
Abstract
The aim of this study is to assess the impact of preoperative comanagement with complex care pediatricians (CCP) on children with neuromuscular scoliosis undergoing spinal fusion. We performed chart review of 79 children aged 5–21 years undergoing spinal fusion 1/2014–6/2016 at a children’s hospital, with abstraction of clinical documentation from preoperative health evaluations performed regularly by anesthesiologists and irregularly by a CCP. Preoperative referrals to specialists, labs, tests, and care plans needed last minute for surgical clearance were measured. The mean age at surgery was 14 (SD 3) years; cerebral palsy (64%) was the most common neuromuscular condition. Thirty-nine children (49%) had a preoperative CCP evaluation a median 63 days (interquartile range (IQR) 33–156) before the preanesthesia visit. Children with CCP evaluation had more organ systems affected by coexisting conditions than children without an evaluation (median 11 (IQR 9–12) vs. 8 (IQR 5–11); p < .001). The rate of last-minute care coordination activities required for surgical clearance was lower for children with versus without CCP evaluation (1.8 vs. 3.6). A lower percentage of children with CCP evaluation required last-minute development of new preoperative plans (26% vs. 50%, p = .002). Children with CCP involvement were better prepared for surgery, requiring fewer last-minute care coordination activities for surgical clearance.
Keywords
Introduction
Children with medical complexity (CMC) have a high prevalence of functional limitations, multiple coexisting conditions, polypharmacy, and high health resource use (Berry et al., 2017b; Duckworth et al., 2014; McLeod et al., 2013; Martin et al., 2014, 2015; Mercado et al., 2007; Minhas et al., 2015; Murphy et al., 2006; Pugely et al., 2014; Ramo et al., 2014). CMC often undergo elective surgeries and related procedures to optimize their health, functioning, and well-being. Preparing CMC for upcoming surgery can be challenging because of the myriad health issues that could affect their perioperative health and safety. The American Academy of Pediatrics endorses perioperative involvement of general pediatricians to help recognize and address health problems that could jeopardize a child’s health as they undergo surgery (Anderson et al., 2014). General pediatrics involvement in preoperative care for children undergoing some surgeries, including spinal fusion for scoliosis, has been associated with increased attention and recommendations for the management of coexisting conditions (Rappaport et al., 2013b). This involvement has also been associated with shorter length of stay and decreased cost for the inpatient episode of care (Berry et al., 2017a; Rappaport et al., 2013a).
Although it is becoming more common for medical and surgical services to coordinate and comanage preoperative care for CMC, there is a critical need for more information on the value added by pediatricians in the preoperative preparation of CMC. For example, in our clinical experience, preoperative preparation for spinal fusion in CMC with neuromuscular scoliosis too often results in the discovery of significant coexisting health issues that can result in last-minute changes in care management (e.g. laboratory and radiographic testing, referrals to specialists, development of new perioperative care plans) and/or cancellation of surgery. Often, these children have active health problems (e.g. asthma or epilepsy) that require modifications in medication and/or equipment before they receive surgical clearance. This occurs despite involvement of well-trained, experienced surgical staff, because of the multi-morbidities, polypharmacy, and fragile health status of these children. It is challenging for physicians who are not involved in the chronic care management of these children to detect and address all of the health issues that could adversely affect perioperative health and safety.
Similar to many institutions, general pediatrics involvement in the preoperative preparation for spinal fusion at our hospital occurs for some but not all patients by a group of complex care pediatricians (CCP) dedicated to caring for CMC. CCP preoperative comanagement includes a generalized health assessment with a major focus on coexisting conditions, medications, assistive technologies, followed by care coordination work with orthopedic surgery clinicians to optimize the children’s health in advance of the preanesthetic evaluation and scheduled surgery. Therefore, we conducted the current study to (1) describe the preoperative management for children with neuromuscular scoliosis undergoing spinal fusion with and without CCP involvement in advance of the preoperative health assessment visit and (2) determine whether CCP comanagement was associated with fewer last-minute care management activities performed by anesthesiology providers for surgical clearance.
Methods
Study design, setting, and population
A retrospective chart review of 79 children with neuromuscular scoliosis aged 5–21 years undergoing spinal fusion at a tertiary-care, freestanding children’s hospital from January 2014 to June 2016 was performed. Underlying neuromuscular chronic conditions included—but were not limited to—cerebral palsy, muscular dystrophy, and spina bifida. Chart review of each child’s electronic health record was performed by two study team members (TG and BE) using a standardized data collection form. Verification of data abstracted from the review was verified by audit (performed by JB) on a 10% random sample of charts. Institutional Review Board at Boston Children’s Hospital approved this human subjects research.
