
Abstract
The purpose of this article is to offer an improved understanding of how parents of children with long-term disabilities are empowered to successfully take up their role as decision-making partners in the design and delivery of the care of their child. The intention is to stimulate dialogue, encourage reflection and provide practical suggestions for health professionals working with children and their families. The reported findings are from a study which was guided by a constructivist grounded theory methodology. This involved an iterative process of repeated cycles of data collection and analysis, which comprised 12 semi-structured, in-depth interviews with 14 parents of children accessing paediatric services within a single National Health Service Trust. A novel model, explaining how the power im/balance and the perceived state of the therapeutic relationship influence how successfully a parent takes up their position in the collaborative partnership, is presented and discussed. It is suggested that by thoughtfully addressing the traditional hierarchy that exists within healthcare, health professionals might facilitate the development of a ‘truly’ therapeutic relationship, which can help promote parental empowerment.
Introduction
Context
Over the past 20 years, there have been considerable developments in the UK government legislation regarding the provision of health and social care to children with long-term disabilities, much of which has been underpinned by the core philosophies of family-centred care (Dunst et al., 1991; Rosenbaum et al., 1998). In 2014, the publication of the Children and Families Act (Great Britain Parliament, 2014) underscored legislative commitment to prioritising the needs and desires of children and their families, positioning parents as collaborative partners in the planning and provision of their child’s specialist care. These core values have since been enshrined in both national and international healthcare policy, informing the National Health Service (NHS) constitution (DoH, 2015), the NHS Long Term Plan (NHS England, 2019) and the World Health Organisation’s ‘Health 2020’ framework (WHO, 2012).
Background
There is a growing body of literature which explores parental perceptions of their role in the collaborative partnership, how this partnership develops and how it can be supported by health professionals. Much of this work seems to support that parents are keen to participate in shared decision-making with health professionals (Lerret et al., 2016; Mak et al., 2017; Rosati et al., 2017); however, there appears to be a number of factors that influence how successfully parents are empowered to do this in practice.
There is recognition that developing knowledge and understanding is vital for parents to feel empowered to take an active role in decision-making (Alsem et al., 2017). Consequently, health professionals need to be aware of parents’ level of understanding (Harvey and Redshaw, 2016; Lipstein et al., 2016), their learning needs (Nightingale et al., 2015) and their readiness for information (Reeder and Morris, 2016). It has been reported that parents can feel frightened and overwhelmed by the increased responsibility associated with shared decision-making (Hutton and King, 2017; Smith et al., 2015) and that, without support, parents are likely to continue to rely on health professionals to administer treatment and care (Kruijsen-Terpstra et al., 2016). Even when parents do consider themselves capable and confident decision makers, there are situations where this has not been supported by health professionals. A study by Fixter et al. (2017) found that while parents of children with cystic fibrosis viewed themselves as experts and wanted to retain the responsibility for decision-making while their child was an in-patient, ward staff did not recognise this and took over. It is possible this finding is made more conspicuous by the context of the study, as in an in-patient environment, it is routine for health professionals to administer care; however, it does bring into focus a tacit imbalance of power between health professionals and parents, which might also exist more subtly in other contexts. Such a hierarchy reflects the persistence of aspects of a more traditional, professional-centred model of healthcare, which preceded the now championed family-centred model (Rosenbaum et al., 1998). The persistence of this ‘traditional hierarchy’ may offer an explanation for the findings of Carlsson et al. (2016), who discovered that parents reported not wanting to speak up or to bother clinicians, even in instances where they felt the handling of their child was inappropriate.
This highlights the need for health professionals to allow space for parental contribution and to be proactive in supporting parents to develop the confidence and competence they need to feel empowered to take on the responsibility for shared decision-making. This is supported in the literature where it has been reported that parental empowerment can be facilitated by health professionals validating and respecting parents’ opinions and existing knowledge (Gates et al., 2018; Hurtubise and Carpenter, 2017; Roscigno, 2016), by listening to parents (Kruijsen-Terpstra et al., 2016) and by actively acknowledging parents as partners (Jansen et al., 2017).
