
Abstract
Few studies have described the various reasons for unplanned transfer to a higher level of care due to clinical deterioration and the clinical profile of those paediatric patients. However, an understanding of the nature of illness is important to patient safety. This study aimed to describe the frequency and clinical characteristics of children who experience unplanned transfer to a higher level of care due to clinical deterioration. A retrospective, descriptive registry study design was used. Of the 92 paediatric patients included, 69% (n = 64) was male. The median age was 2.1 years (interquartile range 0.4–6.9) with 33% being infants under 1 year. The highest number (61.3%) of transfers occurred between 8 and 16 hours. In the 24 hours leading up to a transfer due to clinical deterioration, 15 patients had no vital parameters documented, and 77 patients had least one vital parameter measured. Physiological abnormalities were present in 19 (37.7%) of the 77 patients where vital parameters were documented. This study provides essential baseline data to inform further research to improve care and treatment for critically ill children in paediatric wards. This study’s findings suggest reporting of vital parameters is incomplete and infrequent.
Keywords
Introduction
International studies show that 8.5% to 14.0% of cardiac arrest incidences outside intensive care units involve paediatric patients (Nowak and Brilli, 2007). Survival is only between 15% and 33%, with subsequent significantly poor neurological outcomes in 35% of the surviving children (Robson et al., 2013; Pearson, 2008). In acute healthcare settings, an increased acuity of care as well as higher technology dependency has been seen, with an increased risk of paediatric cardiopulmonary arrest and its associated mortality (Robson et al., 2013). If signs of deterioration in a child are not identified at an early stage, it has an implication on the financial costs for the healthcare system (Duncan and Frew, 2009). Furthermore, the devastating psychological effects that admission of a child to a paediatric intensive care unit (PICU) has on families is well documented (Balluffi et al., 2004). Thus, there is a need to improve early recognition, care and treatment for hospitalized children.
Symptoms of deterioration can be detectable 24 hours prior to a critical event (Pearson, 2008; Robson et al., 2013). Thus, clinical deterioration, unplanned transfer to higher level of care and even death may, in many cases, be avoidable or potentially avoidable (Balluffi et al., 2004; Pearson, 2008; Robson et al., 2013). Paediatric early warning systems (PEWS) have been identified as a means to improve safety for hospitalized children (Pearson, 2008). PEWS is a scoring system based upon simple bedside observations, such as respiratory rate, blood pressure and capillary refill time, providing clinicians with a tool to support early recognition and intervention, helping to identify children at risk of deterioration, providing the clinicians with guidelines for actions and a level of observation (Duncan, 2007; Parshuram et al., 2011). Since PEWS is based upon measurement of vital parameters, there is a need to gain information about the level of nurses’ observations to improve patient safety. Few studies have described the various causes of unplanned transfer to a higher level of care due to clinical deterioration and the clinical profile of those paediatric patients (Krmpotic and Lobos, 2013; Rady, 2014). An understanding of the nature of illness is also important for further improvement of quality of care to seriously ill children.
The purpose of this study is to describe the frequency, clinical characteristics and outcome of children who experience unplanned transfer to a higher level of care due to clinical deterioration and to determine the adequacy of monitoring in these children prior to their deterioration.
Methods
Design
A retrospective descriptive registry study describing a one-year period from 1 January 1 2013 to 31 December 2013. This study is part of a larger study exploring paediatric early warning score models (Jensen et al., 2017a, 2017b, 2018). The present study was conducted before PEWS was implemented in the included hospitals.
Study setting
The study utilized a registry including four hospitals (three regional hospitals, one university hospital) in the Central Denmark Region with 1.2 million inhabitants and covering 13,053 km2. Patients were admitted to one of the five paediatric departments, and patients in the study cohort were transferred to one of the local PICUs or from the regional hospital to the university hospital owing to critical clinical deterioration. See Online Supplemental materials for a detailed description of the participating departments.
