
Abstract
While cross-respiratory infection guidelines reduce the risk of infection, this may have deleterious impacts on the socialization skills of young people living with cystic fibrosis (CF). The purpose of this study was to explore the experience of social isolation among young Canadians with CF, as well as how they navigate these complex contamination restrictions. The thematic analytic qualitative research tradition was adopted and social theories of risk provided theoretical grounding. The youth described a pressing sense of social isolation in their everyday lives. Although most of the youth ‘obeyed’ the cross-contamination guidelines, some demonstrated a more carefree attitude. Social media was employed across the group as a tool to reduce isolation. In accordance with the sociology of risk, youth with CF demonstrate sophisticated decision-making abilities, navigating exceedingly difficult choices to preserve an always-precarious future. While necessary, cross-contamination guidelines might further marginalize an already isolated group of children and youth.
Introduction
When cystic fibrosis (CF) was first described in the 1930s, over 80% of babies died within the first year of life (Congleton et al., 1996). Dramatic advances in medicine, science, and treatment technology have improved the life expectancy of CF patients today. In Canada, for instance, the median age of survival is 50 years (CF Canada) and the disease is no longer considered one of childhood. Despite improved life expectancy, people with CF face enormous psychosocial challenges in the management of the disease. The experience of social isolation in CF is a poorly researched aspect of the illness. Arguably, the cross-contamination guidelines that were ushered into the Canadian health-care landscape in 2003 (Saiman and Siegal, 2003) have worsened the experience of social isolation among young people with CF.
Here, it is necessary to discuss the social context of cross-respiratory infection guidelines in the care of young people with CF. Social support from peers is a critical source of socialization not only for young people with CF but for all children and youth (Craig et al., 2010; Lewis et al., 2016). Specifically, peers may serve as protective factors for young people with chronic illnesses by normalizing their experiences and providing emotional support (La Greca et al., 1995). Historically, people with CF enjoyed rich social opportunities to interact with one another. For example, CF camps had a long history in Southern Ontario in the late 20th century (Rubin, 1991). These camps provided opportunities for social interaction and bonding and promoted a shared understanding about the illness. The social context for CF patients dramatically changed approximately 10 years ago. At this point, researchers found that when CF patients interact with one another in close proximity, there is a slightly greater risk of cross-respiratory infection (Saiman and Siegel, 2003). This scientific finding had a profound impact on the best practice guidelines in the care of CF patients. CF camps are now closed (Reijden et al., 2008). Further, shared waiting rooms in hospitals are discouraged and patients are asked to wear masks when they are in close proximity (CF Canada). Social support groups and group-based research activities have also ceased. Thus, patients are now deprived of the critical socialization opportunities that they were once free to enjoy. CF patients are still encouraged to interact normally with non-CF peers, including other youth with chronic illnesses. Arguably, these restriction guidelines might have particular implications for the lives of young people with CF. However, to date, the lived experience of isolation has not been explored. CF patients might suffer from social deprivation on account of not being able to interact with others who are just like them. In contrast, since interaction with non-CF peers is encouraged, they might still enjoy a normal social life with non-CF peers.
I attempted to elucidate how CF patients have been impacted by these guidelines in the context of their everyday lives. Since the clinical guidelines which prevent people with CF from socially interacting with one another are novel, the lack of research on the experience of social isolation is not surprising. Indeed, a sense of isolation may further damage health among people with chronic illnesses (Hawkley and Cacioppo, 2003). Therefore, exploring the topic of loneliness in CF is arguably an important task. In this article, the experience of social isolation in young people with CF in Canada was investigated, with a particular emphasis on how they negotiate cross-respiratory infection guidelines in the context of their everyday lives.
Review of the literature
Scholars have long since recognized the importance of peer relationships to the development of a healthy self-concept in children and youth (Laursen et al., 2007). While social participation is a measure of a child’s inclusion by their peers, social isolation is an index of social exclusion and refers to the number of negative social engagement experiences that a child has. Since social interaction is a critical component of optimal development, social isolation can profoundly disrupt a youth’s developmental trajectory (Laursen et al., 2007).
