
Abstract
This study investigates the influence of household socioeconomic status and maternal risk factors and health-care service availability on changes in the under-five mortality rate (U5MR) in Bangladesh. Potential risk factors that influence U5MRs were investigated using multilevel logistic regression analysis and 29,697 data points from the Bangladesh Demographic and Health Surveys, 2004–2014. Maternal and child health parameters such as childhood morbidity, low vaccination coverage, poor utilization of perinatal care, and malnutrition were found to be more concentrated in poorer households. Pooled estimates indicated that the aggregate odds of U5MR risk declined by 18% to 2007 to 38% to 2014 compared to 2004. However, inadequate antenatal care, short birth interval, primiparity, illiteracy, delayed conception, and low socioeconomic status were significantly associated with a higher risk of under-five mortality. The magnitude of inequality using these measures were significantly associated with large variations in U5MR changes. Although a significant reduction in U5MR in Bangladesh was found in this study, substantial socioeconomic variations still persist. The analysis suggests that decreasing inequality in society is required for further reductions in child mortality. This will help to achieve a more equitable distribution of child and neonatal outcomes and assist the achievement of Sustainable Development Goals 3.2 by 2030.
Introduction
Globally, child mortality has been reduced significantly over the past 25 years. Despite this, approximately 6 million children die each year before reaching their fifth birthday (United Ttglobally to reduce the under-five mortality rate (U5MR), especially in low- and middle-income countries (LMICs)). The U5MR has dropped globally over these years by 53% (from 91 deaths per 1000 live births in 1990 to 43 deaths per 1000 live births in 2015), but the rate still remain alarmingly high (UNICEF, WHO, World Bank, UNDESA, 2015). Several studies have found a high burden of U5MR remains particularly in South Asian countries (1 death out of 15 live births) and sub-Saharan African countries (1 death out of 8) (Adepoju et al., 2012; Hossain et al., 2015). The high U5MR is especially evident in LMICs (76 deaths per 1000 live births) compared to high-income countries (7 deaths per 1000 live births) (United Nations, 2015).
The Millennium Development Goals (MDGs; 1990–2015) aimed to improve the lives of the world’s poorest people through initiatives to promote improved outcomes in education, health, and welfare. However, only a few LMICs met the MDG-4, which targeted a two-thirds reduction in the U5MR between 1990 and 2015 (Black et al., 2016; You et al., 2015). Bangladesh is one of the few countries that achieved MDG-4, particularly the target of reducing U5MR to at most 48 per 1000 live births with the current rate at 46 per 1000 live births (NIPORT, 2016). The more recent Sustainable Development Goals (SDGs) seek to expand the work initiated through the MDGs. One of the health goals (SDG-3) aims to reduce U5MR to 25 deaths per 1000 live births worldwide by 2030 (United Nations, 2016). According to the World Health Organization (WHO), a total of 79 countries have an U5MR above 25, among them, 47 countries who projected are not to be able to reach the SDG-3 target by 2030 (WHO, 2017). To achieve the SDGs, inequality will need to be reduced both across and within different groups within society (United Nations, 2016). Achieving the goals, especially SDG-3, will move countries closer to achieving Universal Health Coverage (UHC). This will ensure that all people, irrespective of their socioeconomic class, who need health services would receive them, without incurring undue financial hardship. The U5MR target is a priority if UHC is to be achieved (Gwatkin, 2005).
This recent remarkable improvement in child survival in Bangladesh is not evenly spread through the different stratum of society. The present concern is that inequality of U5MR will continue in communities with lower levels of wealth and income and in remote and hard-to-reach areas. Socioeconomic health inequality is well researched in contemporary high-income countries (Hoffmann et al., 2016; Khang and Kim, 2016), but much less researched in LMICs (Houweling and Kunst, 2010). Most indigenous studies generally described the incidence of U5MR and its associated determinants as this remains a significant public health concern in Bangladesh. Reducing inequality and saving more children’s lives by ending preventable child deaths are important priorities in Bangladesh (NIPORT, 2016).
The three objectives of this study are as follows: first, to investigate the distribution of the magnitude of U5MR in Bangladesh over the period 2004–2014; second, to examine socioeconomic inequality in terms of outcomes in maternal and child health parameters; and third, to identify the factors determining the U5MR of Bangladesh, over the 10-year period 2004–2014.
