
Abstract
Congenital heart disease (CHD) is one of the common types of birth defects. Children and young people (CYP) with CHD might exhibit behavioural and emotional changes related to undergoing different medical treatments and hospitalization. Therefore, a literature review was conducted from January 2000 to June 2017 that aimed to understand and evaluate current international literature focusing on CYP’s behavioural and emotional status as patients with CHD. A comprehensive search of Medline, PsycINFO and CINAHL databases was undertaken. Eight quantitative studies were reviewed following strict eligibility criteria. The Mixed Methods Appraisal Tool (MMAT) was used to assess the quality of the reviewed studies. Parents provided proxy reports on their children’s behaviour and emotions in all studies. Half of the reviewed studies presented the self-perceptions of children who were over seven years old. CYP with CHD exhibited internalizing and externalizing behavioural problems, withdrawal, depression, social, and attention problems. CYP with more severe CHD reported greater behavioural and emotional problems than CYP with less severe CHD. Moreover, younger children developed more problems than older children. Future more depth research using qualitative designs is required to explore the personal views of children younger than seven years old on the impact of CHD on their behaviour and emotions.
Introduction
Congenital heart disease (CHD) is a term for several birth defects, which disrupt the normal function of the heart (National Health Service, 2015). These defects can result from abnormal development of the heart’s or major blood vessels’ structures (American Heart Association, 2017). CHD can be present at birth or detected before birth through routine maternal screenings and can cause breathing and/or feeding difficulties in infants (American Heart Association, 2018; National Health Service, 2015). Globally, cardiovascular diseases including CHD are the most common causes of death, with a mortality rate of 17.9 million among adults and children with heart disease in 2016 (World Health Organization, 2017). However, studies of children and young people (CYP) with CHD revealed a recent increase in life expectancy because of the advances in cardiac surgeries and medical management. The survival rate among infants with CHD has been improving in recent years (Oster et al., 2013) and the global mortality rate of CHD has significantly reduced compared to other causes of death between 1990 and 2010 (Lozano et al., 2012). These factors have resulted in a shift of focus by researchers towards improving the long-term outcomes and quality of life of children with CHD (Latal et al., 2009; Nousi and Christou, 2010; Wilmot et al., 2016) and highlighting the need for enhancing the psychoemotional status of children with CHD (Nousi and Christou, 2010). Others have further explored the psychosocial status by testing the readiness of children with CHD to engage in activities, such as summer overnight recreation and weekend camping (Bultas et al., 2015; Desai et al., 2014).
CYP normally are experiencing challenges throughout their development. They can be affected by several circumstances that may contribute to serious behavioural problems, which interfere with their normal development, socialization, or future life. Such behaviours include aggressive or destructive behaviour, or temper tantrums (Royal College of Psychiatrists, 2017). In addition, children’s emotional responsiveness can be affected by influences, such as confronting family issues or experiencing physical disabilities. CYP from a very early age do not only recognize their own emotions; they express them, adapt to and cope with them, and progressively become able to understand and react towards other’s emotions (Smith et al., 2015a). Moreover, biological factors and pathological incidents of children with long-term conditions can have an impact on these children’s emotions (Schaffer, 2004).
Medical and surgical interventions throughout the treatment plan of CHD might also impact on the behavioural and emotional status of CYP. Some studies have revealed evidence of behavioural and emotional issues among CYP diagnosed with CHD, such as depression and social withdrawal (Guan et al., 2014), and high incidence of emotional reactivity (Larsen et al., 2010). A systematic review reported that a significant number of children with CHD, who have had cardiopulmonary bypass surgery, actually later presented with psychological maladjustment (Latal et al., 2009). However, Latal et al.’s (2009) study focused on parents’ reports of their child’s psychological adjustments without investigating the CYP’s own perspectives about the impact of CHD on their behaviour and emotions. Combining perspectives of children and parents would provide a holistic understanding of the impact of CHD on CYP’s behaviour and emotions, which can lead to future development of preventive or supportive interventions for the CYP with CHD and their families. Therefore, this review was conducted with the aim of exploring the existing evidence on the self-perception of children with CHD regarding their own behaviour and emotions as well as exploring parents’ proxy reports on their children’s behaviour and emotions.
