
Abstract
Efforts to improve the quality of care for children have focused on the patient-centered medical home (PCMH), defined by the National Committee for Quality Assurance (NCQA). Little research has focused on caregivers’ role in choosing physicians for children. This study aims to determine whether healthy caregiving behaviors and specific behaviors are associated with children’s receipt of PCMH care. Using data from the 2016–2017 National Survey of Children’s Health, which includes information on child-rearing behaviors, we estimated logistic regressions, controlling for children’s and caregivers’ characteristics, to quantify possible associations. We found that each additional healthy child-rearing practice followed increased a child’s chance of receiving PCMH care by 4.5% (p < 0.001). Being breastfed (children aged 0–5 years), sharing ideas with their caregiver (children aged 6–17 years), their caregiver ensuring homework is finished (children aged 6–17 years), and having TV time monitored (all ages), each increased the likelihood of PCMH use. These findings show that caregiving behavior is independently associated with locus of care. Future research is warranted as educating caregivers about healthy child-rearing may lead them to seek higher quality care for their children. Also, evaluating the effect of behaviors on health outcomes associated with PCMH would be valuable.
Introduction
The patient-centered medical home (PCMH) is a primary care practice model designed to provide accessible, family-centered comprehensive and coordinated care, all characteristics identified as fundamental to high-quality care. Developed in 1967, the model is intended to improve children’s health status and potentially reduce their care costs (National Committee for Quality Assurance, 2019). It was endorsed by several physician organizations in 2007 (e.g., American Academy of Family Physicians, et al. (2007)), and the following year, the National Committee for Quality Assurance (NCQA) published PCMH practice standards (National Committee for Quality Assurance, 2008).
The Affordable Care Act of 2010 promoted the PCMH model’s adoption (Board on Population Health and Public Health Practice, et al. (2015)). Insurers across the United States, including Medicaid agencies, have also embraced the model. Many are providing additional reimbursement, such as case management fees, to providers meeting NCQA standards for the PCMH (Friedberg et al., 2014; Stack and Kier, 2014).
Researchers have defined PCMH practices as those meeting NCQA standards, specifically providing family-centered comprehensive and coordinated care. Most rely on caregivers’ reports of practice characteristics found in national datasets, including the National Survey of Children’s Health (NSCH), to define and identify a PCMH (Rebecca and Malouin, 2010). Recent literature suggests that caregivers do perceive the presence of NCQA PCMH elements, especially in specialty care (Vander Schaaf et al., 2017). Using these designations, evaluations of the PCMH have focused on their ability to change healthcare utilization, reduce costs, and increase healthcare quality with mixed results (Aysola et al., 2013; Deborah Peikes et al., 2012; Golnik et al., 2012; Long et al., 2012; Mosquera et al., 2014; Quattrin et al., 2014; Takach, 2011).
The literature has also identified factors predicting which children are most likely to receive care from a PCMH. Consistently, being a member of a racial or ethnic minority, such as Black/African–American or Hispanic (McCarter et al., 2011; Zickafoose and Davis, 2013); having Medicaid as an insurer (Conrey et al., 2013); living in a low-income household (McCarter et al., 2011); living in non–English-speaking families (DeCamp et al., 2011); and having behavioral/mental health conditions (Knapp et al., 2013) or possible access barriers reduced the likelihood of receiving care from the PCMH (Aysola et al., 2011; Conrey et al., 2013; Romaire et al., 2012a; Singh et al., 2009). Increased perceived need, higher household incomes, and rates of employment increased it (Case and Paxson, 2002; Mukiira and Ibisomi, 2015; Stevens et al., 2010).
Research on caregivers’ decisions to seek care for their children has been frequently investigated. Higher rates of maternal education and healthcare use are associated with increased frequency of children’s use; while increased parental stress, including household instability (Ma et al., 2008; Mukiira and Ibisomi, 2015), higher levels of psychopathology, and lower levels of social support are associated with lower healthcare use (Pratley, 2016).