Methods
Data source and sample
The magnitude of socioeconomic inequality in terms of maternal and child health indicators were examined using the latest four rounds of the Bangladesh Demographic Health Survey (BDHS), which is a nationally representative cross-sectional study of Bangladesh households. A wide range of information on household characteristics including living arrangements, health and nutritional status, health-care services, and knowledge and practices related to health and health-care–seeking behavior is covered. Data were collected by Measure Demographic and Health Survey (DHS) retrospectively by surveying mothers whose youngest children were under-five years of age. The sampling technique, survey design, survey instruments, measuring system, and quality control are described elsewhere (Measure DHS, 2017). According to standard DHS practices, written consent was taken from all potential respondents before conducting the survey. The DHS data set is publicly accessible; however, e-mailed consent also obtained as part of the protocol. Inconsistent, unusual/abnormal and missing observations were excluded from the analysis. Finally, a total of 29,697 samples were analyzed: 2004 (n1 = 6908), 2007 (n2 = 6150), 2011 (n3 = 8753), and 2014 (n4 = 7886). Recall bias and underreporting of deaths might have an effect on the estimated child mortality rates. To handle this concern, data were pooled from multiple surveys.
Definition of maternal and child health indicators
Under-five mortality rate
The U5MR was treated as an outcome variable in the analytical exploration, which is the dominating parameter in measuring child health outcomes and their improvement. According to the DHS guidelines, U5MR was measured in terms of the probability of a child dying before reaching the age of five years and expressed as a rate per 1000 live births (Croft et al., 2018).
Nutritional status
Childhood nutritional status was measured in terms of stunting, wasting, and underweight using three well-established anthropometric measurements recommended by the WHO (WHO, 2008), including height-for-age z-score (HAZ), weight-for-age z-score (WAZ), and weight-for-height z-score (WHZ). Survey data on child height, weight, and age were restricted, and z-scores (HAZ, WAZ, and WHZ) were measured using the WHO (2006) child growth guidelines. A child was defined as stunted if HAZ was below −2 standard deviation (SD) from the mean of the reference population. Similarly, if WAZ was less than or equal to −2 SD and if WHZ was less than or equal to −2 SD, then the child was defined as underweight and wasting, respectively.
Vaccination coverage
Vaccination histories (e.g. BCG, pentavalent 1/DPT1, pentavalent 1/DPT1, pentavalent 1/DPT1, polio 1, polio 2, polio 3, and measles) were constituted as dummy variables based on whether or not children had been vaccinated. The Expanded Programme on Immunization (EPI) card was used where available and historical recall data when the EPI card was unavailable. Children who were younger than the recommended age for each vaccine were excluded from the calculation of immunization coverage.
