
Abstract
The aim of this study was to identify and describe how young children cope with hospitalization in relation to acute and/or critical illness. The study is a qualitative metasynthesis inspired by the approach described by Sandelowski and Barroso. Based on an exhaustive literature search, six studies were included. Data were analyzed through a taxonomic analysis. The findings revealed that the hospitalized children face a variety of challenges during admission to the hospital due to acute and/or critical illness. The main challenge was that hospitalized children strive to cope with different aspects of ‘the unfamiliar’ that emerge in their illness treatment and hospital stay. The unfamiliar refers to unknown experiences on a physical, emotional, and relational level. Subsequently, children cope with the unfamiliar by striving to convert the hospital stay into something more similar to everyday life, using strategies to secure basic needs and constructing familiarity in the hospital stay. The consequences of the children’s coping behavior are discussed and how children strive to keep their integrity intact during illness and hospitalization are revealed.
Keywords
Introduction
This study emerged from a previous study focusing on how people cope with health issues striving to keep their integrity intact (Jørgensen et al., 2017). During this work, it came to our knowledge that coping behavior among hospitalized children facing acute and/or critical illness has been sparsely examined through the experiences of the children.
We know that children admitted to the hospital on grounds of acute or critical illness are in limited physical condition and situated in a noisy and busy environment in which they encounter unknown vocabulary and unfamiliar health-care professionals (Jensen et al., 2012; Zimmer-Gembeck and Skinner, 2016). Thus, children of all ages may experience a range of fears and concerns that require robust coping skills during hospitalization (Coyne, 2006a; Jensen et al., 2012; Salmela et al., 2010; Thomas and Plunkett, 2017).
This is confirmed in the literature on developmental psychology, which states how infants’ and preschool- and school-aged children’s understanding and perception of illness is influenced by their cognitive and psychosocial capacity and skills, which influence their coping behavior in relation to their own illness (Erikson, 1993; Zimmer-Gembeck and Skinner, 2016). In addition, previous experiences of illness and the severity of the illness may have an impact on children’s understanding of their illness, affecting how they think about and act upon illness (Capurso and Pazzagli, 2016; Capurso and Ragni, 2016; Ryan-Wenger, 1996). It is essential to seek knowledge about children’s own experiences in order to adjust and manage their health care in the best possible way. Experiencing illness and hospitalization as frightening may negatively affect children’s development and cause psychological and behavioral difficulties following discharge (Rennick et al., 2014; Salmela et al., 2010). Recently, initiatives involving children in decisions about their health have been developed to ensure that children’s voices are heard, emphasizing a focus on children’s perspectives of hospitalization and illness (Coyne et al., 2016; Jensen et al., 2012; Salmela et al., 2010).
However, the majority of studies addressing children’s perspectives of illness and hospitalization are based on children with chronic illnesses. Data were mainly acquired from adult informants such as parents and health-care professionals (Kosta et al., 2015; Nabors and Liddle, 2017; Senger et al., 2016). Children’s own experiences of the undesirable consequences of being hospitalized (Capurso and Pazzagli, 2016; Salmela et al., 2010) have been sparsely described in the literature to date. Therefore, this study’s main focus is the process of going through hospitalization as expressed either verbally or nonverbally by children themselves.
If we increase our understanding of the children’s coping behavior and experiences of hospitalization and illness, health-care professionals may reinforce clinical interventions that support coping outcomes. In pursuance of insight in children’s coping with illness, we based the study on the published literature. Hence, the aim of this study was to identify and describe coping behavior of acute and/or critically ill children when they are admitted to the hospital.
Methods
Design
The study was performed as a qualitative metasynthesis as outlined by Sandelowski and Barroso (2007). Initially, a systematic literature search revealed that the literature describing the behavior of coping with acute and/or critical illness among children was sparse. However, none of the studies that we identified had been synthesized or published in a metasynthesis. A qualitative metasynthesis may be described as an ‘interpretive integration of qualitative findings that are themselves interpretive syntheses of data” (Sandelowski and Barroso, 2007). A metasynthesis seeks to develop and refine theories while retaining the uniqueness of each individual study (Finlayson and Dixon, 2008). Thus, we found it essential and important to compile children’s experiences of hospitalization and illness to achieve a deeper understanding of their coping behavior. In this study, our understanding of coping is very broad constituting a multidimensional and cyclical behavioral process that includes physical, mental, psychosocial, cultural, and religious/spiritual/ethnic dimensions representing a cascade of physiological, cognitive, affective, and behavioral actions (Jørgensen et al., 2013, 2014, 2017; Jørgensen and Fridlund, 2016).