To examine the topic of social isolation in CF, a review of the literature was undertaken by entering relevant keywords into five academic databases at the University of Toronto including Sociological Abstracts, Psych Info, Ovid Medline, Scopus, and Web of Science. Since scant literature exists on the topic, no date range was set, resulting in articles from the 1980s until the present day. The review yielded nine studies and theoretical position papers that met inclusion criteria.
With the exception of two studies in which levels of social isolation were no higher in patients than mothers (Geiss et al., 1992) or healthy controls (Yarcheski et al., 1987), most authors report a pressing sense of social isolation among young people with CF (Boyle et al., 2001; Congleton et al., 1996; Grossoehme et al., 2012; Wilderman, 2005). Some authors suggest that social isolation diminishes over the course of time as patients and families come to adjust to the demands of the illness (Grossoehme et al., 2012). Other researchers have found that CF patients might be better able to handle social isolation in comparison to other young people with chronic illnesses. This might demonstrate the inherent resilience of the CF population (Tierney et al., 2008). Some authors report worse social isolation among young men with CF in comparison to young women. Women’s more robust social networks and effective problem-solving abilities might account for gendered differences in the felt sense of isolation. However, caution is needed when interpreting Congleton et al. (1996) result. The study was conducted before the implementation of cross-respiratory infection guidelines. Therefore, the social isolation that these patients felt is likely qualitatively different from the participants in the current study. Thus, most authors report that social isolation is a frequently encountered problem among young people with CF.
A few research teams developed online interventions to ease the burden of social isolation (Christian and D’Auria, 2006; Johnson et al., 2001). In general, these online interventions are associated with increases in social support among members of the CF community (Johnson et al., 2001). These interventions are likely effective since they promote a shared understanding over common issues.
With the exception of cross-sectional studies where results are mixed, most researchers have found a higher prevalence of social isolation among people with CF and their caregivers. Online interventions are generally effective in reducing social isolation. However, while some researchers have theoretically discussed the impact that cross-respiratory infection guidelines may have for people with CF, thus far, there is no empirical research on how young people with CF take up and negotiate these guidelines in the context of their everyday lives and most of the evidence is quite outdated. Informed by theories of risk, two questions were explored in this study: What is the experience of social isolation among youth with CF? And, how do youth with CF take up, make sense of, and negotiate cross-respiratory infection guidelines in the context of their everyday lives?
Research design
After receiving funding from the Children’s Hospital Research Institute of Manitoba, this study was approved by the Research Ethics Board at the University of Manitoba. The original intent of this study was to explore the experience of social isolation in the CF community in Canada and to investigate how the cross-respiratory infection guidelines are negotiated by patients, parents, and caregivers. Although 13 participants enrolled in the parent and caregiver component of the study, in this article, only child and youth findings are reported. Since patients and parents/caregivers negotiate social isolation in dramatically different ways, the decision was made to present parental findings in a second article.
To aid in recruitment, a national call for participants was made using the Cystic Fibrosis Canada website, Facebook page, and Twitter feed. Given that CF is a rare genetic disease and that it is generally difficult to recruit participants for studies, broad inclusion criteria were employed. Medically stable patients with CF between 10 and 30 years were included. After the national call was made, interested participants and families from all over Canada contacted the researcher directly via email or phone to express interest. The consent process was explained to all potential participants. Patients who were over 18 signed their own consent forms. For patients under 18 years, the consent was obtained from parents in the form of parental consent. This is the process in place at the hospital in which the study was conducted. To facilitate this, the consent was explained to the primary caregiver. At this point, if the caregiver was interested, they asked their child if they wanted to participate and the consent was obtained from the child. Convenient interview times were arranged for each participant.
Method
According to Braun and Clarke (2006), thematic analysis is a qualitative research tradition used predominantly in the social sciences and humanities. It is a framework that is used for the conceptualization of knowledge and the analysis of data. While thematic analysts differ in their epistemological viewpoints, in this study, Braun and Clarke’s (2006) interpretivist notion of reality was adopted. Thematic analysis is also a way of systematically identifying, coding, and deriving inductive themes through a data set.
