
Abstract
Recent studies have reported contrasting results in the socio-emotional adjustment of Italian adolescents with cochlear implants (CIs). The aim of the present study is to explore the relationship between the socio-emotional adjustment of adolescents with CIs, the quality of their hospital stay, and their age at CI activation. The participants were 29 adolescents with CIs (CI group) and 29 typically developing adolescents (TD group). The Emotional Autonomy Scale, the Loneliness and Aloneness Scale for Children and Adolescents, and the Multidimensional Self-Concept Scale were administered to each participant. The emotional experience reported during the hospital stay was considered for each participant in the CI group. The adolescents with CIs displayed significantly higher levels of loneliness and lower levels of aversion toward aloneness than the TD group participants. Adolescents who had received the CI in preschool displayed a higher level of physical self-concept than adolescents who had received it later. The adolescents’ emotional experiences at the hospital were reported to be quite complex and related to their relationships with parents. In summary, the findings point to a specific type of fragility in socio-emotional adjustment—focused on loneliness/aloneness—rather than a general one.
Keywords
Introduction
Adolescence is described as a period in which the young person experiences a range of types of challenges and changes in many domains, including the socio-emotional, the cognitive, the physical, and the psychological (Rich et al., 2013). Blos (1979) defines adolescence as a second process of separation/individuation, during which the individual typically experiences a redefinition of the ‘relational distance’ (separation) from parents and a strong commitment to relationships with peers (Maes et al., 2015). Although this redefinition of significant relationships, especially the ‘permanent relationships’ (‘close relationship theory’, Laursen and Bukowski, 1997), can be associated with negative emotional experience (e.g. depression, anxiety, impulsiveness, and loneliness), it is fundamental for the construction of identity (Musetti et al., 2012), ‘separated’ from parents’ identification. At the same time, in this process of constructing social identity, a positive identification with peers is fundamental to dealing with these feelings and to acquiring autonomy and social competence.
Loneliness is a crucial experience in the life of individuals (Goossens et al., 2009; Majorano et al., 2015) because adolescents’ social experiences and expectations of social interactions change, as does their perception of what constitutes social isolation (Qualter et al., 2015). As loneliness can be experienced in different relationships, many researchers regard it as a multidimensional concept which presupposes that it can take many shapes (Goossens et al., 2009; Maes et al., 2015), each of which has different degrees, and types, of importance at different stages of development. For example, many studies have shown that healthy aloneness, feelings of separation toward parents, and, at the same time, feelings of intimacy and support by peers are the necessary aspects of the processes of identity construction in relation to family and friends. Individuals, however, can experience different developmental trajectories of loneliness. In the hybrid multidimensional model that Goossens and colleagues developed following wide-ranging research (Goossens et al., 2009; Marcoen et al, 1987), two kinds of loneliness (parent- and peer-related) and two attitudes toward aloneness (affinity and aversion) were considered and assessed by the Loneliness and Aloneness Scale for Children and Adolescents (LACA). The parent-related loneliness could be considered a ‘healthier’ dimension of the experience of loneliness, while peer-related loneliness is considered a risk factor associated with negative psychological outcomes (Vanhalst et al., 2012; Yu et al., 2005). This multidimensional approach has also identified some developmental trajectories in typical populations (Goossens, et al, 2009). Specifically, parent-related loneliness increases and peer-related loneliness decreases during the transition from early adolescence to late adolescence. On the other hand, affinity for aloneness increases and aversion to loneliness decreases (Corsano et al., 2006), alongside the gradual acquisition of autonomy.
The separation/individuation process is complex and contradictory (Beyers et al., 2005). In fact, adolescents have to face both their need for independence and their need for their parents’ protection. This process can be more difficult for adolescents with a sensory disability, such as individuals with severe and profound hearing loss with/without a cochlear implant (CI), who must face the challenge of being deaf/hard of hearing in a sound-dominated world that is not always aware of their needs (Majorano et al., 2015; Moog et al., 2011). Parents often report higher levels of self-esteem, confidence, and outgoing behavior in their children after cochlear implantation (Leigh et al., 2009) but a significant number of research papers have demonstrated that children with CIs are at risk of experiencing communication and language delays, which can harm their cognitive and social development (Le Maner-Idriss et al., 2008; Preisler et al., 2002). Specifically, several studies have identified difficulties in the area of socio-emotional adjustment for adolescents with sensory problems, including loneliness and self-concept (Maes et al., 2017; Theunissen et al., 2014; Yucel and Sennaroglu, 2007). This may be because hearing impairments affect the ability to communicate with others and they may disrupt interpersonal relationships (Cacioppo et al., 2015). Moreover, a poor linguistic and communicative development has been related to lower levels of self-esteem (Hintermair, 2008) and greater social difficulties (Kouwenberg et al., 2012).