The beneficial influence of such practice is highlighted in the study by Lerret et al. (2016). These researchers investigated parental perspectives about shared decision-making and emphasised the health professional attributes that were thought to facilitate parental empowerment (being knowledgeable, transparent, approachable, accessible, dependable and supportive). Indeed, it seems widely accepted that parents highly value a positive relationship with health professionals (Davies et al., 2017; Laurent et al., 2016; Rafferty et al., 2017). A relationship between parents and health professionals which facilitates a positive outcome is commonly referred to as the therapeutic relationship (Cole and McClean, 2003).
While maintaining the therapeutic relationship is very important to parents, it has been recommended that health professionals need to balance this with their professional responsibility to the child (Reeder and Morris, 2018; Rosenberg et al., 2018). It is not clear in the literature how this balance might be successfully achieved and there seems to be limited evidence exploring the link between the therapeutic relationship and the parental empowerment. In a recent study by Ryan and Quinlan (2018), it was recognised that when the therapeutic relationship was poor, parents turned to peer groups for support to become empowered to battle with professionals. While this represents empowerment of sorts, parents in the study reported that these encounters were stressful and, although not discussed in the article, it seems that the outcome was a more confrontational rather than collaborative partnership.
This is a heavily researched topic; however, there is a gap in the literature which draws together these threads of knowledge, to clearly explain the process/es by which parents become empowered to work in partnership with health professionals. Indeed, this lack of understanding has been highlighted in a previous structured review of the literature (Smith et al., 2015).
Aim
This article reports one aspect of a broader study which investigated how parents of children with long-term disabilities take up their role as key decision makers in the collaborative partnership with health professionals. It aims to explore the important themes of dis/empowerment and the influence of the therapeutic relationship. The intention is to encourage reflection and to provide practical suggestions for health professionals working in this field.