Study population
Children admitted to the involved departments who experience in-hospital clinical deterioration requiring transfer to a higher level of care. This includes children transferred to a PICU and children with possible need for intensive care at the regional hospitals who were transferred to the paediatric department at the university hospital to ensure proximity to the PICU.
Inclusion criteria: all children who were transferred from a paediatric department to a PICU due to clinical deterioration; all children transferred from the regional hospital to the university hospital due to clinical deterioration that requires proximity to a PICU; and children who died unexpectedly in the paediatric departments due to clinical deterioration.
Exclusion criteria: children admitted directly to the PICU from the pre-hospital setting; post-surgical cases who died during operation or directly after operation in the PICU; children in neonatal departments, who had not been discharged since birth; children dead upon arrival to hospital care (anticipated deaths); and children who died during palliative end-of-life.
Data collection
Data were extracted from the patients’ electronic charts (‘Central Denmark Electronic Patient Chart’ provided by Systematic – a common IT system for the whole region). Extracted data included: Demographic characteristics: Age, gender, admission date and time; date and time of critical event (transfer to PICU or death in paediatric ward); and date and time of death. Clinical characteristics: Discharge diagnoses were coded into the following categories: cardiac, post-surgical, neurological, respiratory, infection, hydration, and other (e.g. renal, endocrinology). Vital parameters: heart rate, respiratory rate, oxygen saturation, systolic blood pressure, temperature, Glasgow coma score, capillary refill time (during the last 24 hours before transfer to PICU) and outcome (dead/alive). PICU interventions: Invasive ventilation, continuous positive airway pressure (CPAP), use of inotropes, resuscitation (within 24 hours after transfer to the PICU), and extracorporeal membrane oxygenation (ECMO). Length of hospital stay (LOS). Length of PICU stay. Paediatric index of mortality score (PIM3)
PIM3 provides an estimate of mortality risk among children admitted to PICU (Straney et al., 2013). PIM3 consists of 10 variables that should be collected within one hour after arrival at the PICU. It consists of physiological variables and categorical variables that classify patients based on the reason for admission, the use of mechanical ventilation and diagnostic risk data (Straney et al., 2013). PIM3 has been used to evaluate the risk of mortality when registering patients in clinical trials and as a tool for monitoring the quality of intensive care and is not meant to be used as a marker for the severity of illness of individual patients (Straney et al., 2013). PIM3 is reported in the present study for comparison to other studies. We also used invasive ventilation, CPAP and inotropes as markers for the severity of illness.
The main researcher and a co-supervisor retrospectively reviewed the electronic charts of children admitted to the PICU, children who died in the paediatric ward and children transferred from the regional hospitals to the university hospital to identify children fulfilling the inclusion criteria. In case of disagreement, the case was discussed with the research group before inclusion/exclusion. All admissions to the PICU were also reviewed in the study period to find any relevant patients missing in the first data extract.
Data analysis
Data were analysed using STATA version 13. Descriptive statistics were performed and were summarized as percentages, median and interquartile ranges (IQRs) provided for continuous variables.
Ethical considerations
This study was approved by: The Danish Data Agency Board – journal number 2013-41-2269. The Central Denmark Region Committee on Biomedical and Research Ethics – case number 1-10-72-322-13.
This is the ethical committee overseeing projects from all the participating hospitals.
Results
This study screened an administrative database of 24,502 paediatric admissions in multiple hospitals in central region of Denmark, over a period of one year, and identified 92 patients who were defined as having an acute clinical deterioration that required transfer to a higher level of care.
