
Abstract
The aim of this study were to evaluate pain, care burden, depression level, sleep quality, fatigue and quality of life (QoL) among a group of mothers of children with cerebral palsy (CP) and to compare their results with a group of healthy controls. The study involved 101 mothers who had children with CP and 67 mothers who had a healthy child as the control group. Pain, care burden, depression level, sleep quality, fatigue and QoL of all the participants were evaluated by the numerical rating scale, the Zarit care burden scale (ZCBS), the beck depression inventory (BDI), the Pittsburgh sleep quality index (PSQI), the checklist individual strength (CIS) and the short form-36 (SF-36), respectively. Numerical rating scale value was 3.57 ± 2.96 in the patient group. When the two groups were compared, the CP group showed higher scores for ZCBS, BDI, PSQI, total CIS and SF-36 subscales of general health and vitality whereas the scores for role physical, role emotional, mental health and mental component summary were found to be lower in the patients, compared to the control group. Reducing caregiving burden of the mothers’ by other family members and increasing psychosocial supports may help improve the mother’s health status.
Introduction
Cerebral palsy (CP) is one such developmental disorder that begins in early childhood as a set of functional limitations that stem from disorders of the developing foetal or infant brain (Myrhaug et al., 2014). The current estimated prevalence of CP in Turkish children between the ages of 2 and 16 years has been reported as 4 per 1000 live births (Garip et al., 2017). Many children with CP may have limitations in self-care functions such as feeding, bathing, dressing, grooming, ambulation and experience communicative, sensory and intellectual impairments (Svedberg et al., 2010; Tseng et al., 2016). The most children with CP are cared for by their mothers who are primary caregivers in developing countries such as Turkey (Farajzadeh et al., 2018; Garip et al., 2017). Caregiving covers a very wide range of activities such as heavy lifting and turning, bathing, helping the child to use the toilet, getting the child to sleep, dressing and assisting the transfer. Manual handling can put physical strain on mothers and be a contributing factor to a higher pain severity (Mörelius and Hemmingsson, 2014; Terzi and Tan, 2016). In some cases, the provision of such care has sometimes proved to be detrimental to the physical health of mothers of children with CP and to cause some psychiatric conditions such as stress, anxiety and depression in them (Garip et al., 2017; Khanna et al., 2015; Khayatzadeh et al., 2013; Svedberg et al., 2010). The mothers of children with CP report not only declined physical and mental health, but also fatigue and impaired quality of sleep (Garip et al., 2017; Tseng et al., 2016). The prevalence of persistent sleep problems and need for parental night-time attention is high among children with CP (Mörelius and Hemmingsson, 2014). Fatigue is one of the most common complaints of mothers with neurological disorders including CP, but little information is known about its impact on the mothers of children with CP (Davis et al., 2010; Garip et al., 2017). When a more holistic view of health was considered, mothers of children with CP were found to have significantly lower quality of life (QoL) (Dehghan et al., 2016; Garip et al., 2017; Ones et al., 2005). Although long-term caregiving can be detrimental to women’s QoL, only a few studies have directly addressed the effects of children with disability on a mother’s QoL (Khayatzadeh et al., 2013; Tseng et al., 2016).
Despite its importance, the topic of health status of mothers in the context of CP has been poorly investigated (Byrne et al., 2010; Wijesinghe et al., 2015). A few studies have assessed the aforementioned common caregiver problems, such as pain, care burden, increased incidence of depression, sleep disorders, fatigue and impaired QoL in mothers of children with CP separately (Davis et al., 2010; Garip et al., 2017; Khanna et al., 2015; Khayatzadeh et al., 2013; Mörelius and Hemmingsson, 2014; Ones et al., 2005; Terzi and Tan, 2016), but none has examined all these problems collectively in the same patient group. To the best of our knowledge, this is the first study to investigate these problems collectively in the mothers of children with CP in the same patient group. The aims of this study were to evaluate pain, care burden, depression level, sleep quality, fatigue and QoL among a group of mothers of children with CP and to compare their results with a group of healthy controls.