Method
This study employed a constructivist grounded theory (CGT) methodology as described by Charmaz (2014). Charmaz suggests that knowledge is co-constructed through the interaction between researcher and participants (Charmaz, 2017b) and that the meaning-making practice is situated in the social, political and historical contexts of its construction (Charmaz, 2017a). Accepting this philosophical position, it is necessary for the researcher to recognise and explicitly bring to the fore the local conditions/contexts in which their findings were constructed, including their own a priori understandings, views and expectations. This was of particular importance in this study due to the researcher’s dual role as researcher/clinician within the recruiting organisation.
Study design
A patient and public involvement (PPI) group was actively involved in the planning stage of the study as recommended by INVOLVE (2012). They provided information about the appropriateness and relevance of the research topic and the practicalities involved with recruiting participants and undertaking the research. They were also involved in defining the inclusion/exclusion criteria (see Table 1) and developing and modifying participant information sheets, consent forms and recruitment materials.
Inclusion and exclusion criteria.
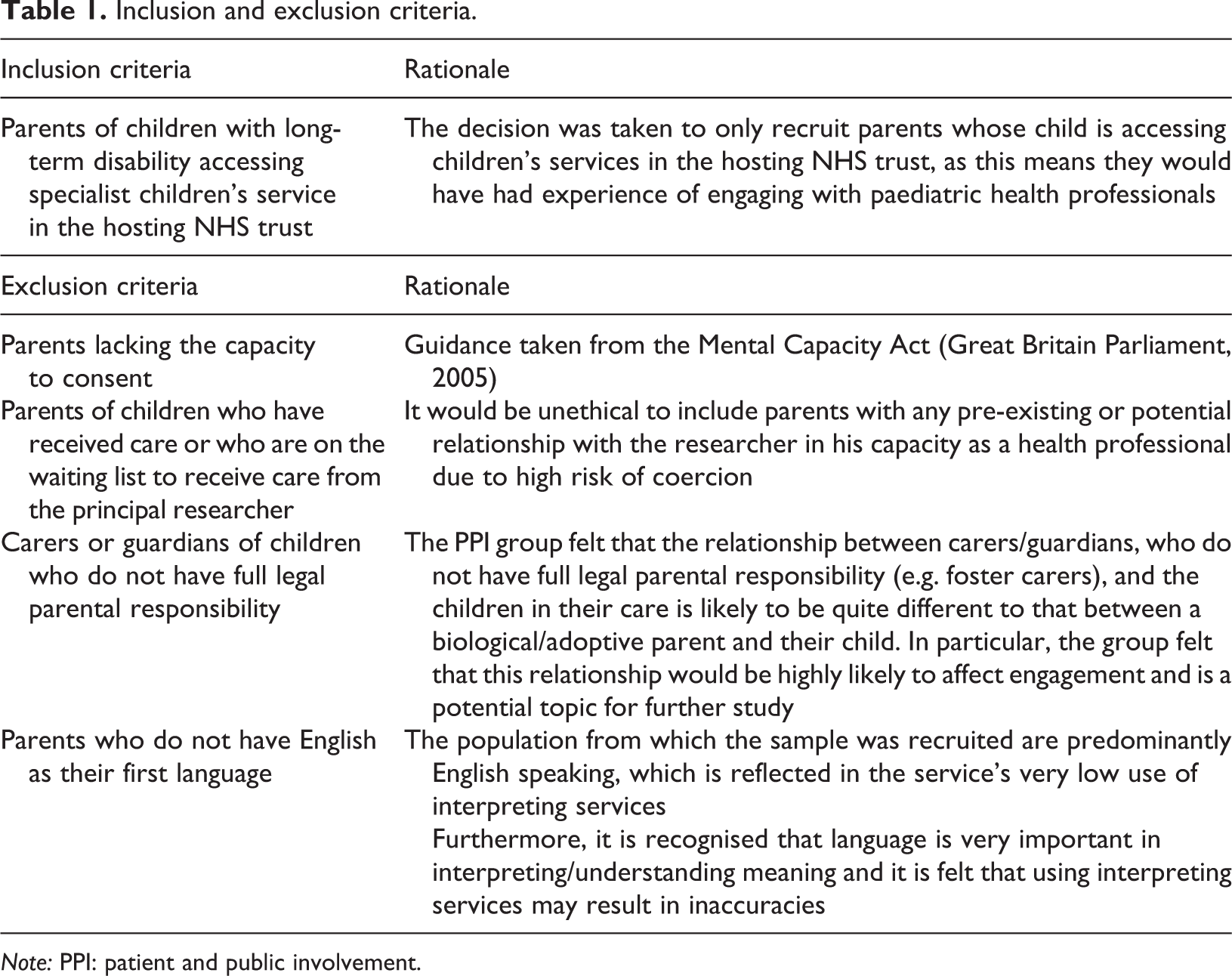
Note: PPI: patient and public involvement.
Data were collected between June 2017 and February 2018 via semi-structured interviews with 14 participants. Participants were recruited from a population of parents of children with long-term disabilities accessing children’s services from a single NHS trust (see Table 2).
Participant demographics.

Note: ASD: autistic spectrum disorder.
The recruitment process was informed by the PPI group and guided by the Research and Governance Framework (DoH, 2005) and good clinical practice guidelines (NIHR, 2016) to safeguard participants and to minimise potential for coercion. Prior to their participation in the study, time was provided to answer questions and to ensure potential participants were aware of the risks/benefits associated with their participation.
