
Abstract
A systematic review examined the association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescents, since it represents an alert to adolescent’s health and well-being. Six electronic databases and gray literature were systematically searched from January 1980 to December 2018. A total of 11 articles met the inclusion criteria. Included studies assessed body weight dissatisfaction using different dimensions/components: satisfaction component of the attitudinal dimension was assessed in five studies, behavior component of the attitudinal dimension was assessed in two studies, perceptual dimension was assessed in two studies, and two studies were unclear about dimension. Behaviors: two assessed only unhealthy eating behaviors, six assessed lack of physical activity, and three assessed both behaviors. Only three studies found an association between body weight dissatisfaction with unhealthy eating behaviors, three with lack of physical activity, and one did not perform a statistical test for an association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity. Few studies have reported an association between body weight dissatisfaction with one of these unhealthy behaviors. There was substantial heterogeneity related to unit of measures, both for body weight dissatisfaction and for behaviors studied.
Introduction
Unhealthy eating behaviors are risk factors for malnutrition in all its forms, as well as for noncommunicable diseases, such as obesity, diabetes, cardiovascular disease, cerebrovascular accident, and cancer (World Health Organization, 2015). Lack of physical activity is a risk for overweight and obesity, diabetes, and cardiovascular disease (Ekelund et al., 2012).
Evidence shows a high proportion of adolescents (10–19 years old) around the world that have unhealthy eating behaviors, such as low consumption of fruits and vegetables (Kann et al., 2016; World Health Organization, 2016), high consumption of carbonated soft drinks daily (Kann et al., 2016; World Health Organization, 2014, 2016), low breakfast consumption (Kann et al., 2016; Pendergast et al., 2016; World Health Organization, 2016), low participation in family meals (World Health Organization, 2016), and lack of physical activity (Sallis et al., 2016; World Health Organization, 2018).
Some studies have shown an association between unhealthy eating behaviors and lack of physical activity with body weight dissatisfaction in adolescence. Body weight dissatisfaction is widespread among adolescents around the world, reaching almost 50%. In general, it is more common among girls than boys and overweight adolescents than underweight adolescents (Al Sabbah et al., 2008; Christofaro et al., 2015; Finne et al., 2011; Matias et al., 2010; Mishra and Mukhopadhyay, 2010; Moehlecke et al., 2018; Sampasa-Kanyinga et al., 2017; Santos et al., 2011). However, even adequate weight adolescents report body weight dissatisfaction (Al Sabbah et al., 2009; Christofaro et al., 2015; Del Duca et al., 2010; Martini et al., 2016; Moehlecke et al., 2018; Santos et al., 2011). These findings show that body weight dissatisfaction is not solely a physiological indicator as BMI-for-age but also involves a subjective construct as body image.
Body weight dissatisfaction is an element of body image. In turn, body image is a multidimensional construct relating to an individual’s perceptions and attitudes toward their own body. It is influenced by sociocultural model, interpersonal experience, and personality (Cash and Smolak, 2012). Moreover, body image is divided into two dimensions: perceptual and attitudinal. The perceptual dimension refers to an individual’s self-perception of their appearance. The attitudinal dimension, however, is subdivided into four components: affective, cognitive, behavioral, and satisfaction. The affective component comprehend feelings related to one’s appearance. The cognitive component refers to knowledge about body image. The behavioral component considers body-checking behaviors and actions to avoid situations or objects that evoke body image concerns. The satisfaction component concerns a person’s appreciation over their body as a whole or to specific parts (Cash and Smolak, 2012).
The satisfaction component of the attitudinal dimension of body image needs to be used to evaluate body weight dissatisfaction. However, literature shows that other dimensions are also used in this evaluation (Thompson, 2004). For example, studies have examined an association between body weight dissatisfaction with lack of physical activity using the perceptual dimension of body image (Finne et al., 2011; Sampasa-Kanyinga et al., 2017) and behavioral component of the attitudinal dimension of body image (Al Sabbah et al., 2008). In addition, studies using the same dimension and component to evaluate body weight dissatisfaction have shown an association between body weight dissatisfaction with lack of physical activity (Matias et al., 2010; Moehlecke et al., 2018), but another one did not (Christofaro et al., 2015).