Childhood morbidity
Childhood morbidity was measured by the number of diarrheal episodes, symptoms of ARI (whether any cough or chest-related breathing difficulties were observed as a proxy for pneumonia), and fever for the youngest children under five years old, which occurred in the two weeks preceding the survey. These constituted binary variables denoting 1 if present and 0 if absent.
Antenatal and postnatal care visits
Antenatal care coverage was defined as the percentage of women giving birth in the last five years, distributed by the highest type of provider of antenatal care for their most recent birth. Further, postnatal coverage was defined as those women who had given birth in the two years preceding the survey and the distribution of the mother’s first postnatal visit for the most recent live birth by time (in weeks) after delivery.
Estimation Strategy
Annualized percentage change
The annual percentage change (APC) of the participant characteristics and health indicators in terms of maternal and child health was estimated to find out the overall trend direction. Further, increased or decreased APC of maternal and child health-care–related outcomes was estimated to examine the magnitude of maternal and child health indicators over the period. The base year for this calculation is 2004 and current year is 2014.

where PCY indicates prevalence at the current year (i.e. latest DHS survey year in 2014), PBY indicates prevalence at the base year (i.e. DHS survey year in 2004), and n indicates duration between the current and base years.
Measuring socioeconomic inequalities for health indicators and U5MR
The inequality analysis commenced with a simple comparison of U5MR and other health indicators across socioeconomic status. The poor–rich difference (PRD) and poor–rich ratio (PRR) of U5MR and other health indicators were estimated. Higher values of PRD and PRR suggest that higher inequality exists (Schneider et al., 2005). However, these measures do not demonstrate the overall picture of childhood mortality when adjusted for household socioeconomic characteristics. Standard measures of concentration index (Conc.I) were used to examine the magnitude of socioeconomic inequality and the trends in U5MR changes during the period of 2004–2014. Hence, concentration curves (CCs) that plot the cumulative proportion of health outcomes against the cumulative proportion of the population ranked from the poorest to the richest were constructed (Kakwani et al., 1997; Schneider et al., 2005). A wealth index was used to plot the CCs to aid the estimation of the Conc.I (Kakwani et al., 1997; Wagstaff et al., 1991). The index takes a