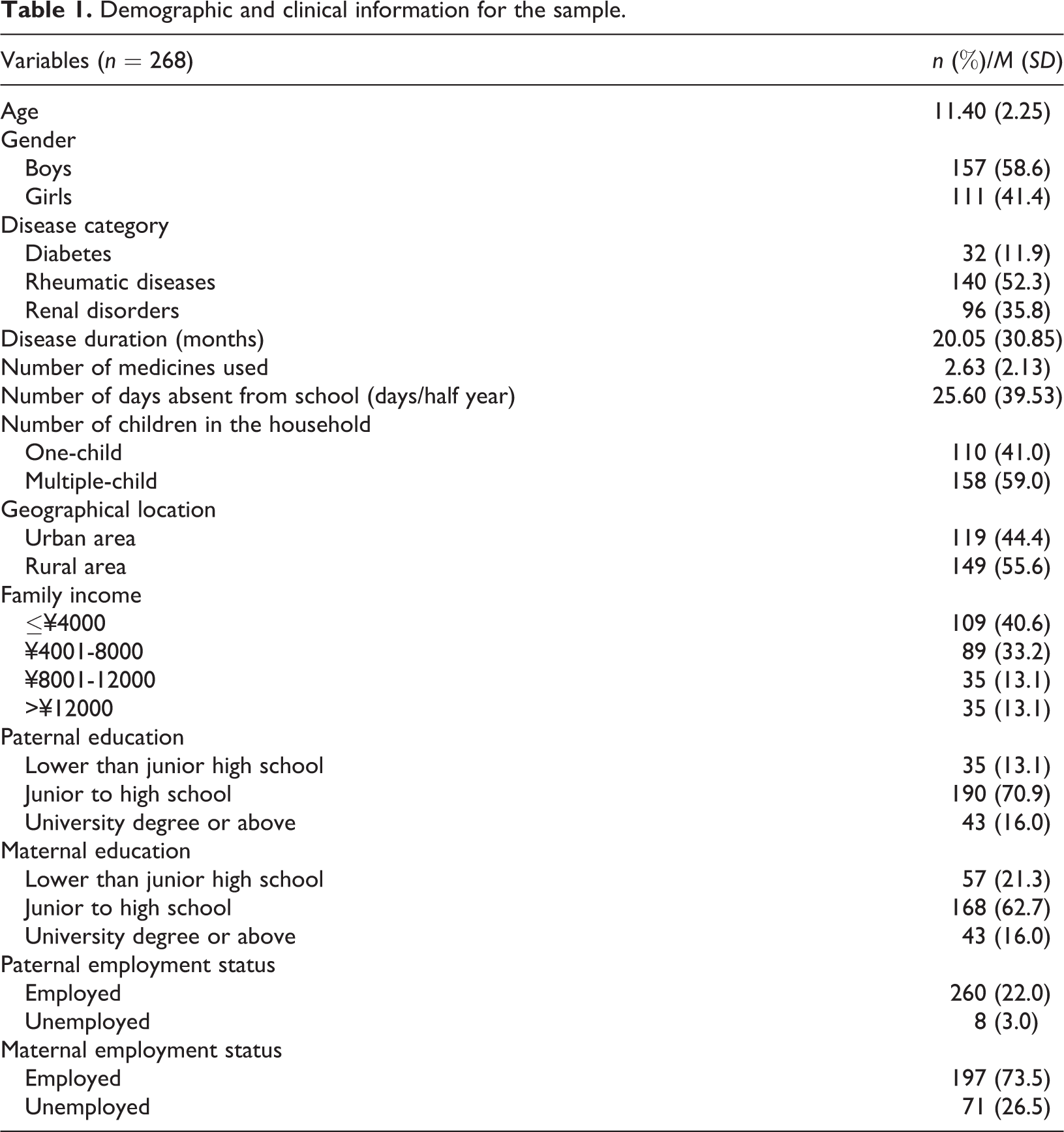
The current study included 268 caregiver–child pairs, with the caregivers in question consisting of 181 (67.5%) mothers, 46 (17.2%) fathers, and 41 (15.3%) grandparents. The average age for fathers was 39.7 years (SD 5.27), ranging from 29 to 58 years, while for the mothers it was 37.5 years (SD 4.83), ranging from 27 to 53 years. Meanwhile, the majority of the CYP (181, 67.5%) were no more than 12 years old. Detailed demographic and clinical data are shown in Table 1.
Demographic and clinical information for the sample.