Thus, the lack of consensus in results justifies undertaking this systematic review. In addition, this review will address a gap in the literature, that is, which dimensions and components are used to assess body weight dissatisfaction. Considering the high prevalence of body weight dissatisfaction, unhealthy eating behaviors and lack of physical activity among adolescents, and potential impact on future and current health status, the relevance of reviewing an association between these factors is also justified. Moreover, during adolescence—a critical and vulnerable phase of life—body image concept is structured (Smolak, 2004), including the concept of body satisfaction/dissatisfaction.
An initial search involving the databases, JBI Database of Systematic Reviews and Implementation Reports, Cochrane Database of Systematic Reviews, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed/MEDLINE, and Prospero, did not identify any systematic reviews that investigated the association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescence.
Therefore, a systematic review was undertaken to examine an association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescents. The protocol of this review was registered on the Prospero by the number CRD42019130018.
Aims and objectives
This systematic review aimed to examine the association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescents. The objectives were (1) to assess the association of body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescents and (2) to assess the dimensions and components of body image used in the studies about the association of body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescents. The review questions were (1) is body weight dissatisfaction associated with unhealthy eating behaviors and lack of physical activity in adolescents? and (2) which dimensions and components of body image are most used to assess body weight dissatisfaction in adolescents?
Methods
Search strategy
The search strategy aimed to find both published and unpublished studies from January1980 to December 2018. An initial limited search of MEDLINE and CINAHL was undertaken followed by analysis of text words contained in the title and abstract and of the index terms used to describe articles. This information helped in the development of a search strategy, which was tailored for each information source. Further databases searched included Embase, PsycINFO, Web of Science Core Collection, and Scopus. The search for unpublished studies included Open Grey literature: Google Scholar, DART-Europe E-theses Portal and Repositório Científico de Acesso Aberto de Portugal (RCAAP). Key terms searched included adolescent terms (preadolescent/adolescent/adolescence/teenager/youth), body weight dissatisfaction terms (body weight/body size/body image/personal satisfaction/dissatisfaction), unhealthy eating behaviors terms (feeding behavior/eating behavior/eating pattern/food habit/eating habit/dietary habit/diet/diet habit/breakfast/carbonated beverage/carbonated drinks/soft drinks/soda pop/fruit/vegetable/family meal/family mealtime), and lack of physical activity terms (exercise/physical activity/physical exercise). British English and American English were applied in the search strategy, as well as singular and plural expressions. Truncation and proximity operators were employed to increase sensitivity of the search (see Supplementary material for full Medline search).
Inclusion criteria
The review considered studies that included adolescents (10–19 years), either male or female, from any country, culture, or ethnicity. According to the World Health Organization, adolescent is defined as any person between the ages 10 and 19 (Patton et al., 2016; World Health Organization, 1986). Papers focusing on a broader age range were included if results were separated for the subgroup of adolescents.
Body weight dissatisfaction was the exposure of interest, which was evaluated according to dimensions and components of body image, as well as their respective units of measure. Therefore, we included studies that measured the perceptual dimension of body image and used units of measure: misperception of the body weight (underestimate/overestimate). We included studies that measured affective and cognitive components of the attitudinal dimension and used units of measure: undesired/unwished weight. We also included studies that measured a satisfaction component of the attitudinal dimension and used units of measure: dissatisfaction with weight (excessive/underweight). Finally, we included studies that measured a behavioral component of the attitudinal dimension and used units of measure: diet to lose weight. These are common units of measure used to evaluate body weight dissatisfaction.