Main outcome measures
The main outcome measures were the last-minute care activities performed during preanesthetic for spinal fusion. With this evaluation, all children had a preoperative health assessment visit performed by an anesthesia nurse practitioner and supervising anesthesiologist focusing on perioperative care and mitigating anesthesia risks. Each assessment included medical record review, current health history, review of systems, and physical examination. For children with active health issues discovered during the preanesthesia visit, care activities were performed to address them, including last-minute referrals and communications with primary and specialty care clinicians for surgical clearance; new development of perioperative care plans (e.g. intra- and postoperative intravenous antiepileptic medication plan for a child with epilepsy); and laboratory and radiographic testing.
Complex care pediatrics and surgery comanagement
Data were compiled in those patients who had preoperative comanagement with a CCP. This comanagement involved a comprehensive health assessment performed by clinicians (e.g. advanced practice nurses, physicians, and care managers) affiliated with an outpatient, general pediatrics clinical program dedicated to CMC. Most assessments required one hour of physician time and involved screening, review, and care management of each child’s coexisting conditions, with attention to the conditions (e.g. undernutrition, gastrointestinal dysmotility, neurogenic bladder, etc.) that might increase perioperative risk and compromised recovery. Each medication, including potential postoperative interruption of administration and side effect as well as dependence on assistive technology (e.g. cerebrospinal fluid shunt, tracheostomy, gastrostomy, etc.) was determined in advance of the preoperative anesthesia evaluation. CCP assessments were initiated with referrals from and communications with orthopedic surgery clinic staff. CCP collaborated with surgical providers to address all of the issues identified from the assessment that might compromise the children’s perioperative health and safety. There was no standardized clinical pathway that prompted a general pediatrics health assessment for all children undergoing spinal fusion. During the study period, 39 children (49%) had CCP comanagement.
Patient characteristics
Patient demographic characteristics included age at surgery, race/ethnicity, and gender. Patient clinical characteristics included the underlying primary neuromuscular chronic condition, coexisting chronic conditions, and American Society of Anesthesiologists Physical Status Classification System (ASA).
Statistical analysis
Using a Fisher’s exact test, the rates of last-minute, care activities performed during the preanesthetic evaluation performed shortly before spinal fusion were compared between patients with and without a preceding CCP health assessment. There were no missing data for any variables. The statistical significance threshold was p < .05.
Results
Study population
Seventy-nine children with neuromuscular scoliosis undergoing spinal fusion were included. Mean (standard deviation (SD)) age at surgery was 14 (3) years; 65% of children were non-Hispanic White and 56% were female (Table 1). The most common underlying neuromuscular conditions were cerebral palsy (43%) and spina bifida (15%). The most common coexisting conditions were epilepsy (58%), enterostomy (54%), dysphagia (49%), esophageal reflux (49%), and sleep apnea (46%). A wheelchair was used for mobility in 70% of patients and an ASA risk stratification score of III was noted in 80% of patients. Ninety-five percent of patients were admitted to the intensive care postoperatively. Mean (SD) inpatient length of stay for spinal fusion was 11.2 (6.6) days.