The mean FaMM, STARx, and PedsQL 4.0 scores and the correlations between them are summarized in Table 2. The correlation results indicated that significantly positive relationships exist between the child’s daily life, condition-management ability, and parental mutuality and the STARx and PedsQL 4.0 scores, and that negative relationships exist between the efforts to manage the condition, family-life difficulty, and impact of the condition and the STARx and PedsQL 4.0 scores. Further, significant positive relationships between the STARx and PedsQL 4.0 scores were also identified in the present study.
Descriptive correlations of the observed variables.
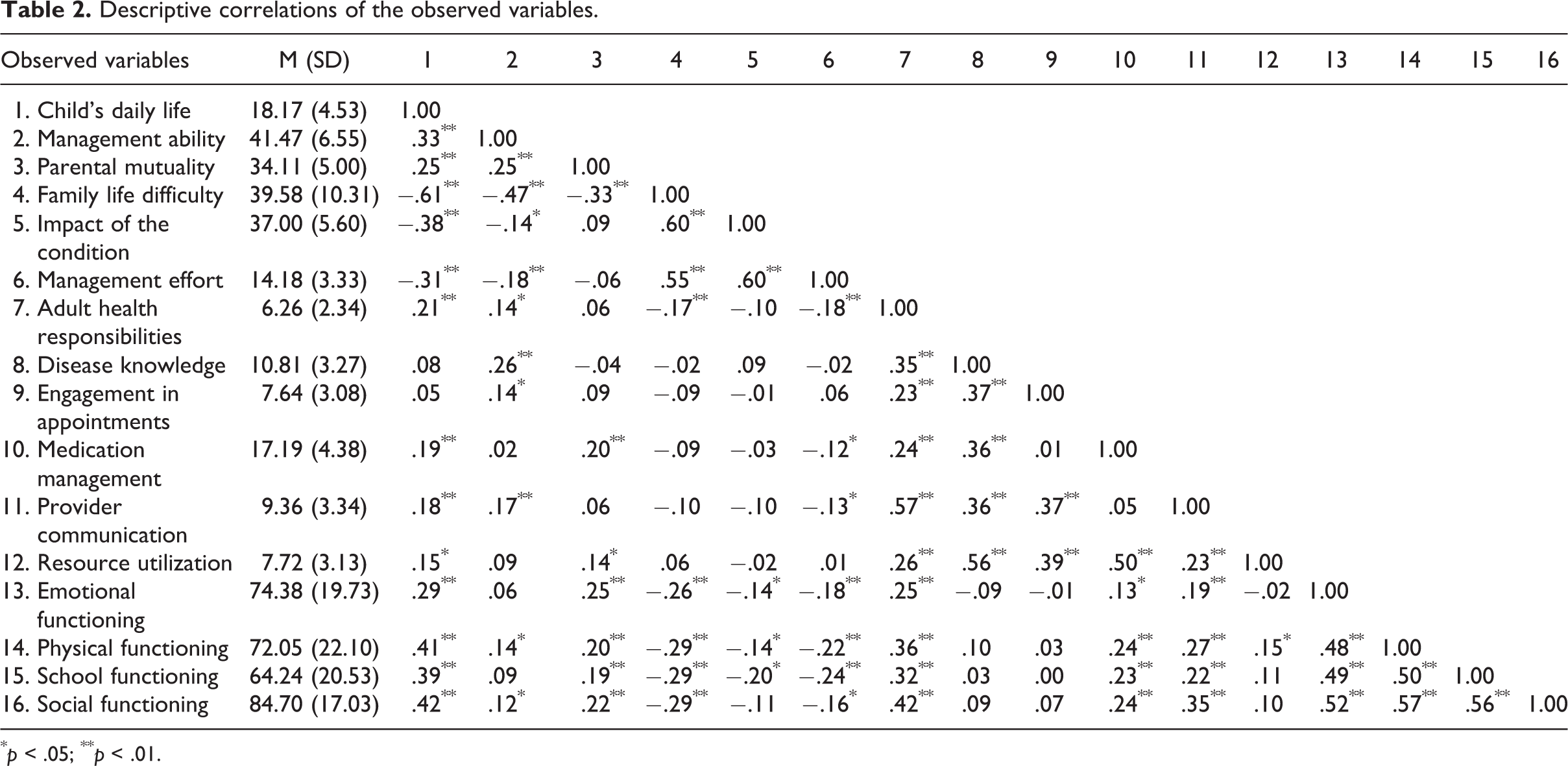
* p < .05; ** p < .01.
To select significant contextual variables within the structural equation modeling, associations between the scores for the six domains of FM, self-management and transition readiness, and the QoL of CYP and the demographic variables were examined using multivariate linear regression analysis. Eight regression models were conducted with these variables, and these are provided in Online Supplemental File 3.