While caregiver characteristics, such as education and caregiver health status, have been found to affect rates of utilization, locus of care, and receipt of PCMH care, limited research has explored the possible relationship between caregiving behaviors and choice of a healthcare provider for a child. On the other hand, there is a large body of literature suggesting that caregiving practices directly affect children’s health. Breastfeeding is positively associated with infant health (American Academy of Pediatrics, 2012), and caregiver propensity to monitor children’s diets and promote regular physical activities help reduce obesity (Maitland et al., 2013). Creating a smoke-free environment reduces asthma exacerbations (Sato et al., 2013; Sun and Sundell, 2011). Decreasing TV time and shared reading have a positive impact on children’s health (Bar-on, 2000; Lagerberg and Magnusson, 2013).
Caregiving practices may also affect children’s health if they influence where and when a child receives health care. Scandinavian countries, for example, include parental caregiving education on smoking (Riley et al., 1993), breastfeeding, and interactions with children, as part of postnatal care at the children’s health center. An additional aim of these programs is to promote children’s health through appropriate healthcare utilization (Wells and Sarkadi, 2012). Mental health providers are investigating parental education programs, including caregiving practices, to encourage initiation and use of services for children with mental health issues (Ingoldsby, 2010; Olin et al., 2010). These programs suggest that investigating caregiving behaviors and their possible relation to locus of care is warranted. Also, as caregiving behaviors vary across income groups and caregiver educational levels, it is important to investigate them in a conceptual framework that controls for all these caregiver characteristics.
Prior work using the 2011–2012 NSCH data found that living in a home where healthy child-rearing practices are followed significantly increased the likelihood of low-income children receiving care from a PCMH, even when controlling for caregivers’ level of education, health status, and household income (Hu et al., 2017).
We build on this work using data from the 2016–2017 NSCH, which identifies PCMH physician practices and caregiving behaviors. We expand the analysis to include all children to investigate more fully possible household income and educational effects. We examine whether the number of healthy caregiving behaviors present in the household, along with that of specific behaviors, is associated with a child receiving care from a PCMH.
We posit that a caregiver determines or chooses a child’s locus of care and draw on the Anderson behavioral model of utilization (Babitsch et al., 2012), used by many researchers (Anderson et al., 2019; Riley et al., 1993), which describes healthcare use as a function of predisposing factors, enabling factors, and need to predict children’s source of care. Predisposing factors are characteristics intrinsic to the patient, such as age. Perceived need is a subjective assessment of need, such as the degree of illness, and enabling factors are resources that encourage/discourage healthcare use, such as insurance status.
Aim
The aim of this study is to determine whether there is an association between a child living in a home where healthy child-rearing practices are followed and receiving his/her health care from a patient-centered medical home (PCMH) and, secondarily, if specific behaviors affect this likelihood.
Methods
Sample
We used data from the 2016–2017 NSCH (Child and Adolescent Health Measurement Initiative, 2019) for our analysis. The survey population (N = 71,811) is weighted for analytic purposes to represent the population of noninstitutionalized children, aged 0–17 years, nationally and in each state. We excluded children who did not use any medical services during the year (n = 8,149, 11.3%) or had missing values on the variables included in our analysis: PCMH use (n = 1,088, 1.5%), child-rearing behaviors (n = 2,334, 3.3%), and other covariates (e.g., moving home, n = 1,645, 2.3%) (see supplemental Table 1 for further details). The final analytic sample included 55,957 children.
Measures
Our dependent variable was caregivers’ report on PCMH use. The NSCH asked caregivers questions about the quality of children’s health care to identify which practices meet NCQA criteria. Caregivers reported on 17 items which were used to identify the five components of the NCQA’s definition of the PCMH: (1) having a personal doctor or nurse, (2) having a usual source for sick and well care, (3) receiving family-centered care, (4) having no problems getting needed referrals, and (5) receiving effective care coordination when needed. We defined a PCMH practice as one meeting all the five criteria, which we refer to as high quality.
Our primary independent variable was caregivers’ child-rearing practices. We created a five-unit scale based on caregiving-related questions which differed by age-group. Three indicators were common in both age groups and asked whether the caregiver (1) smokes inside the household, (2) facilitates the family sharing meals more than 4–6 days per week, and (3) monitors TV time (no more than 1 hour per day). Two age-specific indicators for children aged 0–5 years were whether the caregiver (4) ever breastfed the child and (5) reads or sings to the child every day. For those aged 6–17 years, age-specific indicators were whether the caregiver (6) shares ideas with the child and (7) ensures that the child finishes required homework.