Characteristics of children with neuromuscular scoliosis undergoing spinal fusion.
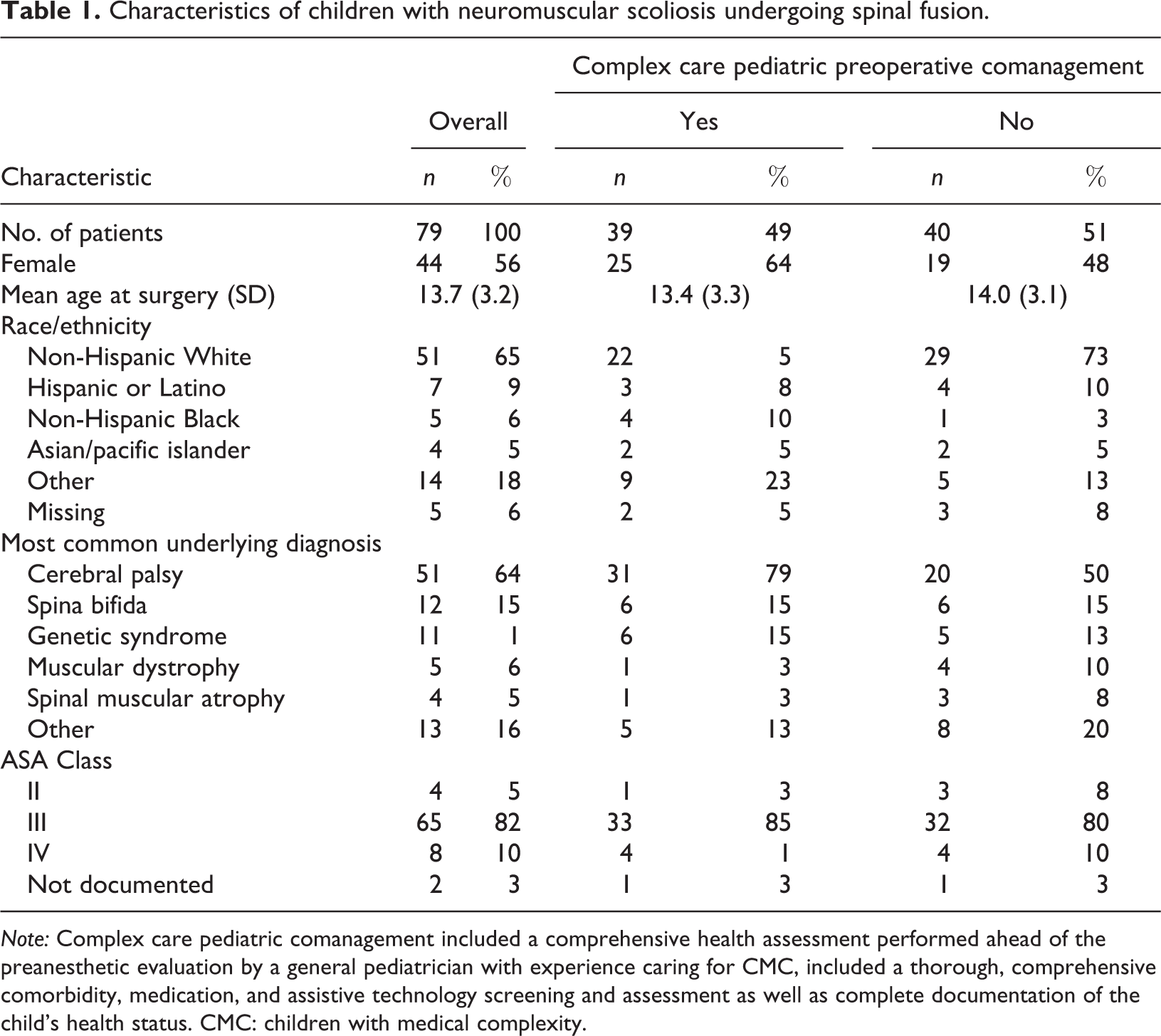
Note: Complex care pediatric comanagement included a comprehensive health assessment performed ahead of the preanesthetic evaluation by a general pediatrician with experience caring for CMC, included a thorough, comprehensive comorbidity, medication, and assistive technology screening and assessment as well as complete documentation of the child’s health status. CMC: children with medical complexity.
Preanesthetic evaluation for all children
The preanesthetic evaluation occurred a median 10 days (interquartile range (IQR) 3–15 days) in advance of scheduled spinal fusion. Every patient required at least one care coordination activity to optimize perioperative health and safety; the rate of activities was 2.7 per patient. Of these care activities, 38% were associated with intervention with respect to neurologic health, 25% cardiac health, 24% respiratory health, and 19% hematologic health (Supplemental Figure).
One of the most common last-minute, preanesthetic care activities (35%) was development of a perioperative care plan. Examples of these plans included adjustments of antiepileptic medications to prevent perioperative seizures (neurologic); assessment of cardiac function with echocardiogram for surgical clearance (cardiac); use of noninvasive positive pressure ventilation (respiratory) to help overcome the effects of restrictive lung disease; and development of perioperative platelet transfusion plans for children with thrombocytopenia (hematology).
The children requiring additional preanesthetic care activities included 13% for referrals to obtain surgical clearance, 18% for additional radiographic testing, 25% for additional laboratory testing, and 34% for communication of care coordination activities and findings across the children’s health-care providers.
Preoperative care activities for children with and without a preoperative complex care pediatrics comanagement
Preoperative CCP health assessments associated with preoperative comanagement occurred a median 63 (IQR 33–156) days in advance of the preanesthesia evaluation. Children with a CCP comanagement had more organ systems affected by their coexisting conditions than children without CCP comanagement (median 11 (IQR 9–12) vs. 8 (IQR 5–11) systems, p < .001). The rate of last-minute, preanesthesia care coordination activities required for surgical clearance, however, was lower for children with versus without CCP comanagement (1.8 vs. 3.6 per patient, p < .001). A lower percentage of children with a CCP comanagement required last-minute development of new perioperative plans (26% vs. 50%; p = .002) (Figure 1). Although not significant at the p < .05 level, a lower percentage of children with a CCP comanagement required last-minute referrals by the anesthesia team for surgical clearance (10% vs. 15%; p = .4) and fewer radiographic tests (13% vs. 23%; p = .2) (Figure 1).

Last-minute, care coordination activities required for preoperative clearance with versus without a upstream complex care pediatrics comanagement for children with neuromuscular scoliosis undergoing spinal fusion. *p < .05.