In general, most studies argue that hearing-impaired adolescents exhibit more psychological problems, for example, depression and anxiety disorders, than normal hearing peers. This can lead them to moving away from friends and family. However, some studies have shown that the data on affective disorders in adolescents with CIs are comparable to those on peers with typical development (Bailly et al., 2003).
Furthermore, for the deaf young person, the activation of a CI during adolescence can make it even more difficult to accept himself and his body self-image. Several studies have focused on the impact of the CI on quality of life, especially with regard to body self-image and psychological satisfaction. In the life of an adolescent with hearing disabilities, the CI may be a hindrance to acceptance by his/her peer group (Celli, 2014). On the other hand, several studies have indicated various benefits and advantages of using CIs. In addition to improved language ability, progress has been identified in socio-emotional skills (Bat-Chava et al., 2014), quality of life (Faber and Grøntved, 2000), and self-concept (Moog et al., 2011). Moreover, although many studies have hypothesized that deaf adolescents are at risk of developing psychological disorders, the empirical evidence is not so consistent, with some studies suggesting that the socio-emotional development of these adolescents is comparable with that of their hearing peers (Yucel and Sennaroglu, 2007).
The contrasting results in this field of research may be related to the high degree of variability in the characteristics of individuals with CIs. First, the age at CI activation could be a very important factor as early implantation allows significant improvements to be achieved not only in linguistic skills, such as speech comprehension and production (Zwolan et al., 2004), but also in psychological well-being. Several studies have assessed the relationship between age at CI activation and language development in children with CIs and most of them have found that earlier implantation is associated with better vocabulary acquisition (Tomblin et al., 2008), especially in the first three years after CI activation (Dunn et al., 2014). Nevertheless, a number of studies have reported considerable variability in the language profiles of children with CIs and contrasting results have emerged for the positive effect on language skills of early age at implantation (Szagun and Schramm, 2016)
A second explanation of contradictory results regarding the socio-emotional well-being of adolescents with hearing problems concerns their emotional experience in the hospital and the support they felt they received during their experience as patients. A hospital stay, short or long, can be perceived by young patients as a traumatic and stressful event. In addition to the medical/physical implications, the adolescent is in a strange environment, to some extent separated from family and peers and deprived of daily activities and leisure (Carney et al., 2003; Corsano et al., 2015). Because adolescence is a period of increased vulnerability to anxiety of separation and one in which the individual’s cognitive ability to understand and accept the hospital stay is still limited, it is important to assess the emotional experience of adolescents at the hospital. The observation and direct assessment of adolescents’ experiences can help us to optimize the quality of care, reduce anxiety and stress, and improve the overall environment (Carney et al., 2003). Furthermore, a positive emotional experience can improve the quality of young patients’ care and reduce distress, thus preventing long-term negative consequences for their socio-emotional well-being (Carney et al., 2003; Corsano et al., 2012). Adolescents can experience exclusion and loneliness if they do not perceive good quality communications in their health care (Coyne and Kirwan, 2012) or support from significant adults because they are basic factors in the construction of positive relationships and feelings of comfort and security. If the adolescents are enabled to tell stories of their emotional experience using emotional terms rather than medical ones, it might help them to integrate their experience in the hospital with their normal life (Corsano et al., 2015). This aspect could be particularly important for children with CIs, testing their ability to integrate the CI activation with their emotional experience, providing an indication of their socio-emotional adjustment.
The present study
The first aim of the present study is to explore the socio-emotional adjustment of adolescents with CIs compared with that of adolescents with typical development (TD) and its relationship with (i) the quality of their hospital stay and (ii) their age at CI activation. Following the literature, we expected that (a) CI adolescents would display higher levels of loneliness (parent- and peer- related), lower levels of affinity for aloneness, and higher levels of aversion for aloneness than TD adolescents and (b) CI adolescents will have lower scores in self-concept scale, particularly in the physical domain, than control adolescents.