Methods
Participants
The study was approved by the Research Ethics Committee of the Medical Faculty and was conducted in accordance with the Declaration of Helsinki. For the present study, 101 mothers who have a child diagnosed with CP were consecutively contacted by telephone at the Selcuk University Medical Faculty between November 2015 and January 2017. Each mother was informed about the study during the telephone call and those who agreed to answer a detailed questionnaire were included in the study. The control group consisted of 67 mothers who have a healthy child. The control group answered the questionnaire with face to face interview.
Children were included if they were diagnosed with CP and type of CP was identified by a paediatrician, paediatric neurologist or physiatrist; and they were aged 18 years or younger. Mothers were included if mother is the most responsible for the day-to-day decision making and care of the child; and children diagnosed with CP lived with them. Exclusion criteria were as follows: (a) children suffered from neurodegenerative diseases or psychiatric illnesses; (b) primary caregiver was not mother; (c) mothers were diminished cognitive function who were unable to complete the questionnaire; (d) mothers provided care for an elderly, chronically ill or disabled relative; (e) mothers had a history of chronic illness, such as diabetes, cardiovascular or pulmonary disease, rheumatologic, orthopaedic, musculoskeletal diseases or any psychiatric disorder; (f) mothers cared for another child below the age of two or mothers were pregnant and (g) mothers had another child at home with special health care needs. Inclusion criteria of controls were (a) mothers had a healthy child and lived together; (b) mothers lacked a history of psychological disorders; (c) mothers did not had chronic disorders; (d) mothers were not pregnant; (e) mothers did not had rheumatologic, orthopaedic and neurologic problem and (f) mothers did not had a disabled person for whom the mother provides basic care.
Measures
Measure of pain
Information on the location of the most painful joint (neck, back, low back, hip, knee, ankle, shoulder or wrist) was obtained from the mothers by a researcher at the interview. Mothers were evaluated for the most painful joint pain during activity; a numerical rating scale (NRS) was used to evaluate pain. This scale ranges from 0 to 10 (with 0 points = no pain and 10 points = severe pain) (Pinto et al., 2013).
Measure of care burden
The care burden of all the participants was evaluated by the Zarit care burden scale (ZCBS). The ZCBS assesses the stress suffered by those who give care to the persons in need. The scale consists of 22 questions and has a likert-type assessment ranging from 1 to 5 as “never,” “rarely,” “sometimes,” “often” or “almost every time.” The highest score is 110 while the lowest is 22 (Ozlu et al., 2009). Questions in the scale are generally about social and emotional aspects, and high scores from the scale indicate that the care giver’s burden is high (Ozlu et al., 2009).
Measure of depression level
The depression level of all the mothers was evaluated by the Beck depression inventory (BDI). BDI is a 21-item self-report questionnaire used to assess the severity of depression. The questionnaire has four possible answers, graded from 0 to 3, with higher values representing a higher level of depression. The highest possible score is 63 points (Beck et al., 1997). The score greater than 17 denotes the presence of depression.
Measure of sleep quality
The sleep quality of all the mothers was evaluated by the Pittsburgh sleep quality index (PSQI). The PSQI consists of a total of 24 questions, 19 of which are self-rated by the individual and 5 of which are answered by the partner or roommate of the individual. The total score ranges between 0 and 21 points with higher values representing worse sleep quality. Based on the total score, sleep quality is rated as good (0–5 points) or poor (6–21 points) (Albayrak et al., 2015). In this study, total of 24 questions were answered by the mothers.
Measure of fatigue
The multidimensional checklist individual strength (CIS) was used to measure chronic fatigue. It consists of 20 statements, the answers to which are scored on a 7-point likert scale. The CIS is divided into four dimensions: (1) the subjective experience of fatigue, (2) reduction in motivation, (3) reduction in activity and (4) reduction in concentration. A total CIS score is obtained by summing the scores from the four dimensions. Higher scores indicate a higher degree of fatigue, more concentration problems, lower motivation and less activity (Ergin and Yildirim, 2012). The total CIS score was evaluated in the present study.