Discussion
The main findings from the current study suggest that preanesthetic evaluation and clearance for children undergoing spinal fusion for neuromuscular scoliosis is a labor-intense process characterized by high rates of last-minute care planning to optimize the child’s perioperative health and safety. We found that all children required at least one last-minute care coordination activity; one-half of children required three or more activities. Most of the activities involved perioperative care planning to address one or more coexisting health conditions. Children with early complex care pediatrics comanagement in their preoperative care had more organ systems affected by their chronic conditions when compared with children without this involvement. Yet, early CCP comanagement in preoperative care, including a general health assessment, was associated with less need for last-minute care coordination activities conducted by the preoperative anesthesia clinical team. Children with CCP comanagement were better prepared for surgery.
The labor-intensive, preoperative activities required to optimize the health of children with neuromuscular scoliosis undergoing spinal fusion observed in the current study complements prior literature. One recent study reported these children have a median of six chronic health conditions affecting multiple organ systems (Berry et al., 2017b). Clearance to undergo anesthesia and surgery safely is contingent upon making sure that these conditions are optimized. Identification of conditions that require attention during the preoperative anesthesia evaluation—which often occurs very soon or immediately before surgery—is not ideal. For some children, there may not be enough time to thoughtfully address the issues that arise (e.g. undernutrition, osteopenia, or worsening epilepsy). Postponing spinal fusion to address these issues is also not ideal, especially for those children with progressive scoliosis that could worsen their health.
The impact of CCP comanagement in helping to prepare children for spinal fusion in the current study adds to a growing body of literature supporting the use of multidisciplinary, preoperative care teams to optimize pediatric surgical outcomes (Miller et al., 2010). For example, preoperative health assessments performed by pediatric hospitalists have been associated with increased detection of coexisting conditions in children with neuromuscular scoliosis that might affect surgical and anesthesia safety as well as the development of perioperative plans to mitigate risks (Rappaport et al., 2013b; Rosenberg et al., 2014; Simon et al., 2007). Similar to the current study, the hospitalists discovered that neurologic-based plans (e.g. for epilepsy control) were one of the most common preoperative care planning needs (Rappaport et al., 2013b). Our study extends previous findings by suggesting that a multidisciplinary approach including early involvement of outpatient complex care clinicians can help identify and address health issues in children with neuromuscular scoliosis, thereby negating the need for last-minute care coordination immediately before surgery.
This study has several limitations. During the study period, there was no established protocol to request preoperative comanagement by a CCP provider. Chart review was not conclusive in determining the reason for CCP consultation and evaluation in some children and not others. It is possible that this consultation was requested for children with more coexisting conditions, making our findings of fewer last-minute care coordination activities for these children more significant. Moreover, there was no standardized approach to the structure of the CCP comanagement activities other than to review and address the children’s coexisting chronic health conditions. All of the CCP providers in the current study had extensive experience caring for and coordinating the care of children with medical complexity, including those with a high prevalence of coexisting complex chronic conditions. The findings may not generalize to the preoperative care received by general pediatrics with less experience caring for this population.
Despite the limitations of the current study, the findings may be useful for anesthesiologists, orthopedic surgeons, general pediatricians, other local practitioners, and patients and their families when striving to optimize the perioperative health and safety of CMC, especially those with neuromuscular scoliosis undergoing spinal fusion. As international attention to children with medical complexity continues to increase, the role of CCP providers—including nurses and clinicians of various fields and backgrounds—in models and systems of surgical care will evolve (Berry et al., 2017a; Brenner et al., 2017, 2018; Glassgow et al., 2017; Van Dongen et al., 2019). Although there were fewer last-minute care activities with upstream CCP comanagement, the rates of these activities were high for all patients. Therefore, further investigation is warranted to assess best practices and approaches for integration of these clinical stakeholders when developing and implementing perioperative care plans (Ferrari, 2017). The effects of these efforts on postoperative health outcomes and hospital resource use should also be explored.
Perhaps future studies might assess how anesthesia providers could educate and integrate with general CCP on their approach to preoperative clearance so that, ideally, the care coordination process could begin in advance for all CMC. Payers, policymakers, and administrators may also wish to explore how health-care payment might enable those opportunities (Gilchrist-Scott et al., 2017). A thoughtful, timely, integrated perioperative effort might be ideally positioned to optimize the health and safety of the children.
Supplemental material
supplement_material - Pediatric complex care and surgery comanagement: Preparation for spinal fusion
supplement_material for Pediatric complex care and surgery comanagement: Preparation for spinal fusion by Jay G Berry, Tyler Glaspy, Brian Eagan, Sara Singer, Laurie Glader, Norah Emara, Joanne Cox, Michael Glotzbecker, Charis Crofton, Erin Ward, Izabela Leahy, Joseph Salem, Michael Troy, Margaret O’Neill, Connor Johnson and Lynne Ferrari in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality (1P30HS024453-01).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.