Participant characteristic
Of the 24,502 admissions in the one-year study period, 240 transfers were identified. Eighty-one patients met the inclusion criteria. From a cross-check of intensive care admissions (n = 601), an additional 11 patients were identified – giving a total of 92 study patients. Sixty-four patients were transferred to ICUs, some of these patients did not need PICU interventions, and 28 from the regional hospitals to a paediatric department at the university hospital, 4 of these patients were then transferred to intensive care. Sixty-nine per cent (n = 64) was male (Table 1). The median age was 2.1 years (IQR 0.4–6.9) with 32.3% being infants under 1 year. In the overall hospital population in the included departments, 55% (n = 13,699) was male (Table 1), and the median age was 5.5 years (IQR 3.8–6.2), with 16.6% under 1 year of age. The most frequent diagnostic groups are outlined in Table 1, where the three most frequent were cardiac 18.3% (n = 17), neurological and respiratory, both with 15.1% (n = 14).
Patient characteristics.
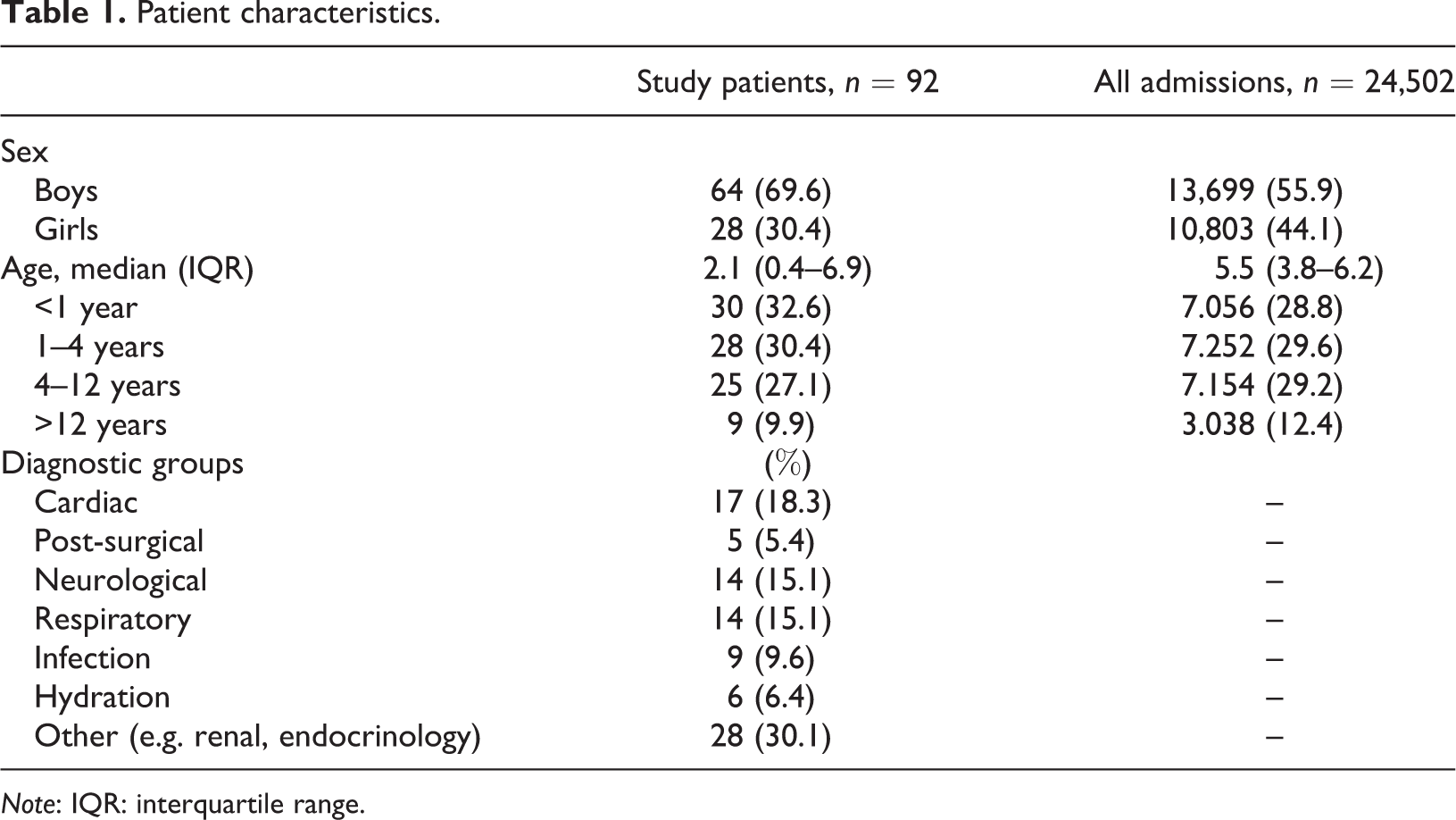
Note: IQR: interquartile range.