Search strategy
An exhaustive literature search was conducted in the electronic databases: Scopus, CINAHL, PsycINFO, PubMed, and Embase. A health science librarian assisted with constructing search strategies and identifying search terms during the initial structured searches. The systematic search was conducted using the terms coping, acute OR critical, child, experience OR perspective AND qualitative. The search strategies are presented in Table 1. During this process, all of the authors discussed the search terms, the use of electronic and manual searching methods, and the choice of databases (Ludvigsen et al., 2016). As recommended by Sandelowski and Barroso, we searched the databases both backward and forward by screening the references of included articles and using the ‘cited by’ function in databases such as Scopus and CINAHL (Sandelowski and Barroso, 2007).
Search strategy.
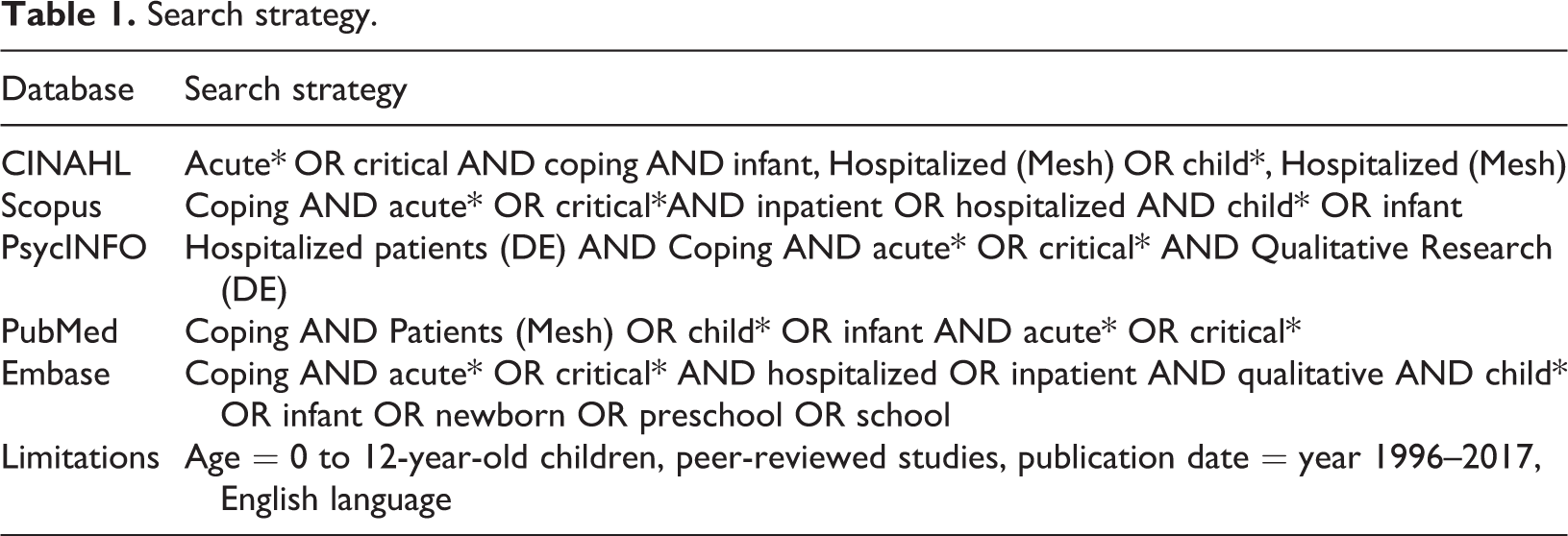
When operating with acute and critical illness, we understand acute illness as a condition that appear rapidly (within hours or days) and might cause death or severe physical or mental functioning if not treated. Critical illness is when there is clinical suspicion that the outcome of the condition might cause death or disability (Sestoft et al., 2015).
Inclusion criteria
We included qualitative studies and studies using a mixed-methods approach, if the qualitative data and results were transparently presented. The studies that addressed children aged 12 years or younger and their experiences of coping with illness were included. Because of ongoing advancements in the pediatric practice field (Sandelowski and Barroso, 2007) we only retrieved studies published between 1996 and 2017.
Criteria of exclusion
Studies that focused on older children or on the parents’ and health-care professionals’ coping with children’s critical illness were excluded. Studies not published in English or published before 1996 were excluded. Figure 1 shows the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flowchart of the literature search.