Measure of QoL
The QoL of all the mothers was evaluated by the short form-36 (SF-36) questionnaire. The SF-36 consists of 36 questions relating to the individual’s perception of how they function in eight dimensions of daily life resulting in eight subscale scores (physical functioning (PF), role physical (RP), bodily pain (P), general health perceptions (GH), vitality (V), social functioning (SF), role emotional (RE) and mental health (MH)) and two summary scores (physical component summary score (PCS) and a mental component summary score (MCS)). All items pertaining to each scale are summed and transformed to form a scale from 0 to 100, where a lower score indicates a worse state of health or well-being (Byrne et al., 2010).
Measure of motor disability
The severity of a child’s motor disability was assessed using the gross motor function classification system (GMFCS). The GMFCS is a 5-level system providing a standardized classification of the patterns of motor disability for children with CP by their age-specific gross motor activity. Distinctions between the five levels, ranging from levels I (least limitation) to V (greatest limitation), are based on self-initiated manual ability, with particular emphasis on handling objects in an individual’s personal space (Palisano et al., 2000).
Information on the characteristics of children (age, gender and body mass index (BMI)); time since diagnosis; type of CP (spastic quadriplegia, spastic diplegia, spastic hemiplegia and dyskinetic, mixed); GMFCS level; the use of assisted devices (wheelchair, walker, canedy, ankle foot orthosis, knee ankle foot orthosis and none); information related to other diseases, disorders or conditions (hearing loss, vision loss, urinary incontinence, fecal incontinence, mental retardation, epilepsy, drooling and dysphagia) diagnosed by medical doctors was collected from hospital charts.
Information on the characteristics of mothers (age, marital status and occupation); comorbid diseases (diabetes mellitus, hypertension, pulmonary disease, coronary artery disease or lack of comorbid diseases); amount of time spent caring for a day (the number of hours per day spent with the child); on the location of the most painful joint (neck, back, low back, hip, knee, ankle, shoulder and wrist) and ratings NRS, ZCBS, BDI, PSQI, CIS and SF-36 scales were recorded from the standard questionnaire presented to mothers during the interview.
Procedure
A pilot study of mothers who have a child diagnosed with CP (n = 6) was conducted by telephone in November 2015, with additional face-to-face interviews being conducted to obtain feedback from four of the mothers. The questionnaire was found to have good face validity and only minor amendments to the survey instrument were needed. The main study was carried out that the mothers who have a child diagnosed with CP answered the questionnaire by telephone interview and the mothers who have a healthy child answered the questionnaire with face to face interview.
Statistical analysis
Data analysis was performed the statistical package for the social sciences. Descriptive statistics for categorical data were presented as numbers and percentages, whereas continuous variables were presented in the form of mean and standard deviations. Clinical data conforming to a normal distribution were compared using a Student’s t test. Nonparametric Mann–Whitney or Chi-square tests (χ 2) were thus performed to compare socio-demographic and clinical measures between the two groups. Pearson’s or Spearman’s correlation coefficient was calculated to investigate the associations between the variables. Correlations from 0 to .25 were considered as “no correlation,” .25 to .50 as a “mild-moderate correlation,” .50 to .75 as a “strong correlation” and between .75 and 1.00 as a “very strong correlation.” The significance level was set at p < .05 (two-tailed).
Results
Of 114 mothers who have a child diagnosed with CP, six were excluded because they did not want to answer the standard questionnaire via telephone interview and seven were excluded because the telephone number was incorrect. The study was performed on 101 mothers who had children with CP (43 girls and 58 boys) and 67 mothers who had a healthy child as the control group. Demographic and clinical data of children are shown in Table 1. Mean age was 34.93 ± 8.7 years for the mothers in the CP group and mean age was 34.28 ± 7.51 years for the mothers in the control group. The demographic and clinical characteristics of the mothers are presented in Table 2.
Demographic and clinical data of children.
