
Abstract
The purpose of this cross-sectional descriptive study is to explore pediatricians’ and neonatologists’ attitudes and standpoints on end-of-life (EOL) decision-making in neonates. Seventy-five physicians, employed fulltime to care for newborns in 23 hospitals in Jordan, completed internationally accepted questionnaires. Most physicians (75%) were supportive of using life-sustaining interventions, irrespective of the severity of the newborns’ prognosis and the potential burden of the neonates’ disabilities on their families. The general attitude of the physicians (59–88%) was against making decisions that limit life support at EOL; even those infants with what are, in fact, untreatable and disabling medical conditions (56–88%). Most physicians (77%) indicated that ethics committees should be involved in EOL decision-making based on requests from parents, physicians, or both. The results of this study indicate strong pro-life attitudes among the physicians whose role is to take care of infants in Jordan. The results also emphasize the need for (1) the creation of clear EOL–focused regulations and guidelines, (2) the establishment of special ethical committees to inform and assist healthcare providers’ efforts during EOL care, and (3) raised awareness and competencies regarding EOL and ethical decision-making among physicians taking care of newborns in Jordan’s intensive care units.
Keywords
Introduction
Advances in technology and clinical knowledge have enabled many children to survive or prolong their lives, when once they would not have done so. Hence, these advances have increased the health-care providers’ awareness of the limits of what is possible in medicine (Janvier and Watkins, 2013). When intensive care treatment is no longer in the best interest of a newborn, physicians often consider end-of-life decisions (EOLDs) to avoid newborns and their families further pain and suffering (Hellmann et al., 2016). The obligations of making EOLDs for dying newborns and discussing such a decision with the neonate’s parents are central to the physicians’ professional role (Epstein, 2010). However, making such decisions constantly inflict ethical challenges upon the health-care team members, particularly the physicians.
Studies have documented the worldwide increment rates of EOLD made in neonatal intensive care units (NICUs) over the past years (Chan et al., 2016; Kim et al., 2018; Michel et al., 2018; Park and Kim, 2016). Rates of EOLDs made at newborns’ EOL were reported to be around 34% in NICUs in Latin America (Fajardo et al., 2012), 54% in Hong Kong (Chan et al., 2016), 63% in the United Kingdom (Aladangady et al., 2017), and between 71% and 81% in Canada (Hellmann et al., 2016; Lam et al., 2016).
Generally, EOLDs for infants with life-limiting conditions in the NICUs may take several forms, including (i) continuation of current treatment without addition of others, (ii) withholding life-sustaining interventions, (iii) withdrawing life-sustaining interventions, and (iv) purposely ending life through the act of ‘euthanasia’. Life-sustaining interventions could include, but are not limited to (a) newborns’ resuscitation, (b) mechanical ventilation, (c) vasopressor or cardiotonic medications, and (d) artificial hydration and nutrition. Such clinical decisions at newborns' EOL were considered in several countries over the last two decades (Cuttini et al., 1997; Eventov-Friedman et al., 2013; Fajardo et al., 2012; Hellmann et al., 2016; Hellmann et al., 2013; Kim et al., 2018; Roy et al., 2004; Wall and Partridge, 1997).
Previous studies indicate that physicians often consider EOLD in newborns who are perceived to be facing imminent death (Aladangady et al., 2017; Fajardo et al., 2012; Hellmann et al., 2016). EOLDs were also considered in newborns with anticipated poor developmental outcomes (Hellmann et al., 2016; Lam et al., 2016; Shivananda et al., 2013) predicting an extremely challenging poor quality of life in newborn survivors (Hellmann et al., 2016; Lam et al., 2016; Verhagen et al., 2010). Quality-of-life considerations, in particular, have emerged as an important factor in the EOLD making process over recent years (Aladangady et al., 2017; Hellmann et al., 2016; Lam et al., 2016).
There are several factors commonly considered in making EOLD in the NICU, in addition to the newborns’ clinical prognosis and outcomes. For example, physicians involved in the EOLD process frequently consider the families’ wishes (Arzuaga et al., 2016; de Vos et al., 2015; Richards et al., 2018). Conflicts between a family’s autonomy and the physicians’ authority are common in the process of EOL decision-making with newborns (Aladangady et al., 2017; de Vos et al., 2015; Richards et al., 2018; Verhagen et al., 2009). Additionally, physicians’ demographic and professional factors were found to inform the tendency of making an EOLD in the NICU. In a pioneer study across Europe, it was found that a neonatologist’s age, length of professional experience, and the importance of religion in his or her life all were related to the probability of making EOLDs in NICUs (Cuttini et al., 2000).
The ethical debate of how and when to limit a newborn’s treatment in the NICU gained international prominence with the increased number of studies comparing the attitudes and practices of EOL decision-making among several countries. Enormous differences in the practices of EOL decision-making in the NICU were found internationally (Cuttini et al., 2000; De Leeuw et al., 2001; Fajardo et al., 2012; Rebagliato et al., 2000; Verhagen et al., 2010). The worldwide variability in EOLD practices suggests considerable cultural and social influences on neonatal EOLDs that are informed by personal rather than professional characteristics of the physicians (Rebagliato et al., 2000). The vast majority of the studies on the topic documented the Western perspective regarding the views and practices of EOLD with neonates. Studies on this sensitive and often controversial topic in the Middle East and Mediterranean countries are surprisingly few.
Jordan is a country in the Middle East with a total population of approximately 10 million (Department of Statistics, 2017). The annual rates of neonatal mortality in Jordan are relatively high, reaching 11 newborn deaths per 1000 live births in 2015 (World Bank, 2018). Of all the neonatal deaths that occurred in the NICUs of Jordan, 79% happened in the first week after birth. Congenital anomalies, prematurity, asphyxia, sepsis, and other respiratory related conditions are among the most common causes of fatality among newborns in Jordan (Batieha et al., 2016).