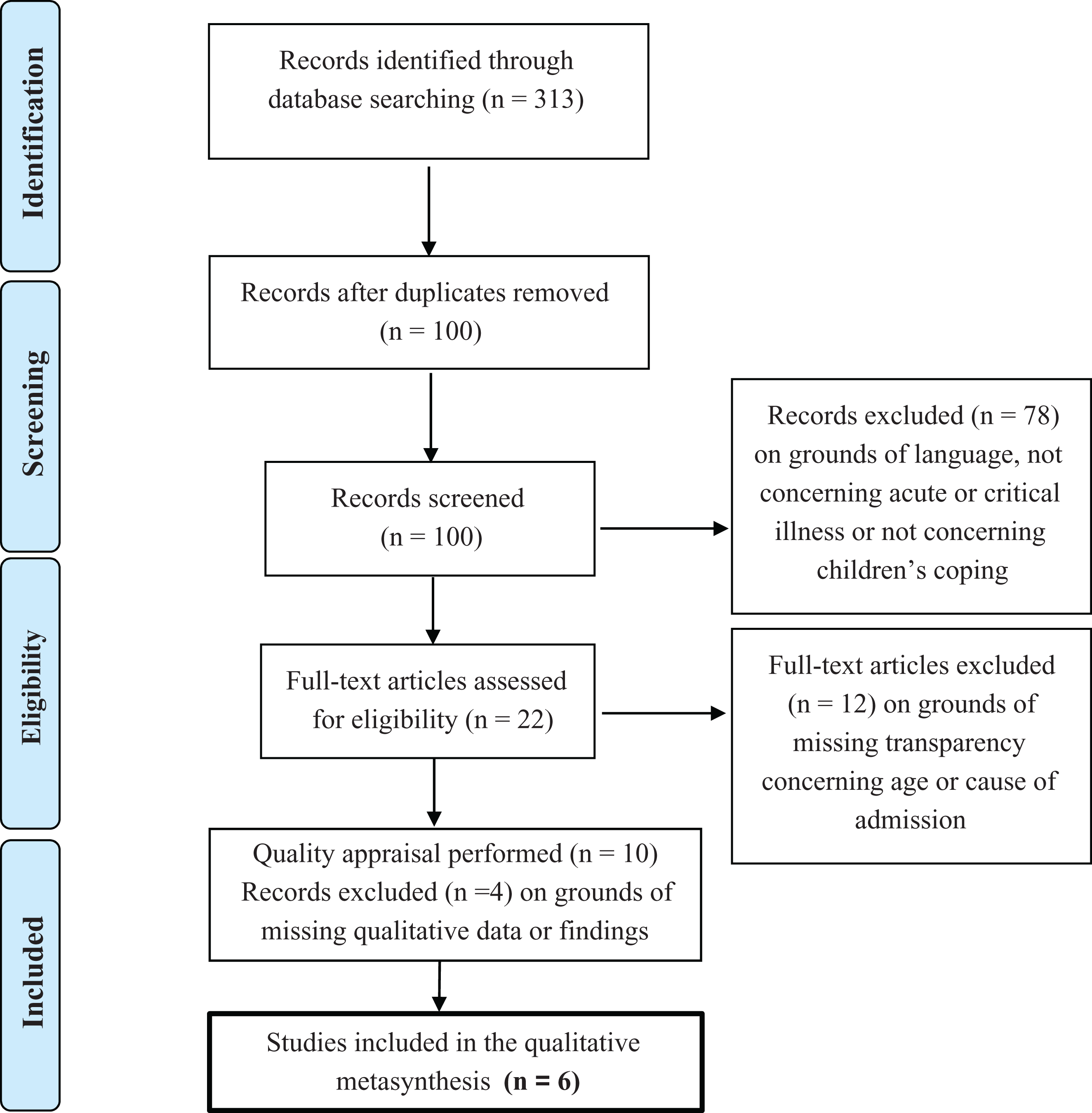
PRISMA flowchart of the literature search.
Quality appraisal
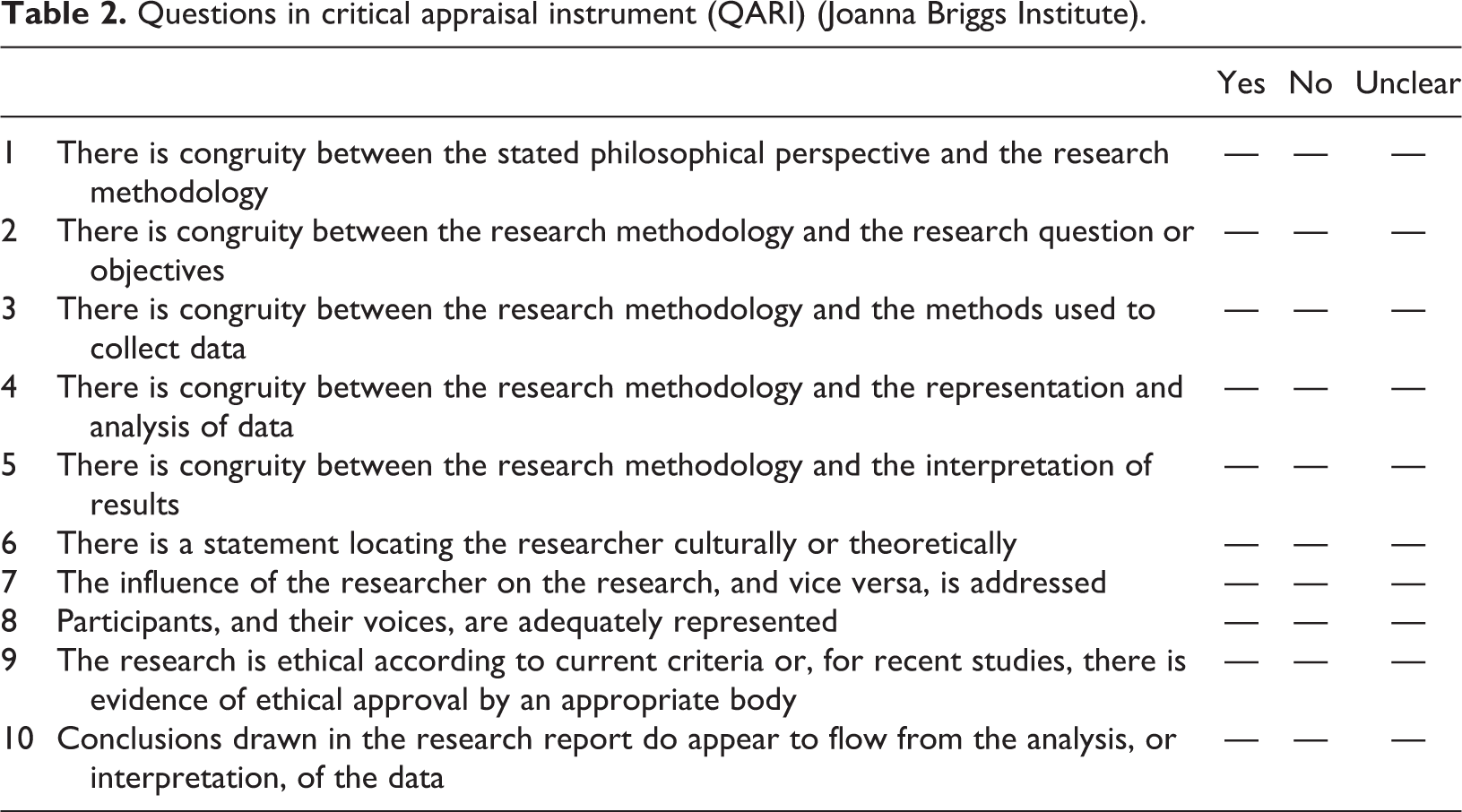
A systematic appraisal of the studies was carried out to reinforce our sensitivity toward the studies. The appraisal supported us to thoroughly evaluate each study and ultimately decide whether to include the specific study (Sandelowski and Barroso, 2007). The quality assessment was done using the Questions in critical appraisal instrument (QARI) (Joanna Briggs Institute, 2014), which included 10 questions on the congruity among basic elements of the