Theoretical framework: Cracks in the medical edifice
This study was theoretically informed by conceptual tenets from the sociology of risk (Bendelow, 2006; Morden et al., 2012, 2015; Wasserman and Hinote, 2011) in an attempt to understand how young people with CF negotiate cross-respiratory infection guidelines in the context of their everyday lives. A few conceptual postulates from this theoretical framework are relevant to the case of CF.
Modernist medicine was based on a total investment in doctors who were regarded as omnipotent bearers of truth, that is, ‘experts’ on the illness experience (Wasserman and Hinote, 2011). However, in the postmodern society—in which there is growing critique over taken for granted ‘truths’—health risks are regarded as dubious and incalculable. Indeed, there is a growing sense of skepticism toward the medical profession. Furthermore, in postmodernity, there is less emphasis placed on expert knowledge and a growing appreciation for the importance of listening to ‘lay’, or everyday, health experiences. Indeed, in the chronic disease era, patients are more critical of medicine’s promises and limitations and often adopt other health models based on lay experience, personal context, and everyday life (Morden et al., 2015). Specifically, there is growing recognition that people do not always act as rationale actors who calculate and summate risk odds and act accordingly upon them (Morden et al., 2012). Rather, individuals might not see themselves as at risk, and come to regard other issues as more important in their lives. For young people with CF, this might mean that there is a growing appreciation for the importance of listening to lay experiences of illness that emanate from the CF community. Furthermore, these conceptual tenets illustrate that young people with CF might not simply disregard infection protocols because medical doctrines deem them as ‘risky’. Rather, young people with CF might navigate these restrictions in ways that make sense to their everyday lives. Additionally, in the past, modernist medicine was based on the notion of diagnostic certainty, medical calculability, and the search for effective treatment protocols (Wasserman and Hinote, 2011). However, since CF is an enduring condition for which there is yet no cure, the structure of modernist medicine is no longer structurally compatible with many of the ongoing chronic illnesses of our current time such as CF, lupus, and chronic fatigue syndrome to name a few. These theoretical postulates might aid in understanding how the CF community negotiates cross-contamination restriction risks.
Recruitment and participants