The outcomes included were unhealthy eating behaviors and lack of physical activity. Despite eating behaviors being influenced by geographic conditions, social, and cultural factors of each context, some unhealthy eating behaviors are similar among different countries. Considering variety of food-based dietary guidelines around the world, this review included studies with at least one of these behaviors, and its respective cutoff points: consuming carbonated soft drinks daily (excluding bottled still or carbonated water, fruit or vegetable juices, coffee, tea, or sports drinks) (Utter et al., 2013); not having breakfast (Adolphus et al., 2016; Bi et al., 2015; Blondin et al., 2016); eating less than five times per week in family meals (Utter et al., 2013); consuming less than five servings of fruits and vegetables per day (World Health Organization, 2015); consuming less than two servings of fruits, consuming less than two servings of vegetables (Montagnese et al., 2015; Painter et al., 2002; Utter et al., 2013) (in the case of studies that evaluated fruits and vegetables separated). With regard to lack of physical activity, we considered studies that evaluated physical activity by various questionnaires available (Sylvia et al., 2013), and only a physical inactivity category was included. In case of studies that provided degrees of physical activity, only the category of low physical activity was included.
The observational studies were considered: prospective and retrospective cohort studies, case–control studies, and analytical cross-sectional studies. Randomized controlled trials (RCTs) were not considered, because no RCT was found in an initial search of the literature. Studies published in English and Portuguese were included. The reason for a time frame as of 1980, were important changes with diet (such as increases in the offer and uptake of processed food, prepared meals, and fast foods) and also a reduction in physical activity.
These diet and physical activity changes have contributed to the pandemic of overweight/obesity around the world (Popkin et al., 2012). Since this pandemic is strongly associated with the exposure of interest of this review, that is, body weight, there is justification to undertake a systematic review considering studies published from 1980.
Exclusion criteria
This review excluded:
– Studies that do not distinguish between adults and adolescents.
– Studies that included pregnant adolescents, since during pregnancy an increase of body weight is a normal physiological change, which can cause a momentary body weight dissatisfaction.
– Studies that investigated exclusively body image, because it refers to a broader concept and does not specifically focus on body weight dissatisfaction.
– Studies that investigated exclusively body weight perception or body weight concern.
– Studies that investigated exclusively eating disorders.
– Studies that investigated exclusively sedentary behavior.
Study selection
All identified citations were collated and uploaded into Mendeley (Mendeley Ltd, Elsevier, The Netherlands) and duplicates removed. Titles and abstracts were screened by two independent reviewers (LSD and KSD) for assessment against the inclusion criteria for the review. The details of the studies that met the inclusion criteria were imported and were retrieved in full, into Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI SUMARI) (Joanna Briggs Institute, 2014). Full text of selected studies was retrieved and assessed against the inclusion criteria. Full text studies that did not meet the inclusion criteria were excluded and reasons for exclusion are provided. The results of the search are presented in a Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram. The disagreements between reviewers/authors were resolved by consensus.
Assessment of methodological quality
Selected studies were critically appraised by two independent reviewers (LSD and KSD) at the study level for methodological quality in the review using standardized critical appraisal instruments from the Joanna Briggs Institute specific for each study type. The critical appraisal instruments have been developed and approved by Joanna Briggs Institute Scientific Committee following extensive peer review (Moola et al., 2017). Any disagreements that arose between reviewers were resolved through discussion or with a third reviewer (CNTP). The majority of included studies reported subjects and settings and clear inclusion criteria. All studies achieved ‘YES’ to at least 60% of applicable questions on the checklist (Table 1).
Joanna Briggs Institute critical appraisal checklist for analytical cross-sectional studies—Auality assessment synopsis table.

Note: N/A: not applicable for this systematic review.
Data extraction and data synthesis
Review authors extracted data regarding specific details about study designs, participants, measures of exposure of interest, and results and outcomes using an adapted version of a standardized data extraction tool developed by the Joanna Briggs Institute (Moola et al., 2017). Due to heterogeneity of measures of unhealthy eating behaviors, lack of physical activity, and body weight dissatisfaction, a meta-analysis could not be conducted. The findings are therefore presented as a narrative.