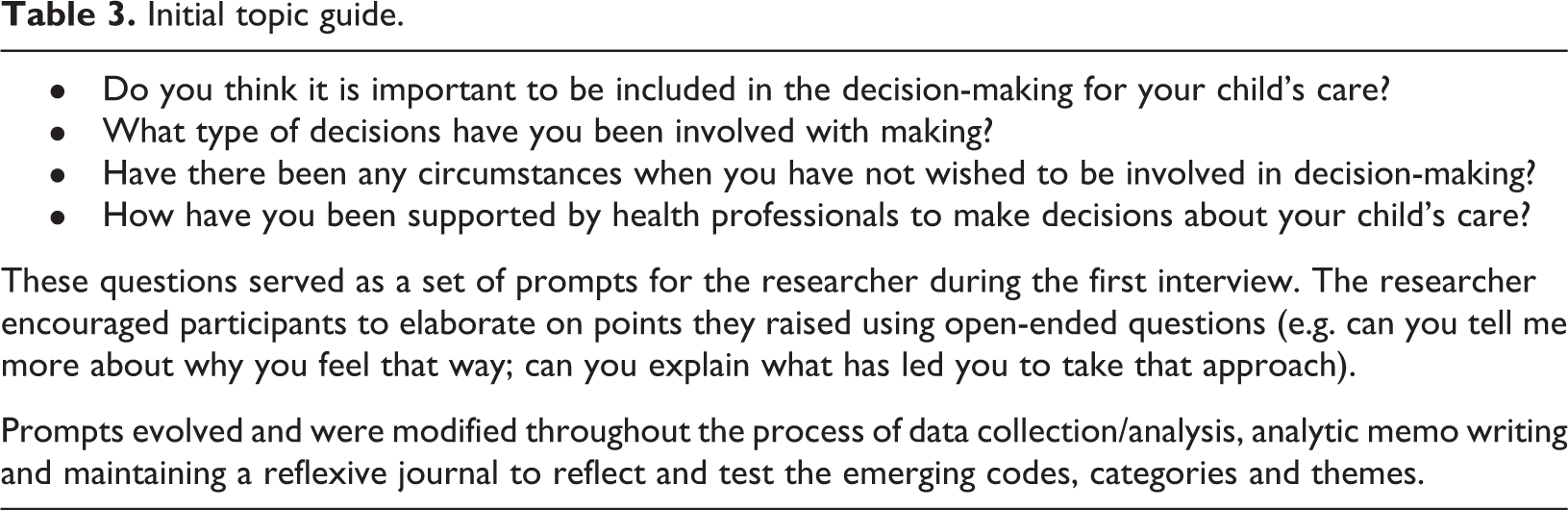
Interview 1 used a topic guide, produced with the support of the PPI group. For the subsequent interviews, the topic guide was iteratively modified, informed by emerging codes/categories and reflections from previous interviews (see Table 3). Interviews were recorded on an encrypted audio device before being transcribed (all data were managed as per NHS information governance guidelines). Throughout this cyclical process of data collection and analysis, informal analytic memos were written, allowing space for the researcher to consider emerging codes/categories and to reflexively interrogate his role in their production. This provided a transparent audit trail of data collection/analysis, which alongside a detailed reflexive journal and regular debriefings with research supervisors ensured the credibility of the findings (Charmaz, 2017a; Teusner, 2016).
Initial topic guide.
Once a main category/theory had emerged, data collection/analysis continued until no new properties could be added (Cresswell, 2013). It was felt that this point was reached after 12 interviews with 14 participants. It is recognised that this is a small sample size; however, it has been suggested that when using CGT methodology, 12 interviews can be sufficient if the population is relatively homogenous (Guest et al., 2006).
Ethical approval was granted by the external Research Ethics Committee review panel at the University of Brighton on 27 April 2017 and by the Health Research Authority on 24 May 2017.
Results
Conceptual categories are presented including excerpts from the raw data, to make more transparent the process by which they have emerged from and are therefore grounded in the data. These categories are then drawn together in a novel model which illustrates how the power im/balance and the state of the therapeutic relationship might influence how a parent takes up their position in the collaborative partnership.
The traditional hierarchy
From participants’ accounts, the predominating scenario was one where the health professional’s views and opinions were prioritised. This was viewed as a ‘traditional hierarchy’, whereby power is held by the health professional and the parent is disempowered to participate in shared decision-making. …when you are dealing with somebody you think is a professional…you kind of take their word for it…(P8) …parents are not experts in the field…we are no healthcare professionals. (P1) …when I go into an appointment I am automatically thinking that [the health professional] will think that I am exaggerating or fussing…(P8) …it hasn’t been working for 6 years…it just doesn’t seem to be registering…[but we] just keep on going basically…(P5) …you know she’s gone to uni, she has done all of her training…what do I actually know…so I let them get on with it…(P7) …the [specialist team] came along and took him and obviously took over…and yeah, [it was] really good. (P14) …if they think you have been reading things up on the internet, they get a bit annoyed…(P11) …I think people are under the illusion that as soon as you are with a doctor, that’s it they can relax, it’s in the doctor’s hands…(P16) …giving a self-help guide is not going to help matters, that is not how healthcare should be done…this is not a DIY job…I don’t think that is right at all…(P1)
In participants’ accounts, it was not always the case that disempowerment and reinforcement of the traditional hierarchy resulted in passive compliance. Some participants reported incidents where they explicitly disagreed with the view of a health professional regarding a specific intervention. …she thought she knew my son better than me…I wasn’t nasty to her…I thought I would try it your way…because you’re the professional…but I knew in my heart it would not work…(P3) …I don’t feel I could say anything…I remember thinking what do I know…because I knew [the splints] were going to be rubbish…and a waste of time, our time…and they didn’t work…(P7)
Here, despite their disagreement, both participants appeared to submit to their position in the power hierarchy and acquiesced with the view of the health professional. While these participants did again comply with the views of health professionals, they did so with more reluctance than the aforementioned situation of ‘passive compliance’. This reluctant concession appeared to contribute to a lack of true engagement with health professionals and to a feeling of dissatisfaction.