negative value when the curve lies above the line of equality, meaning there is a disproportionate concentration of health outcomes among poor households, and a positive value when it lies below the line of equality (i.e. the 45° line, which characterizes a perfectly equal distribution of child health outcomes among participants across socioeconomic positions) (Kakwani et al., 1997; Wagstaff et al., 1991). The Conc.I was derived from these curves as twice the area between the CC and the line of equality. The CC lies above (below) the line of equality if maternal and child health indicators are higher (lower) in values among the poorest. The Conc.I estimated as the covariance between the health indicators and the proportional rank in socioeconomic position (O’Donnell et al., 2009) is as follows:

where Conc.I is the concentration index,
Conc.I acquires a negative value when the curve lies above the line of equality, which indicates a disproportionately higher prevalence of health indicators among the poor (i.e. pro-poor). A positive value of Conc.I signifies a higher concentration of health indicators among the rich (i.e. pro-rich). There is no socioeconomic inequality in the distribution of health indicators (y) when the value of Conc.I is 0, and the CC coincides with the 45° line. In addition, when the outcome variable is dichotomous, the Conc.I has to be corrected to allow comparisons between the groups of individuals from different time periods that may show different levels of health indicators (Erreygers, 2009). In the context of a dichotomous outcome variable, the Erreygers’s (2009) Conc.I is the Conc.I multiplied by four times the mean health or outcome of interest. Erreygers suggests the following corrected Conc.I can be expressed as:

where
Multivariate analysis
The BDHS was conducted using multistage stratified clustered sampling; the dependence among observations derives from several levels of hierarchy, which is a cluster effect in the data set. Therefore, a single-level statistical model is not appropriate to analyze this type of hierarchical data set (Khan and Shaw, 2011). The hierarchy for this study followed participants as level 1. These participants were nested within households in the place of residence as level 2 and divisions as level 3. This multilevel logistic modeling takes into account the hierarchical structure of the data and the variability of the clusters, households, and individuals to achieve robust estimates. To remove the cluster effect, the adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were estimated to identify the associated risk factors with U5MR. The statistically significant level was considered a p value of ≤.05. All statistical analyses were undertaken using Stata/SE 13.0 (StataCorp, College Station, TX).
Ethical approval
