
Abstract
The purpose of this study was to explore nurses’ experiences of encountering parents who are hesitant about or refrain from vaccinating their child. A qualitative approach was chosen and data collected through individual, semi-structured interviews with 12 nurses. The text was analyzed using thematic analysis. Three themes emerged from the interviews: giving room and time for acknowledging parents’ insecurity concerning vaccination, striving to approach the parents’ position with tact, and a struggle between feelings of failure and respect for the parents’ view. The findings indicate that it was crucial to give time, be tactful when meeting parents, as well as to appear credible and up-to-date. The nurses wanted to be open and respect the parents’ views on vaccination but found it difficult and frustrating to be unable to reach out with their message because their quest was to protect the child.
Introduction
Over the years, the vaccination programs of children have reduced the incidence of several diseases, making it one of the most successful and cost-effective measures that can be performed by medical services today (Andre et al., 2008; Healy and Pickering, 2011; World Health Organization, 2013, 2016). In Sweden, vaccinations are voluntary. Over 98% of the child population is vaccinated (The Public Health Agency of Sweden, 2017). Lee Burgad (2018) reported that nurses’ recommendations regarding the vaccination of their child have been important for parents’ decision.
Nurses in Sweden work independently, make their own decisions, have their own surgery in the child health-care center, and provide home visits to families. Vaccinating children up to the age of six years is a major part of the work of child health-care center nurses, based on political principles, action plans, and guidelines (The National Board of Health and Welfare, 2017). As laid down in the National Board of Health and Welfare (2017) directive on drug handling, nurses have the authority to prescribe vaccines in accordance with specified vaccination programs, including supplementary vaccinations.
The parent of a child can be either one or both of the biological parents, or a person appointed by a court of law. In this study, the term parent is used to refer to all of these.
Background
Dissemination of information in different media has a major impact on how families obtain information and their approach to topics of interest. This became clear when Wakefield et al. (1998) published a now withdrawn article containing a hypothesis that the measles, mumps, and rubella vaccine (MMR) could increase the risk of autism. The topic received considerable attention in the media worldwide, resulting in a lower uptake of the MMR vaccination among children in many countries. A few years after the article was published a measles outbreak occurred in England (Bester, 2017; Holton et al., 2012), which caused the first death of an infant due to measles in over 10 years.
How the media spread information plays an essential role. Some facts could be incorrect and experts are portrayed in a way that creates misinformation (Holton et al., 2012). This can cause anxiety in parents and create a so-called media-scare. Furthermore, Lyren and Leonard (2006) state that when parents search for information about vaccinations on the Internet, they find a plethora of anti-vaccination sites with negative facts. Some websites use scientific language and terms that are aimed at or written for physicians or scientists, which can be hard for parents to process and fully understand (Healy and Pickering, 2011). Therefore, the information should be provided in everyday language that is easy to assimilate. Furthermore, a number of websites are based on personal testimonies, which are hard to be critical about (Healy and Pickering, 2011; Lyren and Leonard, 2006; Smith, 2010). Hoyle et al. (2017) called for closer cooperation between nursing and media organizations in order to achieve a balance and present both positive and negative issues within health care, thereby helping families to make informed decisions.
The vaccines used today are safe, well-tested, and effective against infectious diseases that can have serious consequences in children and young people (Healy and Pickering, 2011). Despite their knowledge about the positive outcomes of vaccination, some parents are still hesitant (Healy and Pickering, 2011; Lee Burgad, 2018; Smith, 2010). One reason may be that they have never been in contact with the diseases nor seen how devastating their consequences can be (Diekema, 2005; Harmsen et al., 2013; Healy and Pickering, 2011; Smith, 2010). Vaccinations are a victim of their own success in that parents may perceive the threat of their child becoming infected as so small that vaccination is considered unnecessary (Lyren and Leonard, 2006; Smith, 2010).