Results
Description of studies
The search of the selected databases generated 3458 citations. Additional records identified through other sources included 604 studies. After removing 1748 duplicates, 2314 articles were screened against title and abstract for eligibility for inclusion criteria. Studies excluded after the title and abstract screening were 2188. Therefore, 126 studies were assessed for full-text eligibility; however, two studies could not be retrieved. Thus, 124 studies were the number of articles assessed for full-text eligibility. Of these, 113 were excluded for several reasons: age more than 19 years (n = 6), body image as exposure of interest (n = 64), and exclusively weight control strategies and eating disorders as outcomes (n = 43). Therefore, 11 articles met the inclusion criteria (Figure 1). All of them reported cross-sectional studies. This information is also presented below.

PRISMA flow chart. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Characteristics of the included studies
Study design
All articles included in this review were cross-sectional studies (Al Sabbah et al., 2008; Christofaro et al., 2015; Finne et al., 2011; Fredrickson et al., 2015; Matias et al., 2010; Mishra and Mukhopadhyay, 2010; Moehlecke et al., 2018; Neumark-Sztainer et al., 1996; Sampasa-Kanyinga et al., 2017; Santos et al., 2011; Xu et al., 2018) (Tables 2 to 4).
Summary of included descriptive cross-sectional studies about unhealthy eating behaviors, according to body weight dissatisfaction dimensions and components.

Note: OR: odds ratio.
Summary of included descriptive cross-sectional studies about lack of physical activity, according to body weight dissatisfaction dimensions and components.
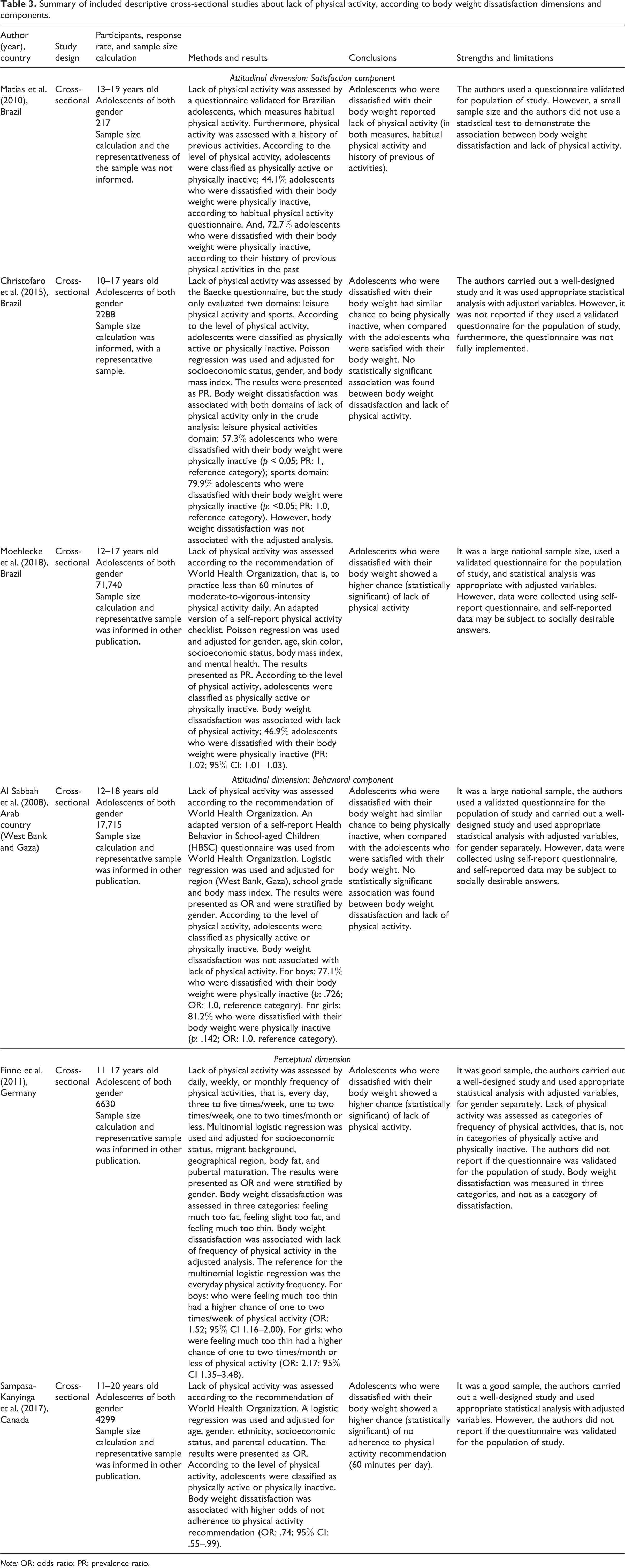
Note: OR: odds ratio; PR: prevalence ratio.