Jordanian culture is deeply rooted in the Islamic traditions and Mideastern customs, with the vast majority of the population in Jordan being Muslims. Jordanians are often considered moderate in their adoption of Islamic values and traditions. The standpoint of Islam is clear about euthanasia (Naga and Mrayyan, 2013); however, it is less direct when it comes to guiding decisions relating to issues such as limiting intensive care and maintaining life-sustaining interventions among dying infants. In the light of this situation, and taking into account the limited national legislation to regulate the neonatal EOL practices in Jordan, exploring the physicians’ practices and attitudes of EOLD became a priority.
Physicians primarily initiate the clinical decisions for hospitalized newborns in Jordan, including those infants with life-limiting conditions and at their end of life. Subsequently, the possibility exists that EOL practices in Jordan could be predicted from the attitudes and values of the involved physicians. The purpose of this study is to describe Jordanian physicians’ standpoints and attitudes toward making EOLD in the NICUs of Jordan; thereby providing a basis for understanding and anticipating the current practices informing EOL decisions and practices in Jordan’s NICUs. By adding the findings from Jordan to the literature from other countries, comparisons and generalizations regarding EOL decision-making could be made internationally.
Methods
Study design
A cross-sectional descriptive design was applied in a large study that explored aspects of EOL care among neonatal nurses and physicians in Jordan. Only the results regarding the physicians’ attitudes and perspectives on EOLD are presented in this article.
Participants
A convenience sampling method was applied. Pediatricians and neonatologists who carry out clinical activities fulltime at the NICUs of 24 hospitals in Jordan were eligible to participate. Because of the exploratory and descriptive nature of the study, there were no exclusion criteria regarding participants’ demographic backgrounds and professional characteristics.
The 24 hospitals were selected for having large NICUs with high turnover rates of newborns. A wide sociodemographic range of the population, from both rural and urban areas of the country, is served by the selected hospitals. The hospitals were selected from all three geographic divisions of the country. Sixteen private and public hospitals were located in the middle cities of Jordan; two of the private hospitals in middle Jordan were faith-based hospitals. Four public hospitals were located in three cities in the north, and three major public hospitals were selected from three cities in the southern divisions.
Variables and measurements
Data for the study were collected using self-administered and internationally-accepted questionnaires. These research instruments were originally developed for the EURONIC Project titled: “‘Parents’ information and ethical decision-making in neonatal intensive care units: staff attitudes and opinions” (Cuttini et al., 1997). The questionnaire was adapted and translated for use in several languages and cultures across the European Union (EU contract no. BMH1-CT93-1242). The questionnaire has two versions, one for nurses and one for physicians; the findings from the physicians’ questionnaire are reported in this article.
The guidelines for cross-cultural adaptation of self-administered instruments suggested by Beaton et al. (2000) were used to adapt the instrument for use with Jordanian culture and terminology. The guidelines for instrument adaptation involved translation and back-translation of the original wording to the formal language in Jordan (Arabic), in addition to careful revision for clarity and cultural match of contents and terminology by bilingual health experts.
The physicians’ survey questionnaires consist of four sections. The first section was designed to collect participant’s demographic, personal, and professional information. Variables included (a) age, (b) gender, (c) having children, (d) religion, (e) perceived importance of religious values in personal life, (f) perceived effect of EOLDs on everyday life, (g) professional position, (h) type of clinical work at present time, (i) involvement in caring for healthy newborns, (j) involvement neonatal follow-up post NICU discharge, (k) overall number of years in the medical profession, (l) length of experience exclusive to newborns’ care, and (m) involvement in research activities.
The second section included multiple choice and Likert-type questions to assess physicians’ attitudes and views regarding EOLD in newborns. This section includes 12 statements on physicians’ attitudes toward EOL decision-making. Responses were measured using a 5-point Likert-type scale ranging from 1 = strongly agree to 5 = strongly disagree. Using factor analysis, Rebagliato et al. constructed a pro-life attitude subscale consisting of a set of 7 of the 12 attitude statements, weighted by their factor loadings. Similarly, a pro-life attitude score was generated in this study. Scores ranged between 0 and 10, with the lowest scores indicating the strongest pro-life attitudes. The seven items were highly intercorrelated, with a Cronbach’s α reliability coefficient = .71, in a sample of physicians from 10 European countries (Rebagliato et al., 2000). Internal consistency and reliability scores were adequate for the seven items in this study, with a Cronbach’s α = .81.
Further questions in the second section of the survey instrument included inquiries about physicians’ opinions and standpoints regarding: (1) situations where it is acceptable to withhold active resuscitation and/or ventilation, (2) barriers affecting EOL decision-making, (3) types of decisions made at EOL, (4) parents involvement in EOL decision-making, (5) nurses’ supposed roles in EOL decision-making, (6) roles of ethical committees in EOL decision-making, and finally, (7) rules and regulations relevant to EOL in neonates.
The third and fourth sections explored self-reported practices on EOL decision-making at the respondent’s work place. Results from these sections are not reported in this article.
Data sources and data collection
Data were collected between August of 2015 and February of 2016. Three research assistants approached physicians face-to-face, inviting them to participate in the study. After agreeing to take part in the project, the physicians were given the questionnaires to complete and return to the research assistants in self-sealed envelopes. No self-identifiers, such as names, were required in this study. Participation was based on the respondents’ free will. No incentives were provided to encourage participation.
The Scientific Research Committee at the School of Nursing, University of Jordan, reviewed and approved the ethical and scientific merits of the study. Further Institutional Review Board (IRB) approvals were obtained from three private hospitals and the Ministry of Health (MoH) in Jordan. The IRB at the MoH permitted the data collection in all of the public hospitals in Jordan. No IRB revisions were required by the remaining hospitals; instead, managerial and departmental approvals were obtained through the hospitals’ official channels.
Statistical methods
Only questionnaires containing 100% completed responses were included in the analysis. There was one contingency question asking about reasons for not including parents in EOLD, around half of the 75 participants provided answers to this question. The statistical package for social sciences for Windows version 21 (IBM® SPSS®, Armonk, New York, USA) was used for data analysis.