The so-called herd immunity protects unvaccinated children due to the fact that the surrounding children are vaccinated, thus reducing the risk of the unvaccinated child becoming infected (Andre et al., 2008; Sobo, 2016). Some parents may rely on herd immunity to prevent their able-to-be vaccinated child from becoming ill (Lyren and Leonard, 2006). On the other hand, Sobo (2016) found that parents who made the decision to vaccinate their child felt that as a good parent you cannot rely on others. However, despite being informed and understanding the vaccine recommendation, some parents still made the decision not to vaccinate (Sobo, 2016). Sjögren et al. (2017) described parents who refrained from vaccination in order to protect their child from suffering and the risk of side effects. In the study by Berry et al. (2017), it was reported that nurses requested strategies in the form of discussion guides that would support them to systematically provide information to parents who declined vaccination, thereby enabling an informed decision on the part of the parents. Lee Burgad (2018) was aware of this issue and developed an education module for the nurses. The result showed that they felt more secure in their delivery of information to parents who were hesitant about or refused to vaccinate their child. Schollin Ask et al. (2017) stress the importance of creating a trustworthy relationship with parents before giving them information about vaccination.
Although child vaccination coverage is high in Sweden, there are still parents who hesitate about or refrain from vaccinating their child. How should child health nurses act in this situation when working alone? Little research on this matter has been conducted in Sweden or Scandinavia, which implies a gaping hole in the research field on child vaccinations in terms of the experiences of child health nurses.
Aim of the study
The aim of the study was to explore the nurses’ experiences of encountering parents who are hesitant about or refrain from vaccinating their child.
Methods
A qualitative approach was chosen where data were collected through individual semi-structured interviews. The reason for using individual interviews was to ensure that each nurse’s experience would be emphasized. Data were analyzed by means of thematic analysis in accordance with Braun and Clarke (2006), thus patterns (themes) were identified, analyzed, and reported. Thematic analysis was deemed relevant due to its ability to highlight the experiences of nurses who encounter parents in the context of vaccinating their child.
Procedures and participants
An invitation letter containing information about the aim of the study was emailed to the managers of 24 child health-care centers of different sizes, requesting their consent to interview nurses employed there. When consent had been obtained an email was sent to the nurses containing more detailed information about the study. The email stated that participation was voluntary, that it was possible to withdraw at any time, and that data would be treated confidentially. Twelve nurses from seven different child health-care centers agreed to take part in the study.
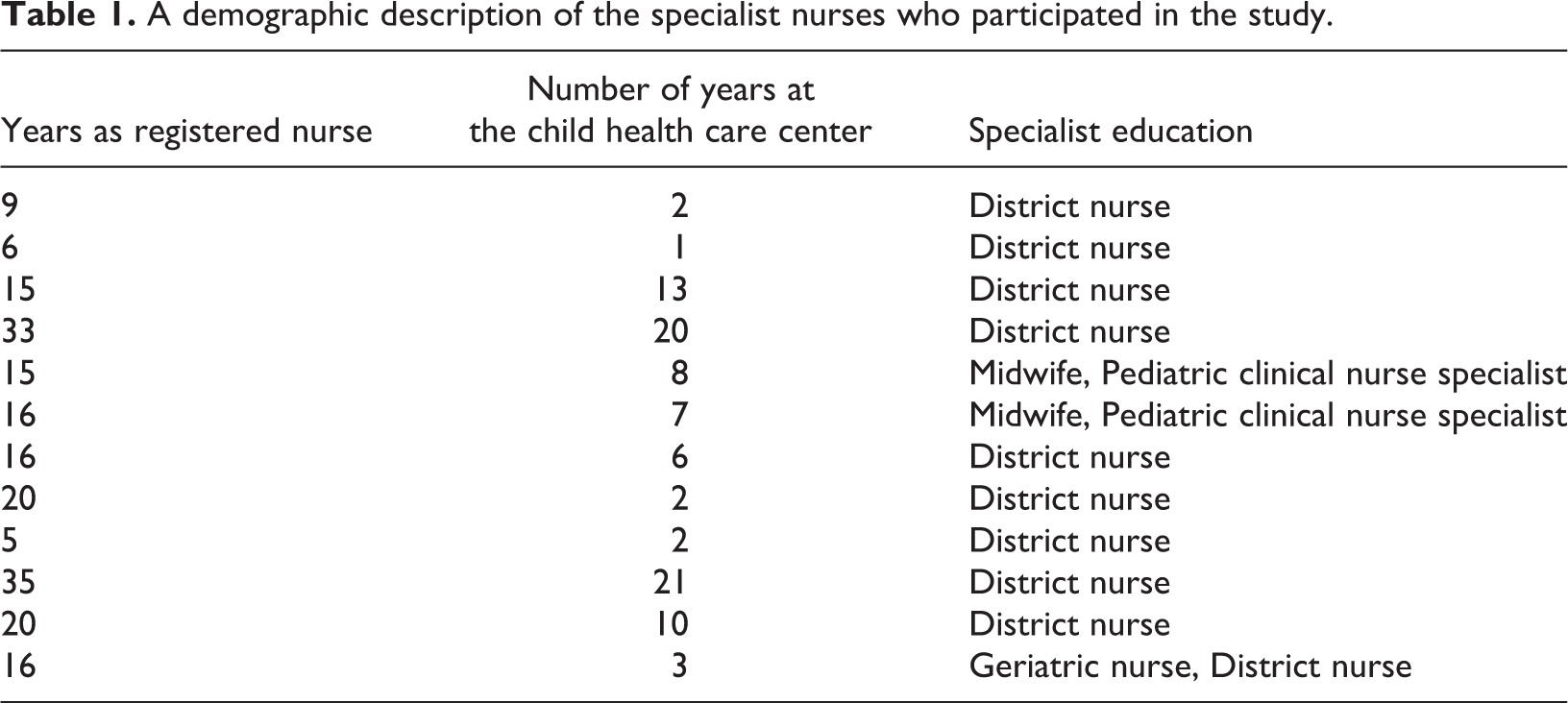