individual studies (Table 2) and the recommendations put forth by Sandelowski and Barroso. The appraisal was performed, and the results were discussed by two of the authors (AH and SLJ) (see Table 3 for the results of the critical assessment QARI), and based on this, four articles were then excluded as they did not explicitly display qualitative data or they lacked result sections (Sandelowski and Barroso, 2002, 2003).
Questions in critical appraisal instrument (QARI) (Joanna Briggs Institute).
Results of the critical assessment (QARI).
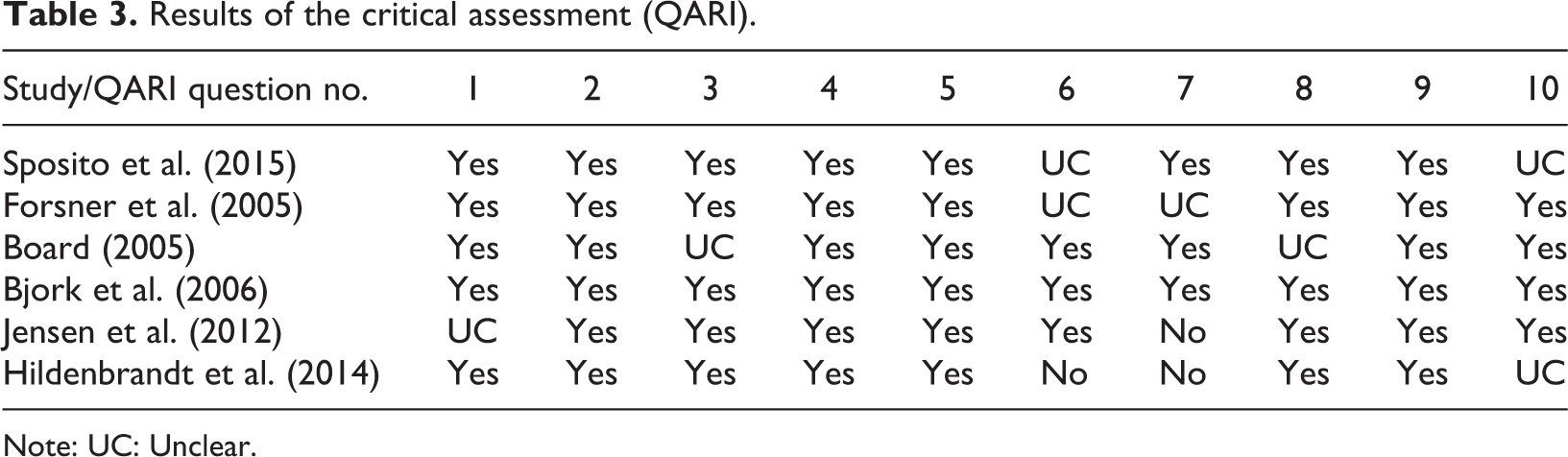
Note: UC: Unclear.