Descriptive statistics were applied to describe professional and demographic characteristics of the participating physicians and to summarize physicians’ responses to the study questions. Ordinal responses were grouped when necessary. Due to the small sample size, a multiple regression analysis was not conducted to evaluate whether the physicians’ demographic and professional variables were necessary to predict physicians’ pro-life attitude scores.
Results
Eighty-one physicians were employed fulltime in the selected hospitals during the data collection period, with one of their main clinical duties involving caring for newborns in the NICUs. All 81 physicians were invited and all agreed to participate in the study. Only 75 questionnaires with completed data, from 23 hospitals, were included in the final analysis. This reduced the response rate from 100% to 93% (75/81).
Male physicians constitute 69% of the participants; ages ranged between 30 and 39 for 50% of the sample. Slightly more than half (55%) of the participants were registered residents in pediatrics, with 60% having five or less years of overall clinical experience specific to newborns’ care (med = four years; interquartile range = 7). The majority of the physicians (95%) perceived an influence of EOLD on their personal lives. All participating physicians were Muslim; 77% considered their religious values as very important in their personal lives. Table 1 includes more information on the personal and professional characteristics of the sample.
Sample characteristics (N = 75).

Note: NICU: neonatal intensive care unit.
Attitudes of physicians to EOL decisions-making
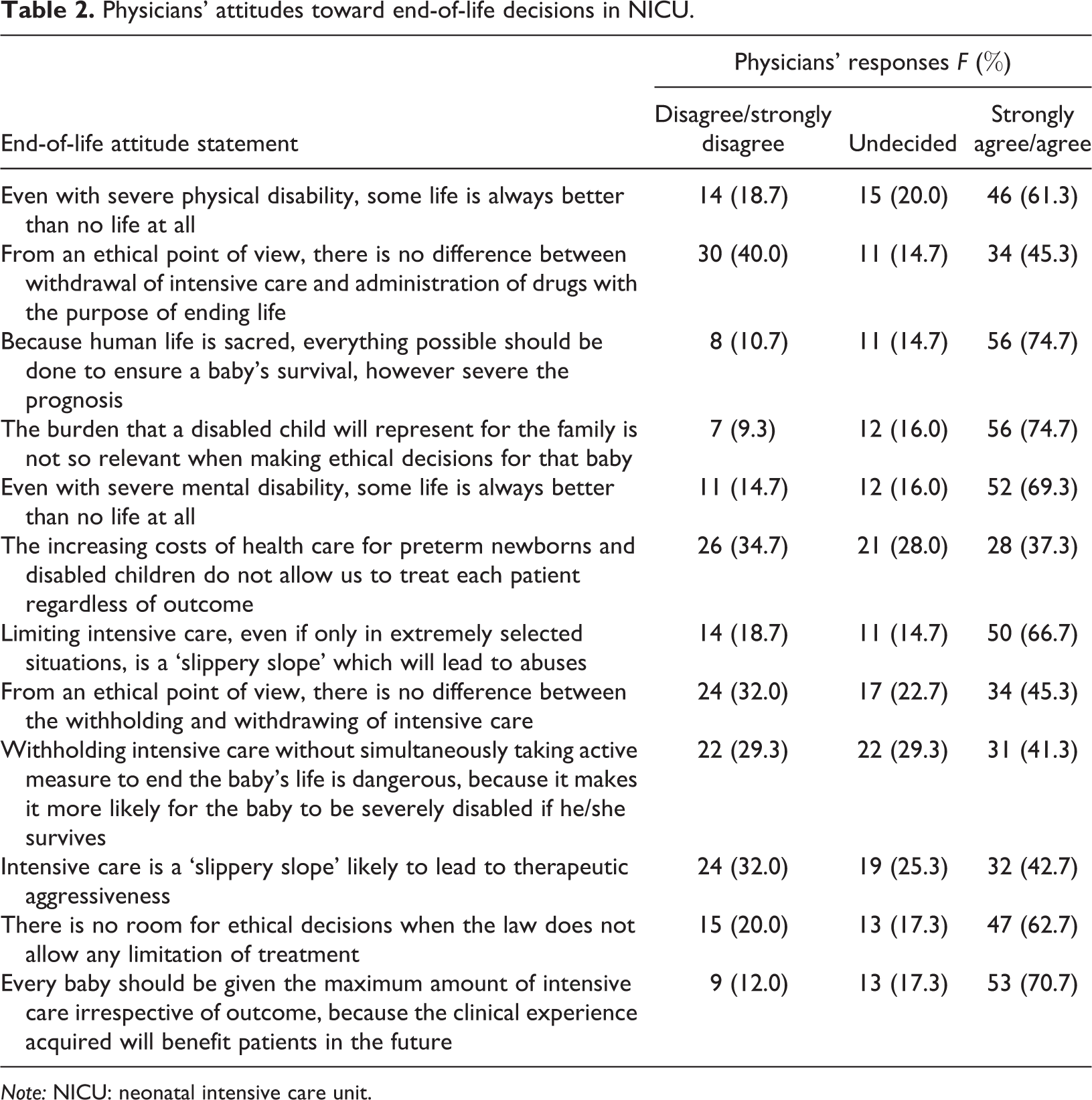
The attitude of most of the participants was supportive to employing the maximum interventions to sustain a newborn’s life in the NICU (Table 2). Most participants agreed with implementing life-sustaining measures, irrespective of (a) the severity of the newborns’ prognosis (75%), (b) the probability of physical disabilities (61%), (c) the probability of mental disabilities (69%), and (d) the burden of the children’s disabilities on their families (75%). While 67% of the participants considered decisions to limit intensive care in the NICU can lead to abuse, only 43% believed that intensive care might lead to therapeutic aggressiveness.
Physicians’ attitudes toward end-of-life decisions in NICU.
Note: NICU: neonatal intensive care unit.