Nine children and young people with CF participated in this study, including one male and eight females. Participants resided in the provinces of Ontario, Manitoba, British Columbia, Quebec, and Alberta. Age ranged between 10 and 24 years. Patient participants were mainly Caucasian of mixed socioeconomic background. Although objective indicators of health were not obtained in this qualitative study such as lung function parameters, according to self-report, the degree of illness severity among youth greatly varied (Table 1).
Participants.

Data collection
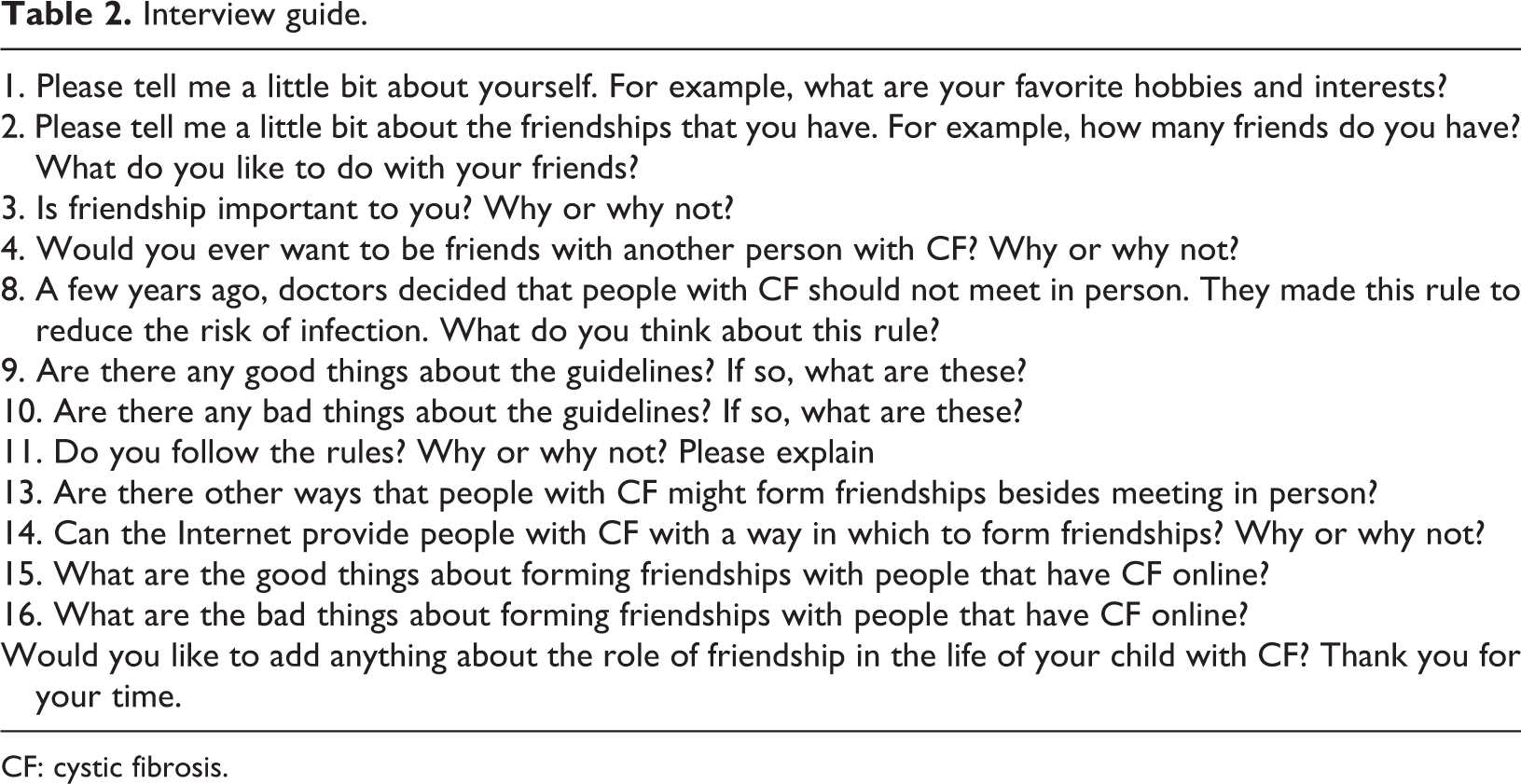
Qualitative semi-structured interviews were the primary means of collecting data. The interview guide was based on the existing literature and clinical observations (Table 2). Convenient interview times were arranged for all interested participants and I conducted all of the interviews. Interviews for participants residing in Manitoba were conducted at the Children’s Hospital Research Institute of Manitoba. Interviews for participants residing outside of Manitoba were conducted over the phone. Interested readers should email the author to get a copy of the interview guide.
Interview guide.
CF: cystic fibrosis.
Data analysis
The interviews were audiotaped and transcribed verbatim by a research assistant. The transcripts were read multiple times to become familiar with the data. After this in-depth reading activity, each transcript was read individually, with the view toward coding recurrent patterns of meaning in each individual transcript. Initial code names were given to recurring patterns of meaning. This method was conducted on each individual transcript. At the next level of coding, common patterns of meaning were grouped together within the entire data corpus. When a novel code arose in a new transcript that was not observed in previous transcripts, new code names were developed. Themes were refined by ensuring conceptual clarity which entailed making sure that theme content was reflective of theme names. Although the data were not deductively coded, attempts were made to add explanatory and interpretive power to the findings by considering the theory (Braun and Clarke, 2006). Disagreements between the readers arose in two cases. These were dealt with by discussing the disagreements and developing consensus. The findings are presented subsequently and pseudonyms have been used.
Findings
The participants described a pressing sense of isolation in their everyday lives on account of both having CF and not being allowed to interact with others that have the same condition. When navigating the cross-respiratory infection guidelines, most participants ‘followed’ the rules by restricting their access to others with CF. However, other patients ‘broke the rules’. They felt that restricting themselves from others with CF was an unnatural and excessive way to live. Regardless of whether they were rule followers or rule breakers, all participants felt that social media played a beneficial role in their lives, serving to break and diminish isolation.