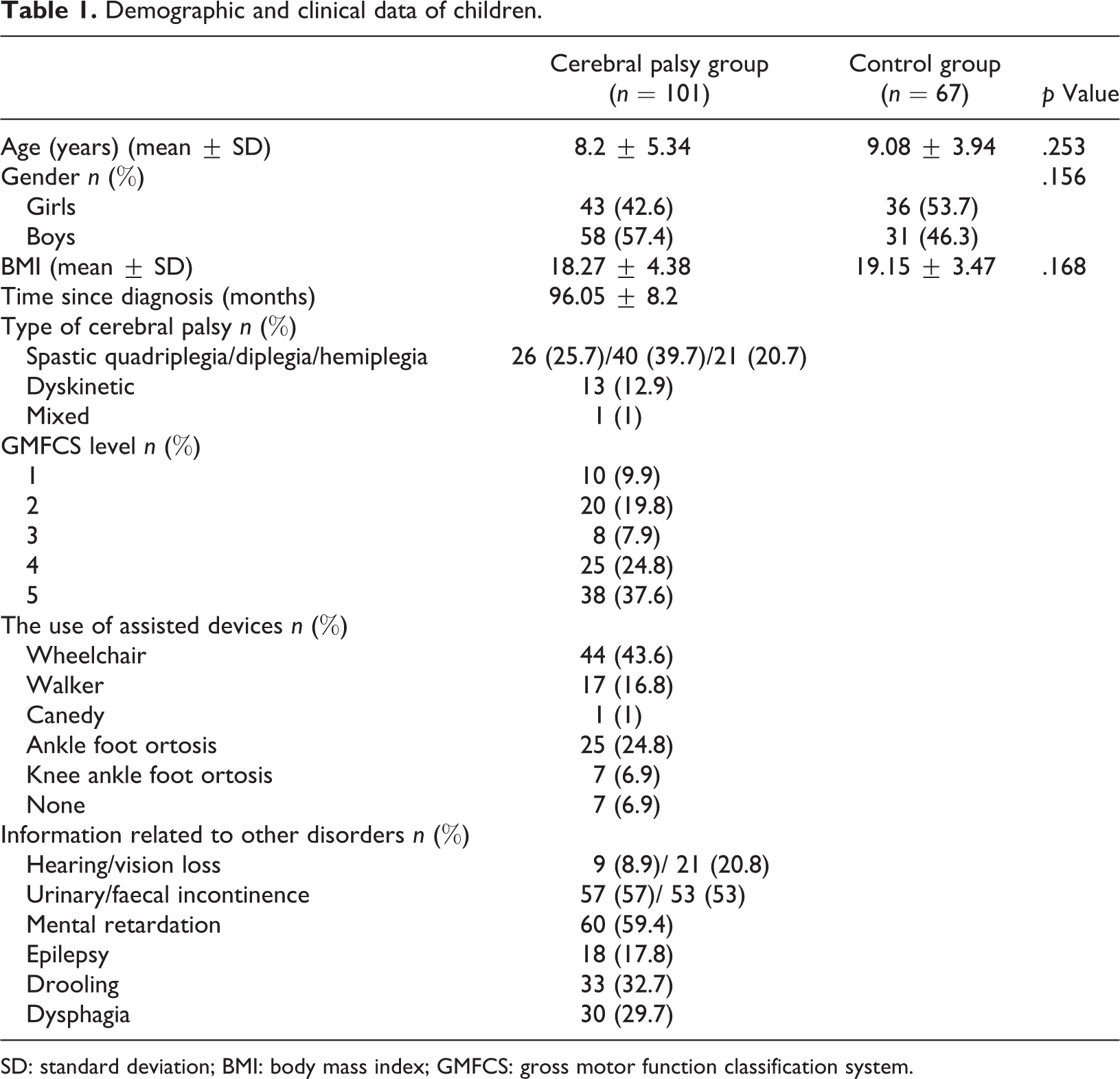
SD: standard deviation; BMI: body mass index; GMFCS: gross motor function classification system.
Demographic and clinical data of the mothers.