EOLDs in newborns with specific medical conditions
Physicians were asked their opinions relating to EOLDs in the cases of (a) newborns with fatal conditions and (b) newborns with a poor clinical prognosis. One-third of the physicians (33%) indicated that setting limits to intensive interventions is justified in newborns with fatal conditions, while only 16% indicated it is justified for newborns with poor neurologic prognosis.
When asked about withholding emergency cardiopulmonary support in newborns with specific untreatable and disabling conditions, physicians’ attitudes varied, but only slightly (Table 3). Generally, most physicians were against making such EOLDs in newborns, an attitude which applied to almost all of the untreatable and disabling medical conditions seen in neonates. Thoracolumbar myelomeningocele, Down syndrome with severe congenital heart malformation, and severe asphyxia in full-term babies were on the top list for no limitation of life-sustaining interventions. That is between 84% and 88% of the physicians indicated that it is “never” to “sometimes” acceptable to withholding emergency cardiopulmonary support among newborns with these conditions. This attitude was contrary to newborns admitted to NICU for prematurity and anencephaly. A minimum of two-thirds of the participants (65%) agreed to the withholding of emergency cardiopulmonary support in (i) severe preterm infants, (ii) extremely low birth weight newborns (61%), and (iii) newborns with anencephaly (79%). Only in the chromosomal abnormality, trisomy 13, were the physicians inconsistent in their opinions about making EOLDs.
Physicians’ attitudes of withholding emergency cardiopulmonary support in neonates with specific medical conditions.

Barriers affecting EOLDs in NICUs
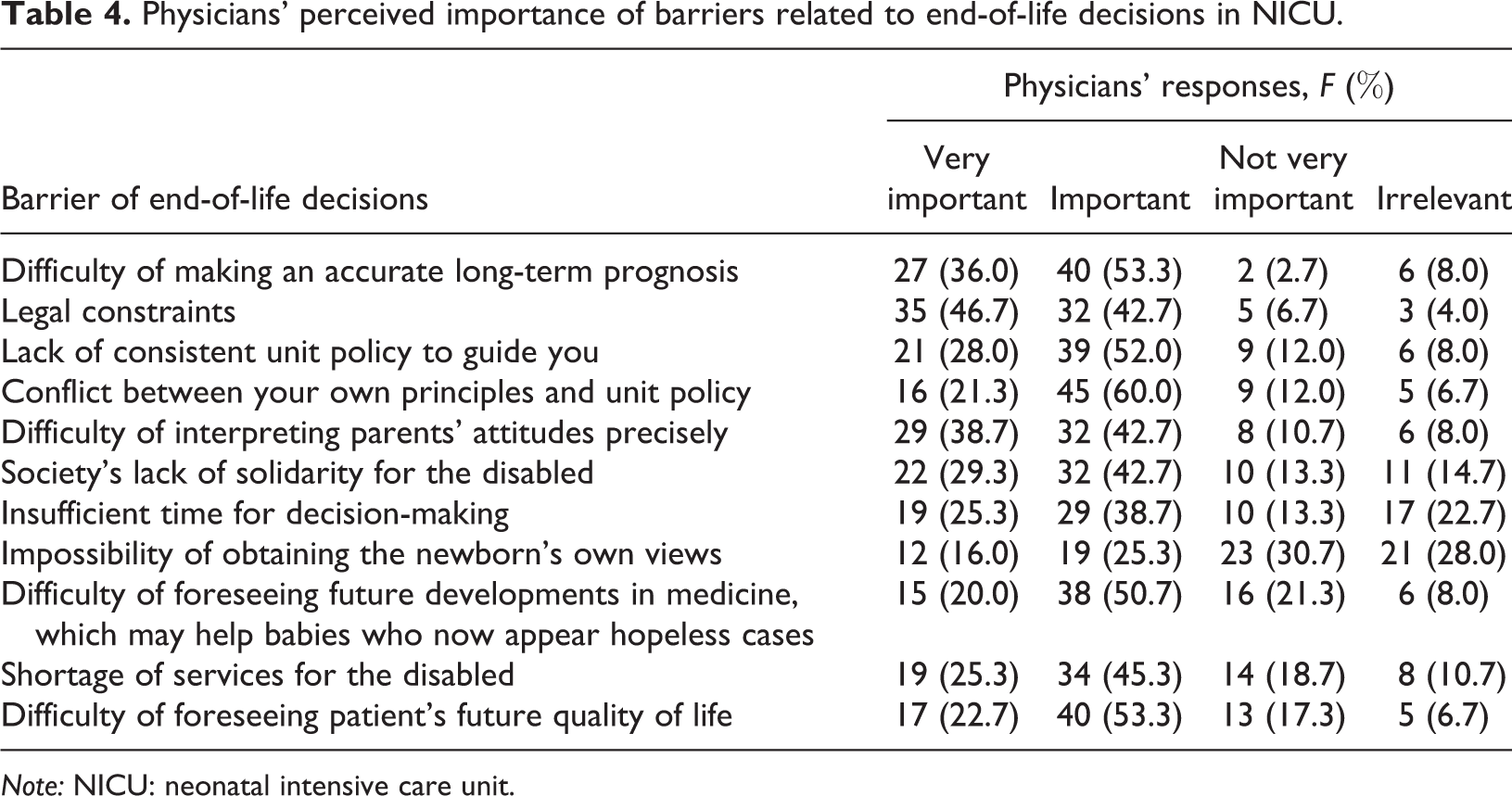
Physicians’ perspectives on the importance of barriers that may affect decision-making at neonates' EOL are detailed in Table 4. The highest rated barriers were (i) difficulty of making an accurate long-term prognosis (89%), (ii) legal constraints (89%), (iii) conflicts between physician’s own principles and unit policies (81%), (iv) difficulty of precisely interpreting parents’ attitudes (81%), and (v) lack of unit policies for guiding decision-making (80%). In addition, the difficulty of accurately foreseeing a newborn’s future quality of life was perceived important by 76% of the physicians. The impossibility of obtaining the newborn’s own views, if was possible, was basically irrelevant, according to 59% of the physicians.