All alone
Participants often described ‘feeling lonely’ and isolated—or that they were the only ones with CF. Some participants were old enough to recall what clinical practice was like before cross-contamination guidelines were implemented. While they understood that a change in practice was necessary to ensure patient safety, this often made them feel isolated and alone. Mikayla is in her early 20s and has an identical twin sister with CF. She explains that the change in clinical practice since she was a child has greatly intensified her experience of isolation: It can be really isolating. I do kind of miss clinic because I never had CF camp, but when I was younger, clinics involved, you would kind of all sit in one waiting room and then, you went into the clinic. Like you could kind of mill around in the hallways and stuff and that has changed, because now they have a thing, especially my clinic, where you just stay in the one room and then all the doctors and pharmacists and everything come to you which to me is, you don’t really get to see anyone else who’s there, so it kind of just feels like you’re the only one there. And it can be isolating. I mean it’s an internally isolated, like I don’t feel I have no friends or family that I can rely on but I do feel isolated ya, to some extent. I guess it’s like the, what I was talking about earlier with the big mental disconnect. I just really noticed it. It’s like if someone was talking about, is it like a conversation about oh, like I don’t know, “where do you see yourself in 10 years or like what are your long term goals”? Even that kind of stuff where I really feel like…my life experience is very unusual, and it makes me feel disconnected sometimes, from like people in my life. Isolation is bad for your mental health. You know for mental health and stuff like that sometimes it can be a bit of a bother. Well I mean a part of me does want to be more social with other people, but, I mean, for my mental health. I think the disadvantages are feeling isolated and feeling like you can’t connect to other people because of your disease. You can’t attend social functions related to CF where there might be somebody else there…I know a lot of people don’t necessarily adhere to them (rules), just because they feel like it’s not, it’s not worth it. We would be friends but like, it’d be hard because we can’t really be friends like because she also has the disease the same thing and we can get more sick if she has a cold. If she didn’t know what CF meant, I would try to help her understand.
Navigating risk
The participants carefully negotiated cross-respiratory infection guidelines in the context of their everyday lives. Some of the older participants with CF—in their early 20s—were old enough to recall what clinical practice was like before the implementation of these guidelines. Other participants vividly recalled the social, interactive nature of medical appointments in the CF clinic before the guidelines were implemented. The two central ways that participants navigated risk—by either being a rule follower or a rule breaker—are described subsequently as subthemes.
Rule followers
The majority of the participants made the decision to follow the restriction guidelines. They demonstrated adherence to them because they did not want to undertake any action that might expose them to greater medical risk or hasten mortality. Some rule followers understood the reasons as to why other CF patients might hedge their bets and throw caution to the wind. They demonstrated a level of empathy toward others who might choose a different course of action from themselves. Other participants expressed scorn—almost a judgment of sorts—against rule questioners, believing them to be irresponsible and reckless with their lives and others. For example, Sophie questions why anyone with CF would do anything to further harm their health and expose others to risk in the process: I think that honestly, we go through enough setbacks that putting ourselves at risk, whatever that risk might be, but you’re acquiring something or you’re passing something on to someone that you care about, you know I don’t think that’s quite worth it. Well, I think that I believe when the guidelines came out, I was thick into my molecular genetics degree biology courses, microbiology, so I really understood the science, and I’ve always had a really good relationship and a high level of trust with my doctors as well, so just those things combined. I’m older. I see a lot of people in bad spots and I see people putting themselves in bad spots, and then you know…Everybody’s an adult, they have a choice to make whether they want to spend time with other CF’er’s or not. Or be close or not be close or have relationships with like, not just friendship relationship. And so as you watch those things, and then you see the results of what can happen in those situations.
Questioning the rules
Other participants felt that the restriction guidelines were ‘excessive’. While they did not purposively go out of their way to meet other people with CF, they demonstrated a ‘lax’ or relaxed attitude toward the rules. These participants felt that the rules were somewhat unnatural and overly complicated. They felt that quality of life and social health was perhaps more important than purposefully arranging one’s life to avoid interacting with other CF patients.