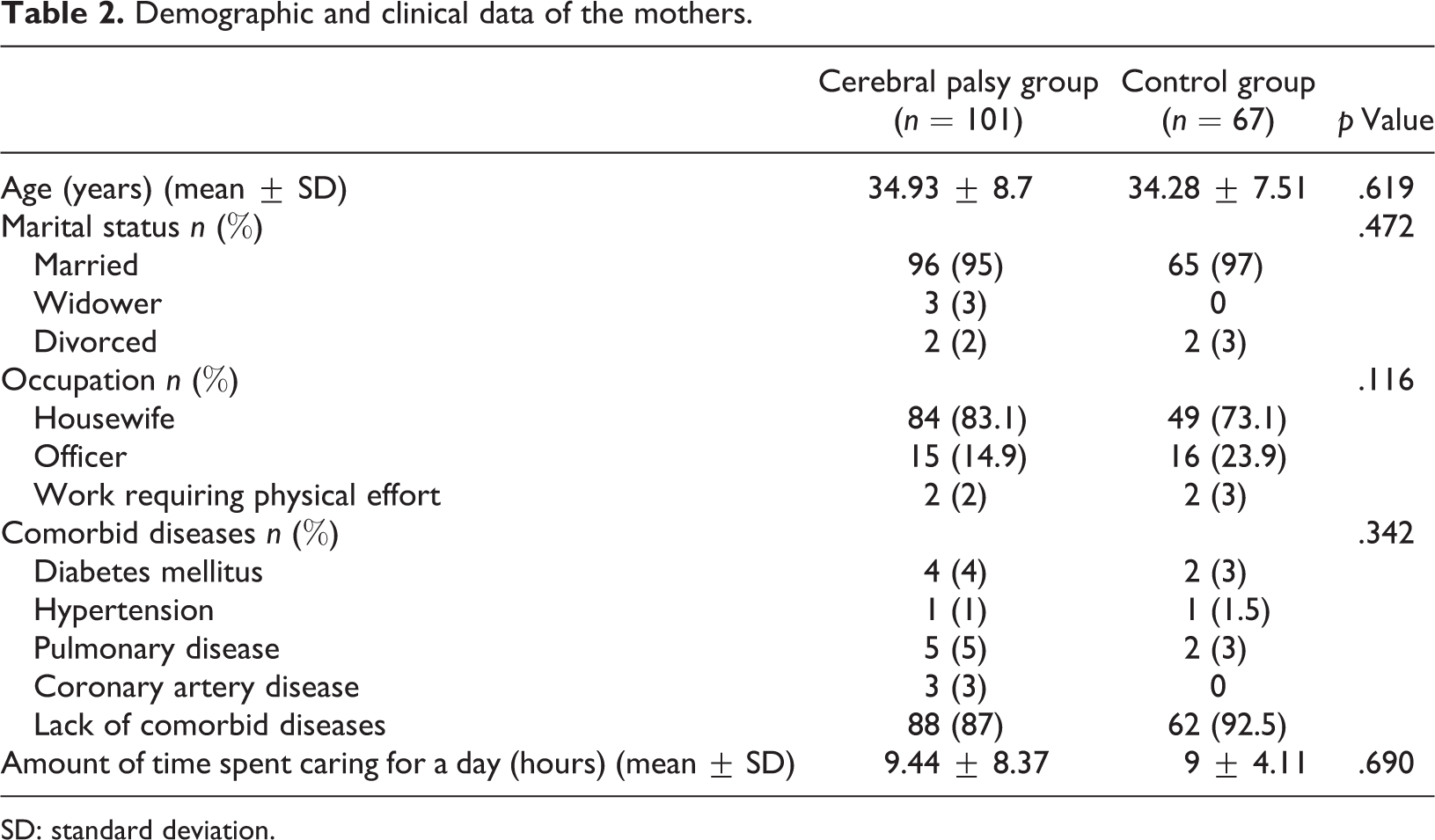
SD: standard deviation.
The severity and the characteristics of pain are shown in Table 3 for the mothers.
The severity and characteristics of pain in the mothers of children with cerebral palsy and the mothers of healthy children.

NRS: numerical rating scale; SD: standard deviation.
When the two groups were compared, the CP group showed higher scores for ZCBS, BDI, PSQI, total CIS and SF-36 subscales of general health and vitality whereas the scores for role physical, role emotional, mental health and mental component summary were found to be lower in the patients, compared to the control group (p < .05; Table 4).
The comparison of the mothers of children with cerebral palsy and the mothers of healthy children based on ZCBS, BDI, PSQI, total CIS and SF-36 subscale scores.