Physiological status preceding transfer
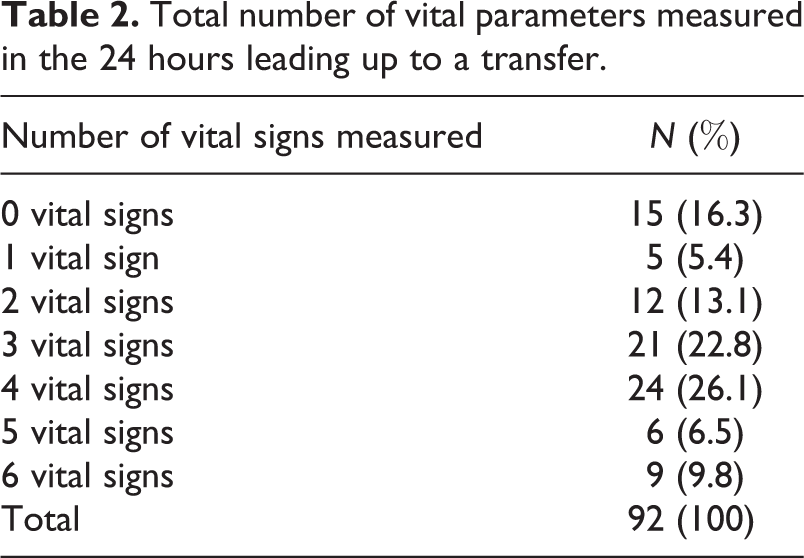
Patients in the study cohort often had no vital signs recorded in the 24 hours before clinical deterioration. Of these children, 16% had no vital signs recorded in the 24 hours before clinical deterioration (Table 2). Of those who did have at least one vital sign recorded, one in four had a vital sign abnormality identified. Physiological abnormalities (defined in the footnote to Table 3) were present in 19 (24.7%) of the 77 patients where vital parameters were documented (Table 3). As demonstrated in Table 3, the most common physiological abnormalities were tachycardia, with 16.3% (n = 15) and 15.2% (n = 14) with hyperthermia (>38.5). In all the included vital parameters, missing data were found, ranging from 23.9% (n = 22) in heart rate to 100% (n = 92) in capillary refill time (Table 3).
Total number of vital parameters measured in the 24 hours leading up to a transfer.
Frequency of recorded physiological abnormalities in 24 hours preceding transfer.