Thirteen-year-old Charlotte explains the current setup of the CF clinic which does not allow for social interaction with other participants. She acknowledges that this creates greater social isolation during clinic appointments and prevents friendship building: The bad things I guess you feel like you can’t make a friendship or something…like um, if you’re in hospital or whatever, when you go out to the hall you have to wear a mask and like, everything like that. Your rooms are like on the total opposite sides of the hall and stuff (as other people with CF). So I feel like the rules, they really suck. I actually don’t know of another chronic disease where people with the chronic disease can’t fucking talk to each other. It’s ridiculous. And I know, like back in the 90’s they had to shut down all these CF kids camps like it’s just terrible, and it’s already, it’s such an isolating disease anyway. You can’t control every situation, you can’t control every environment that you’re in and, just accepting that. And knowing that what’s meant to be is going to be and, you just take reasonable precautions that you see fit, and that’s how you live your life. I think information about infection is always good, and like I said obviously there’s science backing this. But I don’t think they’re making those policies for fun or anything. But I think that they need to give people the choice in their own lives.
Online spaces: Connecting across time and space
The participants frequently employed social media as a tool to reduce social isolation. Social media allowed participants located at great geographic distances to build new relationships. Participants joined private Facebook groups with others across the globe as their central forum for social media exchange. Other participants used Instagram, chat rooms, and Facetime to connect with others.
Annabelle participates in a private Facebook group which consists of both young women and young men with CF. Sharing an online space with others that have CF has made her realize that the disease is broader than just herself. In the group, Annabelle and her friends talk about ‘good days and bad days’ (Charmaz, 1991). Interestingly, this is the title of the infamous book by Kathy Charmaz on the lived experience of chronic illness. Just knowing that it’s not just you, it’s not just your family like, it’s happening to other people. Which weirdly does make you feel better. It’s bigger than me. It’s more, and not bigger but like, more interconnected, like even though we can’t hang out face to face, we can sort of, like make a bit of a community with CF? And I know, like my friend, the one I’m talking about, she actually sends Facebook chats for me and Mikayla and her, and also a couple of other guys that she knows who have CF, and we all just kind of like talk and check in and be like “oh man this great thing is happening or like this shitty thing is happening”. Creating support groups for places to ask questions is important, or, um places to give feedback to other people but, with those, you’d have to kind of, you’d have to go in and, give as much as you can expect to get back, like you have to be brave enough to go on there, and ask a question. I maintain my connections to the girl I knew in British Columbia with CF. I’d say the advantage there is, is just, kind of hearing how she’s doing. It’s strange like knowing that there’s someone else that’s going through the same thing you’re going through and how are they doing, and if they’re doing well, it kind of gives you hope and sometimes if they’re not doing so good, you can feel bad if you’re doing good, or maybe you just feel scared that you might not do good or, things like that. Ah, maybe you could have like a, group chat thing. You could have questions for each other, if you wanted to, see what other people do and stuff. “Oh, I’m having trouble fitting this in with what you guys do”? And stuff like that, just trying to get other’s opinions. Or like if they’ve never been hospitalized before and they want to know kind of what to expect they could ask what other people have done.
Discussion
In this study, the experience of social isolation among young Canadians living with CF was investigated. Other investigators have not explored the realities of isolation in the wake of the relatively new cross-contamination guidelines that were implemented in 2003. Indeed, although researchers have identified the importance of peer support for young people with chronic illnesses (Craig et al., 2010; La Greca et al., 1995), the experience of social deprivation after the implementation of the cross-respiratory infection guidelines has yet to be explored. Further, while clinicians and researchers believe that online social support is critical to the development of young people with chronic illnesses (McKenna and D’Alasandro, 2011), there is little empirical research on this topic.