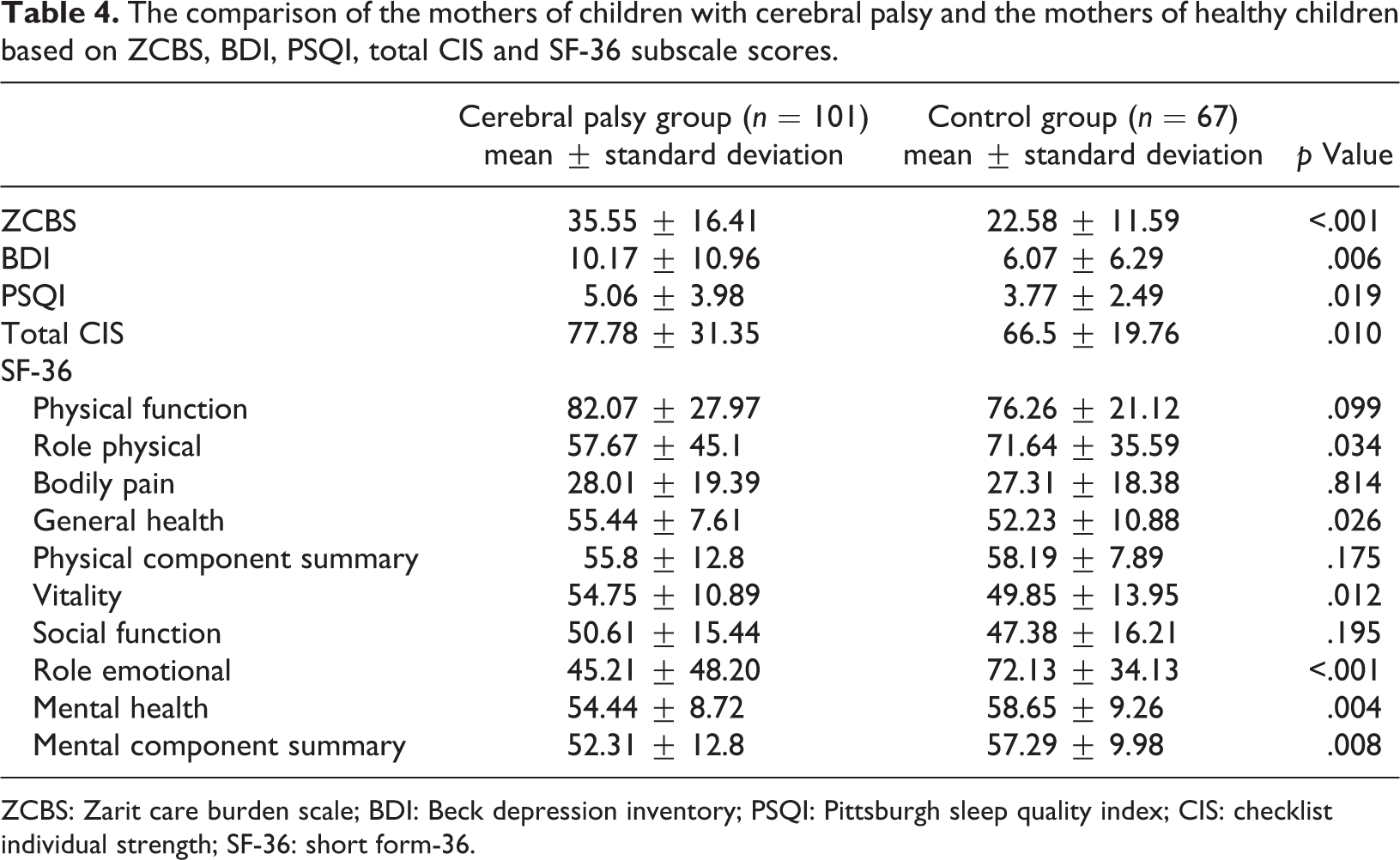
ZCBS: Zarit care burden scale; BDI: Beck depression inventory; PSQI: Pittsburgh sleep quality index; CIS: checklist individual strength; SF-36: short form-36.
In the correlation analyses of the NRS, ZCBS, BDI, PSQI, total CIS and SF-36 subscales of physical component summary and mental component summary from the CP group are shown in Table 5.