Summary of included descriptive cross-sectional studies about unhealthy eating behaviors and lack of physical activity (both measured), according to body weight dissatisfaction dimensions and components.

Note: OR: odds ratio; PR: prevalence ratio.
Exposure of interest
Body weight dissatisfaction was assessed as follows: five studies used a satisfaction component of the attitudinal dimension (Christofaro et al., 2015; Matias et al., 2010; Moehlecke et al., 2018; Neumark-Sztainer et al., 1996; Santos et al., 2011), two studies used a behavior component of the attitudinal dimension (Al Sabbah et al., 2008; Xu et al., 2018), and two studies used the perceptual dimension (Finne et al., 2011; Sampasa-Kanyinga et al., 2017). However, the methods of two studies were unclear about how they measured body weight dissatisfaction (Fredrickson et al., 2015; Mishra and Mukhopadhyay, 2010) (Tables 2 to 4).
Outcomes measures
Two studies assessed only unhealthy eating behaviors (Mishra and Mukhopadhyay, 2010; Neumark-Sztainer et al., 1996). Unhealthy eating behaviors evaluated were as follows: inadequate consumption of fruits or vegetables, in this case, less than once a day (Neumark-Sztainer et al., 1996), and food group of vegetable–fruit–milk–cereals and of snacks–ice cream–beverages, according to tertile of consumption of these food groups (Mishra and Mukhopadhyay, 2010) (Table 2).
Six studies assessed only lack of physical activity (Al Sabbah et al., 2008; Christofaro et al., 2015; Finne et al., 2011; Matias et al., 2010; Moehlecke et al., 2018; Sampasa-Kanyinga et al., 2017). Among these, three studies assessed lack of physical activity according to the recommendation of World Health Organization (2018), that is, to practice less than 60 minutes of moderate-to-vigorous-intensity physical activity daily (Al Sabbah et al., 2008; Moehlecke et al., 2018; Sampasa-Kanyinga et al., 2017). One study assessed lack of physical activity by the Baecke questionnaire validated for Brazilian adolescents (Matias et al., 2010). This questionnaire included Likert-type scale questions that measure habitual physical activity related to three domains: school activities, leisure physical activity, and sports. Moreover, this study assessed physical activity with a history of previous activities. According to the score of answers to Likert-type questions of this questionnaire, adolescents were classified as physically active or physically inactive (Matias et al., 2010). One study assessed lack of physical activity by the Baecke questionnaire, but this study only evaluated two domains: leisure physical activity and sports. Again, according to the score of answers to Likert-type questions of these two domains, adolescents were classified as physically active or physically inactive (Christofaro et al., 2015). One study assessed the lack of physical activity by daily, weekly or monthly frequency of physical activities, that is, every day, three to five times/week, one to two times/week, and one to two times/month or less (Finne et al., 2011) (Table 3).