Due to the cross-respiratory infection guidelines, the participants often felt isolated in their everyday lives. This experience appeared to be slightly different for older and younger participants. Older participants felt internally isolated. By this, they felt a strong sense of ‘disconnection’ from same age peers, or the feeling that others would not be able to relate to the rather bizarre experience of having to isolate themselves from others with the same lived experience. Internal isolation led to feelings of difference, the sense that one’s life was neither usual nor ordinary. Older participants also felt ‘mentally drained’ by social isolation and often contemplated whether obeying the rules was worth the cost. The nature of social isolation for younger participants appeared to be qualitatively different. Younger participants recognized the impossibility of ever having a ‘real’ friendship with another person with CF because doing so would either ‘make her sick or make me sick’. Indeed, younger participants already doubt the authenticity of friendship with other ‘CF-ers’, are aware that having a friendship can make them sick, and interpret getting sick or making others sick as ‘bad’.
Researchers have not examined how youngsters with CF feel about cross-respiratory infection guidelines or the differences in how these messages are interpreted across different developmental stages. The strict adherence to medical doctrines demonstrated by the younger patients might already speak to the infiltration of medical discourse into their everyday lives. Further, it appears that knowledge about cross-respiratory infection guidelines changes across the developmental continuum of adolescence, from early to late stages. Characteristic of ‘normal’ developmental progression, younger patients with CF do not appear to question the merit or truth value of these medical restrictions. In stark contrast, older youth with CF demonstrate abstract reasoning about their predicament (Piaget, 1972). They have developed a sophisticated critique of the guidelines and are able to speak to both the necessity and the harm of this practice. Future researchers might wish to investigate developmental differences in how cross-respiratory infection guidelines are interpreted across the youth continuum.
Most of the participants chose to ‘live by the rules’. In so doing, they did not want to take any action that might worsen their prognosis—or, worse—hasten their mortality. In an ethical mandate of sorts, they did not want to take an action that might harm themselves or others. Rule followers, however, did not blindly permit medical discourse to circumscribe their lives. Some rule abiders had developed a sophisticated critique of the medical doctrines that governed their lives. Further, rule followers demonstrated varying reactions toward rule questioners. Some were able to empathize with other participants and understood that feelings of isolation might prove to be too much to bear. Other rule followers adopted a somewhat more judgmental, scornful stance toward rule transgressors. They described rule breakers as irresponsible, dangerous, and somewhat reckless in their actions. There were only a few rule questioners in the study. These participants did not purposefully go out of their way to socially interact with other youth. However, they appeared to live their lives in a less ‘black or white’ fashion, demonstrating a greater degree of laxity. They did not worry excessively when bumping into another CF patient at the clinic or a community event. They knew that from a historical perspective, people with CF have interacted for far longer than they have been isolated. Further, they felt that the rules were excessive, unrealistic, and also unfair given the extra planning that was required to purposefully avoid interacting with other youth.
These findings can be analyzed within the context of the literature. It appears that the negotiation of cross-respiratory infection guidelines is an ongoing, dynamic process, rather than a one-time, discrete event. Further, the negotiation of rules is enormously complex. Following a distinct course of action—not meeting others with CF—did not preclude thinking about alternatives and reflecting on the choices that others made. Most importantly, based on this finding, it is possible to make critiques of risk theory.
Social theorists of risk often purport how risk discourse infiltrates all aspects of social life. Further, risk theorists explain how risk discourse has resulted in a ‘moral panic’ around health issues. As health actors, people constantly fret over our exposure to risk and take actions to live less risky lives. Risk discourse—embedded within biomedical discourse—is also flavored with moral connotations that carry notions about good and bad behaviors. Thus, those that engage in risky behaviors that harm self and others are often constituted as morally flawed (Wasserman and Hinote, 2011). In this study, the adoption of risk discourse was incredibly complex and nuanced. In contrast to its presentation in many kinds of literature, participants did not uncritically adopt risk discourse with little thought or reflection. Some participants adopted risk discourse by following the rules, but reflectively and empathetically demonstrated understanding toward those participants who refuse to feel further imprisoned by CF. A few participants adopted risk discourse uncritically, expressing little reflection on the guidelines and outright scorn for those whose actions hurt an already vulnerable group of participants. Still, other participants actively resisted risk discourse. They pointed to the historically and culturally changing nature of the best practice guidelines and felt that purposefully avoiding other people was ultimately an excessive, black and white, and unnatural manner of living. Clearly, future research is needed on the navigation of risk in the context of everyday life for youth with CF. However, it is clear that the adoption of risk discourse is neither clear nor uniform; youth demonstrate complex and varied responses that make sense in their context of their daily lives. The factors and processes that predict whether one becomes a rule breaker or rule questioner require more investigation. For instance, youth with CF who are more embroiled within the medical domain might be more willing to follow the rules.