Intercorrelations among study variables in the cerebral palsy group.

BMI: body mass index; GMFCS: gross motor function classification system; NRS: numerical rating scale; ZCBS: Zarit care burden scale; BDI: Beck depression inventory; PSQI: Pittsburgh sleep quality index; CIS: checklist individual strength; SF-36: short form-36.
Discussion
Some studies have assessed pain, care burden, increased incidence of depression, sleep quality, fatigue and impaired QoL in caregivers of children with CP separately (Davis et al., 2010; Garip et al., 2017; Khanna et al., 2015; Khayatzadeh et al., 2013; Mörelius and Hemmingsson, 2014; Ones et al., 2005; Terzi and Tan, 2016), to the best of our knowledge, this is the first study to investigate these problems collectively in the mothers of children with CP in the same patient group. In this study, it was found that the mothers of children with CP had higher pain, care burden, depression level, worse sleep quality, increased fatigue and lower mental component of the QoL in comparison to matched healthy controls.
The mothers of children with CP provide active support to their children in terms of feeding, bathing, dressing, ambulation and assisting the transfer during which they may be exposed to problems in the musculoskeletal system (Terzi and Tan, 2016). In the study of Kaya et al. (2010), it was found that musculoskeletal and lumbar pain were significantly higher in the mothers of children with CP, and the incidence of low back pain was 44.7% in this group. The study of Tong et al. (2002) found that the most common type of pain was low back pain (71.1%) in female caregivers of children with physical disabilities. Consistent with these studies, the severity of pain evaluated with the NRS was detected to be higher in the mothers of children with CP in this study. In the present study, the mothers who had a history of rheumatologic, orthopaedic and musculoskeletal diseases were not included into the study to assess the complaints of pain objectively. The most painful site was lumbar joints followed by neck joints in the present study. The incidence of low back pain was 34.6% and neck pain was 23.8%. Therefore, these joints in particular may be examined in the mothers of children with CP presenting with pain. In addition, exercise program and patient education may be provided as a prophylactic measure.
The majority of children with CP are cared for at home by mothers, and this brings with it some challenges. These challenges, frequently referred to as the caregiver burden, can affect aspects of mothers’ and children’ well-being (Wijesinghe et al., 2015). In this study, it was found that care burden was significantly higher in the mothers of children with CP in comparison to control group. Social support might reduce the increased care burden associated with greater functional impairments.
There is an increased incidence of depression among mothers of children with CP (Garip et al., 2017; Khanna et al., 2015). The study of Unsal-Delialioglu et al. (2009) found that the stress resulting from dealing with a chronic condition is a risk factor for the development of depression in the mothers. Also, Yilmaz et al. (2013) reported that disability in a child and accompanying challenges may negatively affect psychological health of mothers of children with CP. The round-the-clock nature of caregiving often leads caregivers to feel alone and think nobody understands their condition. After suffering from care burden, caregivers visits to the doctor have negative thoughts and feelings of uncertainty. All of these contribute to the increased incidence of depression in the mothers of children with CP. Our results supported previous studies (Garip et al., 2017; Khanna et al., 2015; Unsal-Delialioglu et al., 2009; Yilmaz et al., 2013) that suggested depression levels are higher in the mothers of children with CP when compared with controls. Reducing caregiving burden of the mothers’ by other family members and increasing psychosocial supports may help improve the mother’s mental health, which may also consequently improve the psychosocial well-being of their children with CP.
The mothers of children with CP reported impairment in sleep quality and fatigue, both were common in the disease process (Garip et al., 2017; Tseng et al., 2016). The children with CP who had sleep problems and need for parental night-time attention were associated with mothers’ poor sleep quality (Mörelius and Hemmingsson, 2014). Sleep quality is important and could have contributed to higher error rates and fatigue at home and work (Khayatzadeh et al., 2013; Scott et al., 2006). There are many factors such as poor levels of physical exercises, decrease in perceived social support, medical and therapy appointments which may cause fatigue in the mothers of children with disability (Slater, 2010). In a study where 90 mothers of CP children were evaluated in terms of their fatigue levels, it was reported that fatigue levels of mothers with CP children were higher than those with healthy children (Garip et al., 2017). As consistent with these studies, the mothers of children with CP in our study had low sleep quality and higher level of fatigue when compared with controls. The mothers who have low sleep quality and increased fatigue may negatively affect the efficacy of treatment programme for CP children.