Three studies assessed unhealthy eating behaviors and lack of physical activity (both measured) (Fredrickson et al., 2015; Santos et al., 2011; Xu et al., 2018). Only one study assessed these behaviors combined in one variable named lifestyle groups that could be healthier behaviors group (both eating and physical activity), healthier diet only group, physically activity only group, unhealthier behaviors group (both eating and physical activity) (Xu et al., 2018). While the other two studies assessed behaviors separately, both studies evaluated the consumption of fruits and vegetables, but categories of inadequate consumption were distinct as follows: less than five portions of fruits or vegetables per day (Santos et al., 2011), and less than one serve of fruits per day and less than three portions of vegetables per day (Fredrickson et al., 2015). In relation to lack of physical activity, both these studies adopted a recommendation by World Health Organization (Fredrickson et al., 2015; Santos et al., 2011) (Table 4).
Association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity
Only three studies found an association between body weight dissatisfaction with unhealthy eating behaviors; three studies found an association between body weight dissatisfaction with lack of physical activity; and one did not perform a statistical test (Tables 2 to 4).
Regarding two studies that assessed only unhealthy eating behaviors, in one of these, body weight dissatisfaction was associated with unhealthy consumption of fruits or vegetables (Neumark-Sztainer et al., 1996), but the other study did not show a statistically significant association with the lower tertile of the food group consumption of vegetable–fruit–milk–cereals (Mishra and Mukhopadhyay, 2010) (Table 2).
Among the six studies that assessed only lack of physical activity, three reported statistically significant associations between body weight dissatisfaction with lack of physical activity (Finne et al., 2011; Moehlecke et al., 2018; Sampasa-Kanyinga et al., 2017). Two studies did not show an association between these variables (Al Sabbah et al., 2008; Christofaro et al., 2015), and one study did not perform a statistical test (Matias et al., 2010) (Table 3).
The three studies that assessed unhealthy eating behaviors and lack of physical activity, and one study did not report a statistically significant association between body weight dissatisfaction with both behaviors (Santos et al., 2011). Another study observed an association only with inadequate consumption of fruits: less than three portions per day (Fredrickson et al., 2015). The study that assessed behaviors combined in one variable, reported an association with the healthier diet only group (Xu et al., 2018) (Table 4).
Discussion
The purpose of undertaking this systematic review was to examine the association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescents. Due to different measures of unhealthy eating behaviors, lack of physical activity, and body weight dissatisfaction, a narrative analysis of 11 included studies was undertaken.
Several epidemiological surveys have reported a high proportion of adolescents that adopt health-risk behaviors. For example, 50–60% do not consume three to five servings of fruits and vegetables per day (Kann et al., 2016; World Health Organization, 2016), 20–70% consume carbonated soft drinks daily (Kann et al., 2016; World Health Organization, 2014, 2016), and 20–40% do not have breakfast (Kann et al., 2016; Pendergast et al., 2016; World Health Organization, 2016). In addition, less time is spent sharing family meals, since 30–50% of adolescents do not participate in family meals seven or more times per week (World Health Organization, 2016).
In addition, there appears to be high levels of lack of physical activity, evidence supported by a systematic review that reported a decrease in physical activity in adolescence (Dumith et al., 2011). More than 80% of the world’s adolescent population is physically inactive, that is, to practice less than 60 minutes of moderate-to-vigorous-intensity physical activity daily (Sallis et al., 2016; World Health Organization, 2018).
The 2016 Lancet Commission on adolescent health and well-being has revealed that unhealthy eating behaviors and lack of physical activity are associated with poor health status (Patton et al., 2016). It is, therefore, important to understand the factors associated with unhealthy eating behaviors and lack of physical activity. One of these factors may be body weight dissatisfaction.
The prevalence of body weight dissatisfaction in adolescents is high in several countries. For instance, for adolescent girls aged 11 years, results of the Health Behavior in School-aged Children study 2013/2014 showed high rates of body weight dissatisfaction in Denmark (26%), Israel (24%), and Poland (25%). For adolescent girls aged 15 years, high rates of body weight dissatisfaction were in Denmark (44%), Czech Republic (37%), and Iceland (39%). For boys aged 11 years, highest rates were found in Denmark (22%), Israel (21%), and Greenland (20%). For boys aged 15 years, highest rates were found in Israel (20%), Czech Republic (19%), and Luxembourg (17%) (World Health Organization, 2016). In general, it appears that body weight dissatisfaction is reported by girls and varies according with the beginning or ending of adolescence. In addition, individuals who are or believe they are overweight/obese report more frequently dissatisfaction with body weight, so it is highly prevalent in overweight rather than in non-overweight adolescents (Al Sabbah et al., 2009; Caro et al., 2015; Instituto Brasileiro de Geografia e Estatística, 2016).