Aim and objectives
This review aimed to understand and evaluate current international literature about the behavioural and emotional status of CYP with CHD. Our objectives were to: explore the range of behavioural and emotional issues of CYP with CHD; explore CYPs’ own perceptions about their behaviour and emotions, and their parents’ proxy-reports on their children’s behaviour and emotions; and identify what research is required to enhance healthcare providers’ knowledge concerning the behaviour and emotions of CYP with CHD.
Methods
This literature review was guided by the University of York Centre for Reviews and Dissemination (2009) (CRD) guidance on undertaking systematic reviews. Following these stages: (1) developing the review question, a search strategy and defining inclusion and exclusion criteria, (2) elaborating the research evidence including conducting a thorough search, (3) selecting studies, (4) extracting data, (5) assessing the quality of the reviewed studies, (6) synthesizing the data and (7) disseminating the review. Since this review aimed to explore all studies meeting the criteria, studies assessed as low quality were not excluded.
The research question guiding this review was ‘What is the impact of having CHD on the behaviour and emotions of CYP?’ The inclusion and exclusion criteria are described in Table 1 according to the type of study population, outcomes, study methods or design, settings or countries of research conduct, publication year, and publication language.
Eligibility criteria.

Search strategy
A systematic search process was undertaken, starting by breaking down the review question into keywords and related terms using the population, exposure, outcome format. Final keywords were selected with support from a librarian at the University of Leeds (Figure 1).

Planning search keywords and terms.
A comprehensive search of Medline, PsycINFO and CINAHL databases was undertaken to identify sources related to medicine, psychology, behavioural sciences, nursing and allied health professions. In the advanced search engine, the Boolean operators “and” or “or” were used to broaden the results. Adjacency of phrases was maintained by adding (adj) between the words, for example, ‘Congenital adj heart adj disease’. Moreover, using truncation (*, $) at the end of each keyword allowed retrieval of all possible results related to that word stem. These strategies enabled widening of the search results.