The DHS data set is publicly accessible; however, mailed consent was also obtained as part of the protocol (https://dhsprogram.com/data/available-datasets.cfm). Approval was received from the Measure DHS program to use the data sets in this study.
Results
Distribution of socioeconomic and demographic characteristics of study participants
Table 1 presents the changes in socioeconomic and demographic indicators between 2004 and 2014. The proportion of adolescent pregnancy and delay in conception was annually reduced by 2.42% and 1.56%, respectively. Furthermore, the prevalence of early marriage significantly dropped by 12.25% and annually declined by 1.56%. The percentage of no-schooling experience (21.14%) of the mothers showed a significant reduction by 8.20% annually. The higher fertility preference (>3 children) of mothers was reduced by 2%. In addition, preceding birth interval was significant and followed an increasing trend. Receiving recommended antenatal care visits (four or more) were significantly increased by 2.54% per year.
Background characteristics of the study population.
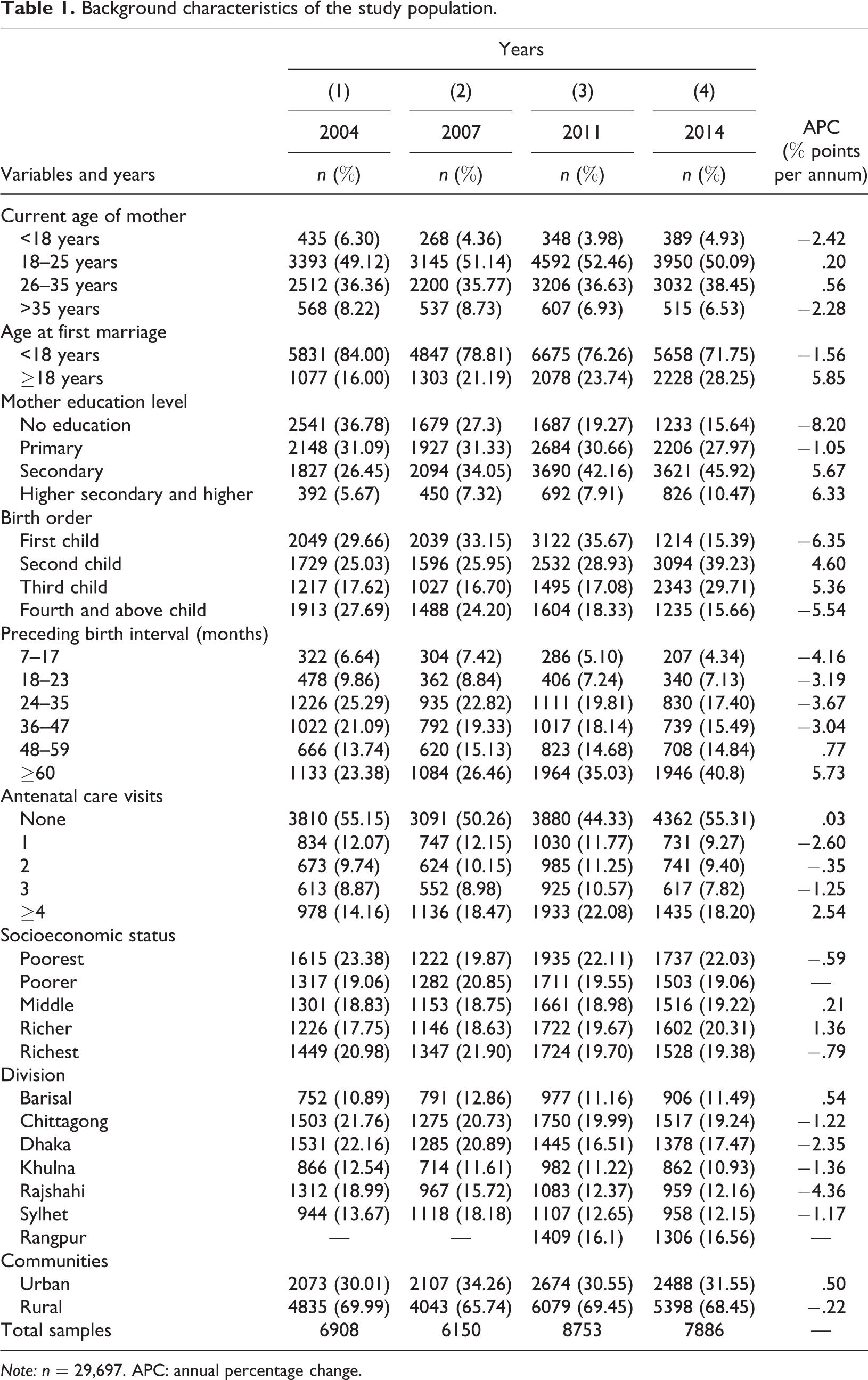
Note: n = 29,697. APC: annual percentage change.
Distribution of U5MR across wealth status
Figure 1 depicts trends in U5MR stratified by wealth quintiles. Although the rate of U5MR is consistently reduced across wealth quintiles, the reduction rate was highest in the richest households. U5MR trended downward across all socioeconomic groups, with the richest quintile performing better than their poorest in terms of annualized absolute decline.

Distribution of U5MR across wealth quintiles. U5MR: under-five mortality rate.
The PRD and PRR of U5MR between poorest and richest households decreased from 49 to 23 per 1000 live births as shown in Figure 2. Expressed as a rate-ratio between the poorest and richest households, the rate-ratio was 1.7 in 2004 and slowly increased to 1.8 in 2014. Although the overall U5MR has dropped, children from the poorest households are bearing a relatively increasing share of the burden compared with children from the richest. Consistent with the earlier results, the CI for U5MR significantly increased (in absolute value) from .070 in 2004 to .107 in 2014 as shown in Figure 3. The negative values signify that the U5MR was disproportionately concentrated in the poorest households.

Unequal distribution of U5MR by wealth status. U5MR: under-five mortality rate.
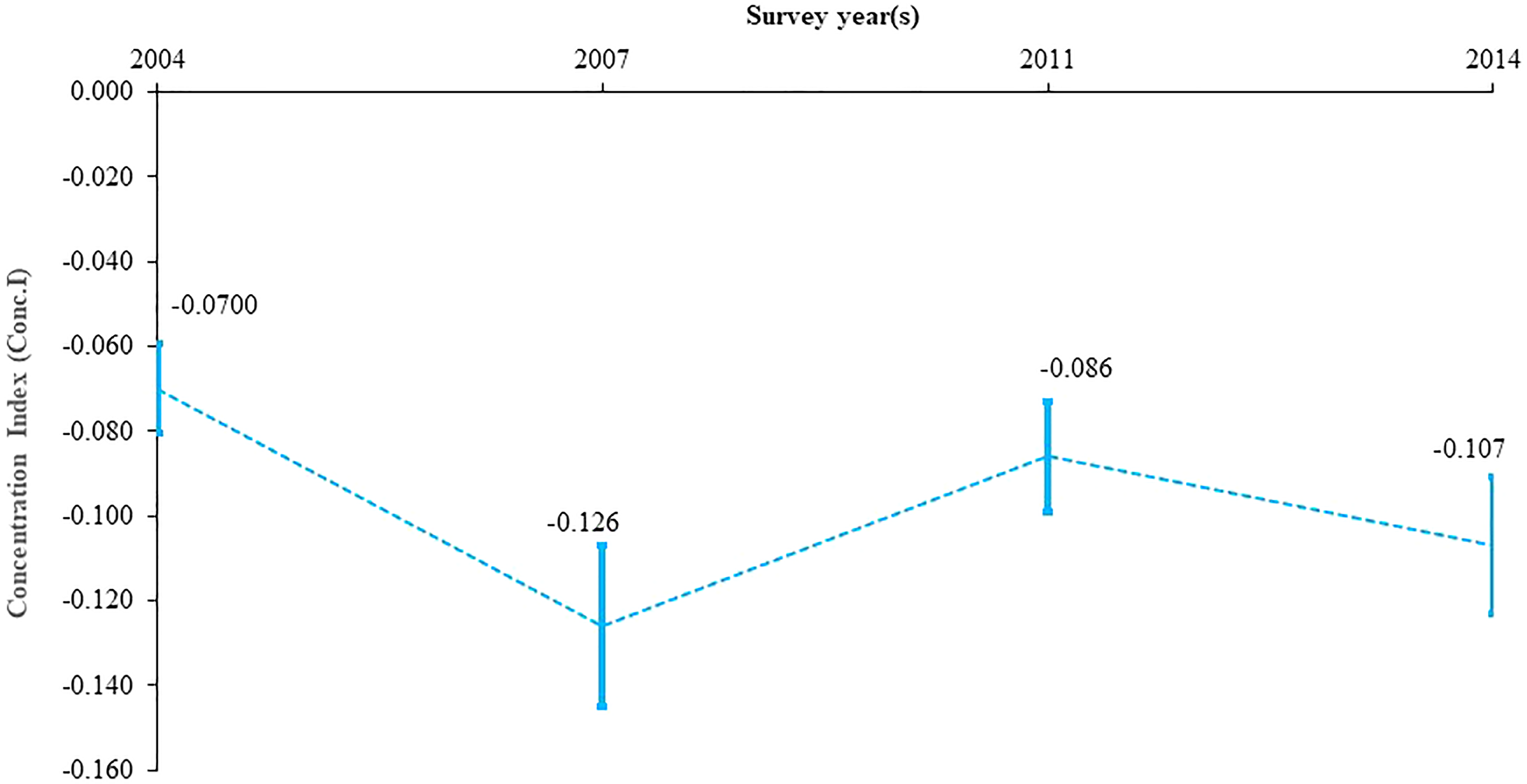
Trend of inequality of under-five mortality rate.
Magnitude of socioeconomic inequalities for maternal and child health parameters