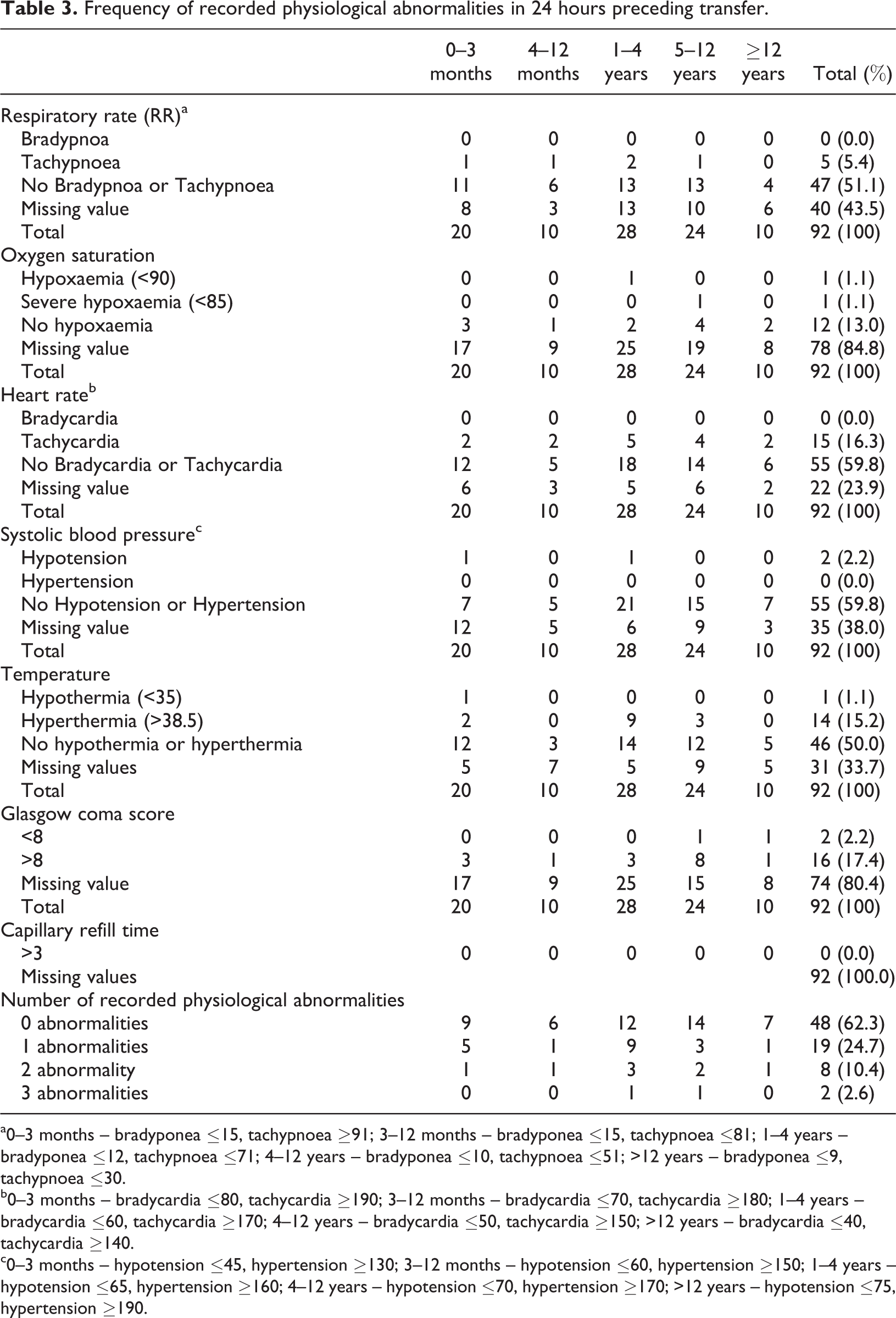
a0–3 months – bradyponea ≤15, tachypnoea ≥91; 3–12 months – bradyponea ≤15, tachypnoea ≤81; 1–4 years – bradyponea ≤12, tachypnoea ≤71; 4–12 years – bradyponea ≤10, tachypnoea ≤51; >12 years – bradyponea ≤9, tachypnoea ≤30.
b0–3 months – bradycardia ≤80, tachycardia ≥190; 3–12 months – bradycardia ≤70, tachycardia ≥180; 1–4 years – bradycardia ≤60, tachycardia ≥170; 4–12 years – bradycardia ≤50, tachycardia ≥150; >12 years – bradycardia ≤40, tachycardia ≥140.
c0–3 months – hypotension ≤45, hypertension ≥130; 3–12 months – hypotension ≤60, hypertension ≥150; 1–4 years – hypotension ≤65, hypertension ≥160; 4–12 years – hypotension ≤70, hypertension ≥170; >12 years – hypotension ≤75, hypertension ≥190.