Study selection
The total number of articles retrieved from all three databases was 2425. Covidence software was used to aid screening papers and importing them into Endnote reference manager (Babineau, 2014) for arranging and indexing references of all papers (Reuters, 2011). Twenty duplicates were removed, and the remaining 2405 articles were screened by reading titles and abstracts, by one author (ND), resulting in 96 studies. Then, the author (LM) reviewed (rescreened) the screened titles and abstracts of 96 studies. If the titles and abstracts were not clear, the full text was read by one author (ND). The full text of 96 studies was assessed against the eligibility criteria (Table 1) by the author (ND), resulting in 8 included studies (Figure 2). Agreement between all authors was reached regarding the eligibility of the eight studies. The data of the eight studies were extracted by one author (ND) into Table 2 and, two authors reviewed the data extraction (LM and VS). Then, quality appraisal of the eight studies was done by ND, and two authors (LM and VS) reviewed the quality appraisal of 2two studies.
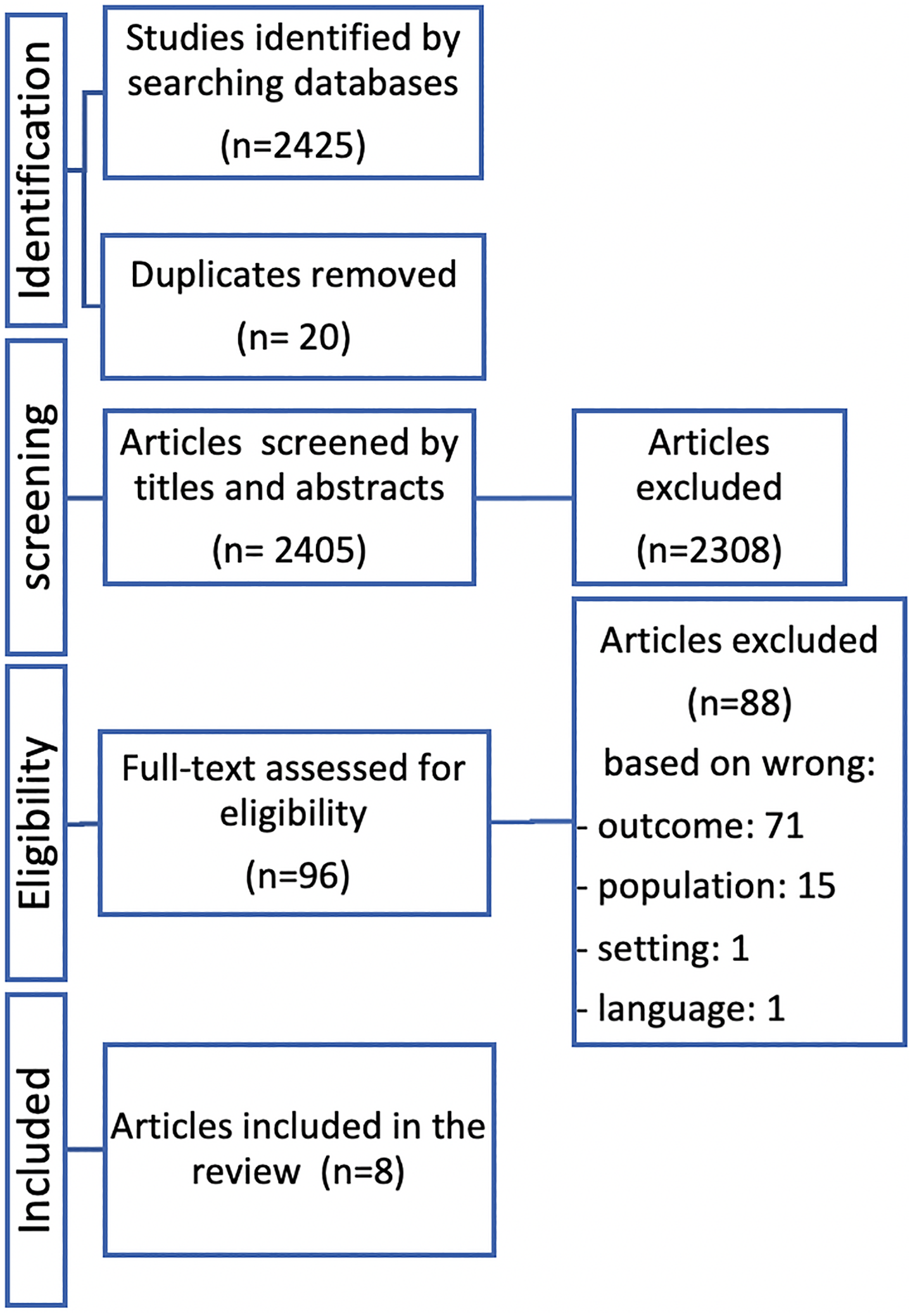
PRISMA chart for studies selections. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Summarized description of the reviewed studies.
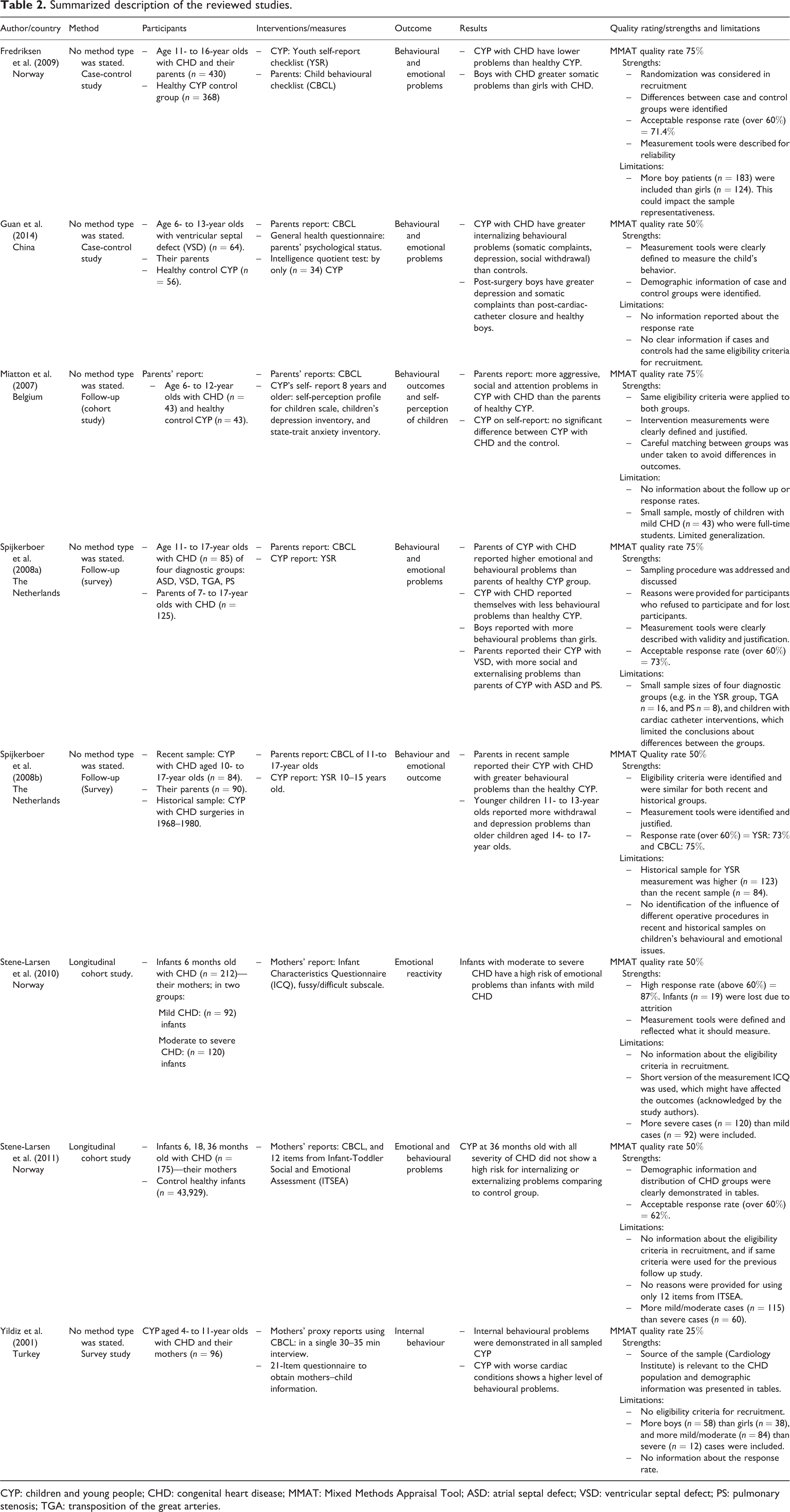
CYP: children and young people; CHD: congenital heart disease; MMAT: Mixed Methods Appraisal Tool; ASD: atrial septal defect; VSD: ventricular septal defect; PS: pulmonary stenosis; TGA: transposition of the great arteries.
Quality appraisal