The second aim is to investigate the relationship between the age at CI activation and socio-emotional adjustment. Following the literature, we expected that, relative to their age-mates who experienced CI activation at a later age, CI adolescents with a lower age at CI activation would (a) display higher scores in the self-concept scale, particularly in the physical domain and (b) feel less lonely, probably in both types of relationship examined,.
Our third aim was to investigate the emotional experiences of adolescents with CIs during their stays in hospital. We expected to find a relationship between a positive emotional experience in hospital (expressed by the ability to use emotional terms rather than medical terms and higher number of words) and socio-emotional adjustment as measured by other instruments.
The study could have important implications for professional practice in hospitals in the social and health care of adolescents with CIs, specifically for the assessment of socio-emotional development (as well as helping with the assessment of their cognitive and linguistic abilities) and the development of support programs for the adolescents and their families designed to prevent long-term problems in socio-emotional development.
Methods
Participants
Two groups were included in the present study. The first group (CI group) comprised 29 adolescents (17 males and 12 females) with CIs, aged between 12 years and 20 years (M = 14.3, SD = 2.3). In order to be enrolled in the study, participants had to meet the following criteria: (1) a diagnosis of nonsyndromic severe and profound hearing loss, (2) normal inner ear morphology, (3) the absence of intra-, peri-, and postoperative complications, (4) exclusive use of oral language, and (5) hearing parents. Some of the adolescents were diagnosed within their first four years (n = 20). All participants had routine and follow-up visits at the Otorhinolaryngology Operational Unit ‘G. Saliceto’ Hospital, in Piacenza (PC, Italy). The second group (TD group) comprised 29 typically developing adolescents, individually matched for gender, age, and socioeconomic family status. Parents’ years of education were also considered. The mothers’ average years of education in the CI group were 15.79 and in the control group 16.15. No significant differences emerged between the groups. None of the adolescents in the control group had disabilities or learning problems and they lived in the same geographic area as those in the CI group. Both parents of each adolescent in each group signed the informed consent form and the study was approved by the local ethical committee (Prot. no. 1594/2016).
Instruments
Emotional autonomy
The Italian version (Maleddu and Scalas, 2002) of the Emotional Autonomy Scale (EAS; Steinberg and Silverberg, 1986) was administered. This scale investigates emotional autonomy from parents and consists of 20 items, which can be answered on a 4-point Likert-type scale: 1 = strongly disagree; 2 = somewhat disagree; 3 = somewhat agree; and 4 = completely agree. Following Beyers et al. (2005), the factorial model consisting of two dimensions was used: separation (e.g. ‘My parents and I agree on everything’ α = .83) and detachment (e.g. ‘I might be surprised to see how my parents act at a party’ α = .58), that is, respectively, adaptive and disadaptive forms of emotional distancing from parents.
Loneliness and attitudes toward aloneness
The Italian version (Melotti et al., 2006) of the LACA (Marcoen et al., 1987) was used in order to explore participants’ sense of loneliness and attitudes toward aloneness. The questionnaire consists of four subscales, each composed of 12 items, rated on a 4-point Likert-type scale: 1 = frequently; 2 = sometimes; 3 = rarely; and 4 = never. The four subscales assess loneliness toward parents (e.g., ‘My parents make time to pay attention to me and to listen to me’; reverse coded L-Part, α = .69), loneliness in relation with peers (e.g., ‘I feel left out by my friends’, L-Peers, α = .94), aversion toward aloneness (e.g., ‘When I am alone, I feel bad’ A-Neg, α = .83), and affinity toward aloneness (e.g., ‘I want to be alone’ A-Pos, α = .83).
Self-concept
The Italian version (Bergamini and Pedrabissi, 2003) of the Multidimensional Self-Concept Scale (MSCS; Bracken, 1992) was administered to each participant. The MSCS is a questionnaire containing six subscales each of 25 statements, each of which has four possible alternative answers: Absolutely true (AV); True (V); Not true (NV); and Absolutely not true (NAV). The questionnaire aims to evaluate adolescents’ self-concept in six areas: social (e.g. ‘I like most people’, α = .82), competence (e.g. ‘I’m too lazy’, α = .78), affect (e.g. ‘Lots of things scare me’, α = .81), academic (e.g. ‘School work is hard for me’, α = .91), family (e.g. ‘I feel appreciated by my family’, α = .91), and physical (e.g. ‘I’m attractive’, α = .85).
