
Abstract
The purpose of this study was to develop a scale to measure high-risk neonatal infection control competency among nurses in neonatal intensive care units (NICUs). The study participants included 251 nurses working in NICUs at seven hospitals in South Korea. The scale was designed to measure high-risk neonatal infection control competency in terms of performance (HirNICCS_P) and knowledge (HirNICCS_K), which were addressed by 42 and 54 items, respectively, and was initially subjected to content validity testing by a panel of experts in neonatal nursing. The items were divided into five factors: (1) basic care, (2) skin care, (3) feeding management, (4) medication and invasive procedures, and (5) environment management. After participant completion of the scale, construct validity was examined using exploratory and confirmatory factor analyses, and internal reliability tests were also performed. The total variance of validity was 53.7% for HirNICCS_P, and the Cronbach’s alpha values for reliability were .95 for HirNICCS_P and .67 for HirNICCS_K based on a Kuder–Richardson-20 test. We concluded that this scale can be used to assess the performance and knowledge with regard to infection control competency among neonatal nurses and that its application can support strengthening of infection control education for nurses who score low on performance and knowledge competency.
Introduction
According to the South Korean national statistical data for 2017, the country’s total fertility rate stood at 1.05 in 2017, down from 1.25 in 2007. During the same 10-year period, the percentage of low–birth weight newborns increased by 1.47 times (Statistical Office, 2017). Although in recent years the survival rate of high-risk neonates has increased with advances in care in neonatal intensive care units (NICUs), healthcare providers face ongoing challenges in providing care for vulnerable infants.
High-risk neonates undergo various invasive procedures to support their survival, and their hospital stays tend to be prolonged. Furthermore, their infection rate ranges from approximately 20%–33%, which is substantially higher than that among normal neonates (Kim and Park, 2008). Healthcare-associated infections (HAIs) consistently occur due to frequent therapeutic interventions performed on neonates with an immature immune system (Adams-Chapman and Stoll, 2005; Huskins and Golmann, 2009). Infection in one site among neonates is readily spread throughout the body, resulting in a high incidence of sepsis compared to that in children or adults. Particularly, very low–birth weight neonates (<1500 g) and extremely low–birth weight neonates (<1000 g) have immature nervous and endothelial cells surrounding the vascular, digestive, and respiratory tissues, and thus, all their organs are easily injured (Guerina, 1998). Recently, that four newborns died from infection, which resulted from an intravenous injection at a neonatal unit of a university hospital in Korea, has brought attention to the intensive care unit (ICU) environment, highlighting the importance of systematic ICU infection control (Kim, 2018).
Appropriate infection control procedures undertaken by nurses are crucial to lower morbidity and mortality from HAIs that have a high risk in the NICU (Haleyn et al., 1980). It has been reported that approximately 30–35% of HAIs are preventable with aggressive infection control (Haleyn et al., 1980) and that adherence to infection control protocol rises with increasing knowledge (Yoo et al., 2012). For these reasons, developing an infection control competency scale, assessing NICU nurses’ knowledge and competency regarding infection control, is important to help ensure more effective infection control and prevention. Nurses are expected to provide safe and effective care, and their work has a direct effect on patients’ treatment and recovery (Meretoja et al., 2004). The relevant competencies involve well-balanced knowledge and a set of skills, attitudes, and intellectual strategies (McLagan, 1996), that is, having appropriate values and judgments and delivering effective and high-quality nursing in one’s specialty (Yanhua and Watson, 2011).