Search outcome
The six studies that were included were all based on qualitative data addressing children’s coping with acute and/or critical illness when hospitalized. The majority of the children included in the six studies experienced acute hospitalization due to different diagnoses or illness caused by cancer, trauma, or infection. Other reasons for admission varied from cancer or medical conditions to surgical conditions. The studies represented a total sample size of 73 children between the age of 7 months and 12 years. Data were collected through interviews, questionnaires, and observations. Table 4 lists the further characteristics of the included studies’ design and analysis of data.
Studies included in the review (n = 6).

Note: PICU: Pediatric Intensive Care Unit; PEAU: Pediatric Emergency and Assessment Unit.
Data analysis
Analyzing the studies, we searched for any finding that addressed children’s coping with hospitalization in relation to acute and/or critical illness. When analyzing the studies, we were inspired by Sandelowski and Barroso who define findings as: ‘The data-driven and integrated discoveries, judgements, and/or pronouncements researchers offer about the phenomena, events, or cases under investigation’ (Sandelowski and Barroso, 2003, pp. 909–910). The analysis was inspired by a taxonomic analysis approach, which is an inductive form of domain analysis that can show the conceptual range of findings and is useful in developing models and theories (Sandelowski and Barroso, 2007), allowing the researcher to interpret the underlying meaning of the findings. The analysis was guided by the following four questions which were developed to examine coping in relation to illness and health challenges (Jørgensen and Fridlund, 2016; Jørgensen et al., 2017). The four questions listed in Table 5 were cardinal points in the patients’ narratives on how they coped with health challenges.
Questions used throughout the analysis.

First, the findings were extracted and placed in the electronic analysis program NVivo 11, which helped to organize and analyze the unstructured information (Bazeley and Jackson, 2013). Then, all authors thoroughly read the findings while focusing on the analytic questions concerning the children’s challenges, motivation, and coping strategies when hospitalized due to acute and/or critical illness.
This process was dynamic and constantly changing as the analysis revealed new perspectives and motives in the children’s coping behavior. This involved numerous discussions, such as the process of differentiating between and illustrating the underlying factors causing the children’s behavior. This process also revealed that the last analytic question, ‘What seems to be the consequence of this behavior?’, could not be adequately dealt with during the analysis, as the consequences were not distinctly addressed in the extracted findings. Therefore, this question will be addressed in the discussion with a focus on possible integrity-eroding or integrity-protecting consequences.
Findings
The overarching finding in this study was that the children coped with the unfamiliar by converting the hospital stay into something more similar to everyday life using strategies to secure familiar basic needs such as parents, nutrition, engaging in relations with health-care professionals, and thereby constructing an everyday life at the hospital through parents, play, imagination, and social interaction. The unfamiliar was the greatest challenge the children had to face. Connected with the unfamiliar were several challenges that affected the children’s coping with hospitalization and illness. These children were experiencing an unfamiliar role as a patient, being in an unknown environment where the body had limited physical functioning and experiencing pain and discomfort in unknown ways. These findings are expanded and presented below.
The presentation of findings is structured as follows: First, the challenges the children face and struggle with are presented, and then the overarching coping behavior of the children is brought forth. Second, the different coping strategies of the children are described.
The unfamiliar
The overarching finding of this study was that children admitted to the hospital found hospitalization to be unfamiliar and predominantly strived to cope with the unfamiliar.
The environment made them feel insecure, the noises were unfamiliar, and the routines at the hospital as well as the health-care professionals were new and foreign to them. In addition, the children had to cope with pain and discomfort, which they might never have experienced before. They felt their physical functioning was reduced and needed physical care and assistance (Bjork et al., 2006), and they also felt uncertain about the medical procedures and about what was going to happen. The language used at the hospital was unknown and at times incomprehensible (Jensen et al., 2012). Being a patient was an unfamiliar role that left them passive and excluded from their everyday life: ‘Ah it’s bad to stay in the hospital…there is nothing to do’ (Sposito et al., 2015). This was markedly a new situation that they needed to learn how to navigate and respond to. These unknown factors made the children vulnerable and insecure as they experienced a loss of control. Being confronted with these aspects of unfamiliarity could cause the children to face an existential threat or fear. To prevent loss of control and to cope with this new life situation, the children worked hard to convert the unfamiliar into something familiar.