Emotional experiences
A qualitative instrument composed of four open-ended questions assessing the emotional experience of the stay in hospital was administered to each adolescent with CI. Specifically, following Corsano et al. (2012), each participant was asked to describe an event or encounter at the hospital during their CI activation where he/she felt scared, happy, angry, and sad, respectively. Each adolescent provided four stories that were then analyzed, counting the number of emotional terms and the number of medical terms across the four types of stories.
Procedure
All instruments were administered individually by members of the research group between October and December 2015, during the follow-up to the adolescents’ stay in hospital, within the Otorhinolaryngology Operative Unit at ‘G. da Saliceto’ Hospital in Piacenza (PC, Italy), and in three different schools in the North of Italy. In each case, the procedure lasted about 40 minutes and each participant was assured that they would receive all the assistance and clarification they might need.
Results
We considered statistical differences in socio-emotional development between the CI and the TD groups by means of a series of t tests for independent samples. Then we assessed the statistical differences between children with CIs (early and late activation) using t test for independent samples. Then, we considered the relationships between emotional competence expressed in the stories and socio-emotional adjustment using correlational analysis.
Group differences in socio-emotional adjustment
Descriptive statistics for the two groups are presented in Table 1. A series of t tests for independent samples was used to assess significant differences between the two groups.
Scores in the MSCS, LACA, and EAS subscales for the two groups.

Note: MSCS: Multidimensional Self-Concept Scale; Loneliness and Aloneness Scale for Children and Adolescents; EAS: Emotional Autonomy Scale; TD group, typically developing adolescents; A-Pos, affinity toward aloneness; A-Neg, aversion toward aloneness; L-Peers, peer-related loneliness; L-Part, parent-related loneliness.
The significant values are reported in boldface.
Across the six dimensions of self-concept, no significant differences emerged between the CI and the TD group. Significant differences between the two groups were found in peer- and parent-related loneliness and aversion but not in affinity toward aloneness. Specifically, adolescents with CIs displayed more peer-related loneliness (t(56) = 2.77, p < .01) and parent-related loneliness (t(56) = 3.70, p < .001) and lower levels of aversion toward aloneness (t(56) = −2.15, p < .05). On separation and detachment, adolescents with CIs displayed lower levels of separation and higher levels of detachment than typically developing adolescents, although the differences were not significant (p = .14 and p = .40, respectively).