In more extreme cases of disagreement, some participants described the need to fight against the views of the health professionals. …but he wasn’t going to do that…and obviously, when it’s your child…you want to fight for whatever is going to [help]…(P9).
In these situations, it is important to note that ultimately, the power balance is still in favour of the health professionals and as such, it is possible that these parents are just labelled as difficult.
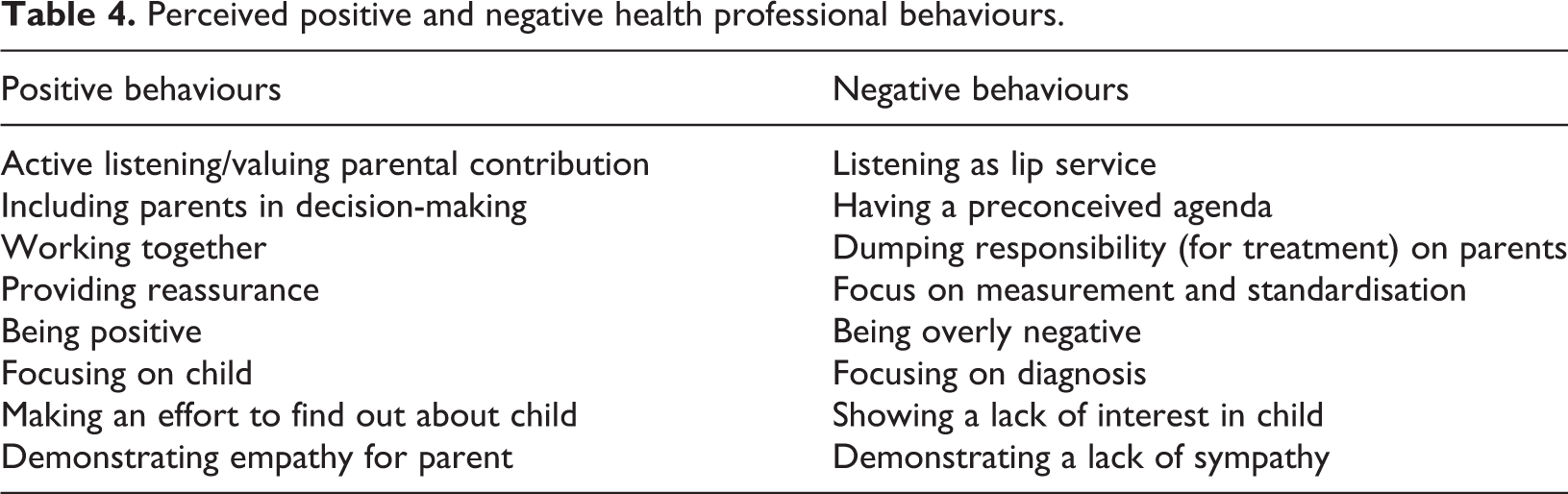
To understand why some participants were accepting of their disempowered position in the traditional hierarchy, whereas others were dissatisfied, the researcher went back to the data to look for any other actions or processes that might be influencing the situation. It emerged that the state of the therapeutic relationship seemed to have a strong de/stabilising influence on the traditional hierarchy. Re-reading the transcripts, health professional behaviours were identified that participants perceived as either positive or negative (Table 4). The positive behaviours appeared to contribute to produce a stable partnership, reinforcing the traditional hierarchy, whereas the negative behaviours destabilised the partnership.