Timing of transfer
The time of day with the highest number of transfers, 61.3% (Figure 1) was between 8 and 16 hours. The month with the highest percentage of transfers, 14.0%, was October (Figure 2). In addition, in Figure 2, the monthly distribution of hospital admissions and transfers are presented.
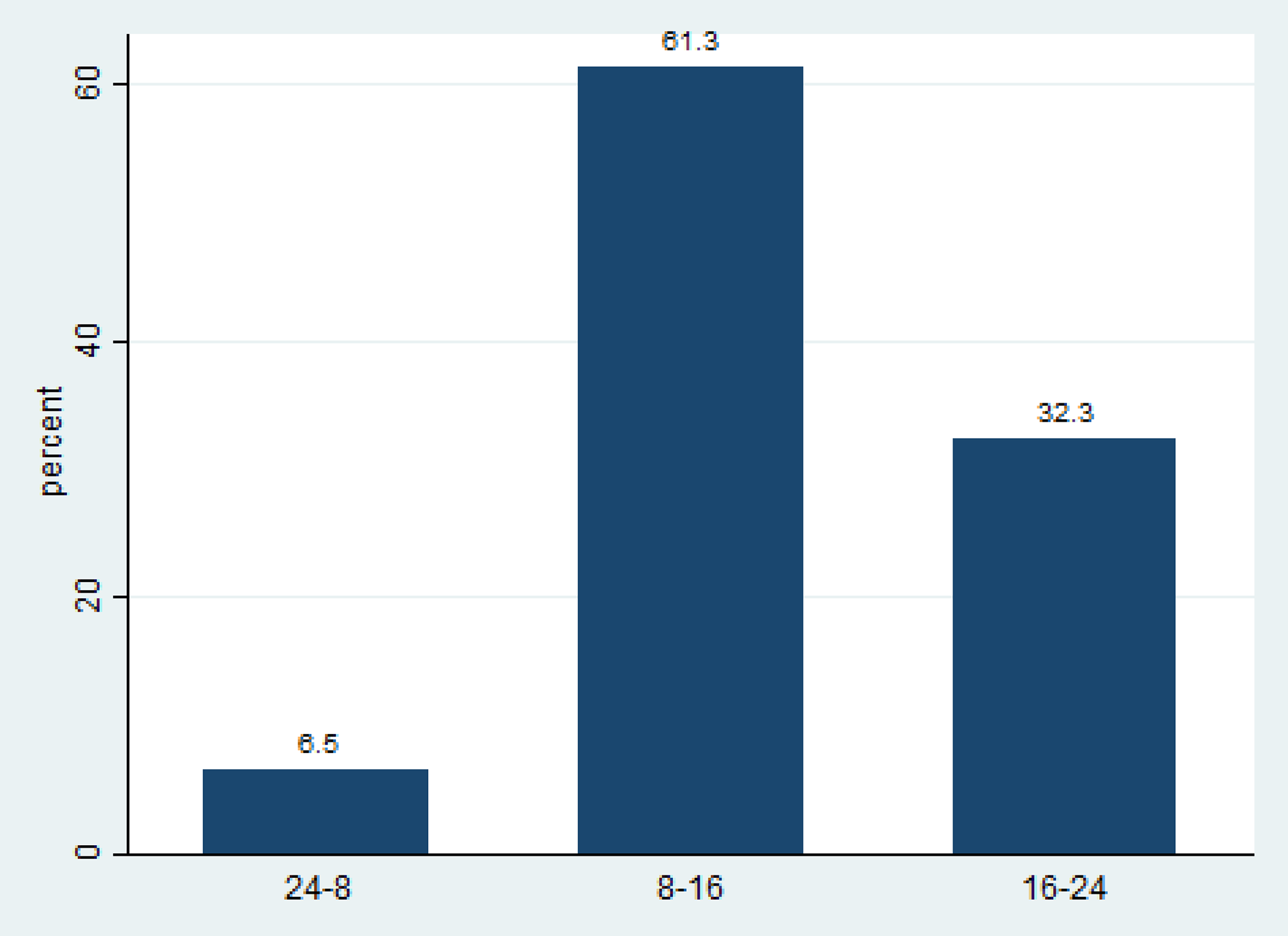
Transfer by time of day (%).