All studies were critically appraised using the MMAT, a standard appraisal tool with confirmed reliability and validity of its pilot version (Pace et al., 2012; Pluye et al., 2011). The reliability and validity of MMAT were also demonstrated in this review. Scoring of a paper’s quality could be calculated as 25% if one criterion was met, and 100% if all criteria were met (Pluye et al., 2011). Broadly, out of the eight reviewed studies, seven were rated as medium to high quality (50% or 75%), and only one was rated as low quality (25%). The high-quality study fulfilled almost all the quality criteria with clear descriptions and explanations.
Data extraction
Following the CRD guidance on data extraction processes (Centre for Reviews and Dissemination, 2009), information was extracted from the reviewed studies into a table based on general information (author name, year of publication, country of origin), study method, participants’ characteristics, interventions, outcomes, and results (Table 2). All eight reviewed studies were quantitative in design: case-control studies, n = 2 (Fredriksen et al., 2009 and Guan et al., 2014); cohort studies, n = 3 (Miatton et al., 2007; Stene-Larsen et al., 2010; Stene-Larsen et al., 2011); and survey studies, n = 3 (Spijkerboer et al., 2008a; Spijkerboer et al., 2008b; Yildiz et al., 2001). All studies were published in the English language and were conducted in the following countries: Belgium, n = 1 (Miatton et al., 2007); China, n = 1 (Guan et al., 2014); Norway, n = 3 (Fredriksen et al., 2009; Stene-Larsen et al., 2010; Stene-Larsen et al., 2011); the Netherlands, n = 2 (Spijkerboer et al., 2008a and Spijkerboer et al., 2008b); and Turkey, n = 1 (Yildiz et al., 2001). Only two studies included participants aged 6–36 months (Stene-Larsen et al., 2010; Stene-Larsen et al., 2011), and the others included 4- to 18-year-olds. Moreover, the studies varied in the manner of assessing behaviour and emotions in CYP with CHD. Some asked only for the parents’ or mother’s perceptions of their child’s behaviours and emotions, using the child behavioural checklist (CBCL) (Guan et al., 2014; Yildiz et al., 2001; Stene-Larsen et al., 2011) or Infant’s Characteristics Questionnaire (Stene-Larsen et al., 2010), whereas others combined parental perceptions using the CBCL with CYP’s self-perceptions using the Youth Self-Report (Fredriksen et al., 2009; Miatton et al., 2007; Spijkerboer et al., 2008a; Spijkerboer et al., 2008b).