Perceived positive and negative health professional behaviours.
Addressing the hierarchy
While the prevailing situation was for the traditional hierarchy between the parent and the health professional to persist, there were a few participants who were able to describe situations where the power imbalance had been addressed. This allowed participants to become empowered to take a more active role in the decision-making for their child.
One of the key factors in this process seemed to be the participants’ level of knowledge and understanding. P7 and P10 had both been given a diagnosis for their child, which they explained allowed them to develop an improved understanding of their child’s condition. …having a very clear diagnosis right from the start has been very helpful in terms that you know all the things to look up…I think you can become almost a mini doctor in a way…(P7) …because obviously you become an expert parent don’t you…with everything I have learned…I know what’s what…(P10)
P16, who also had a diagnosis for his child, explained that he proactively made an effort to ask lots of questions to ensure he fully comprehended what was happening and felt that he understood his child’s difficulties better than the health professionals. …I feel now that I know him better than any sort of doctor…its not to say I know everything about hydrocephalus,[or] I know everything about shunts…I don’t…but I know about his shunt, I know about his hydrocephalus and his history, because I’ve been there the whole time…(P16)
While becoming knowledgeable did appear to be very important, it did not seem to be enough for participants to become empowered. It appeared that there were other structures and processes, which also seemed necessary to successfully address the hierarchy. One important factor was the apparent need for parents to actively wrest back responsibility for decision-making from health professionals and also for health professionals to be willing to hand over that responsibility. P16’s account demonstrated that this was an atypical position for both parents and health professionals and he felt that, at times, this required a very strong intervention from the parent. …[the nurse told me]…you haven’t got to be rude, but sometimes you need to kick-off to get what you want…and I said ‘I can do that’…and then fair play to him, [the consultant] listened to me and we had the argument about what they were going to do…and he said ‘I agree with you’ and he said ‘to be honest, I apologise, but a lot of parents aren’t like you…they don’t want to know the ins and outs…all they want to know is can we sort the problem out’…(P16)
There were some occasions where participants described situations when health professionals had been more willing to hand over responsibility; however, this seemed to be limited to the carrying out of treatment programmes, with the health professional retaining responsibility for decision-making. P11 explained that she felt all the responsibility for doing the treatment plans was ‘dumped on’ her, but that this was not balanced by being given an equal voice at meetings.
Interestingly, there were some incidences where it seemed that all responsibility had been handed back to the parent, with reduced support from the health professional. P10 explained that while she was happy to take on the role as expert, she felt that this should not be taken for granted and that she needed support to make decisions, not just be left to get on with it. …I would still expect to be the expert, but I suppose sometimes you want someone to tell you, to say to you, you know, this is what is happening…otherwise you feel like you are the only one doing it and it can be a bit tough sometimes…(P10)
In this situation, P10 had become expert and empowered; however, something had destabilised her partnership with the health professional, leading to a feeling of dissatisfaction, abandonment and again the perception that there was a need to fight for what she felt was needed.
Re-reading the data and comparing this with the experiences of other participants, it seemed that it was the perception of negative health professional behaviours that produced an unstable partnership, which in turn effected how readily/successfully P10 took up her position as an expert empowered parent. The converse position is highlighted in P16’s account, where he described a stable, trusting relationship with health professionals, …We have got to know the doctors quite well…so they were quite forthcoming in letting us go home, rather than keeping him in…I’d say, ‘I’ll keep an eye on him, I’ll do the obs[ervations]…if I need you I’ll ring you, or I’ll bring him back’…and that works…If they trust you it does work…(P16)
This example demonstrates a situation where P16 had been supported to become an expert empowered parent, leading to a reduced reliance on health professionals. P16 was able to describe other circumstances where he felt that his actions as an expert empowered parent lead to reduced requirement for specialist support or interventions. …it was more to do with his epilepsy [than a blocked shunt]…I said, ‘I don’t want you to send him for a CT scan and that operation, just to put your mind at rest’…and he agreed…he said ‘well actually, you know your child’…(P16)
These findings have been drawn together and are presented here in a novel model (Figure 1), which is discussed below.