We included covariates in the model based on our conceptual framework. Predisposing factors were child’s race, caregiver’s age, and caregiver’s physical and mental health status. Enabling factors included highest level of education within the household, child’s insurance status, primary language, household income level, family structure in terms of a two-parent family or not, number of children, household stability in terms of number of times moving, and proxies for barriers to access (Agiro et al., 2012), living in rundown housing, and feeling safe in the neighborhood. Need-based factors were child’s age, biological sex, physical health status, and presence of special health care needs.
Statistical analysis
We described all variable values for the full sample and stratified by age groups, children aged 0–5 years and children aged 6–17 years. Chi-square tests were used to compare the characteristics between two age-groups. Multivariable logistic regression with state fixed effects was first used to estimate the association between the total number of healthy child-rearing practices present in the home and the receipt of care from a PCMH. We reported marginal effects for the independent variable, total count, to quantify the effect of a unit increase in the number of healthy caregiving practices followed in the household and the likelihood of receipt of PCMH care.
For the secondary analysis, with specific behaviors as independent variables, we used a similar approach and estimated separate models for children aged 0–5 years and 6–17 years, given differences in the composition of caregiving behaviors. We also reported marginal effects for the analysis of individual caregiving behaviors which showed the impact on the likelihood of PCMH use from engaging in each behavior.
We included state fixed effects to account for the clustering of households and conducted variance inflation factor (VIF) analysis to test for multicollinearity among the independent variables (O’bslbrien, 2007). All independent variables had a VIF < 10 and thus exhibited limited multicollinearity. None were excluded from the model. Data were analyzed using Stata/SE 15.1 (StataCorp, 2017), and SVY commands were used to account for the complex survey design. Type I error was set at 0.05 to determine statistical significance. This study was categorized as nonhuman subject research by the Emory Institutional Review Board.
Results