Results
The findings from the reviewed studies are presented below as a narrative summary under three categories.
Identified behavioural and emotional issues in CYP with CHD and the agreement between child’s self-perception and parental proxy reports
All reviewed studies identified behavioural and emotional problems in CYP with CHD. Perceptions were obtained from only parents in half of the reviewed studies (n = 4; proxy reports), whereas the other studies combined parental proxy reports and CYP self-perceptions (n = 4). In studies that revealed only parents’ proxy reports about their CYP’s emotional and behavioural problems, parents reported internalizing behavioural problems in school-aged children (6–13 years) with ventricular septal defects (VSDs) in China (Guan et al., 2014) and children aged (4–11 years) with different severities of CHD in Turkey (Yildiz et al., 2001). Two other studies, where only mothers’ reports were obtained, revealed that infants could demonstrate different emotional problems depending on age and CHD severity in Norway (Stene-Larsen et al., 2010; Stene-Larsen et al., 2011). It is worth noting that despite the differences in culture, child age, and CHD severity in children, all parents were similar in reporting the existence of behavioural and emotional problems in their CYP.
In studies with a combination of parents’ and CYP’s perceptions, disagreements were noticed between the perceptions of both groups. Parents reported their CYP (using the CBCL) (Achenbach, 1991) with more behavioural and emotional problems (p = .005) than their CYP perceived themselves using the self-perception profile for children (Harter, 1985) (p = .794) and the State Trait Anxiety Inventory for children (Spielberger et al., 1973) (p = .588) (Miatton et al., 2007). While in other studies, CYP perceived themselves with more behavioural (p < .0001), internalizing and externalizing problems (p < .001) (Fredriksen et al., 2009), with more withdrawal/depression, social, attention and with higher total scores of behavioural and emotional problems (all p < .05) than their parents reported them (Spijkerboer et al., 2008a).
Proxy reports of parents of CYP with CHD differ from the proxy reports of parents of healthy CYP. Parents of CYP with CHD rated their CYP with more problems than parents of healthy CYP in somatic complaints (mean 2.1 and 1.6, respectively), social problems (mean 3.4 and 2.3, respectively), attention problems (mean 5.0 and 4.0 respectively), internalizing problems (mean 8.3 and 7.0, respectively), and in the total scores of behavioural and emotional problems (mean 30.0 and 25.5, respectively) (Spijkerboer et al., 2008a), a higher level of behavioural (mean 55.5 and 48.5 respectively), attention (mean 61.5 and 54.6 respectively), and aggressive problems (mean 54.0 and 52.1, respectively) (Miatton et al., 2007) and greater internalizing behavioural problems (mean 13.12 and 6.02 in boys, 11.2 and 4.80 in girls, respectively) (Guan et al., 2014).
Contradictory reports arose when CYP were asked to report their own views. The self-perceptions of CYP with CHD in comparison to the self-perceptions of healthy CYP were investigated in only three studies in this review. Unlike in the proxy reports of parents of healthy CYP and parents of CYP with CHD, CYP with CHD reported themselves with either lower scores of behavioural and emotional issues (Fredriksen et al., 2009; Spijkerboer et al., 2008a) or with no greater scores than healthy CYP (Miatton et al., 2007). In another study in the Netherlands, a comparison was undertaken of CYP with CHD between the recent sample (who had their operations or catheterizations between 1990 and 1996) and historical sample (who had their operations between 1968 and 1980). Although less invasive procedures were reported in the recent sample, parents in the recent sample reported that their CYP had more behavioural problems than parents of CYP in the historical sample (Spijkerboer et al., 2008b). This finding can be determined by comparing the population distribution in the historical (n = 98) and recent samples (n = 90), and the total behavioural problems scores of both samples (mean 30.6 and 29.6, respectively), as acknowledged by the authors (Spijkerboer et al., 2008b). However, parents’ reports and CYP’s self-reports did not differ in this study, and similar levels of behavioural and emotional problems were demonstrated in recent and historical samples (Spijkerboer et al., 2008b).