The study was performed in the western part of Sweden. The inclusion criteria were that the nurses had to have experience of working within the child health-care center, be Swedish-speaking, be free to participate in interviews during working hours or afterwards, and have experience of encountering parents who hesitated about or refrained from vaccinating their child. The nurses were all women and their work in child health-care centers varied between 1 and 21 years (mean: 8 years). They all had some kind of specialist nurse education (Table 1).
A demographic description of the specialist nurses who participated in the study.
Ethical considerations
The ethical application was approved by the local ethics board at the university. The nurses participating in the study were given both written and oral information at different times to ensure that no misunderstandings occurred before the interviews started.
Data collection
The nurses were given the opportunity to decide the time and place for the interview, all of which took place in a room at their workplace in an undisturbed atmosphere between January and March 2017. They were recorded and later transferred to a computer. The interviews were based on a semi-structured interview guide and the average duration of the interviews was around 30 minutes. The initial question was on the nurses’ description of their experiences of the encounters with parents who were hesitant about or refrained from vaccinating their child, followed by main reasons for their doubts. Additionally, the nurses were asked to describe situations where the parents were hesitant but also situations where the parents had already decided to refrain from vaccination. These issues were clarified by follow-up questions such as: Can you give examples? How do you mean?
Data analysis
Braun and Clarke (2006) have described a six-phase thematic analysis process, which influenced the present study. First, the recorded interviews were transcribed verbatim. The first phase of the analysis included several readings of each data set in order to gain an idea of the content. The transcribed text was analyzed by the authors, who collaborated throughout the process and attempted to achieve consensus. Initially, the analysis process involved searching for meanings and patterns that were deemed to be important for the issue under study and simultaneously striving to become familiar with all aspects of the data. In the second phase, initial codes were identified and ideas formed about content of interest. This part of the coding process involved coding as many meanings and patterns as possible in order not to miss any important information. In the third phase, all data were coded and sorted into potential subthemes and overarching themes (see the example in Table 2). In the fourth phase, candidate subthemes and themes were identified, after which they were examined and refined in order to obtain an idea of how they fit and describe the content of the data. In the fifth phase, the themes were labeled with titles that were both clear and strong. The sixth and final phase involved completing the analysis and presenting the findings in a way that will hopefully convince the reader of the credibility of the study.
An example of the analysis process showing codes, a subtheme, and the theme.

Findings
The findings comprise three themes: giving room and time for acknowledging parents’ insecurity concerning vaccination, striving to approach the parents’ position with tact, and a struggle between feelings of failure and respect for the parents’ view and eight subthemes.