Structural equation model
First, a confirmatory factor analysis was conducted to examine the measurement model’s determination of latent variables, including easy aspects of FM, challenging aspects of the FM, self-management and transition readiness, and QoL of CYP; the standardized loadings of the indicator variables are summarized in Online Supplemental File 4. Then, a structural equation model was explored. The original structural equation model, which examined the relationships between the latent variables of the easy aspects of FM, challenging aspects of FM, transition readiness, and QoL, showed a good fit to the current data [χ2 = 149.68, df = 86, p < .001, NFI = .93, CFI = .97, RMSEA = .053 (90% CI = .038–.067), SRMR = .066]. As hypothesized, when we added the contextual variables that were significant predictors in the multiple linear regression analyses to the structural equation model, the statistical parameters for the initial model consequently indicated an imperfect fit [χ2 = 464.65, df = 227, p < .001, NFI = .89, CFI = .94, RMSEA = .063 (90% CI = .054–.071), SRMR = .075]; then, after removing the nonsignificant paths and revising the model according to the modification indices, the final model was found to fit well with the sample (χ2 = 340.28, df = 185, p < .001, NFI = .91, CFI = .95, RMSEA = .056 (90% CI = .047–.065), SRMR = .074) (Figure 2).

Final structural model with standardized estimates. * p < .05; ** p < .01. QoL: quality of life.
These results fully support hypothesis 1. The analysis indicated that fewer number of medicines used (β = −.19, p < .001), higher maternal education (β = .14, p = .011), and higher family income (β = .23, p = .002) predict high levels of easy FM. Meanwhile, diabetes (β = .13, p = .026), longer disease duration (β = .12, p = .027), more number of medicines used (β = .22, p < .001), one-child family (β = .15, p = .005), and lower family income (β = -.39, p < .001) predict high levels of challenging FM. Further, hypothesis 2 was fully supported because perception of easy levels in FM positively influenced self-management and transition readiness (β = .15, p = .019), and QoL (β = .69, p < .001), and hypothesis 3 was partially supported because perception of difficult levels in FM were found to indirectly influence self-management and transition readiness and QoL through negatively affecting perception of easy levels in FM (β = −.52, p < .001). Finally, hypothesis 4 was fully supported because self-management and transition readiness positively influenced QoL (β = .25, p < .001). Furthermore, there were also significant direct relationships identified between contextual factors, self-management and transition readiness, and QoL. Specifically, diabetes (β = .15, p = .003), fewer number of medicines used (β = −.19, p < .001), and rural families (β = .17, p < .001) predicted better self-management and transition readiness, while higher family income directly predicted poorer QoL (β = −.20, p = .014). Consequently, this structural equation model explained 39% of the easy aspects of FM, 29% of the challenging aspects of FM, 18% of the CYP’s self-management and transition readiness, and 14% of the QoL.
Discussion
Focusing on Chinese families that include CYP with chronic diseases, our study mapped the complex relationships that exist between FM, self-management and transition readiness, and QoL, and elucidated the mechanisms through which aspects of FM affect CYP’s transition readiness and QoL.
Our finding is consistent with previous findings that FM and self-management are intimately linked (Grey et al., 2015). The pathway from challenging aspects of FM to easy aspects of FM, influenced the CYP’s self-management and transition readiness and QoL (see Figure 2). This indicates that FM indirectly affects CYP’s QoL by determining the difficulty of aspects of self-management and transition readiness.
Our identification that easy aspects of FM serve as regulating agents is an important finding. Both Western and Chinese studies have noted the importance of child identity (belong to easy aspects of FM) and its potential to influence the relationship between a child and their family (Im et al., 2014; Zhang et al., 2013b). CYP with chronic diseases should face the challenges associated with managing the condition and integrate them into their identity. As CYP gain skill and knowledge in their ability to manage their diseases, they assume increasing levels of responsibility and independence; however, parents may experience difficulty changing from being caregivers and accountable decision makers to assuming supportive or consultative roles. Particularly, they have low confidence in their children’s abilities to transition to self-management or handle unanticipated fluctuations in their illness trajectory without constant parental vigilance (Ersig et al., 2016). In fact, parents who treat CYP as more vulnerable may cause these CYP to experience more difficulties in relation to their daily behaviors (Cipolletta et al., 2015). Thus, it may be beneficial for pediatric health-care settings to develop effective training programs that can improve parents’ cognition concerning the illness and the CYP and help them promote their children’s autonomy whilst remaining sensitive to the CYP’s situation (Houtzager et al., 2015). According to Ferris et al. (2015), medication management is an essential aspect for achieving success in the transition process, and belief in the CYP’s capabilities and satisfaction in regard to collaboration in family care are closely tied with adherence to medication (Beacham and Deatrick, 2013). Focusing on this aspect of transition readiness, particularly with the aid of the aforementioned modified components regarding easy aspects of FM, may be the key to successful transition.