Effect of age and gender on the behavioural and emotional issues in CYP with CHD
No relationship was found between age and behavioural problems among young children (4–11 years) in Yildiz et al.’s (2001) study. While in Spijkerboer et al. (2008a), younger children (11–12 years) perceived themselves with more anxiousness/depression, rule-breaking, aggressive behaviour, externalizing problems, somatic complaints, and higher total behavioural problems scores (means = 39.6 in boys and 42.0 in girls) than older children (13–17 years) with mean scores for total behavioural problems (27.5 in boys and 32.4 in girls). Other reviewed studies also revealed behavioural problems in young children 6–12 years (Miatton et al., 2007) and 6-13 years (Guan et al., 2014). Thus, younger children were found to have more behavioural and emotional problems. Relying on these findings, it was anticipated that younger children’s behaviour and emotions could be affected by the time of the child’s first invasive treatment for CHD. A prediction might be that the younger the child’s age at the time of their invasive treatments the more behavioural and emotional problems. However, in the reviewed studies, age at invasive treatment and its relation to behavioural and emotional problems were not demonstrated in Spijkerboer et al’s (2008a), or Miatton et al.’s (2007) studies, whereas Guan et al. (2014) have found that age at invasive treatment is a biological risk (p = .03) of behavioural problems for 6- to 13-year-olds with CHD.
However, in studies that included infants, conflicting results were demonstrated. In a longitudinal study investigating the risk of developing emotional problems in infants with CHD, mothers of the infants reported that at age 36 months, their infants showed no risk for developing internalizing or externalizing emotional problems (Stene-Larsen et al., 2011). The same infant group, precisely the subgroup of moderate to severe CHD, at an earlier assessment when they were six months old, showed 60% higher risk of developing emotional problems (Stene-Larsen et al., 2010; Stene-Larsen et al., 2011). It was also acknowledged in the same study that different tools were used with different age groups and that may have impacted upon the results (Stene-Larsen et al., 2011).
Gender did seem to have an impact on the behaviour and emotions of CYP with CHD. Boys were reported to have scored themselves with more somatic complaints than girls (Spijkerboer et al., 2008a) (the actual scores were not provided in the study) and with more total behavioural problems scores (mean boys 27.2 vs. 23.1 girls) (Fredriksen et al., 2009). Precisely, in Guan et al. (2014), boys who were post-cardiac surgery exhibited more significant depression (23.8%) and somatic complaints (23.8%) compared to boys of post-cardiac-catheter interventions (4.2% and 8.3,% respectively) and healthy control boys (0% and 3.2%, respectively), whereas girls who were post-cardiac surgery showed more thought problems (12.5%), depression (25.0%), somatic complaints (25.0%) and social withdrawal (37.3%) problems than healthy girl controls (3.8%) (Guan et al., 2014).
Effect of disease complexity and treatment severity on behavioural and emotional issues in CYP with CHD
Different CHD complexities can lead to different kinds of treatments or management, which could be through medications (non-invasive treatments) or cardiac-catheter or cardiac surgery (invasive treatments) (National Health Service, 2018). When investigating the relation of the presence of behavioural and emotional issues in CYP with CHD and the different invasive treatments they had gone through, three studies revealed different conclusions. In comparisons between the cardiac-catheter and cardiac-surgical treatments, boys, unlike girls, in the post-surgical treatment group demonstrated more depression (23.8% vs. 4.2%) and somatic complaints (23.8% vs. 8.3%) than boys in the post-catheter treatment group (Guan et al., 2014). Additionally, CYP who had undergone both invasive treatments exhibited more behavioural problems than healthy CYP (33.3% post-surgical and 20.8% post-catheter vs. 12.9% healthy children) (Guan et al., 2014).
When Spijkerboer et al. (2008a) compared four CHD diagnostic groups of different CHD severities, they found that CYP with VSD revealed more social (mean 4.4) and externalizing problems (mean 9.0) than CYP with atrial septal defect (ASD) (mean 2.2 and 5.2, respectively) and pulmonary stenosis (PS) (mean 2.4 and 5.0, respectively) with main effect p < .05, as reported by their parents. Medically, VSD comprises more severe symptoms than ASD and PS. However, CYP in the same study reported themselves with results that are conflicted with the parents’ proxy reports. According to CYP’s self-reports, no significant relationships were found between the severity of CHD and behavioural and emotional issues (Spijkerboer et al., 2008a). In a study of infants aged 36 months with different severities and different invasive treatments of CHD, all infants did not differ in showing any risks of developing emotional problems (Stene-Larsen et al., 2011). However, when they were six months old with moderate-severe CHD, they did demonstrate 60% higher risk of emotional problems (Stene-Larsen et al., 2010). Hence, these results suggest that CYP with high disease severities develop more problems than lower disease severities.