Giving room and time for acknowledging parents’ insecurity concerning vaccination
Working to create trust that lasts
It was important for the nurses to devote time to the meeting with parents who felt insecure and give them space in order to find out what they felt unsafe about. The standard 30 minute meeting was often too short and sometimes it was necessary to spend an hour with the parents. When the nurses outlined the benefits of the vaccine while not forcing a decision, it gave the parents time to go home and consider the benefits of vaccinating their child and hopefully decide that they should vaccinate. They also invited the parents to call back if they had any questions after the meeting. …have discussed for and against in an open conversation, so that we really had an open dialogue where they expressed what they think and feel. Then they go home and think about it and come back and want to wait another month. So we are discussing it all the time. It takes time to correct misunderstandings when the parents do not know that a study from Denmark showing that children could be at risk of autism after vaccination was fake.
Being open and allowing the parents to explain their point of view
The nurses tried to discover what the parents thought by asking open-ended questions about the reason for not vaccinating their child. The open-ended questions enabled them to discreetly gain an understanding of the parents’ standpoint. The nurses awaited the parents’ decision because they wanted to ensure that the parents had properly understood what they had been told. They were anxious never to be judgmental and avoided criticizing the parents when they outlined their reasons for abstaining from having their child vaccinated. The nurses realized that they had to accept the parents’ decision, even if they did not agree with it. They already had a long-term relationship with the parents and considered it important to preserve it and be the person the parents could trust when other issues arose. …you must respect the fact that some parents do not want to vaccinate their child. Many of them may be a little ashamed about saying no, but then I usually try to explain that the entire child health center is a voluntary advisory and support service. We do not make decisions for you. That is up to you.
Striving to approach the parents’ position with tact
Developing the ability to reach out to parents
The nurses described that thanks to their experience they gradually developed an ability to reach out to parents with their message. They considered the parents’ decision about vaccination crucial. Many years ago I learned that warnings do not help, and it is always the parents who decide in the end. I am not the one who makes the decision.
Meeting obstructive parents or those who are unconvinced by the information about the benefits of vaccination
At each meeting with parents, the nurses raised the issue of vaccinating their child. There were situations where parents were really obstructive, making it pointless for the nurses to continue discussing the issue. The parents did not want any input and were unwilling to reexamine their decision. One nurse described such a situation at a home visit: When I arrived for a home visit the father just opened the door and said, ‘Just so you know, we do not vaccinate any children here!’ No, I thought, why should I mention the vaccination? I did not even have time to say hello. Then I wonder what his information consists of if he does not even want to have a discussion but had just decided. Only the mother was present at this visit. I did not even have the opportunity to talk to the father.
Choosing your moment to raise the question
In some situations, the nurses felt that the parents were receptive to information and tried to start a dialogue, as well as making an even greater attempt to build a good relationship with them. With their knowledge of vaccination and the spread of infection, they gently tried to get parents to understand the benefit of vaccinating their child. I can build a relationship. I cannot talk about it every time, but I can choose my moment when the [issue] comes up. As I’m new here, I had the opportunity to raise the question when a mother came whose child had not had the MMR. As a new employee I could say: ‘I see you have not vaccinated your child’ and ask her a little more when I had the chance.
Enabling the parents to reflect on their decision
The nurses described that some of the parents were well informed about all vaccinations. They gained the impression that they read a great deal and wanted to know as much as possible. At the same time, some parents realized that they lacked enough knowledge to sort out all the information they had obtained. In some cases, the nurses enlisted the help of the physician at child health center to give the parents more information. However, the nurses had the responsibility to share their knowledge and start a process that would enable the parents to reflect on whatever decision they made. If the decision was already made when coming to the surgery, it was almost impossible to convince such parents to change their decision not to vaccinate their child.
One nurse described the meeting with a mother who was extremely well informed. This meant that the nurse had difficulty responding because the mother tried to change the nurse’s mind to get her views confirmed. In that situation, the nurse could only sit and listen to the mother’s opinions without confirming them. I try to have as much knowledge as possible about the vaccinations we give, but you never know what questions will arise, because sometimes they have read about things that I might have missed, and then I’ll have to read it. …there has been information added to the Hep B part since I started work here. This meant that we gave more information about it, and I did too. I think it’s good to update your own knowledge from time to time. You get stuck easily. I had to update myself and reflect.