Table 2 demonstrates the wealth-stratified inequality on health indicators. There is a notable difference observed between the poorest and the richest households for maternal and child health indicators. Individuals from the poorest households were much more likely to experience malnutrition, lower vaccination coverage, poorer utilization of perinatal care, and thus a higher risk of childhood morbidity. Examining nutritional status, the rate of stunting consistently declined across wealth quintiles and the reduction was greater in the richest quintile relative to the poorest. A similar story holds for the underweight parameter. The concentration index (Conc.I) for nutritional status, that is, stunting and underweight, significantly increased from −.119 and −.112 in 2004 to −.157 and −.157 in 2014, respectively. The negative values signify that stunting and underweight were disproportionately concentrated in poorer households. Although Bangladesh has made remarkable improvements in vaccination coverage, inequality still exists between the poorest and richest quintiles. However, the poorest quintile shows better outcomes in terms of annualized absolute improvement compared to the richest quintile. Children from the poorest households experienced morbidities disproportionately higher than the richest. The inequality in utilization of antenatal and postnatal care (for mother and child) services trended downward overall, which was a similar picture for postdelivery care.
Distribution of wealth-stratified inequality on maternal and child health indicators.
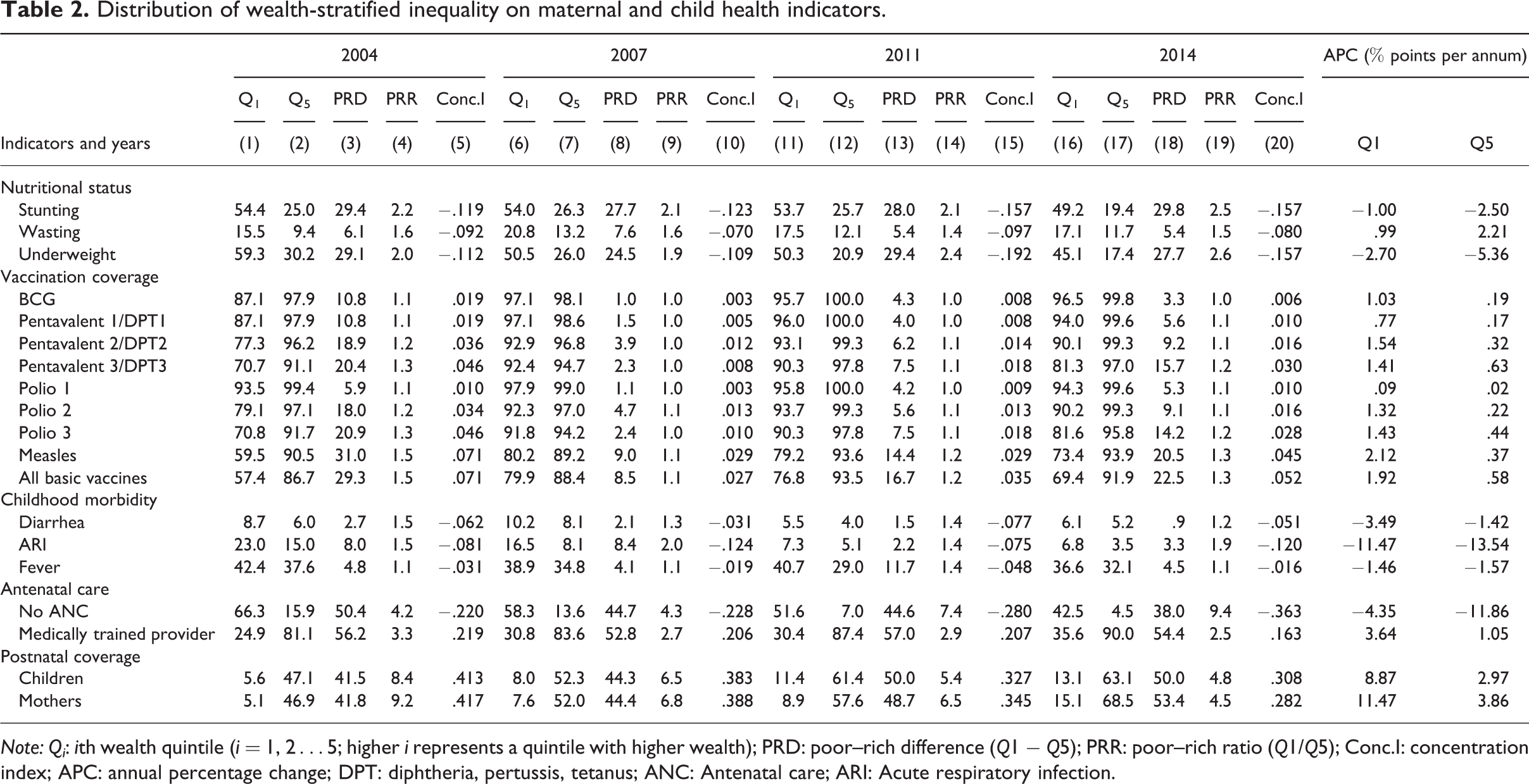
Note: Qi: ith wealth quintile (i = 1, 2…5; higher i represents a quintile with higher wealth); PRD: poor–rich difference (Q1 − Q5); PRR: poor–rich ratio (Q1/Q5); Conc.I: concentration index; APC: annual percentage change; DPT: diphtheria, pertussis, tetanus; ANC: Antenatal care; ARI: Acute respiratory infection.
Factors influencing higher risk of U5MR
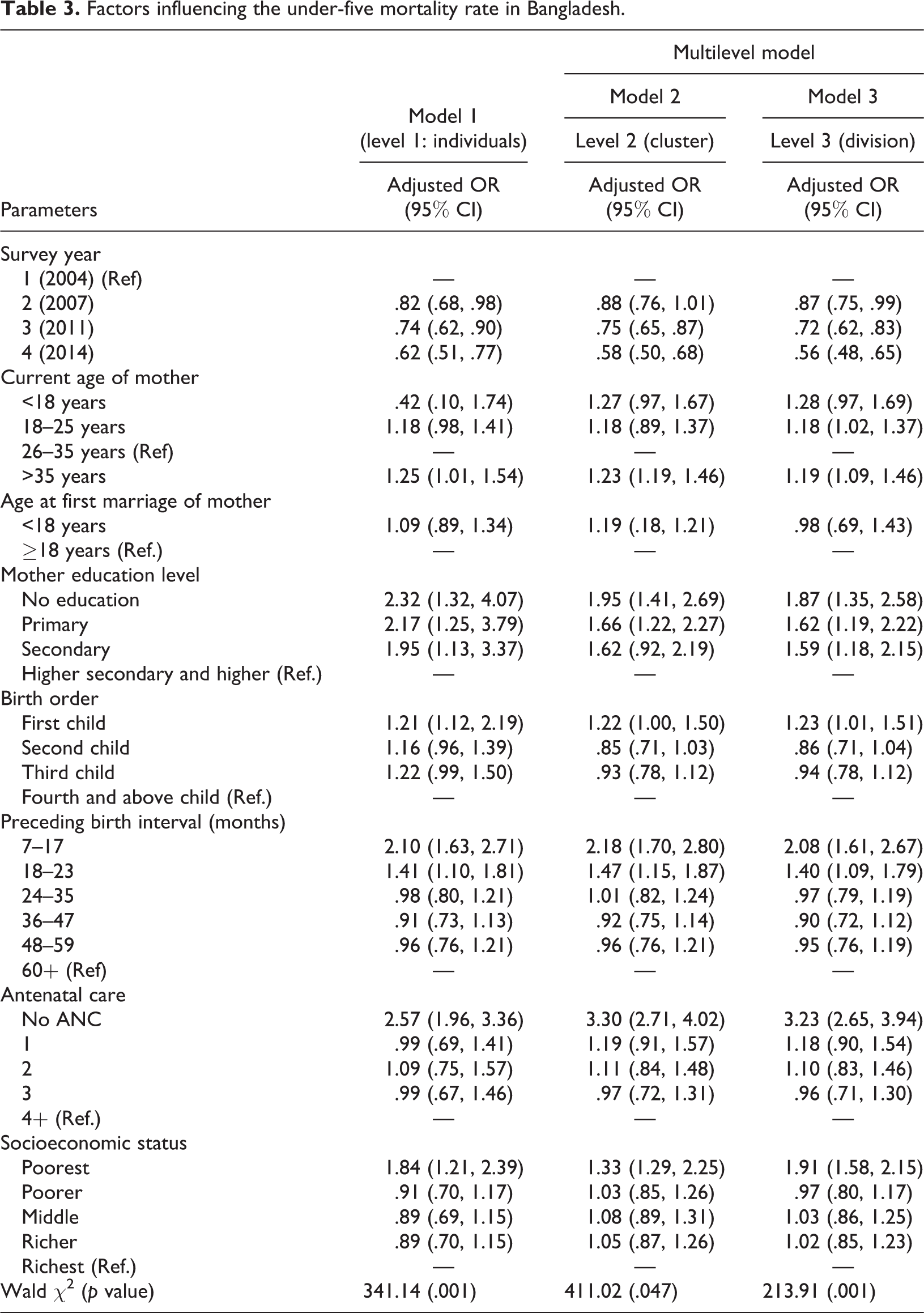
Model 1 shows that the odds of having U5MR were significantly reduced by 18% in 2007, 26% in 2011, and 38% in 2014 compared to 2004 (Table 3). After controlling for confounding factors, the risk of U5MR was highest in model 1 among the children whose mothers were aged 35 years or above (OR = 1.25, 95% CI 1.01–1.54), had no formal education (OR = 2.32, 95% CI 1.32–4.07), delivered with a short birth interval (OR = 2.10, 95% CI 1.63–2.71), did not receive any antenatal care (OR = 2.57, 95% CI 1.96–3.36), or came from the poorest households (OR = 1.84, 95% CI 1.21–2.39). Models 2 and 3 also show similar associations consistent with model 1, the odds of having higher risk of U5MR were also more pronounced among older women, those who were illiterate, and those who received inadequate antenatal care services or came from disadvantaged households. However, the magnitude of the effect of those independent factors varied over the study period.
Factors influencing the under-five mortality rate in Bangladesh.
Discussion