Physicians’ perceived importance of barriers related to end-of-life decisions in NICU.
Note: NICU: neonatal intensive care unit.
Types of EOLDs in NICUs
Physicians’ perceived acceptability levels of specific EOLDs in NICUs are detailed in Table 5. Almost all of the participating physicians (95%) reported that the act of administering drugs in the NICU, for the purpose of ending a newborn’s life, was unacceptable. Decisions related to withholding and withdrawing life-sustaining interventions were perceived unacceptable by most of the physicians. Responses ranged from 79% of physicians against withholding intensive care to 65% against withdrawing life-saving drugs. Reponses were almost split equally on the acceptability of continuing current treatments without adding others, with 51% finding this decision to be unacceptable.
Physicians’ perceived acceptability of end-of-life decisions in NICU.

Note: NICU: neonatal intensive care unit.
Parents, nurses, and ethics committees’ involvement in EOLDs
Physicians’ responses regarding parents, nurses, and ethics committees’ involvement in EOLDs are detailed in Table 6. None of the physicians indicated that parents should be excluded from decision-making about their child’s future. Rather, 75% of the physicians reported that parents should have some explicit form of involvement in EOL decision-making.
Physicians’ responses toward parents’, nurses’, and ethics committees’ involvement in end-of-life decisions.
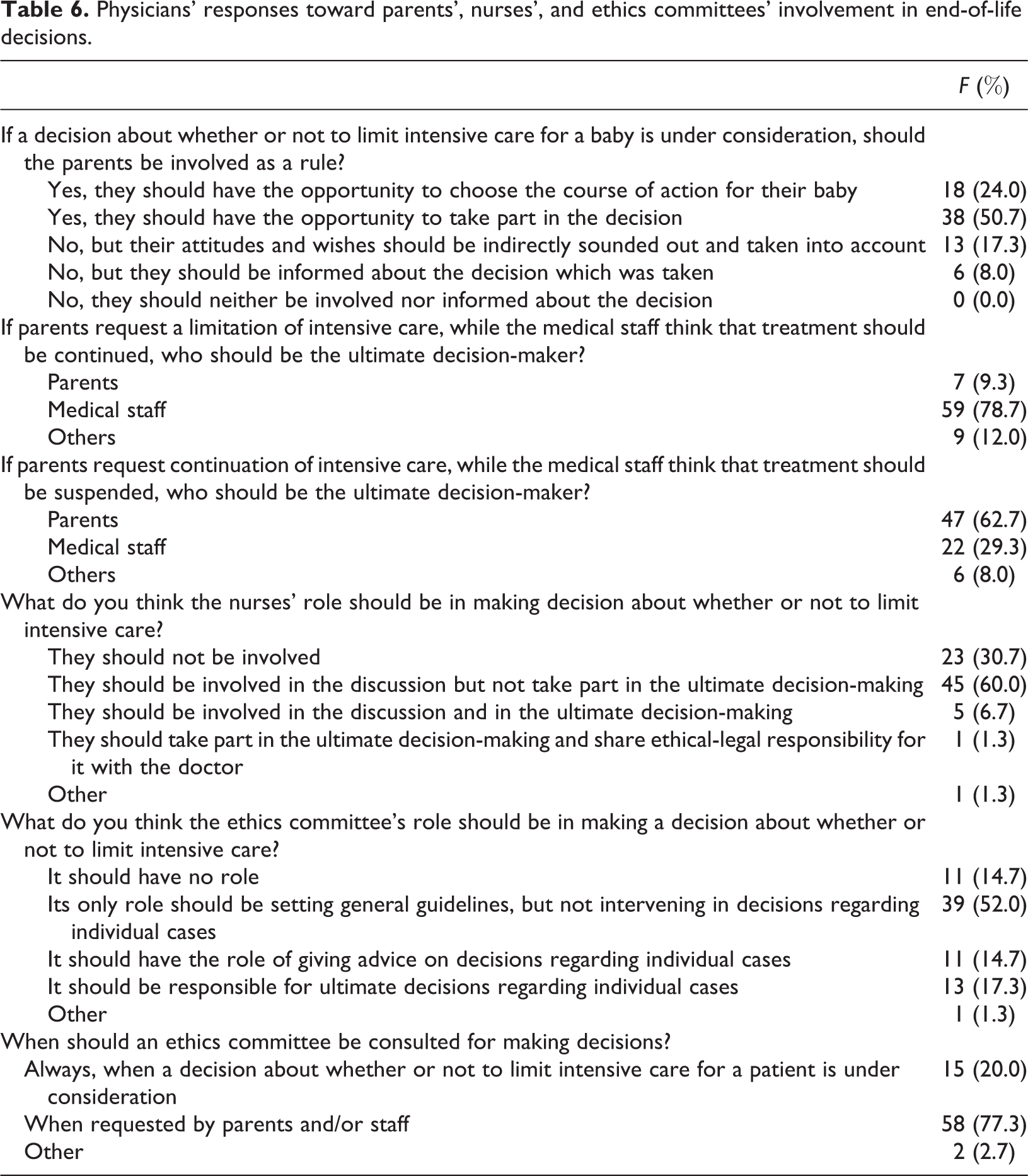
Physicians’ responses varied on who should be the ultimate decision-maker if conflict arose between physicians’ and parents’ opinions regarding minimizing life-support at newborns' EOL. If parents request a limitation to, or cessation of, intensive care while the medical staff think that treatment should be continued, 79% of the physicians indicated that the ultimate decision-making body should be the medical staff. However, 63% of the respondents indicated that the ultimate decision-makers should be the parents; if parents request continuation of intensive care, while the medical staff think that treatment should be suspended, that request should be granted.