A struggle between feelings of failure and respect for the parents’ view
The duty and obligation to inform
The nurses considered it their duty and responsibility to provide clear information, both verbally and in writing. There was material available from which parents could deepen their knowledge as a basis for their meeting with the nurse. Sometimes, the parents asked them for their personal opinion. They answered clearly that their views on the matter were irrelevant. The nurses stated that the vaccine would not be offered if the child health-care center did not believe it was good for the child. Although the parents subsequently refused to vaccinate their child, it was nevertheless the nurses’ responsibility to contribute all information on which they can base their decision. …I just want you to know that I would like to give you information so that you know what you are saying no to, and because it is my duty to give you information.
Balancing between taking over and giving up
The nurses found it difficult and frustrating when the parents failed to grasp the importance of vaccinating their child. They devoted a lot of effort into trying to control their feelings and themselves. When they failed, they wanted to shake the parents and ask the question: ‘why do you not vaccinate?’…this is not something to play with and I actually become annoyed by their insensitivity. I think they are playing with the children’s lives, but that is my personal opinion. It is something I have to work on all the time. I’m sitting on knowledge that the parents do not have, which I can use well but also in situations when I am frustrated. Then it becomes a power game. It is the poor little innocent child who, in that case, suffers from these diseases. It is not a decision that affects the parents and their body but the child. It is really frustrating and challenging.
Discussion
The aim of the study was to explore nurses’ experiences of encountering parents who are hesitant about or refrain from vaccinating their child. In this study, the nurses’ view was that the parents who refrained from vaccinating their child had failed to grasp the whole picture of why they should vaccinate. They understood that the parents’ worries were caused by a fear of exposing the child to something unnatural that could result in a permanent disability, also described by Sjögren et al. (2017). These concerns resulted in the nurses allocating more time to inform the parents and highlighting the child’s right to receive protection against communicable diseases. Creating time meant not following the clock but allowing parents the time the nurses considered they needed (cf. Nurminen, 2009). Cases where the extra time did not produce results caused frustration among the nurses. However, they mentioned that the struggle was sustainable as long as hope was involved (Eriksson, 2006). The nurses regarded it as their duty to fight for the children’s future health, which gave them the courage to continue the struggle (Eriksson, 2006).
Delkhosh et al. (2014) showed that parents’ negative perception about the adverse effects of the vaccine was that the risk of becoming ill was greater if they vaccinated their child than if she/he contracted a disease. One of the main causes of concern was alleged side effects, of which autism was most apparent (Austvoll-Dahlgren and Helseth, 2012; Bester, 2017; McCauley et al., 2012). Despite the fact that the nurses confirmed that this information was incorrect, parental worries were a significant factor in the hesitancy about vaccination and seemed to be widespread (Casiday et al., 2005; Diekema, 2005; Harmsen et al., 2013; Healy and Pickering, 2011; Luthy et al., 2010). The study by McCauley et al. (2012) confirms the side effects of Pandemrix®, the vaccine developed to counter swine flu, which created a fear that their child would suffer from narcolepsy. These two specific concerns have clearly contributed to more work for nurses in promoting child vaccinations.
The present study indicated that the nurses tried to step in and protect the child but did not always succeed. To protect is to care for and be responsible for the other, based on ethos (Eriksson, 2006; Karlsson, 2013). Karlsson (2013) described ‘to care for’ as being there and as an obligation to protect from illness and injury. To protect is one of the core values of caring, especially in the case of a child who cannot speak for her/himself. Although the participants spoke about the child’s best interests, they were not always able to change the parents’ conviction not to vaccinate their child. Despite the fact that the nurses made every effort to ensure that the parents understood the outcome of their decision not to vaccinate, they were uncertain whether the parents really grasped the information provided and what consequences the refusal to vaccinate might have for their child. Those parents who refused to accept more information were experienced as the most difficult and created frustration, which Berry et al. (2017) viewed as an insult against the nurses’ professional identity. The nurses’ sense of frustration increased even more if one parent wanted to vaccinate and the other did not. Some parents came to the meeting ready to stand up for their view, and while they pretended to listen to the information they actually paid no attention whatsoever. Kurup et al. (2017) discussed the importance of understanding cultural and systemic factors that affect parental perceptions of vaccination.