Similar results were found in countries not represented in the HBSC international study. A national survey conducted with Brazilian adolescents found 30% of body weight dissatisfaction, with girls having the highest percentage of dissatisfaction (Instituto Brasileiro de Geografia e Estatística, 2016). In a cross-sectional study conducted in a Municipality of Spain, 40% of adolescents were dissatisfied with their own body weight (Caro et al., 2015).
During the undertaking of database searches, it was observed that a large number of citations in the literature were related exclusively to body image or weight control strategies and eating disorders such as diet, bulimia, anorexia, binge eating, or restrict dieting. Therefore, the theme body weight dissatisfaction and its relation with unhealthy behaviors, not related to health disorders, appear to be understudied and underestimated.
Among studies that assessed unhealthy eating behaviors, the focus was food groups, especially consumption of portion of fruits or/and vegetables (Fredrickson et al., 2015; Neumark-Sztainer et al., 1996; Santos et al., 2011). In such studies, it was observed that a heterogeneity of recommended portion values, as less than one portion per day—for both fruits or vegetables (Neumark-Sztainer et al., 1996), or less than five portions per day of fruits and vegetables (Santos et al., 2011), or less than one portion per day of fruits and less than three portions per day of vegetables (Fredrickson et al., 2015). This variety of portion values is due to distinct food-based dietary guidelines around the world (Montagnese et al., 2015; Painter et al., 2002).
Other studies that related to eating behaviors reported that one study examined eating behaviors as a combined variable that included several foods (Mishra and Mukhopadhyay, 2010). Another study examined eating behavior as a combined variable that included physical activity, resulting in a variable named lifestyle group (Xu et al., 2018).
The disadvantage of analyzing eating behaviors as a combined variable restricts findings and prevents examination of an association between body weight dissatisfaction with each specific eating behavior, since the variable represents a simultaneity of behaviors. Furthermore, the present review observed limited evidence about an association between body weight dissatisfaction with other eating behaviors, such as consumption of soft drinks, eating breakfast, or having family meals. It is worth noting that comprehending an association between body weight dissatisfaction with unhealthy eating behaviors is important for adolescent current and future health, since unhealthy behaviors start or are consolidated during adolescence (World Health Organization, 2017) and are related with development of noncommunicable diseases, cardiovascular diseases, cancer, type 2 diabetes, and others (Patton et al., 2016).
In comparison to eating behaviors, it was noted that almost all of the studies selected in the present review examined lack of physical activity (Al Sabbah et al., 2008; Christofaro et al., 2015; Finne et al., 2011; Fredrickson et al., 2015; Matias et al., 2010; Moehlecke et al., 2018; Sampasa-Kanyinga et al., 2017; Santos et al., 2011; Xu et al., 2018). Interestingly, it was observed that a variety of recommended values were utilized similarly, as reported for eating behaviors.
Most studies assessed lack of physical activity according to the World Health Organization recommendation, that is, to practice less than 60 minutes of moderate-to-vigorous-intensity physical activity daily (Al Sabbah et al., 2008; Fredrickson et al., 2015; Moehlecke et al., 2018; Sampasa-Kanyinga et al., 2017; Santos et al., 2011). Two studies examined lack of physical activity by habitual physical activity—Baecke questionnaire (Christofaro et al., 2015; Matias et al., 2010) or by daily, weekly, or monthly frequency of physical activities (Finne et al., 2011). As mentioned above, just one study assessed lack of physical activity combined with unhealthy eating behaviors (Xu et al., 2018).