The children were challenged by being in an unfamiliar place filled with unknown medical procedures and uncertainty about the length of hospitalization. The daily routines, such as when to eat, when to sleep, when to be quiet, and when to play, were new and different to them. Lack of insight about the hospital agenda and their treatment caused fear and insecurity among the children. One example was that if the children pulled the help string by the hospital bed, then this could be a good thing since help would arrive, but it was also frightening when they did not know what would happen afterward (Forsner et al., 2005). Being in a high-tech environment like Pediatric Intensive Care Unit/Pediatric Emergency and Assessment Unit was also a challenge, as the intubation, pain, and serious atmosphere had very few similarities to home and everyday life (Board, 2005; Jensen et al., 2012). Another challenge was the unfamiliar medical language spoken at the hospital. The children had difficulties understanding the medical terms used by the health-care professionals and therefore they could make little sense of their illness and treatment (Forsner et al., 2005; Jensen et al., 2012; Sposito et al., 2015), which may also have caused further insecurity among them.
When hospitalized due to acute and/or critical illness, the children found themselves in a situation characterized by severity, pain, discomfort, tiredness, and reduced energy. These conditions placed them in an unfamiliar role as somewhat passive patients. The patient role included adapting the habitus and norms of the hospital and establishing positive relations with the health-care professionals.
Overarching coping behavior: Converting the environment of the hospital into everyday life
The children’s dominant coping behavior included converting the unfamiliar into something familiar. This coping behavior contained different aspects, all representing the process of creating a more familiar situation during hospitalization. The children actively tried to integrate the aspects of their everyday life at the hospital, for instance, by playing with their own toys or talking to their friends online (Bjork et al., 2006; Forsner et al., 2005; Sposito et al., 2015) and sought to create a known, transparent environment and establish relationships with the health-care professionals. The two most predominant coping strategies in this conversional process were securing familiar basic needs and constructing an everyday life during hospitalization.
Coping strategies
Strategies targeted familiar basic needs
In this study, several of the children’s coping strategies targeted basic physical, emotional, and relational needs.
Naturally, the children needed to fulfill their physical needs such as eating, drinking, and medication, but they also coped with physical and emotional discomfort through massage, bathing, relaxation, sleep, and comfort (Bjork et al., 2006; Board, 2005; Sposito et al., 2015). To fulfill their emotional and relational needs, the presence of their parents was the most commonly used coping strategy. The children enjoyed the close contact with their parents and developed a strong symbiotic relationship. Some of the children begged to be able to hold hands, hug, or at least see and hear their parents at all times (Bjork et al., 2006). Thus, the parents served as a secure platform for children of all ages, and they had a significant comforting role. In particular, the infants and preschool-aged children needed to have their parents close by at all times including during medical procedures, play, and sleep.
Another relational need was the need to establish positive relations with the health-care professionals, whom the children were well aware, were the ones making the decisions about their treatment. Children of all ages were interested in interacting with the health-care professionals and especially the preschool-aged children did fun things with, kissed, and hugged the health-care professionals. The children acted as ‘good patients’ as most of them did what they were told without protesting. For instance, one child said: ‘Understanding why I take chemo helps me not to complain about the treatment’ (Sposito et al., 2015).
The children wanted to be involved and participate in procedures, conversations, and decisions about their illness or treatment. They sought knowledge so that they could understand their situation: ‘I prefer knowing what’s going to happen so that I can prepare myself’ (Sposito et al., 2015). At the same time, it was important for the children to be on good terms with the health-care professionals. They had a great need for recognition and praise from them. However, even though the children did not know the meaning and context of the medical terms, they still used them during conversations with the health-care professionals (Jensen et al., 2012; Sposito et al., 2015).
Constructing an everyday life at the hospital
Another coping strategy concerned building or constructing an everyday life at the hospital. The children strived to maintain their habitual status as children and they all tried to transform the space of the hospital into their familiar everyday life by bringing their own toys, clothes, games, or electronic devices (Bjork et al., 2006; Jensen et al., 2012). Again, the parents and their physical presence helped the children to remain children in these unfamiliar situations.
All children coped with their situation through fun and play. Playing in general was a familiar activity to the children that helps them to construct a more familiar environment. When the children attended play activities, it distracted their minds and distanced thoughts of illness. The youngest children played with their toys and they played with their parents. They attended play activities initiated by play therapists. The older children listened to music, played video games, or had online conversations with their friends. Often the children played the same games as they did at home. Therefore, playing helped the children make the unfamiliar familiar. Many of the children used coping strategies that combined reality and imagination. For instance, sometimes they seemed to believe that their illness would disappear if it was ignored or if they hid themselves from it (Forsner et al., 2005). The children then had an opportunity to create an arena for coping with the situation through the familiar language of play.