Scholars have discussed the impact of technology on people with chronic illnesses (Greene et al., 2011). However, only a few research teams have explored the role of social media in the lives of patients with CF. In this study, participants frequently used a range of social media platforms as a forum to reduce the experience of social isolation. While Facebook was the most commonly used platform, the participants also used Instagram, websites, chat rooms, and Facetime. In most cases, social media was used as a way to connect with other ‘CF-ers’ in the global community regarding shared issues. During times of hospitalization, participants used live chats such as Facetime to remain connected with non-CF peers outside of the hospital. In this regard, social media use was extremely extensive in the lives of youth with CF and broadly employed for a number of different purposes.
McKenna and D’Alessandro (2011) suggest that technology is a ubiquitous facet of the lives of millennials as well as those who come after. Hundreds of chronic illness groups use social media to engage in dialogue and communication about illness- and non-illness-related issues. McKenna and D’Alessandro (2011) encourage researchers and clinicians to integrate technology into health-care interventions for children, lest our work becomes obsolete and unable to keep pace with modern childhoods. Since technology is a normative part of their lives, another research team describes young people with CF as ‘digital natives’ (Dale et al., 2016). For youth with CF, online spaces might play an even more important role in their lives. Participants felt that social media was an important tool to sidestep social isolation in the CF community. Researchers and clinicians should recognize the value of social media for youth with CF given the context of cross-contamination guidelines. Special efforts to incorporate media and technologies should be made when creating new studies, programs, and interventions (McKenna and D’Alessandro, 2011). Specifically, in practice settings, clinicians might promote and encourage patients to utilize online social media platforms as mechanisms to reduce social isolation.
However, the participants did not uniformly enjoy technological use with other youth. Indeed, most participants suggested that technology is only ever a ‘second best’ and cannot replace the value of ‘real’ relationships that unfold in person. Further, learning that another CF patient had fallen ill or passed away was, in general, very upsetting for group members. Illness and death in the online CF community not only marked a change in online friendships but also served as a reminder of one’s own mortality. Indeed, for participants who preferred an ‘I don’t want to know’ approach to dealing with CF—a passive denial or avoidance of sorts—learning of another persons’ suffering and deterioration was quite traumatizing. In this way, researchers should recognize that while technology can be enormously helpful in the lives of youth with CF, it is not without the potential for harm.
Limitations
Despite the effort to recruit a broad range of people with CF, eight females and one male participated. Thus, the findings might reflect the experience of social isolation among females with CF. Males with CF might face particularly gendered aspects of social isolation such as the cultural expectation to not display their emotions. In the future, researchers should continue to investigate how social isolation is experienced by young men with this condition. Further, it was exciting to talk to patients who were old enough to recall their lives before the implementation of the contamination restrictions. However, in order to fully elucidate the experience of isolation pre- and post-contamination restrictions, in the future, it might be important to study homogenous groups who either did or did not experience the change in clinical practice.
The complexities of contagion: Conclusion
Today, people with CF are discouraged from interacting socially given a greater risk of cross-respiratory infection. These rules are important for the CF community and are widely adopted. However, arguably, to better understand the social worlds and lives of youth with CF in a global context, it is important to investigate the social–psychological ramifications of the guidelines in the wake of this advancement. The findings illustrate the complexity of contagion—or the complex ways in which children and youth with CF live their lives in the wake of yet another barrier imposed by their illnesses. They do not uniformly or uncritically adopt the rules and instead illustrate profound intelligence, reflection, and insight as they navigate what continues to be one of the most challenging illnesses of our time to treat.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank the Children's Hospital Research Institute of Manitoba's Small Grants Program for funding this study.