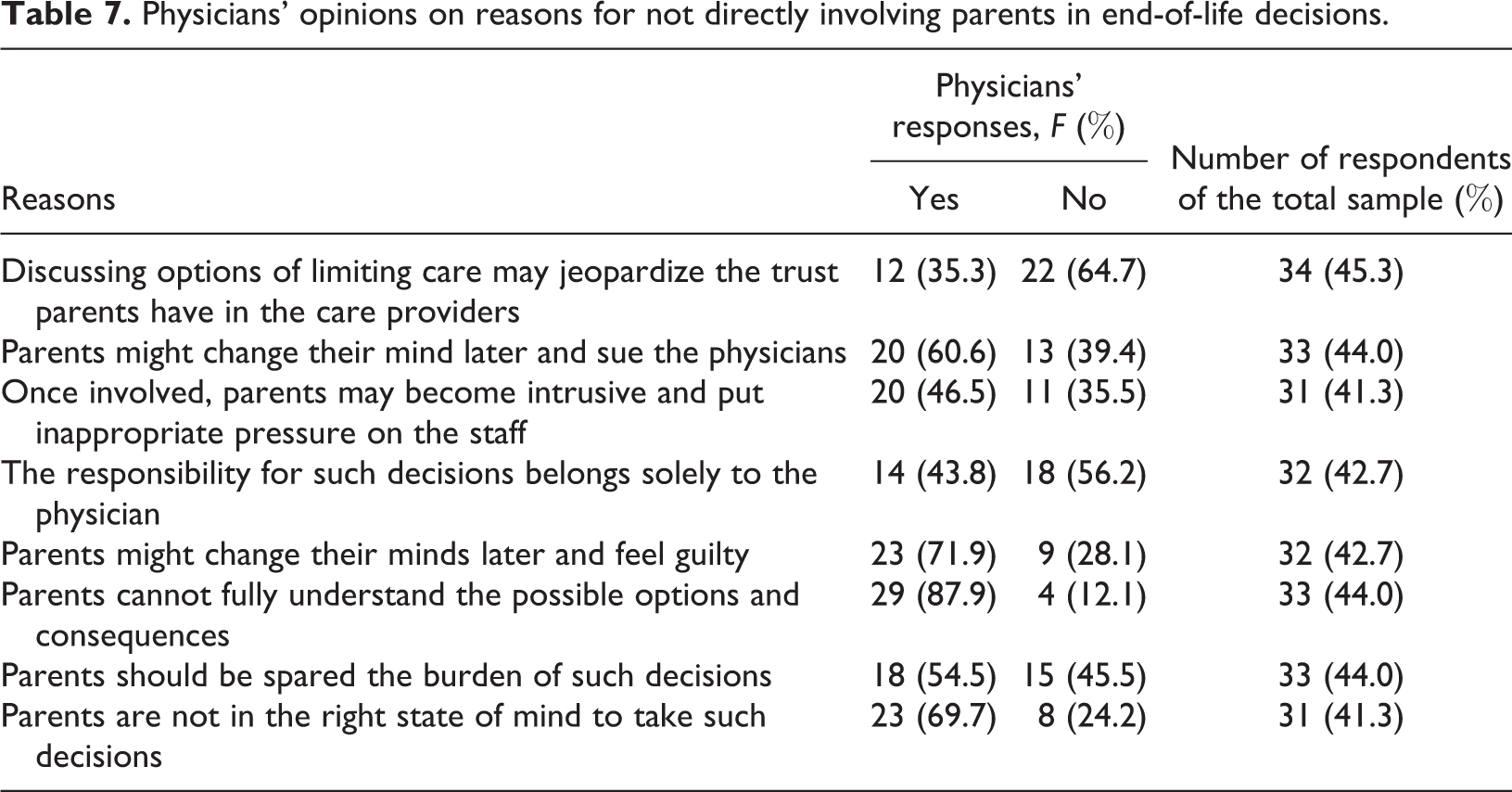
Less than half of the 75 physicians (32 of 75) answered the contingency question on reasons for not directly involving parents in EOLD in NICU, as shown in Table 7. ‘Parents’ limited capacity to fully understand the complexity of care’ was the most frequently offered reason for not directly involving parents in EOLD, reported by 28 of the 32 respondents. The next most common reason was ‘parents’ susceptibility to changing their minds regarding EOLD in order to avoid feeling guilty later on’, reported by 23 of 32 respondents. While 23 of 31 respondents were concerned about the issue of parents’ intense emotions that might blur their decision-making process.
Physicians’ opinions on reasons for not directly involving parents in end-of-life decisions.
Approximately two-thirds of the physicians (60%) indicated that nurses should be involved in the EOL discussions as well as in the ultimate decision-making, whereas almost one-third (31%) indicated that nurses should be excluded from the EOL decision-making process. The majority of physicians (84%) indicated that ethics committees should take some level of involvement in EOLD. Slightly more than half of the physicians (52%) indicated that the committees’ roles should be in setting general guidelines and not intervening in decisions regarding individual cases. Three-quarters of the physicians (77%) indicated that ethics committees should be involved as a result of requests from parents, physicians, or both.