When the amount of the burden and difficulties of caregiving increases, mothers feel hopeless and as a result their QoL decreases significantly (Farajzadeh et al., 2018; Garip et al., 2017). Some of the studies found that providing care for a child with functional limitations and long-term dependence influenced mothers’ QoL (Garip et al., 2017; Khayatzadeh et al., 2013). Mörelius and Hemmingsson (2014) found that parents of children with CP were at risk for impaired QoL, especially with regard to vitality, social functioning and depressive emotions. In the present study, significantly worse scores for the mental component summary (including vitality, social function, role emotional and mental health) were observed during the assessment of the QoL in the mothers of children with CP when compared with control mothers. Parental distress and mothers’ ratings of their own mental symptoms negatively influence the most important aspects of mothers’ life especially mental health. It is probably because mothers provide lifelong care to their CP child at home throughout a whole day such that they have faced long-term stressors, making them suffer from mental symptoms. In the present study, physical component summary scores of SF-36 were lower in the mothers of children with CP when compared with control mothers, but there was no significant difference in both groups. If more mothers of children with CP are evaluated, it may be seen that the physical component of the QoL is significantly impaired in this study.
In the present study, it was observed that there was a positive correlation between BMI measures in children with CP and mothers’ pain, depression level, sleep quality and fatigue. To the best of our knowledge, this is the first study to emphasize the importance of BMI measures in children with CP. The higher BMI measures in children may be a disadvantage of caregiving for the mothers. Therefore, the exercise programme and nutrition of children can be regulated correctly and their weight gain can be kept under control.
Conflicting results about the relationship between GMFCS level and mothers’ pain severity, depression level, sleep quality, fatigue and QoL have been reported by previous studies (Tuzun et al., 2010; Turkoglu et al., 2016). GMFCS level of the child was correlated with ZCBS scores, but gross motor function was not correlated with mothers’ pain severity, depression level, sleep quality, fatigue and QoL in this study. No significant correlation may be accounted for by the distribution of the GMFCS, in that most of the children had been diagnosed as having fourth and fifth levels. It is known that pain, increased care burden and depression level, deteriorated quality of sleep and fatigue are highly frequent symptoms of mothers of children with CP, and many have shown that these parameters are interrelated, triggering and negatively affecting each other (Mörelius and Hemmingsson, 2014; Wijesinghe et al., 2015). In the present study, it was observed that there was a positive correlation between mothers’ pain severity, care burden, depression level, quality of sleep and fatigue, but no significant correlation was found between the QoL and these parameters. Evaluation and correct treatment of these parameters in mothers of children with CP will help to remove the vicious cycle of triggering each other and ensure more positive results in treatment and follow-up.
The present study has several limitations. First, because the study was conducted in a single center, the results cannot be generalized to the whole population, so it has decreased the strength of the study. Second limitation is that we obtained pain severity, care burden, depression level, quality of sleep, fatigue and QoL scores only from mothers. Because most children with CP are cared for by their mothers in developing countries such as Turkey. The evaluation of the fathers would be valuable, as it may be related to both mother’s and child’s mental status and QoL. Finally, this study was cross-sectional, not longitudinal. Despite limitations, this study provides a partial view of the impact of the children with CP on their mothers.
While previous studies have assessed pain, care burden, depression level, sleep quality, fatigue and QoL in the group of mothers of children with CP separately, our study highlighted the importance of these parameters by examining all of them in the same patient group, comparing the results with a matched control, and analysing their interrelations. This study suggests that the mothers of children with CP have higher pain, care burden and depression level, worse sleep quality, increased fatigue and lower mental component of the QoL in comparison with matched healthy controls. Therefore, more attention should be given to mothers’ needs. Because the mother is the centre of support for the needs of the child with CP and plays an essential role in the rehabilitation, if the mother fails, the child suffers. Further research in longitudinal and multicentre studies that include both parents as participants is necessary.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.