In a previous study, some parents expressed frustration vis-à-vis health-care professionals who hurried through meetings without giving any time to answer their questions (Luthy et al., 2010), something that the nurses in the present study strived to give. The participants in our study expressed the importance of allocating enough time for the meeting, so that interested parents could really reflect on and discuss the information they received, thus enabling them to make informed decisions with the best interest of the child in mind (Leask et al., 2012).
Several studies show that the nurses in child health-care centers have the best prerequisites for providing vaccination information due to their long relationship with the parents (Bester, 2017; Delkhosh et al., 2014; Luthy et al., 2010; McCauley et al., 2012). In this study, some nurses stated that it was important to let the parents know their viewpoint, while others did not. Those who shared their opinions with the parents felt that it strengthened trust and that a larger number of hesitant parents chose to vaccinate their children as a result.
Limitations
The aim of the study was to explore the nurses’ experiences of encountering parents who are hesitant about or refrain from vaccinating their child. The method employed was a qualitative thematic analysis in accordance with Braun and Clarke (2006), which was deemed appropriate because of its suitability for identifying, analyzing, and searching for patterns or themes that reflect the nurses’ experiences of encountering parents at the child health-care center. In order to ensure that the selection of participants was as varied as possible, information letters about the study were sent to both larger and smaller health-care centers in western Sweden. The wide range of child health-care centers from different communities, the age differences, and years of experience among the participating nurses are all factors that can contribute to transferability to similar care settings. All participants in the study were women. It is possible that new perspectives would have emerged if male nurses had been included, which also might have had an impact on the meeting with parents who hesitate about or refuse vaccination. Limited time was the most common reason given by nurses who declined to participate in the study, followed by not having encountered parents who hesitated about or refrained from vaccinating their child. They were informed about how the data would be dealt with and coded, so that no material could be linked to the participants. It was important to explain this and make the nurses feel safe, therefore enabling them to speak freely about their experiences.
The 24 emails sent to child health-care center managers resulted in 12 nurses agreeing to participate. Having contacted so many child health-care centers, it can be considered disappointing that only 12 nurses agreed to participate. However, 12 is an acceptable number and they provided large amount of rich, in-depth data, which Braun and Clarke (2006) state is important when conducting a thematic analysis. The quality of the data made it possible to highlight and illuminate the patterns and themes in line with Braun and Clarke (2006).
Both authors are registered nurses, one in surgical care and the other in intensive care. They have no previous experience of working in a child health-care center but are used to encountering parents and children in other caring situations.
Conclusion
The findings indicate the complexity of informing parents who are hesitant about or refrain from vaccinating their child. It is essential to allow time and be tactful when meeting the parents, in addition to appearing credible and up-to-date. Consequently, nurses need to allocate extra time for meeting parents who are hesitant about or refrain from vaccinating their child. Additionally, repeated meetings and dialogue with the parents are crucial, as is repeating the information about the benefits of vaccination. Furthermore, the nurses worked to create a lasting relationship based on trust. Although they wanted to be open to and respect the parents’ views on vaccination, they found being unable to reach out to the parents with their message difficult and frustrating, because their quest was always to protect the child. They did their best not to view their efforts as a failure.
This study is only one contribution to the literature on why parents decide not to vaccinate their child. More studies are needed in order to understand how parents think and reason when making the decision not to vaccinate their child. In addition, more knowledge is required to prepare nurses for meeting reluctant or hesitant parents, so that they do not become upset, frustrated, or believe that they have failed in their duty.
Footnotes
Acknowledgements
The authors are grateful to the nurses who participated and shared their valuable experience, to University West and to the Ethical Review Board at University West, as well as to Felicia Karlberg and Anna Holm who conducted and transcribed the recorded interviews. The authors would also like to express our gratitude to Monique Federsel who scrutinized the English language in the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.