In order to test the role of age at CI activation in adolescents’ socio-emotional adjustment, analyses were conducted of the differences between individuals with CI activated at an early age (before 6 years, n = 15) and those with CI activated later (n = 14). Data analysis (Table 2) showed that adolescents who received the CI at the earlier age displayed higher levels of physical self-concept (t(27) = 2.93, p < .01).
Means and SD for the children in the CI group according to their age at CI activation.
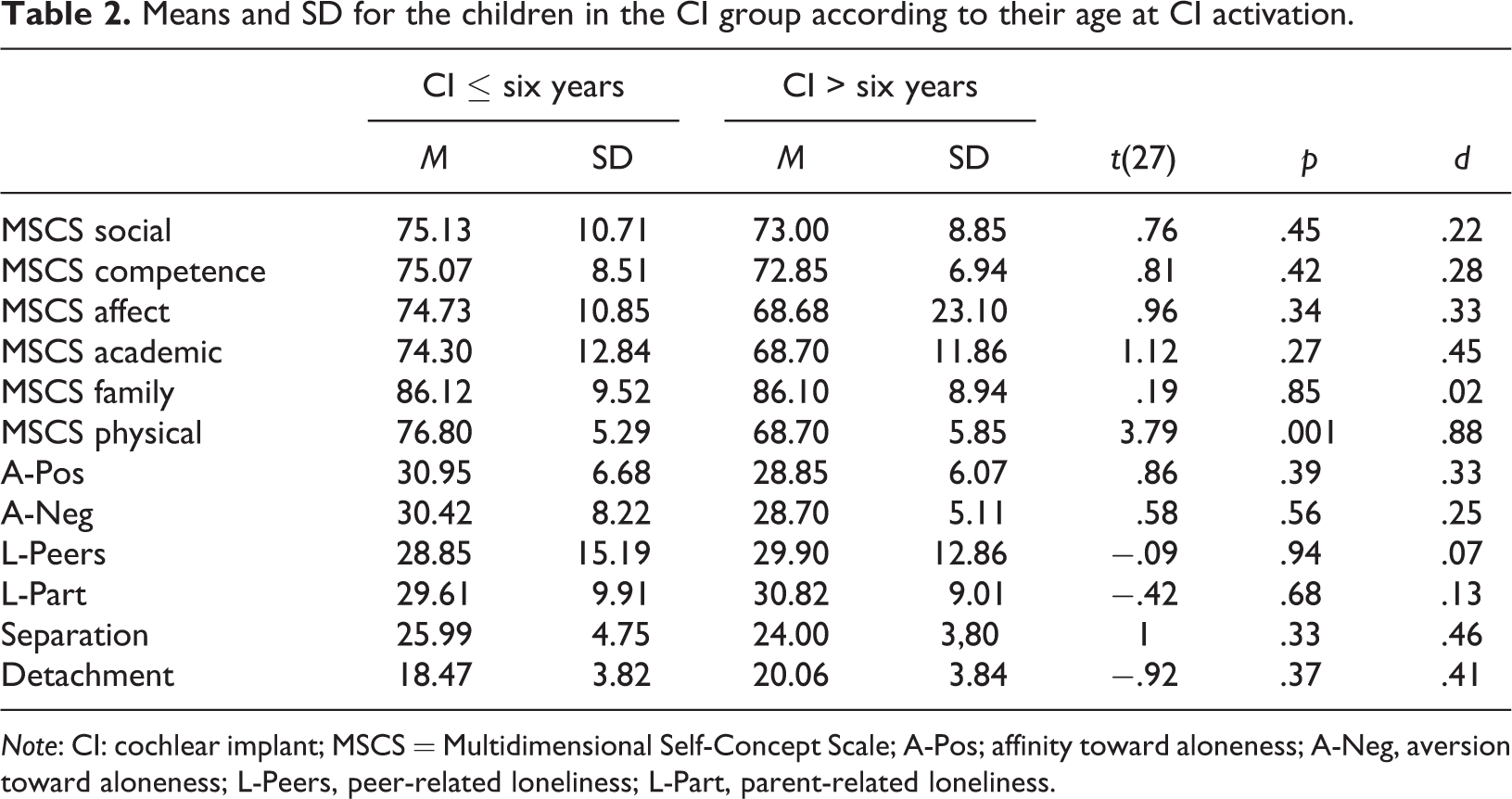
Note: CI: cochlear implant; MSCS = Multidimensional Self-Concept Scale; A-Pos; affinity toward aloneness; A-Neg, aversion toward aloneness; L-Peers, peer-related loneliness; L-Part, parent-related loneliness.
The emotional experience at the hospital of the adolescents with CIs
Most of the adolescents’ stories about their experience at the hospital were quite short and did not have a complex narrative structure. They provided a story for each of four emotions: happiness, fear, anger, and sadness. For each story, the number of terms (both medical and emotional) and the number of words used were counted. Paired t tests showed that more medical terms than emotional terms were produced (t(14) = 3.57, p = .003). Repeated ANOVA measures showed that adolescents with CIs displayed significant differences in the number of words produced relating to the different emotions, F(3, 39) = 5.75, p = .002, n 2 = .93. Paired t tests showed that more words were produced about events in which they experienced happiness and fear than about events in which they experienced anger and sadness (happiness vs. sadness: t(14) = 3.09, p = .001; happiness vs. anger t(14) = 2.40, p = .03; fear vs. sadness: t(14) = 3.33, p = .005; fear vs. anger: t(14) = 2.85, p = .01).
Not all adolescents reported an event for each of the four emotions. Those who did not report an event for a particular emotion said they did not feel that particular emotion during their stay in the hospital (n = 12) or did not remember any particular episode (n = 8). Only one participant preferred not to give an answer about any of the four emotions in the questionnaire: He felt that he had nothing to say about his experience. Examples are reported in Online Appendix A.
Finally, the relationships between emotional autonomy, loneliness, self-concept, and emotional aspects of the stay in hospital were analyzed (the latter by the number of emotional terms produced in the stories) using partial correlation because the time periods between the dates of CI surgery and dates of the storytelling were different, controlling for chronological age. Partial correlation analysis showed a negative correlation between the number of emotional terms and feelings of loneliness toward parents (r(14) = −.61; p = .02). No other significant correlations emerged.