In many LMICs including Bangladesh, inequality in childhood mortality due to socioeconomic and demographic factors is a major public health concern. The childhood mortality rate reflects a country’s socioeconomic development and the health status of its children. The present study captured the socioeconomic inequality in maternal and child health indicators and also investigated potential risk factors that were associated with a higher risk of U5MR. The overall risk of U5MR has declined from 88 per 1000 live births in 2004 to 46 per 1000 live births in 2014, and the country was able to achieve MDG-4 (Chowdhury et al., 2011). The results show that U5MR has consistently declined across wealth quintiles over the period 2004–2014. However, the annual reduction rate was slightly lower among the poorest quintile compared with the richest. The results indicate that the inequality gap has substantially increased over time. This finding is in line with the time trend measures of inequality that had been experienced by the most disadvantaged populations elsewhere (Minnery et al., 2015). The results suggest that the observed increasing socioeconomic inequalities in U5MR are an ongoing public health challenge in Bangladesh (Khang and Kim, 2016; Minnery et al., 2015). This inequality unfortunately pervades the entire society, which means the poorest children are relatively more disadvantaged compared with children from richer households. This situation signifies the need for immediate policy attention to address the problem. Addressing these disparities by improving the health of disadvantaged children up to the level of more advantaged groups would significantly improve health overall (Houweling and Kunst, 2010).
The magnitude of inequality in terms of maternal and child parameters were disproportionately concentrated among the most socioeconomic disadvantaged households over the study period. Disadvantaged household members were more likely to report adverse outcomes such as chronic malnutrition, lower immunization coverage, poorer utilization of pre- and postdelivery care services, and increased childhood morbidities. Similar findings were found in previous studies whereby children from the most disadvantaged households experienced higher rates of chronic malnutrition (Rabbani et al., 2016), lower immunization coverage (Devasenapathy et al., 2016), poor utilization of pregnancy-related health care (Sarker et al., 2018), and higher childhood morbidities (Mahumud, Alam, Renzaho, et al., 2019). It is apparent from this study results and the literature that strong leadership, health system reform, improved health services, and low-cost and effective health interventions in relation to the women’s preferences for maternal health-care services (Mahumud, Alamgir, Hossain, et al., 2019) are needed to mitigate and improve the health indicators. Importantly, health education and awareness are needed to improve the lower utilization of health services by poorer communities. Furthermore, nutrition-related programs should be the main driver to reduce chronic malnutrition in poorer households (Huda et al., 2018).