The other main result emerging from this research concerning FM is that the challenging aspects of FM are indirectly related through the easy aspects of FM to the self-management and transition readiness and QoL of the CYP, which indicates that different aspects of FM vary in importance for CYP with chronic diseases. CYP’s daily lives, management competence, and family cooperation can form an interconnected web that mediates the negative impact FM challenges have on self-management and transition readiness and QoL. Further, parents’ concerns regarding the CYP’s health and future have been found to be negatively associated with parents’ decisions to empower the CYP to assume self-care roles (Vuorenmaa et al., 2016). Furthermore, the incongruence between the CYP’s beliefs and those of their parents’ concerning management of the illness can cause conflicts between the parents and CYP (Daneman and Nakhla, 2011). A greater number of family conflicts and less encouragement of independence have also been found to be associated with ineffective self-management, as well as difficulties in assuming control of parental management (Babler and Strickland, 2015). Certainly, it can be difficult for parents to differentiate illness-related issues from general family events, which may potentially generate family conflicts; therefore, in order to develop good self-management, clinicians should consider how a change in one domain of FM can potentially alter the entirety of the FM patterns.
Self-management and transition readiness was found to mediate the relationship between easy aspects of FM and QoL, suggesting that when caregivers find FM to be easy, the self-management and transition readiness of CYP is better (Lo et al., 2016). This partially supports the finding stipulated in previous literature that family involvement is important for assisting transition, and that ‘better child and parent preparation’ is a priority for the improvement of self-management (van Staa et al., 2011b). By reviewing parental interventions over the last 20 years, it has become clear that successful parenting programs for parents of chronically ill CYP should feature an emphasis on the importance of good illness-management skills, and they should also focus on enhancing positive parenting, which can help improve a CYP’s adjustment and QoL (Morawska et al., 2015).
FM was found to mediate the relationships between CYP-specific and parent-level factors and CYP’s outcomes. Our results strengthened the evidence that higher income, higher maternal education, and fewer number of medicines used to predict easy aspects of FM, and that lower income, one-child family, longer duration, and more number of medicines used to predict challenging aspects of FM, with these eventually influencing self-management and transition readiness and QoL. (Ferris, et al., 2015; Hua et al., 2014; Zhang et al., 2013a; Zhang et al., 2013b). These findings shift FM from being a predictor to serving as a mediator, and clarifies that it is influenced by the characteristics of the CYP and family.
Limitations
There are several limitations to our study. First, the cross-sectional design of the present study did not afford an exact assessment of the causality between the variables. Second, only three categories of illnesses were included in our study; thus, the results do not represent all families having CYP with chronic conditions. Finally, condition-management effort did not have high reliability, which might result from the small number of items involved (Waltz et al., 2004). Further research consisting of a larger and more diverse sample is therefore needed.
Clinical implications
The findings of the study highlight that health professions should provide FM support programs that focus on augmenting parents’ perception of their children and the diseases in question in such a manner that they are convinced to promote their children’s autonomy. This study also implies that addressing FM challenges relating to illnesses may be useful for reducing the risk of poor transition readiness and maladjustment to the transition. Knowledge generated from the study can be useful to clinicians and researchers that prepare CYP and caregivers to adapt as a unit and strengthen the positive influences FM has on CYP’s self-management and transition readiness and QoL, exploring effective interventions targeting the caregivers’ illness-management ability, opinions of condition impact, and their relationships. Through this, clinicians could implement education and build parents’ confidence to allow the CYP to successfully manage the disease and facilitate transition.
Conclusion
This study used caregiver–child data to examine the relationship between FM, self-management and transition readiness, and QoL in an attempt to expand understanding of methods of developing self-management and transition readiness in the context of specific FM, which may in turn affect CYP’s QoL. This study was unique in that it identified FM-related facilitators and barriers to CYP’s self-management and transition readiness skills and explored optimal mechanisms for the provision of family-focused transition support within health-care settings.
Supplemental Material
Supplemental Material, Supplementary - Family management affecting transition readiness and quality of life of Chinese children and young people with chronic diseases
Supplemental Material, Supplementary for Family management affecting transition readiness and quality of life of Chinese children and young people with chronic diseases by Nan Sheng, Jiali Ma, Wenwen Ding, and Ying Zhang in Journal of Child Health Care
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grants from Shanghai Municipal Commission of Health and Family Planning (grant number 201540212) and Shanghai Municipal Education Commission-Gaoyuan Nursing Grant Support (grant number Hlgy1602gj and Hlgy17003jys).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.