Various ranges of recommended values restrict comparisons between the studies. Moreover, it was observed that validated questionnaires targeted at adolescents were applied in few studies (Al Sabbah et al., 2008; Matias et al., 2010; Moehlecke et al., 2018). Applying a validated questionnaire, or at least conducting a pilot of the questionnaire, enhances rigor and reduces the chance of different interpretations that may result in misleading findings.
Some of the studies clearly showed an association between body weight dissatisfaction with unhealthy eating behaviors (Fredrickson et al., 2015; Neumark-Sztainer et al., 1996; Xu et al., 2018) and lack of physical activity (Finne et al., 2011; Moehlecke et al., 2018; Sampasa-Kanyinga et al., 2017). Therefore, this review cannot report unanimous and conclusive findings. Some possible explanations have already been discussed, that is, variation in recommended values for unhealthy eating behaviors and lack of physical activity, and the lack of validated scales target at adolescents.
In addition, it is important to note that the studies included in this review utilized different ways of measuring body weight dissatisfaction. This is relevant since these measures represent different dimensions and components of body image, that is, examine different perspectives of body weight dissatisfaction. Only a satisfaction component of the attitudinal dimension represents the body weight dissatisfaction, and only five of the studies assessed this dimension (Christofaro et al., 2015; Matias et al., 2010; Moehlecke et al., 2018; Neumark-Sztainer et al., 1996; Santos et al., 2011).
Literature has shown that some covariates such as country/region of origin, age group, gender, and body mass index are related to both body weight dissatisfaction (exposure of interest) and unhealthy eating behaviors and lack of physical activity (outcomes) (World Health Organization, 2016). In other words, these covariates can be potential confounders and statistical analysis should be adjusted, and this was observed in the majority of studies selected (Al Sabbah et al., 2008; Christofaro et al., 2015; Finne et al., 2011; Moehlecke et al., 2018; Neumark-Sztainer et al., 1996; Sampasa-Kanyinga et al., 2017; Xu et al., 2018).
Limitations
This systematic review has some limitations. One of the limitations is inclusion of only observational studies, since there are no RCT evaluating an association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity. Another limitation is the heterogeneity of studies included with respect to measures of unhealthy eating behaviors, lack of physical activity, and body weight dissatisfaction. Despite the comprehensive search across all databases, some eligible studies may have been missed. The review only included studies in English and Portuguese, so additional studies written in other language may have been excluded.
Implications for practice
Evidence from this systematic review suggests the need for health professionals, educators and parents to consider adolescent’s thoughts and feelings about their body weight. In other words, body weight satisfaction/dissatisfaction is an important aspect that should be incorporated in any adolescent’s assessment, and it is necessary to avoid any comment that leads to body weight dissatisfaction. Thus, health systems would act effectively with regard to unhealthy eating behaviors (inadequate consumption of fruits or vegetables) and lack of physical activity among adolescents.
Implications for research
This systematic review suggests the need for further investigation, considering the use of satisfaction component of the attitudinal dimension of body image, use of a validated questionnaire of unhealthy eating behaviors and lack of physical activity for adolescents, and use of adjusted statistical analysis. In addition, there is a need to undertake further studies that explore other unhealthy eating behaviors. Lastly, there is a need for prospective and retrospective studies or case–control studies, since cross-sectional design preclude any conclusions about the direction of causality.
Conclusions
The association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity varied greatly among the included studies. Just a few studies reported any association between body weight dissatisfaction with one of these unhealthy behaviors. For all outcomes, there was substantial heterogeneity related to measures, even for the exposure of interest. Regardless of heterogeneity, body weight dissatisfaction can be seen as an associated factor with these unhealthy behaviors.
Supplemental material
supplementary_material - The association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescents: A systematic review
supplementary_material for The association between body weight dissatisfaction with unhealthy eating behaviors and lack of physical activity in adolescents: A systematic review by Luciane Simões Duarte, Claudia Nery Teixeira Palombo, Katherine Solis-Cordero, Aline Yukari Kurihayashi, Mary Steen, Ana Luiza Vilela Borges and Elizabeth Fujimori in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.