The influence of the therapeutic relationship on dis/empowered parents’ position in the collaborative partnership.
Discussion
Existing literature suggests that parents need support from health professionals to take up their role as key decision makers (Gates et al., 2018; Hurtubise and Carpenter, 2017; Roscigno, 2016); however, there is evidence to suggest that this represents a significant challenge for both health professionals (Shields, 2017; Watts et al., 2014) and parents (Hutton and King, 2017; Smith et al., 2015). This study supports that the prevailing situation is for the persistence of a traditional hierarchy, where the locus of power and control lies with the health professional and where parents are disempowered (Coyne et al., 2016; Shields, 2017; Uniacke et al., 2018). The findings of this study advance the understanding of this complex situation, identifying a number of processes and behaviours that appear to either reinforce or address this hierarchy.
Reinforcing the traditional hierarchy
It has been recognised that, despite being enthusiastic about their involvement in decision-making (Lerret et al., 2016; Mak et al., 2017; Rosati et al., 2017), parents can feel frightened and overwhelmed by the prospect of the associated increased responsibility (Hutton and King, 2017; Smith et al., 2015). The findings of this study develop this idea by suggesting that, in the absence of appropriate support, parents are likely to take up a position of passive compliance, devaluing their own contribution and increasing their reliance on health professionals. Furthermore, this scenario might be reinforced by health professionals who are perceived to actively retain responsibility for decision-making. It is possible that the reluctance of health professionals to hand back responsibility is underpinned by the perceived threat of a loss of control and power, associated with more family-centred approaches (Espe-Sherwindt, 2008; Shields, 2017; Watts et al., 2014). This is further complicated by the tension faced by health professionals who will ultimately be held legally accountable for any adverse effects of ‘shared’ decision-making on the well-being of the child (Batalden et al., 2016).
Despite growing evidence that health professionals can no longer control the content/flow of health-related information (Reeder and Morris, 2016), and the extent to which parents are reported to search for information online (Edwards et al., 2018; Nicholl et al., 2017), the findings of this study support the suggestion that health professionals are continuing to discourage parents from this practice (Gage and Panagakis, 2012; Kirk and Milnes, 2016). Interestingly, this study also found that parents typically ignore this advice and continue to look for information online; however, they do this more covertly/secretively, so as not to ‘annoy’ or undermine the health professionals. It is suggested that if health professionals continue to delegitimise parents’ efforts to source information independently, it might have the effect of further devaluing parental contribution and is very likely to create a barrier to useful open discussion.
It is suggested that health professionals should be cognisant of the impact of these ‘hierarchy reinforcing’ behaviours, in particular the extent to which they might influence their own clinical practice. The following section develops this idea by identifying and discussing the processes and actions that proactively redress the power imbalance, empowering parents to take a more active role in decision-making.
Addressing the traditional hierarchy
It has been recognised that increasing parental knowledge is a key component of their becoming empowered (Kruijsen-Terpstra et al., 2016); however, it is suggested that it is too simplistic to equate the development of knowledge with empowerment. The findings of this study suggest that in addition to supporting parents’ development of understanding, health professionals need to make more effort to address the persisting power imbalance.
Initiatives already exist that are designed to draw parents into a more unified group with health professionals (e.g. Team around the child; Multidisciplinary Team Meetings), and this remains high on the national agenda (NHS England, 2019). Despite this, current literature has identified that health professionals need to be more prepared to acknowledge parents as partners (Jansen et al., 2017). The findings of this study suggest that this action cannot be limited to what might be perceived as the ‘dumping’ of responsibility for additional caregiving, rather that health professionals should foster genuine collaboration with parents to form a decision-making partnership. Similarly, earlier work has also recommended that health professionals should be ready to validate parents’ efforts to access information independently (Gates et al., 2018; Hurtubise and Carpenter, 2017; Roscigno, 2016) and even take action to encourage this practice (Reeder and Morris, 2016). The findings of this study suggest that health professionals need to ensure this practice moves beyond lip service and be ready to engage in frank and authentic discussion, with a willingness to challenge their own preconceived views/assumptions/dogmas and concede the intellectual higher ground.