The adjusted analysis results demonstrate that the childhood mortality risk was highest among children whose mothers were aged 35 years or more. Several reasons might contribute to this adverse outcome. For example, advanced maternal age (>35 years) is significantly associated with an increased risk of adverse pregnancy outcomes including hemorrhage, miscarriage, stillbirth, preterm birth, intrauterine growth restriction, and low birth weight (Fall et al., 2015; Government of Bangladesh, 2012). Further, older mothers are more likely to suffer from chronic illness and pregnancy-related complications (Fall et al., 2015; Neill et al., 2013). Therefore, the risk of U5MR may be reduced further by counseling older women, both before and after conception, as well as improving access to modern contraceptive to reduce unplanned and high-parity births (Black et al., 2016; Minnery et al., 2015).
The length of preceding birth interval significantly contributed to a higher risk of mortality. Findings from the present study signified that children who were born with shorter preceding birth intervals (≤18 months) were at a greater risk of childhood mortality. A number of previous studies confirm this study finding (Ezeh et al., 2015; Mustafa and Odimegwu, 2008; Rutstein et al., 2005; Whitworth and Stephenson, 2002; Zere et al., 2015). Further, this situation significantly contributes to adverse maternal health outcomes and increase the high risk of infectious diseases (Gribble, 1993; Rutstein et al., 2005). These mothers commonly experience chronic malnutrition, deliver low-birth-weight babies, and have premature births. All these factors influence the risk of having a small or an extreme low birth weight for child leading to higher child mortality (Alexander et al., 2003; Lau et al., 2013).
The study results found that illiterate mothers increased the risk of U5MR compared with more highly educated mothers. A mother’s educational achievement has a substantial association with child survival. Educated mothers are significantly associated with good knowledge on maternal and child health care as well as having a higher socioeconomic status (Caldwell, 1979, 1994; Das, 1990). Further, educated mothers are more conscious regarding child health, illness, preventive care, and proper utilization of modern health services. An educated mother also allows change in the traditional patriarchal relationship in terms of decision-making. Women’s empowerment plays a significant role in reducing adverse child health outcomes (Caldwell, 1979, 1994; Das, 1990).
Further results show that mothers receiving insufficient antenatal care is a significant contributor to increased childhood mortality. This outcome is similar to previous studies in other LMICs (Houweling and Kunst, 2010; Minnery et al., 2015; You et al., 2015). These results suggest that the degree of risk may be reduced by offering a standard frequency of antenatal care.
Despite the overall decline in childhood mortality, inequality measurements showed that progress toward achieving SDG-3 might not be equally distributed. The study results show that children from the poorest households have had significantly higher risk of premature death compared to the richest households. Previous studies conducted in LMICs also found a positive association between poorer households and higher levels of U5MR (Gwatkin et al., 2007; Houweling and Kunst, 2010; Khang and Kim, 2016; Minnery et al., 2015). Women from lower economic groups cannot afford proper health care during pregnancy due to financial hardship, high out-of-pocket costs, and widespread informal payments for health services, especially in rural, remote, and disadvantaged areas. Health sector changes should concentrate on addressing these equity issues, which should induce greater mortality reductions in the future. An adjusted target of economic empowerment programs for disadvantaged women and a scale-up of equal access to health care will reduce U5MR further (Ahmed et al., 2013). Sustained economic growth is a necessary condition to reduce the impoverishment of households and improve overall health. Activities both in health services and in socioeconomic development are reflected in improvements in the key determinants of health (Ahmed et al., 2013). Further, an exploration of maternity health-care changes designed to reduce or modify controllable parameters that are associated with adverse outcomes is also urgently needed.
Conclusions
The results from this study found that Bangladesh has experienced a significant reduction in under-five mortality over the period 2004–2014. Proven reproductive, maternal, newborn, and child health interventions have contributed to this development. However, inequality in outcomes persist and this is a burning issue that needs addressing if UHC and SDG-3 are to be achieved in the future.
Priority areas to be addressed include inadequate antenatal care, short birth interval, primiparity, low levels of mother’s education, and delayed conception. The main child health indicators including increased morbidity, low vaccination coverage, and malnutrition continue to be more concentrated in poorer households. Policy makers should focus on addressing community resilience and cohesion; improving leadership and participatory governance for health, individual, and community strengths that protect and promote health; improving the quality of health services; and creating better access to proper health-care facilities. Setting targets to reduce health inequalities can help drive action and is one of the principal ways of addressing health development and accomplishing equity-oriented UHC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.