The monthly distribution of hospital admission and transfers. The percentage refers to the total numbers of refers and total number of hospital admission, respectively.
Outcomes
Interventions initiated in the PICU are presented in Table 4. Eleven patients (17.2%) received invasive ventilation, continuous positive airway pressure was provided for seven patients (11%) and ECMO was applied to one patient. Inotropic support was provided for 15.6% (n = 10). No patients died or were resuscitated within 24 hours after transfer to the PICU. The mean length of stay in the PICU was 0.9 days (IQR 0.38–2.8), and patients with a PICU stay had a hospital LOS median of 6.1 days (IQR 2.5–11.6). In the overall population in the included departments, the mean hospital LOS was 1.68 (IQR 1.26–2.28; Table 4).
PICU interventions and outcome.

Note: PIM3: paediatric index of mortality score; IQR: interquartile range; LOS: length of hospital stay; PICU: paediatric intensive care unit; CPAP: continuous positive airway pressure; ECMO: extracorporeal membrane oxygenation.
Discussion
Using a national administrative database, we conducted a retrospective cohort study to identify paediatric inpatients who experienced clinical deterioration that justified transfer to a higher level of care. Our study revealed that 16% of patients experiencing in-hospital clinical deterioration requiring transfer to a higher level of care did not have their vital parameters measured within 24 hours prior to transfer. Incomplete and infrequent reporting of vital parameters has been shown in other studies as well (Krmpotic and Lobos, 2013; Parshuram et al., 2011). Changes in vital parameters and behavioural changes indicating decline of a patient’s condition may be present in the 24 hours prior to an adverse event. Nurses’ bedside observations are therefore essential because their observations are the first step in identifying signs of clinical deterioration. This result could indicate that the monitoring practice rely on nurses’ clinical experience to detect children at risk of deterioration, but it also demonstrated that this practice fails as Bunkenborg et al. (2013) also found in their study, where they explored the nursing practice of monitoring in-hospital adult patients.
Twenty-one per cent had documented abnormal vital parameters, while other studies have reported a higher number of patients with abnormal vital parameters. Krmpotic and Lobos (2013) reported that 56% fulfilled at least one medical emergency team (MET) criteria in a study where she identified 39 children who experienced unplanned admission to the PICU within 24 hours after being admitted to the emergency department. It is possible that a higher number of patients in the present study had abnormal vital parameters, because many of the participating children had few or non-vital parameters documented. For example, no patients had capillary refill time measured, and respiratory frequency was missing in 43.5% of the patients. Capillary refill time has been reported as inconsistently performed (Lobos and Menon, 2008) and has been demonstrated to be a poor marker of cardiac output (Lobos et al., 2012). As no patients had capillary refill time documented, it could indicate that it was not part of the nurses’ bedside observations. However after this study was conducted, a PEWS has been implemented (Jensen et al., 2017a, 2017b, 2018) and subsequent very good inter-rater agreement of capillary refill time measurement has been reported (Jensen et al., 2017a). However, it is important to bear in mind that capillary refill time has to be combined with other signs of circulatory dysfunctions in order to make the diagnosis of circulatory dysfunction (Resuscitation Council (UK), 2016).
In the children experiencing clinical deterioration in the present study, almost twice as many patients were infants under one year, compared to the overall hospital population where 16.5% was infants under one year. This finding is similar to Kinney et al. (2008), who documented that 42% of the children received at MET call was under one year in a study examining 172 patients who activated a MET call. Krmpotic and Lobos (2013) reported male patients and infants under one year as prevalent in their study. We also found significantly more male patients (69%) in the children experiencing in-hospital clinical deterioration requiring transfer to a higher level of care. In the overall hospital population, 55% was boys. These findings could indicate that this age group is vulnerable and may need closer observations and that nurses’ clinical experience is insufficient to detect clinical deterioration. The three most common diagnosis groups were cardiac, respiratory and neurological, which is in line with other studies reporting on the clinical profile of children experiencing a MET call (Kinney et al., 2008) or early unplanned admission to the PICU (Krmpotic and Lobos, 2013).