EOL rules and regulations
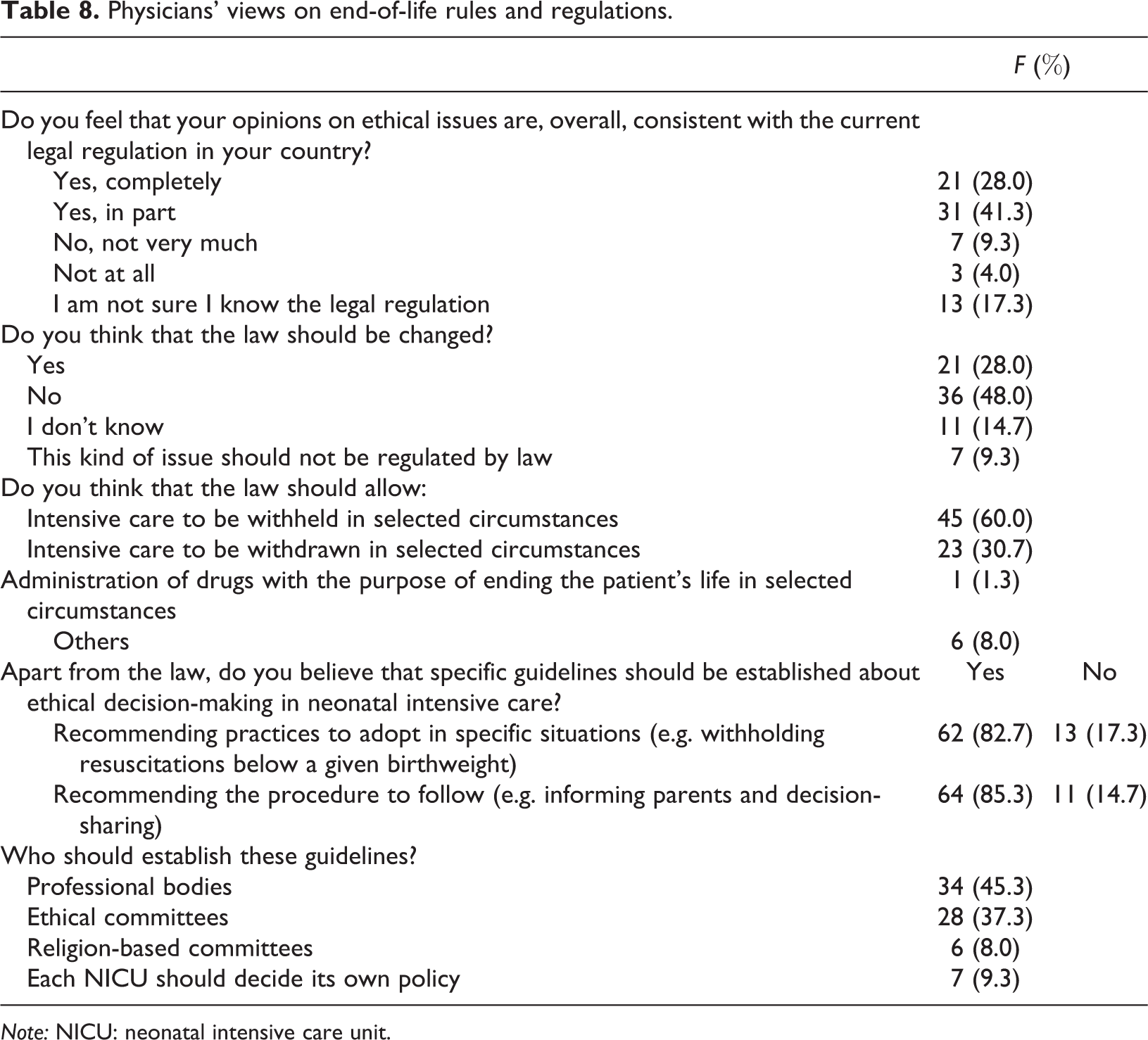
When physicians were asked their views on EOL rules and regulations (Table 8), 91% indicated that legislation should clearly allow intensive care to be withheld and withdrawn in selected specific circumstances. In addition to legislation, most of the physicians believed that specific ethical guidelines should be established to provide recommendations on EOLD practices in the NICU. These guidelines could be adopted (i) in specific ethical situations (83%) and (ii) to suggest acceptable procedures to follow (85%). Also, 85% of the respondents indicated that the guidelines should be established by professional bodies working together with ethical committees. Only 9% indicated that religion-based committees should establish such guidelines.
Physicians’ views on end-of-life rules and regulations.
Note: NICU: neonatal intensive care unit.
Discussion
This descriptive study investigated the standpoints and attitudes of physicians in Jordan regarding decision-making at EOL in 23 in-country NICUs. The physicians advocated life-sustaining and intensive interventions in NICU, irrespective of (a) the newborns’ clinical prognosis, (b) anticipated developmental outcomes, or (c) anticipated quality of life if the infant survived. The physicians’ attitudes toward life-advocacy were central and consistent in the overall findings of this study. The conflicting physicians’ reports of who should be the ultimate decision-maker, if contradictions rose between the physicians’ authority and the parents’ autonomy at a newborns’ EOL, have additionally supported the notion of strongly held pro-life attitudes among the physicians involved in this study. These conflicting reports involved a consensus among the physicians that the ultimate decision-maker should be the party who is supportive of life rather than the ending of life whether it was the physicians or the parents.
Most physicians were against minimizing life support at newborns' EOL, relative to almost all of the untreatable and disabling medical conditions identified in this study. This finding is also consistent with the overall life-advocacy attitudes of the respondent physicians. However, the study’s findings suggest that, to a certain degree, the quality of life and the issue of a disability-burden are not influential considerations for the physicians in Jordan when they are obliged to become involved in the EOL decision-making process. Possibly, the physicians in this study perceive that sustaining a newborn’s life while being hospitalized at their work place is their primary duty and obligation. While on the other hand, the newborns’ health condition or quality of life after discharge may not be perceived by the physicians as their immediate physical and emotional burden. Our outcome about quality of life consideration in EOL decision-making is contrary to the general attitude found among the physicians in other countries (Aladangady et al., 2017; Hellmann et al., 2016; Lam et al., 2016; Verhagen et al., 2010). The variability between this current study’s findings and those from other studies could support the notion of cultural relevance of EOLD practice in NICUs. Particularly important is the issue of ‘cultural sensitivity’ when discussions are being held regarding neonatal EOL decision-making.
Although ‘life advocacy’ was the dominant attitude among the physicians in this study, this attitude was not that obvious in the cases of premature and low-birth-weight infants. In relation to that point, Weiner et al. (2015) conducted a study to compare EOLD for preterm infants with those of infants with congenital anomalies. Their research suggested that the infants' medical diagnoses would influence the level of care provided at the time of an infan's death. It is possible the health-care professionals view EOLD for premature newborns differently, relative to other diagnoses. Specifically, decisions for extreme preterm infants were based on clinical judgments that further treatment would not be beneficial, rather than the perceived and anticipated poor quality of life (Weiner et al., 2015). In this study, the physicians’ opinions of EOLD, regarding EOLDs in preterm and low birth weights, could be explained by the findings of Weiner et al. (2015). This is especially true considering the conditions of the neonatal intensive care service provided in Jordan.