Description of variables by Andersen model factors (NSCH, 2016–2017, weighted).
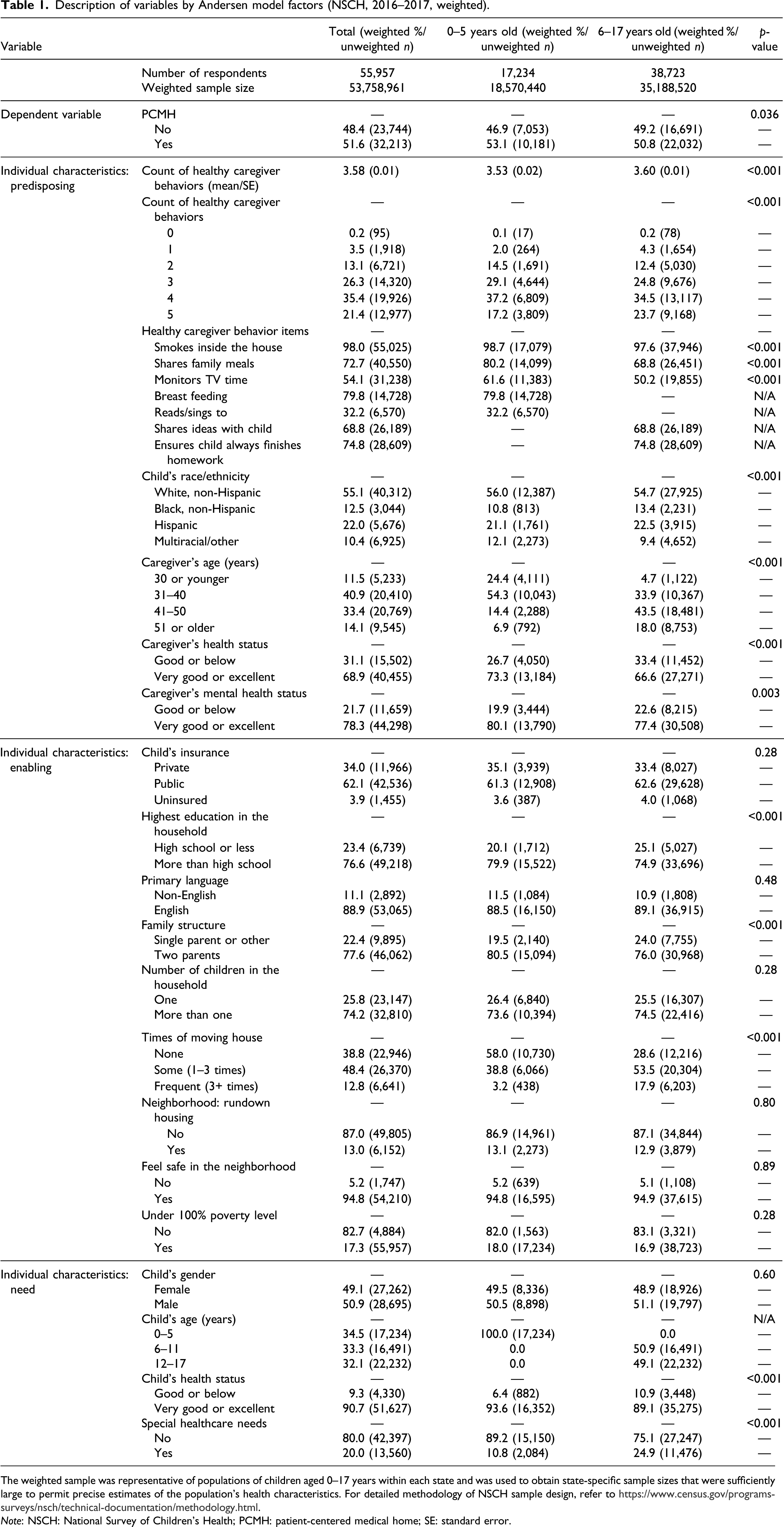
The weighted sample was representative of populations of children aged 0–17 years within each state and was used to obtain state-specific sample sizes that were sufficiently large to permit precise estimates of the population’s health characteristics. For detailed methodology of NSCH sample design, refer to https://www.census.gov/programs-surveys/nsch/technical-documentation/methodology.html.
Note: NSCH: National Survey of Children’s Health; PCMH: patient-centered medical home; SE: standard error.
In regard to the caregiver, 68.9% (n = 40,455) and 78.3% (n = 44,298) reported very good or excellent physical health and mental health, respectively, with children in the lower age-group having significantly greater percentages than older children (p < 0.001 and p = 0.003 respectively). More caregivers, 18.0% (n = 8,753), were aged 51+ years for older children, while 6.9% (n = 792) were aged 51+ years for younger children (p < 0.001).
Roughly, a third of children were covered by Medicaid/CHIP. Over 75% (n = 49,218) lived in households where caregivers had more than a high school education, 77.6% (n = 46,062) in households where two parents were present, 74.2% (n = 32,810) with more than one child in the household, and 88.9% (n = 53,065) spoke English as their primary language; 17.3% (n = 55,957) had a household income of less than 100% federal poverty level. Over 12% (n = 6,641) of children moved more than three times since they were born, with significantly more older children moving than younger children (n = 6,203, 17.9% vs n = 438, 3.2%.p < 0.001). Regarding housing, 13.0% (n = 6,152) reported living in rundown housing, while 94.8% (n = 54,210) felt safe in their neighborhood.
The mean age of the children was 8.3 years (SE = 0.05); slightly over half were male (n = 28,695, 50.9%) and white (n = 40,312, 55.1%). The vast majority (n = 51,627, 90.7%) of the children had health status ratings of very good or excellent, although older groups had significantly more in the good or below than younger groups (p < 0.001). One-fifth had special needs with significantly more children in the older, 24.9% (n = 11,476), than 10.8% (n = 2,084) in the younger group.
Regression results predicting the effect of number of healthy caregiver behaviors on the likelihood of patient-centered medical home use (National Survey of Children’s Health, 2016–2017, weighted).