Discussion
The aim of this study was to identify and describe the coping behavior of acute and/or critically ill children admitted to hospital. Six studies featuring children from 0 to 12 years of age were included. This discussion will primarily focus on expanding the phenomenon of the unfamiliar/familiar as well as discussing potential and possible consequences of the children’s coping behavior.
Coping with the unfamiliar was the most pivotal and predominant challenge among the hospitalized children. This is supported by other studies that have discovered that hospitalized children feel rootless and cope with homesickness (Thurber et al., 2007), seek normalization through play and relations in the new environment of the hospital (Woon, 2004), and strive for protection and comfort (Wilson et al., 2010). Acknowledging especially acute hospitalization to be a foreign field to most children and parents is essential. In our study, we discovered how children seek familiarity through converting the environment surrounding them. In seeking familiarity, the presence of their parents is children’s most essential coping strategy.
Children also repeatedly feel excluded from the decision-making around their treatment. One child stated, ‘They talked mostly with my mother and father’ and ‘They talked about adult stuff’ (Jensen et al., 2012). Often the children are not met in their needs of being included and informed, which may bring them feelings of inferiority and insecurity (The National Council for Children, 2017; Coyne, 2006b; Jensen et al., 2012). Thus, during hospitalization, they have limited control and sometimes force themselves into conversations above their intellectual level. This is worsened by the fact that children’s psychological development challenges coping with illness (Ryan-Wenger, 1996), as does their use of magical, perception-bound, and intuitive thinking (Erikson, 1993).
Coping and play are important factors in a child’s development and support the ability to adapt (Capurso and Ragni, 2016). Therefore, play is a fundamental part of children’s lives, and a natural ingredient when a child is ill and admitted to the hospital. Playing supports coping with illness in children of all ages. When children use play as a coping strategy, playing creates a transitional area where fantasy and external reality coexist (Winnicott, 1971). Furthermore, children cling to their preferred toys and well-known games and styles of play (Bjork et al., 2006; Board, 2005; Forsner et al., 2005; Hildenbrand et al., 2014; Jensen et al., 2012; Sposito et al., 2015).
However, the foreign field of hospitalization complicates parents’ abilities to support children’s coping, which is challenged by parental stress and anxiety (Suleman et al., 2016). The parents strive to be in control of the situation, participate, and sufficiently communicate to appear as competent parents (Hall, 2005). To reduce anxiety and worry among both children and parents in departments of pediatrics, the family-centered care (FCC) approach may be useful. Wright et al. (1996) define a family as ‘a group of individuals who are bound by strong emotional ties, a sense of belonging, and a passion for being involved in another’s lives’. Internationally, health-care professionals working from the FCC approach perceive inclusion of the entire family, through open communication, participation, and collaboration, as vital to the health of both child and family (American Academy of Pediatrics, 2012).
Being hospitalized and meeting unfamiliar surroundings may be an integrity-threatening experience for both adults and children (Jacelon, 2004; Jørgensen and Fridlund, 2016; Morse, 1997). Keeping the integrity intact is the most predominant motivation for coping with health issues in pursuit of maintaining a sense of wholeness as a person (Jørgensen et al., 2017). In this study, we find that children work hard converting the unfamiliar into something more familiar, recognizable, and secure, and that this may be their way of preserving their sense of wholeness and thereby their integrity.
In addition, integrity can be shared and jointly threatened within a family (Jørgensen et al., 2017). Parents may play an enormous part in keeping the integrity of the child and family intact. This reciprocity between child, parents, and family is described by Suleman et al., who found that because parents are children’s most important coping strategy, parents’ experiences of anxiety, fear, stress, and worry may naturally affect children’s experiences of a situation (Suleman et al., 2016). Thus, it is important that health-care professionals must continuously be attentive to parents’ coping as well. To reduce anxiety and worry among both children and parents in departments of pediatrics, FCC seems to be a useful approach, where the family is considered to be the child’s primary source of strength and support (Institute for Patient- and Family-Centered Care, 2012; Shields et al., 2006). Through an FCC approach, the parents can gain resources to maintain what is familiar to the children. The parents might be able to hold on to routines known by the child, for example, by singing familiar lullabies, bringing food from home, reading the same stories over and over. By maintaining what is familiar, the children might experience reduced anxiety and increase their coping capacity.