It is anticipated that the adoption of these participatory behaviours will go a long way to shift the locus of power/control and represent the type of additional support that parents require to feel empowered to take an active role in decision-making.
The influence of therapeutic relationship
Where the participatory practices described are suggested to support parents’ becoming empowered, relational practices appear to either stabilise or destabilise the health professional/parent partnership.
The benefits of a positively perceived therapeutic relationship have been well-documented (Fordham et al., 2012; Laurent et al., 2016; Reeder and Morris, 2018); however, the findings of this study suggest that, in certain circumstances, positively perceived relational behaviours might in fact act as a barrier to parents becoming empowered. It appears that positively perceived behaviours have a stabilising influence on the health professional/parent partnership, which typically is the traditional hierarchy. In these situations, parents might be superficially satisfied with the service they are receiving; however, it is suggested that this stabilises passive compliance, increasing their reliance on the health professional. This adds support to the model presented by Reeder and Morris (2018), which warns health professionals of prioritising the therapeutic relationship and reinforcing the idea that it is not enough just to be nice (Espe-Sherwindt, 2008).
In contrast, negatively perceived relational behaviours seem to destabilise the partnership, leading parents to feel dissatisfied and to push back (fight) against health professional opinion, regardless of their level of empowerment. For parents in a disempowered position, this seems to manifest as a reluctant acquiescence with health professionals. It is reasonable to argue that in these situations, parents are not truly engaged and are not signed up to the decisions being made, which means that any intervention based on these decisions is likely to fail. Interestingly, even when parents do feel empowered to make decisions about the care and treatment of their child, negatively perceived relational behaviours can undermine their confidence, leading them to feel abandoned and unsupported. This provides additional explanation to the findings of Carlsson et al. (2016), who described some parents reporting feeling empowered but alone.
Unfortunately, it seems that it is a rare occasion when the power imbalance is addressed, when parents feel empowered and when they also perceive positive relational behaviours. It is suggested that these situations represent true parental empowerment and a ‘truly’ therapeutic relationship, where a stable partnership offers parents reassurance and support to take on the responsibility for decision-making. Furthermore, this is likely to lead to improved parental satisfaction and reduced reliance on health professionals, which has potential economic benefits for the NHS.
Implications for practice/further research
It is recommended that paediatric health professionals should consider the following: Increasing awareness of behaviours and practices that might reinforce the traditional health professional/parent hierarchy and create barriers to parental empowerment (e.g. taking over responsibility for decision-making/delegitimising parental contribution/focussing on standardised measurements). Increasing awareness that positively perceived health professional behaviours have a stabilising influence on the parent/health professional partnership, which is typically the traditional hierarchy. The development and evaluation of practical initiatives to promote parental empowerment. This might include updating/informing staff training programmes or developing interventions, which prioritise collaboration and foster a truly therapeutic relationship between health professionals and parents.
Limitations
It is acknowledged that the sample size of 14 was low for a CGT methodology. While literature recommends that with a sample size of 12, it is possible to reach theoretical saturation (Guest et al., 2006), it is suggested that this number might not command respect of the reader (Charmaz, 2014).
It is also recognised that data collection was limited to semi-structured interviews and did not include any observations. A justifiable criticism of this is that the researcher may have been more focussed on lived experiences of participants, rather than on social processes (Benoliel, 1996); however, it is hoped that this was addressed through the iterative process of reflexivity.
It is accepted that that the same findings/understandings would not be constructed by another researcher with different life experience, which raises important questions about the transferability of the findings. As the methodology employed moves beyond interpretation and description to develop substantive theory, it is suggested that its application and resonance might extend beyond the specific participants and context of this study.
Conclusions
This article presents a new explanation of the structures and processes which influence how a parent of a child with long-term disabilities is either empowered or disempowered and how this affects their engagement in the collaborative partnership. It is suggested that by addressing the traditional hierarchy within healthcare, health professionals might facilitate the development of a ‘truly’ therapeutic relationship, which can help promote parental empowerment.
Footnotes
Acknowledgements
This study was conducted as part fulfilment of an NIHR-funded Masters of Research Degree. The authors would like to acknowledge the support offered by the hosting healthcare organisation and the participants involved. The organisation has not been named to protect participant confidentiality.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.