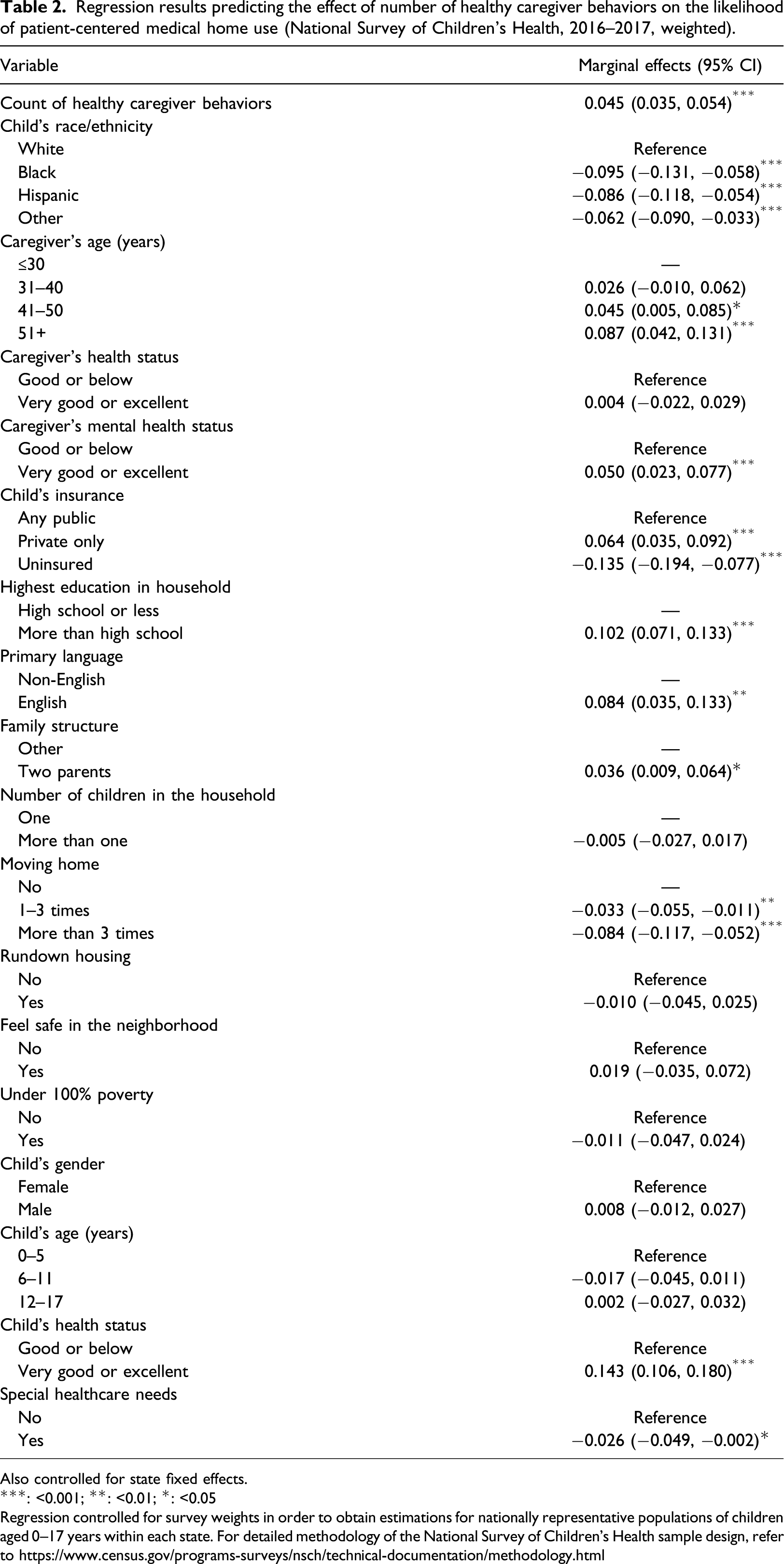
Also controlled for state fixed effects.
***: <0.001; **: <0.01; *: <0.05
Regression controlled for survey weights in order to obtain estimations for nationally representative populations of children aged 0–17 years within each state. For detailed methodology of the National Survey of Children’s Health sample design, refer to https://www.census.gov/programs-surveys/nsch/technical-documentation/methodology.html
A caregiver having relatively better mental health status, being aged 51+ years, and English speaking increased the likelihood of PCMH use by 5% (95% CI: 0.023, 0.077), 8.7% (95% CI: 0.042, 0.131), and 8.4% (95% CI: 0.035, 0.133), respectively. Living in a household with two parents and having private insurance all increased the likelihood of PCMH use (p < 0.05). Other significant factors for receipt of PCMH care were the child having very good/excellent health, which increased it by 14.3% (95% CI: 0.106, 0.180); being black, which decreased it by 9.5% (95% CI: −0.131, −0.058); having special health care needs, which decreased it by 2.6% (95% CI: −0.049, −0.002); and moving three or more times, which decreased it by 8.4% (95% CI: −0.117, −0.052).