No patients died or experienced resuscitation within 24 hours after transfer. These findings add to the discussion of cardiopulmonary arrest and death as sensitive indicators for deterioration (Krmpotic and Lobos, 2013; Jensen et al., 2017a). Studies on PEWS had difficulties showing an effect on mortality due to the low rate of cardiopulmonary arrest and death in paediatric patients (Duncan et al., 2006; Edwards et al., 2009; Parshuram et al., 2009; Tibballs et al., 2005). Interestingly, 61% of the transfers was during daytime (8–16 hours) when the staffing ratio is higher than in the evening, when 32% of the transfers occurred (Figure 1). This could be related to that the staffing levels are higher in daytime which might influenced the observation level of the patients helping to recognize children in risk of deterioration as Aiken et al. (2014) has documented a correlation between staffing level and mortality.
There were a seasonal variation in admission rates. Several factors could influence this variation. Seasonal variation is not an unfamiliar phenomena in paediatrics as respiratory conditions often are a reason to a higher number of admissions during autumn and winter (Souza et al., 2007). Respiratory syncytial virus is the most common cause of hospitalization for acute lower respiratory tract infection in children younger than five years with seasonal variation but appears to be active from November to April (Broberg et al., 2018). However, other reason such as the competences of the healthcare professionals might influence the transfer rates. There are trainees in all of the included hospitals which could influence the rate of transfers.
During the study period, no standardized PEWS guideline was used. It has been documented that children have abnormal vital parameters 24 hours before a transfer to PICU (Tume, 2007). Thus, it would be interesting to examine if the implementations of a PEWS system would improve documentation of vital parameters, help identify children at risk of deterioration and decrease the number of unplanned PICU admissions.
Limitations
There are several limitations to this study. It is a descriptive, retrospective review of electronic patient charts. We did not attempt to evaluate any interventions such as the implementation of PEWS. Such a study is, however, being conducted now. Hence, it would be very interesting to examine if the implementations of a PEWS system would improve the nurses’ documentation and patient outcomes. Another limitation is the small sample size, as in-hospital clinical deterioration requiring transfer to a higher level of care was an uncommon event. Future studies with a larger sample size comparing this patient group to a control group who did not require unplanned transfer are warranted.
Conclusion
The present study provides essential baseline data to inform further research improving care and treatment for critically ill children on paediatric wards. The findings in this study shows incomplete and infrequent reporting of vital parameters. Infants under one year seem to be a vulnerable age group and may need closer observations.
Supplemental material
Supplemental_material - Clinical profile of children experiencing in-hospital clinical deterioration requiring transfer to a higher level of care
Supplemental_material for Clinical profile of children experiencing in-hospital clinical deterioration requiring transfer to a higher level of care by Claus Sixtus Jensen, Hans Kirkegaard, Hanne Aagaard and Hanne Vebert Olesen in Journal of Child Health Care
Footnotes
Acknowledgements
The authors would like to thank the BIostatistical Advisory Service (BIAS) at the Faculty of Health, Aarhus University for statistical support and also like to thank Business Intelligence department for helping in extracting data from the electronic patient system.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Maria Dorthea and Holger From Foundation, the Novo Nordisk Foundation (NFF150C0016756 and NNF130C0006135), the Aase og Ejnar Danielsens Foundation, the Central Denmark Region Emergency Research Programme, Aarhus University Hospital, the ‘Acute Patient’ research programme, the Department of Child and Adolescent Health, Aarhus University Hospital and The A.P. Møller Foundation for the Advancement of Medical Science 15-161.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.