Several studies related to knowledge, attitudes, practices, and confidence concerning infection control have been published in Korean nursing journals (Kim, 2009; Kim et al., 2016; Park, 2007), but only two studies have examined infection control in the NICU. One study focused on infection control standards for medical devices in the NICU (Kim et al., 2010), and the other study focused on the effect of education on infection control for multidrug-resistant organisms among NICU nurses (Lim and Bang, 2016). Further, previous studies have developed various tools to measure and enhance nurses’ competency (Ahn et al., 2017; Kang et al., 2008; Kwon et al., 2002; Park and Kim, 2014). However, only one study has assessed awareness and performance levels in relation to infection prevention in hospitals among ICU nurses (Lee and Kim, 2002), and no study has evaluated infection control competency of NICU nurses. Thus, this study aimed to develop an infection control competency scale to more effectively evaluate the performance and knowledge of infection control among nurses caring for high-risk neonates. In addition to producing a useful tool for evaluating the infection control competency of NICU nurses, the study provides basic data that can support development of improved infection control programs for NICUs.
Methods
Study design
This methodological study was performed to develop a tool for assessing high-risk neonatal infection control competency of NICU nurses and to test its validity and reliability.
Development of the tool
Stage 1—item development
A research team consisting of two pediatric nursing professors and two pediatric nursing PhD students identified instrument contents relevant to high-risk neonatal infection control through a literature search of the US Centers for Disease Control and Prevention (CDC) (2017) and Korea CDC (KCDC) (2017) websites. The research team also obtained information from the US Standard Precautions for Healthcare-related Infection guidelines, Korean Ministry of Drug and Food Safety (2016) Guidelines for Safe Use of Injections, Hospital Nurses Association’s (2017) recommendations on Evidence-based Clinical Nursing Practice Guideline-Intravenous Infusions, and Guidelines for Isolation Precautions in Healthcare Settings. We converted relevant information into items included in this study through several seminars and meetings. As a result, contents related to high-risk neonatal infection control were divided into performance and knowledge components, and the numbers of initially identified items were 117 for performance and 134 for knowledge.
Stage 2—content validity testing for initial items
The preliminary tool developed to generate a high-risk neonatal infection control competency scale was structured to include closed-ended and open-ended items, and its content validity was tested using the Delphi technique. An expert panel consisting of four NICU nursing managers, five charge nurses, and two infection control nurses conducted the evaluations. The experts’ mean total clinical career duration was 16.6 years (SD = 9.00), and the mean career time spent at an NICU and at an infection control unit was 7.7 years (SD = 6.30). They rated each item using a four-point Likert scale: “very inappropriate (1)”, “inappropriate (2) ”, “appropriate (3) ”, and “very appropriate (4) ”. An item-level content validity index (I-CVI) and a scale-level content validity index (S-CVI), which calculated the percentage of ratings that were marked as 3 or 4 for each item, were used for closed-ended items. Also, experts were instructed to write any opinions they might have concerning any additional items in the open-ended item section.
In the first round of content validity testing by the expert panel, the I-CVI for performance items ranged from .88 to 1.00, and the S-CVI was .95. The I-CVI for knowledge items ranged from .65 to 1.00, while the S-CVI was .77. After revising the items based on experts’ opinions in the first round, a second round of expert validity testing was conducted. The I-CVI for performance items ranged from .64 to 1.00, and the S-CVI was .99. The I-CVI for knowledge items ranged from .64 to 1.00, and the S-CVI was .95. A discussion was then held among the research team to select items to be deleted or retained. In addition to items having a low I-CVI, some items that were found to vary across hospitals were deleted. However, items believed to be essential by the research team were not deleted even if they had a low I-CVI in terms of making a positive selection based on factor analysis. Items deleted included those involving disinfectants (alcohol, chlorhexidine, and Betadine) whose use differed by institution or in application. Finally, of items with an I-CVI of ≥.80, 78 performance and 79 knowledge items were selected.
During the research team discussion, minor differences among Korean hospitals were identified that related to items concerning breast milk storage duration in refrigerators, the replacement timing of total parenteral nutrition fluid sets, and the usage duration for lipid agents. Therefore, we modified such items to employ times and durations recommended in the US CDC (2017) infection control guidelines and American Society for Parenteral and Enteral Nutrition (ASPEN) (2019) guidelines (Mehta et al., 2017).