Notably, uninsured children were 13.5% (95% CI: −0.194, −0.077) less likely than those with public insurance to receive PCMH care, while those with private insurance were 6.4% (95% CI: 0.035, 0.092) more likely.
We similarly estimated the marginal effects of individual child-rearing behaviors on receipt of PCMH care, stratified by younger (0–5 years old) and older (6–17 years old) age-groups, controlling for the same set of covariates (supplemental Table 2). In the younger group, monitoring a child’s TV time and the child being breastfed before were positively associated with PCMH use by 4.6% (95% CI: 0.011, 0.082) and 5.2% (95% CI: 0.002, 0.101), respectively. All other covariates exhibited similar direction and effect size as in the full sample model, with the exception that caregiver age, caregiver mental health status, and living in a two-parent household were no longer significant.
In the older age-group, children having caregivers who monitored their TV time, 5.7% (95% CI: 0.033, 0.081); shared ideas with their children, 10.1% (95% CI: 0.074, 0.128); and ensured that they finished their homework, 4.8% (95% CI: 0.021, 0.075), increased the likelihood of the child receiving PCMH care. All other covariates showed similar directions and effect sizes compared to the full model except that living in a two-parent household and the child having special needs were not significant.
Discussion
We found a significant, positive association between a child receiving his/her health care from a PCMH and a child living in a home with healthy child-rearing practices. In our NSCH study sample, just over half of children received care from a PCMH. More children aged 6–17 years, 23.7% (n = 9,168), lived in homes engaging in all five healthy caregiving behaviors, than, 17.2% (n = 3,809), for those aged 0–5 years. Engaging in each additional healthy caregiving behavior increased the likelihood of the child receiving care from a PCMH by 4.5%, meaning that if a caregiver adopted two additional behaviors, the percent increase would rise to 9%.
The individual behavior that had the greatest effect on the likelihood of PCMH use for the older age-group was caregivers sharing ideas with them. Interactions of this type have been associated with improvements in children’s emotional, mental, and behavioral development. Child health centers in Sweden promote conversational interactions between parents and children as a way to improve physical health and promote appropriate health care utilization (Lagerberg and Magnusson, 2013). For younger children, breastfeeding had the largest effect, which was practiced by 79.8% (n = 14,728) of caregivers.
Our covariate results are congruent with other studies which indicate that children who are privately insured; white; whose caregivers had relatively good mental health; and who live in two-parent, stable, and more educated households are more likely to have the PCMH as a source of care (Conrey et al., 2013; Hu et al., 2017; Knapp et al., 2013; McCarter et al., 2011; Zickafoose and Davis, 2013). Some of these factors, such as household education, child’s insurance status, and child’s health status, had sizable effects on PCMH use (i.e., with over 10% increase in likelihood). Education level may correlate with knowledge of the healthcare system, possibly facilitating access to PCMH practices or the ability to identify and report these practices. It may also reflect an income effect not detected by the income specification in our model. The effect of insurance suggests an ongoing access constraint for some children. Although only 3.9% (n = 1,455) of children were uninsured, they were 13.5% less likely to receive care from a PCMH, relative to a child insured by Medicaid/CHIP. Being privately insured increased the relative likelihood of PCMH use by 6.4%, compared to Medicaid/CHIP beneficiaries.
Medicaid agencies have been promoting the PCMH model, with an estimated 46 states implementing it in some form. However, our data did not allow us to link the child’s residence with a practice location. Consistent with the existing literature using this dataset, we attempted to capture access constraints through reported characteristics of the neighborhood in which the child lived under the hypothesis that practices may be less likely to locate in neighborhoods perceived as less desirable by the caregivers (Aysola et al., 2011). Further exploration of access through linking child’s residence and PCMH availability is an important area for future research (Cunningham, 2015).
The covariate with the greatest effect size is children’s health status, with those in relatively better health being more likely to receive PCMH care. The results may reflect endogeneity, meaning that PCMH care positively affects children’s health over time. As our data are cross-sectional and not longitudinal, we do not know how long a child has been seen by a PCMH practicer or the same provider within a practice and, therefore, cannot address this issue. Also, many children experience discontinuities in care, not just the uninsured. Providers are willing to accept Medicaid move in and out of the program, and privately insured children can change networks where providers available change as a function of their parents’ insurance arrangements.