Despite the intention of Spijkerboer et al. (2008b) to include CYP with different severities of CHD who had undergone invasive treatments, the effect of the type of invasive treatments on CYP’s behaviour or emotions was reported as unknown (Spijkerboer et al., 2008b). Likewise, due to the small sample (n = 43) of CYP with mild severity of CHD (Miatton et al., 2007), no conclusion could be drawn about the effect of CHD severities on CYP’ behaviour and emotions, as acknowledged by Miatton et al. (2007).
In studies of CYP with different severities of CHD, but with no report of the type of treatments of CHD (invasive or non-invasive), no differences in behavioural and emotional problems were found across all severities of CHD in Norway (Fredriksen et al., 2009). In contrast, in Turkey, it was found that the more severe the cardiac condition, the higher the withdrawal behaviour (p = .002) and somatic complaints (p = .029) that were demonstrated in CYP with CHD (Yildiz et al., 2001).
Discussion
This review identified the common behavioural and emotional issues in CYP with CHD through the parents’ perceptions or proxy reports and CYP’s self-perceptions, and a disparity was noted between child–parents’ perceptions. CYP perceived that they experienced more issues than as assessed by their parents. This could have been due to differences in awareness of issues between CYP and their parents, or the parents’ refusal to face their CYP’s sickness (Fredriksen et al., 2009), whereas other parents may have overrated their child’s level of behavioural and emotional issues. Miatton et al. (2007) speculated that parents of CYP with CHD might be over concerned about their child’s condition or more alert to the related issues of their children’s illness (Spijkerboer et al., 2008a) and therefore tend to over-assume the presence of issues in their children (Miatton et al., 2007; Spijkerboer et al., 2008a). However, parents are considered understanding and supportive of their children and their actual knowledge about their child’s condition should be appreciated, essentially to improve the care provided for their child (Smith et al., 2015b).
CYP’s denial to admit the presence of problems and to try to live as a normal life as possible can also justify why the CYP perceived themselves with fewer issues. Patients sometimes reach some point where they refuse to be recognized as patients or deny the existence of the disease, which may lead them to deny the existence of behavioural and emotional problems (Fredriksen et al., 2009). Hence, this could result in them not seeking medical advice or care when needed, especially with older children when their parents become, sometimes, less involved in taking care of them. However, the combination of both perceptions of parents and CYP is crucial to fully understand the behaviour and emotions of CYP with CHD, as acknowledged by two studies included in this review (Fredriksen et al., 2009; Spijkerboer et al., 2008a).
It is also important to highlight that only quantitative studies and no qualitative studies were found in the international literature concerning assessing the behavioural and emotional status of CYP with CHD. Therefore, in-depth exploration of CYP’s self-perceptions and parents’ proxy reports on the behavioural and emotional status of CYP with CHD was limited. A deeper investigation can best be studied using a qualitative design, as it needs an exploratory approach that aims to look at CYP’s perceptions in depth (Pope and Mays, 2006).
As presented above, few studies have investigated the effect of age and gender on behavioural and emotional status in CYP with CHD. Understanding the differences, if present, between boys and girls in developing behavioural and emotional problems will facilitate the development of individualized interventions to reduce these problems. Hence, child age and different developmental stages for each child regardless of chronological age could also impact the presence of behavioural and emotional problems. Therefore, if young children develop more problems than older children, as demonstrated in Spijkerboer et al. (2008a), then different interventions should be delivered to the younger age group. However, further investigations should be conducted around the influence of the child’s age, developmental stage, and gender on the behavioural and emotional status of CYP with CHD, as only three of the reviewed studies explored the impact of gender on developing behavioural and emotional issues in CYP with CHD.