Discussion
Looking first at the results relating to our first aim, socio-emotional adjustment, the results indicated, partially in line with previous studies, no significant differences between adolescent with CIs and adolescents with TD, in some dimensions. Adolescents with CIs displayed similar levels of self-concept and emotional autonomy to those of their hearing peers, but more peer- and parent-related loneliness and less aversion for aloneness. The results confirmed that, especially regarding their relationships with others, adolescence may represent a particularly difficult period for adolescents with hearing problems, who are aware of being at a disadvantage relative to their peers (Tomassini, 1999). Several studies have indeed indicated the difficulties that adolescents with hearing problems encounter, including difficulties in developing friendships with hearing peers, lower levels of social competence, increased levels of loneliness (Most et al., 2012), and lower conversational skills, which can lead to difficult interactions with others (Bat-Chava et al., 2014). As regards the lower level of aversion toward aloneness, perhaps adolescents with CIs feel less negative about being on their own because they are more used to it and so, perhaps, it does not loom large as a problem. It might also be that they are able in a way to rationalize their difficulties in social relationships (Goossens et al., 2009) because they feel more alone. Although adolescents with CIs displayed more loneliness, their self-concept and emotional autonomy were not different from their hearing peers. This reflects the fact that socio-emotional development in this population is both complex and highly variable internally. A comparison of the results on this sample with other findings on adolescents with learning disabilities (Majorano et al., 2017) indicates that both the groups display higher levels of peer-related loneliness, confirming that social relationships might be particularly difficult for adolescents with disabilities or developmental difficulties and that loneliness could be a risk factor for these individuals.
Turning to the second aim of the work, related to self-concept, an interesting datum emerged specifically on the age at CI activation. Individuals who received the CI early displayed a more positive physical self-concept. In line with previous studies, early implantation could be a factor that implies considerable improvements not only in cognitive and linguistic development but also in the socio-emotional domain, such as relational skills and self-concept (Mance and Edwards, 2012; Moog et al., 2011; Warner-Czyz et al., 2015). The interesting aspect of the present study is that the only significant difference between adolescents with CIs and their peers was the physical dimension of self-concept. In line with other studies (Celli, 2014), these findings support the idea that activation of the CIs after the preschool period could be one critical factor in the construction of identity and physical self-concept, especially in relation to the redefinition of body image; by contrast, CI activation in early infancy could allow individuals to better represent the transformations associated with the activation of the implant and to deal with them more easily.
With regard to the third aim of the study, the emotional experiences of the adolescents with CIs during their stay at the hospital for surgery appear to be rather complex. The results indicate a small number of events related to anger and sadness and a significantly greater number around fear and happiness. Furthermore, it was shown that participants who reported a greater number of emotional terms presented lower levels of loneliness toward their parents, which might indicate positive perceptions of support by, and relationship with, their parents. However, this is a fairly complex route because after diagnostic investigation the family can find the role of processing and accepting the diagnosis difficult (Vallarino et al., 2014).
Implications for practice and limitations of the study
The present study could have one important implication for practice: the emergence of the importance of support for the socio-emotional adjustment of adolescents with CIs, especially the role of parents who, along with medical staff, could play an important role in supporting their children during their hospital stay. Better assessment of, and fuller consideration of, the socio-emotional aspects of this experience for adolescents with CIs could prevent long-term maladjustment.
The study has, however, some important limitations. First, the sample is small and is limited to a specific region; it could therefore be considered a preliminary analysis and future research could extend the results using a larger sample that also included cultural differences. Second, the present research is based on self-reports and a major improvement in future studies would be the use of a multi-informant design: The perceptions of parents of children with disabilities will be valuable, especially those who have a negative representation of their child’s competence. Finally, the present study could be extended to other groups of adolescents with learning disabilities or difficulties with similar characteristics.
Supplemental Material
Supplemental Material, jchc-2017-0077-File005 - Socio-emotional adjustment of adolescents with cochlear implants: Loneliness, emotional autonomy, self-concept, and emotional experience at the hospital
Supplemental Material, jchc-2017-0077-File005 for Socio-emotional adjustment of adolescents with cochlear implants: Loneliness, emotional autonomy, self-concept, and emotional experience at the hospital by Marinella Majorano, Marlies Maes, Marika Morelli, Tamara Bastianello, Letizia Guerzoni, Alessandra Murri, and Domenico Cuda in Journal of Child Health Care
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.