The specification of our income variable was general. We used income at or below 100% of the federal poverty line or above. While it was insignificant, more granular specifications may identify an income effect, such that children living in relatively wealthier households are likely to have relatively better health and greater access to a PCMH.
Reverse causality is also worth considering in relation to the association. One could argue that receiving care from a PCMH may lead to healthier child-rearing practices among caregivers. The literature to date suggests this is unlikely. Pediatric visits are time-limited; providers have minimal time to devote to caregiving behaviors and often face challenges managing children’s health issues during the visit (Hill et al., 2019). Further, changing adult behavior is difficult as discussed extensively in the stages of change literature (Prochaska and DiClemente, 1983). For example, studies related to diet show that even intensive, sustained interventions aimed at adults and children produce very limited effects (Quattrin et al., 2014).
Implications
These findings have important implications for caregiving education programs, prenatal and beyond. Practicing healthy child-rearing behaviors may provide additional, indirect health benefits as they affect where a child receives care. Caregiving education programs, prenatal and beyond, should be promoted, and those focused on older children should include an emphasis on interpersonal interactions. These programs should also be expanded to include information about the healthcare system, care quality, and concepts of care coordination to build on the association between caregiving behaviors and locus of care. Such efforts could help change expectations about care for their children and potentially lead them to request higher quality services.
The results also have implications for evaluations of the effects of PCMH care on children’s health outcomes. Healthy child-rearing practices positively affect children’s health. Children receiving care from a PCMH may exhibit better health status, in part, as a product of high-quality caregiving. Evaluations examining the effects of PCMH care on children’s health outcomes, which do not include caregiver behaviors, may be subject to omitted variable bias (Fairchild and MacKinnon, 2009).
These findings also underscore that certain unmodifiable factors continue to act as constraints on a child receiving PCMH care. Efforts should be focused on those which can be modified and addressed, such as targeted enrollment of minority and non-English–speaking children; continued efforts to ensure that more children are insured and PCMH practices are more widely available.
Limitations
Our study has several limitations. First, there may be self-report bias in survey data. The NSCH uses caregiver-reported quality indicators to determine PCMH use, not documented enrollment in an NCQA-designated PCMH. Certain minority groups or non-English speakers may be unfamiliar with the terms, such as care coordination, and thus less likely to report them.
We identify high-quality physician practices using NCQA guidelines. Physician practice quality may not be fully represented by NCQA metrics. Also, we assessed a limited number of caregiving behaviors; others may be relevant but are not included here.
Caregiver behaviors are also self-reported and may be biased upward. Overall, 98% of respondents reported not smoking in the household, a considerably higher percentage than found in national reports (U.S. Department of Health and Human Services, 2007). Our analysis may also be affected by missing data and data specifications. Approximately 10.7% (n = 7,705) of the sample was excluded because of missing values, which may not be random. We examined the distribution of PCMH by the count of healthy caregiver behaviors for each variable with missing values and did not observe remarkable differences between children with missing values and those without missing values for that variable. Access to care is measured through proxies which may not fully capture or underestimate this problem.
Conclusions
Our results show a significant association between the number of high-quality child-rearing behaviors present in the home and children’s receipt of care in a PCMH. Parental education programs should include child-rearing practices in their curriculum as they may indirectly benefit children’s health through affecting parents’ choice of physicians. Further research is warranted into child-rearing practices, including other potentially important behaviors, and locus of care for children and eliminating constraints that some children may face in accessing PCMH care.
Supplemental Material
sj-pdf-1-chc-10.1177_1367493520933458 – Association of healthy child-rearing practices and children’s receipt of care in patient-centered medical homes
Supplemental Material, sj-pdf-1-chc-10.1177_1367493520933458 Association of healthy child-rearing practices and children’s receipt of care in patient-centered medical homes by Victoria L Phillips and Xin Hu in Journal of Child Health Care
Supplemental Material
sj-pdf-2-chc-10.1177_1367493520933458 – Association of healthy child-rearing practices and children’s receipt of care in patient-centered medical homes
Supplemental Material, sj-pdf-2-chc-10.1177_1367493520933458 Association of healthy child-rearing practices and children’s receipt of care in patient-centered medical homes by Victoria L Phillips and Xin Hu in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.