Illness increases children’s need for physical and emotional closeness with their parents, and children rely on their parents to interpret the situation (Coyne, 2006a). Thus, the healthy growth of children’s coping system is predicated on sensitive caregiving and secure parent–child attachment (Zimmer-Gembeck and Skinner, 2016). In this perspective, parents’ role in keeping the integrity of the child and family intact leaves the parents as a profound and pivotal coping resource to their children requiring a sufficient attachment between parent and child. However, health-care professionals seem to play a similar role of solidarity in keeping children’s integrity intact. Consequently, health-care professionals must be aware of the mutuality between health-care professional, parents, and child in the task of keeping the integrity of the child, parents, and family intact.
Despite the motivation to keep integrity intact, some coping behaviors may erode the integrity (Jørgensen et al., 2017). Consequently, the culture and values of a department of pediatrics as well as the behavior, routines, and language of the health-care professionals may additionally play a part in securing or unintentionally eroding children’s integrity. A child’s integrity is always unique and calls for a necessary curiosity among health-care professionals to understand what is at stake in each individual child and seek the motive behind their coping behavior. If the motive is understood and individual, tailored support can be given to the child by health-care professionals and parents, this may result in integrity-preserving coping behavior in the child (Jørgensen et al., 2017).
Future perspectives
Specialized professional competences in pediatrics influence positively on both quality of care and length of admission; therefore, health-care professionals need to possess the necessary education to provide the best possible treatment to children and their families (Bryant-Lukosius et al., 2015; Newhouse et al., 2011). This includes approaching the children open-mindedly and letting go of prior understanding of what the children experience as necessary. According to Vessey (2003), health-care professionals have to reexamine what they know, not just what they think they know, to gain insight into the needs of hospitalized children. Besides seeking the motivation behind children’s coping behavior to support coping, health-care professionals must understand children’s psychological development to execute appropriate and efficient communication with ill children. Varying communication to accommodate the different intellectual levels in children and parents is necessary and defies the assumption that children are small adults. On the contrary, children require special attention and adjustments of care (The National Council for Children, 2017; Carlsson, 2014).
We need to further explore the phenomenon of what is ‘familiar’ and ‘unfamiliar’ to hospitalized children and what parts of integrity (e.g. physiological and psychosocial dimensions) are threatened in meeting the unfamiliar. Furthermore, since familiar and well-known coping strategies such as implementing habitual routines, artifacts, and vocabulary during hospitalization seem to help children to transform something unfamiliar into something more familiar, we need more knowledge of how to support the transformation and how hospitalization can be familiarly organized and adjusted in clinical practice.
Limitations
Sandelowski refers to the assumption that in a qualitative metasynthesis, interpretation is at least three times removed from the target experiences under investigation (Sandelowski, 2006). The authors were conscious of this element of distance and attempted to remain as loyal as possible to the data sources. Some studies were thematic or interpretive, and some were descriptive. We extracted only findings from the result sections of the studies, since our focus was exclusively on the children’s means of coping with hospitalization in relation to acute and/or critical illness.
Despite an exhaustive literature search, the metasynthesis is based on only six studies. This may be perceived as a small data set and thereby a limitation. However, the studies are internationally representative. The limited number of studies gave us the opportunity to work thoroughly in an in-depth analysis and the findings reflect experiences across the studies, which is considered a strength in this study. The literature searches were performed by the first author but were initiated and monitored in cooperation with a health science librarian for validation of the search process. Throughout the process of searching for literature, quality appraising, analyzing, and interpreting the data, all authors have collaborated to contribute to validation of the findings. A weakness of the study is, however, the limited number of identified studies, which makes it difficult to draw any definite conclusions on children’s coping with acute or critical illness during hospitalization. The grounds for comparing the different studies are challenged by the wide span of age and cause of admission. For instance, the difference between infants and school-aged children considering their psychological development is enormous. Moreover, only one of the included studies revolved around children below the age of six, which means conclusions about this group should be made with caution. Nonetheless, we find that coping transcends beyond illness, age, or gender. Coping has the same overarching structure, which is to protect the person’s integrity. This structure of coping with illness is generated on grounds of both empirical studies and reviews holding more than a thousand references (Jørgensen and Fridlund, 2016; Jørgensen et al., 2017). This substantiate the argument that when coping with illness, coping has a homogeneous structure that is evident no matter the type of illness, age, and so on.
Conclusion
Our study identified and described how young children cope with hospitalization in relation to acute and/or critical illness. Coping with the unfamiliar was the most pivotal and predominant challenge among hospitalized children, and it was met by a coping behavior of converting the unfamiliar to something more familiar to reduce the discrepancy between the hospital stay and being at home experiencing everyday life. Children executed this conversion to preserve their integrity. In their efforts to do so, parents as well as the health-care professionals play an important part in keeping the integrity of the child and family intact. This calls for communication skills and knowledge of children’s psychological development in health-care professionals. Future research should further explore the phenomenon of what is ‘familiar’ and ‘unfamiliar’ to hospitalized children. We need to examine what threatens the integrity of hospitalized children and how to organize familiar hospitalization in clinical practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respects to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.