It is important to note that researchers in the reviewed studies investigated the behaviour and emotions of children who were younger than seven years old by relying only on parents’ proxy reports and in children aged 4–11 years (Yildiz et al., 2001), 6–13 years (Guan et al., 2014) and 6–12 years (Miatton et al., 2007). CYP provided their perceptions regarding their own behavioural and emotional issues only when they were seven years and older (Fredriksen et al., 2009; Miatton et al., 2007; Spijkerboer et al., 2008a, Spijkerboer et al., 2008b). Thus, no self-perceptions of children younger than seven years old were obtained. A better understanding of their behaviour and emotions would be achieved by gathering the children’s personal perceptions and hearing their voices.
The reviewed studies demonstrated that CHD complexity and disease severity seemed to have a consistent effect on the behaviour and emotions of CYP with CHD. The higher the complexity of CHD, the worse the behavioural and emotional status of CYP with CHD. Prolonged hospitalization which is linked to the moderate and severe or complex cases can explain this. Long hospitalization periods for infants and CYP related to complex conditions, including severe cardiac conditions, could increase the mortality rate and cause psychosocial issues in these CYP (Davies et al., 2014). Another explanation could be that the development of emotional problems in CYP with moderate-to-severe CHD is related to the genetic link between the heart and the child’s emotions as it was identified in velocardiofacial syndrome, a heart-related condition (Gothelf et al., 2004). Likewise, the more invasive the management procedures, the greater the behavioural and emotional issues. Post-surgical CYP presented more behavioural and emotional issues than post-cardiac-catheter CYP. Again, the prolonged hospitalization and follow-up time needed for the surgical groups may have impacted on the behaviour more than the cardiac-catheter group who had a less invasive procedure and shorter periods of hospitalization (Guan et al., 2014).
Limitations and strengths of the review
This review is limited in its generalizability as it concentrates on studies that are published in the English language only. Moreover, grey literature was not searched. Therefore, information from the non-English and grey literature might be missed from this review. Another limitation is the exclusion of studies, which investigated the psychosocial status in CYP with CHD, which may have eluded to behaviour and emotions. However, the assessment of psychosocial status can also include domains, such as psychological, psychiatric, mental, or spiritual status, which are not within the focus of this review’s aim. Therefore, articles which studied the psychosocial status of CYP were excluded.
Implications for practice
It is anticipated that the findings of this review will assist International Healthcare Providers in gaining new knowledge and paying particular attention towards these CYP and their families and referring them to get appropriate support. Healthcare providers have a significant influence on educating and teaching parents how to deal with their CYP who have emotional or behavioural issues. Further research will potentially inform the development of future preventive interventions, such as support groups of behavioural and emotional care for CYP with CHD and their families.
Conclusion
All reviewed studies mainly relied on the parents’ proxy reports on their CYP’s behaviour and emotions, and only some of the reviewed studies explored the self-perceptions of CYP, which were obtained only from seven years and older. Indeed, it was highlighted in the reviewed studies that researchers ought to consider CYP’s perceptions about their own behaviour rather than relying only on parents’ proxy reports.
By reviewing the literature, it was clear that CYP with CHD can develop behavioural and emotional issues and that there is a need to incorporate parents’ proxy reports (parents’ perceptions) with their CYP’s self-perceptions. Although parents’ and CYP’s perceptions were obtained in most of the reviewed studies, disparities between both perceptions were clearly demonstrated. Further justifications or explanations of the differences between the two perceptions are needed. Also, further investigation around the relationship between gender and the behavioural and emotional issues in CYP with CHD is needed.
It was identified that there is a need for future qualitative studies that explore in-depth the self-perception of CYP with CHD on their behaviour and emotions, especially for those who are younger than seven years old.
Footnotes
Acknowledgements
We are grateful to the facilities and assistance provided by the UoL (University of Leeds) library’s research support adviser with the literature search.
Author contributions
ND, guided by VS and LM (co-authors and PhD supervisors), conceived the review design. The search strategy was carried out by ND and guided by VS and LM. ND screened the articles by titles and abstracts, and LM rescreened the titles and abstracts of 96 studies. The full text of all reviewed studies was read by ND. The data of the reviewed studies were extracted by ND and guided by VS and LM. The quality appraisal of the reviewed studies was done by ND, and then LM and VS reviewed the quality appraisal of two studies. ND summarized the findings of the reviewed studies narratively and constructed the manuscript. All authors contributed to and agree with the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was granted a doctoral scholarship program from King Abdul-Aziz University in Saudi Arabia, which supported this work. The other authors received no financial support for the research, authorship, and/or publication of this article.