In Jordan, the clinical resources for optimal neonatal intensive care are significantly limited, a condition that is common among many developing countries. A panel of experts determined that 63% of neonates who died in Jordan received less than optimal intensive medical care (Batieha et al., 2016). In context, it is reasonable to conclude that the mortality rate among preterm newborns in Jordan is disproportionately high. The mortality rate among preterm newborns in Jordan was reported to be 30 times higher than it is among term neonates (Razeq et al., 2017). The physicians’ opinions on EOLD for the premature and low-birth-weight infants could be explained by the physicians’ perceived acknowledgment of what is clinically and currently possible to be implemented for these infants in Jordan’s NICUs.
Physicians’ opinions about the acceptability of different types of EOLDs indicate that physicians in Jordan prefer conservative measures when dealing with the challenging issue of a newborn’s EOL and the decisions that have to be made in such a situation. In the absence of rules and regulation on EOLD, the cultural perspectives on life and death in Jordan that are embedded in Islamic values can help explain the physicians, conservative approaches to EOLDs; attitudes that have been revealed in this study.
Islam, like many other religions, views life as sacred and a divine trust from God (Naga and Mrayyan, 2013). Therefore, saving life is a duty, while purposeful and unwarranted taking of human life is sinful and is not an acceptable option to escape suffering from disease and illness (Naga and Mrayyan, 2013; Rathor and Fauzi, 2012). These values might explain the physicians’ obvious opposition, as revealed in this study, to the active interruption of a newborn’s life via the use of lethal drugs. Within the same perspective, continuing treatment without adding others can be viewed by the physicians as a benign option at EOL and might encompass less moral responsibility on behalf of the physicians when compared, for example, to euthanasia or assisted suicide.
Studies from different countries indicate that withholding and withdrawing life-sustaining treatments were the most common EOLDs made in the world’s NICUs (Cuttini et al., 2000; Hellmann et al., 2016; Michel et al., 2018; Roy et al., 2004; Verhagen et al., 2010; Weiner et al., 2011). However, from a conservative perspective of EOLD, withholding and withdrawing life-sustaining measures are a sort of middle ground compromise that can be perceived to be shady and debatable areas. Withholding and withdrawing life-sustaining measures include some forms of clinical interference and interruption of life, but at the same time, they indirectly allow nature to take its course without the ‘artificiality’ of using advanced technology for the prolongation of life that may hold suffering and be of a poor quality. This current study’s findings further suggest that certain cohorts of physicians in Jordan face an ethical dilemma regarding the withholding and withdrawing of life-sustaining interventions relating to newborns receiving intensive treatment, a crucial issue that warrants investigation in further studies.
The dilemma of withholding and withdrawing treatment in an NICU is heightened when there is no clear legislation or guidelines to inform the medical professionals’ decision-making, as pointed out by the physicians in this study. It is both safe and somewhat disturbing to state that there is limited clarity in the policies about EOLD for neonates at the end of life in Jordan (Naga and Mrayyan, 2013) particularly those regarding neonates with poor prognosis and fatal conditions. The physicians in this study indicated a pressing need for clear guidelines to inform when and how to withhold and withdraw life-sustaining interventions relating to newborns in Jordan’s NICUs. Health-care professionals and ethical committees, rather than religious bodies, were recommended by the physicians in this study to establish such guidelines. The results of this research emphasize the need for (1) clear regulations and guidelines and (2) the establishment of ethical committees to inform and assist healthcare providers’ efforts during EOL decision-making in NICUs.
In conclusion, decision making and practices at EOL are globally controversial. In respect to the cultural and professional relevance of EOL decision-making, such decisions should be informed by the principles of non-malfeasance, beneficence, and respect for the dignity and humanity of the newborns and their families. An interdisciplinary approach is needed for such decisions to be made in the best interests of the newborns and their families. In addition, physicians have to respect a family’s autonomous choice of life-sustaining intervention for their dying newborns, if or when that child is located in an intensive care unit.
There were certain limitations in this study that should be corrected in future studies; one such limitation being the use of self-reported questionnaires for data collection. The issue of respondents providing ‘socially acceptable answers’ is a widely acknowledged pitfall associated with the use of self-reported questionnaires (Caputo, 2017; Dodou and de Winter, 2014; Van de Mortel, 2008). EOL decision-making may be considered a sensitive topic to talk about, given the conservative attitudes toward EOL practice that were evident in this study. The data collection procedures that were taken to protect the confidentiality and anonymity of the respondents in this study may have contributed to minimizing this limitation. Additionally, although efforts were made to enroll as representative a sample as possible, the sample size was relatively small when it came to the researcher running a fully powered predictive analysis. Nevertheless, this study elicited and then recorded initial, yet under-documented evidence, regarding physicians’ perspectives on (1) the level of neonatal nurses’ supposed involvement in making EOLDs and (2) the degree of supposed parents’ autonomy during EOL decision-making in Jordan. Both of these issues warrant further research and evaluation in order to describe the EOL decision-making process in Jordan more broadly and in greater depth, so as to improve EOL decision-making for newborns, both in Jordan and further afield.
Footnotes
Acknowledgements
The author would like to thank Dr Marina Cuttini and all the investigators and staff who took part in the EURONIC Project on ‘Parents’ information and ethical decision-making in neonatal intensive care units: staff attitudes and opinions’ (EU contract no. BMH1-CT93-1242; Principal Investigator: Marina Cuttini) for granting permission to use a modified version of the project’s questionnaire in this study and also thank the University of Jordan for providing the logistic and financial support while conducting the study.
Author contributions
Nadin M Abdel Razeq designed and carried out the full study and exclusively wrote the study manuscript in its final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Deanship of Academic Research and Quality Assurance at the University of Jordan.