Stage 3—modifying and adapting the tool based on a pilot study
A pilot study was performed involving six nurses working in three NICUs of tertiary and general hospitals to assess whether there were any issues with the developed tool in relation to clarity of the scale items, comprehensibility of expressions, and time taken to complete the questionnaire.
Construct validity and reliability testing
Construct validity and reliability testing of the preliminary tool was undertaken using data collected from NICU nurses.
Sample population
NICU nurses in Korea were set as the target population, with NICU nurses in tertiary hospitals and general hospitals as the accessible sample population. Convenience sampling was used to select nurses from four tertiary hospitals and three general hospitals in the Seoul, Gyeonggi, Gangwon, and Gyeongnam regions with the cooperation of the respective nursing units. Under the inclusion criteria, participants had to (1) be nurses working in a hospital NICU and (2) agree to participate in this study. Nurses who provided incomplete answers to tool items or who did not agree to participate were excluded. For factor analysis, a sample size of ≥200 was considered adequate (Tak, 2007).
Data collection procedure and ethical considerations
This study was approved by the institutional review board (IRB) of the researcher’s affiliated institution in relation to ethical considerations for the participants (IRB No. GIRB-A19-Y-0001). Data were collected from February to March 2019. Prior to questionnaire distribution, the researcher and a research assistant informed participants of the purpose, anonymity, and confidentiality of this study. Questionnaires were then administered only to those who signed a consent form. Participants were also informed that their participation was completely voluntary and that they would not be disadvantaged for not participating. Completed questionnaires were retrieved by the researcher and research assistant, and all participants were given compensation of about US$10.
Measurements
Compliance with standard precautions
To test the criterion validity for compliance with standard precautions, we used the 15-item ‘compliance with standard precautions’ tool for assessing hospital nurses’ compliance with standard precautions for infection control as modified and adapted by Seo (2009). Each item was rated on a four-point Likert scale between “always true (4),” “almost always true (3),” “rarely true (2),” and “never true (1).” The total score ranged from 15–60, and a higher score indicated higher compliance. The Cronbach’s alpha (α) reported by Seo (2009) was .76.
Knowledge of standard precautions
To test the criterion validity for knowledge of standard precautions, we used a tool initially developed by Zhao (2007) containing items derived from the revised standard precautions published by the United States (US) Healthcare Infection Control Practices Advisory Committee in 2005 that was then modified and adapted by Seo (2009). This tool consists of 25 items, and each item is answered with a “yes,” “no,” or “I do not know.” A correct answer was given a score of 1, and an incorrect answer or “I do not know” was given a score of . The score ranged from 0 to 25, and a higher score indicated a higher level of knowledge. In a study by Kim (2012), in which the same tool was used on nurses, the Cronbach’s α was .70.
Data analysis
The collected data were statistically processed using SPSS/WIN 18.0 and AMOS 18.0 software. Descriptive analysis was employed to determine general characteristics and study variables using frequencies, percentages, means, and SDs. The construct validity of the items for infection control performance was analyzed using confirmatory factor analysis (CFA). Data distribution was confirmed through the mean (SD), median, skewness, kurtosis, and histogram. To identify the underlying construct which factors of the scale constituted a coherent group of items (Knapp and Brown, 1995), principal component analyses (PCA) that were unaffected by normality (Kang, 2013) were applied with orthogonal rotation (varimax). The number of factors was computed using eigenvalue, scree plot, and factor loadings. The subcategory classifications were analyzed using Pearson correlations. Items for infection control knowledge were dichotomized in terms of scoring (correct or incorrect) for analysis, and “I do not know” was treated as an incorrect answer. Item difficulty and discrimination were computed per item response theory using the ltm package in R software 3.3.3. Criterion validity was tested by analyzing correlations between compliance with standard precautions and knowledge of standard precautions. Internal consistency coefficients (Cronbach’s α values) were computed to assess reliability for infection control performance, and the Kuder–Richardson (KR)-20 test was applied to assess reliability for infection control knowledge.
Results
Participants’ general characteristics
General characteristics (N = 251).
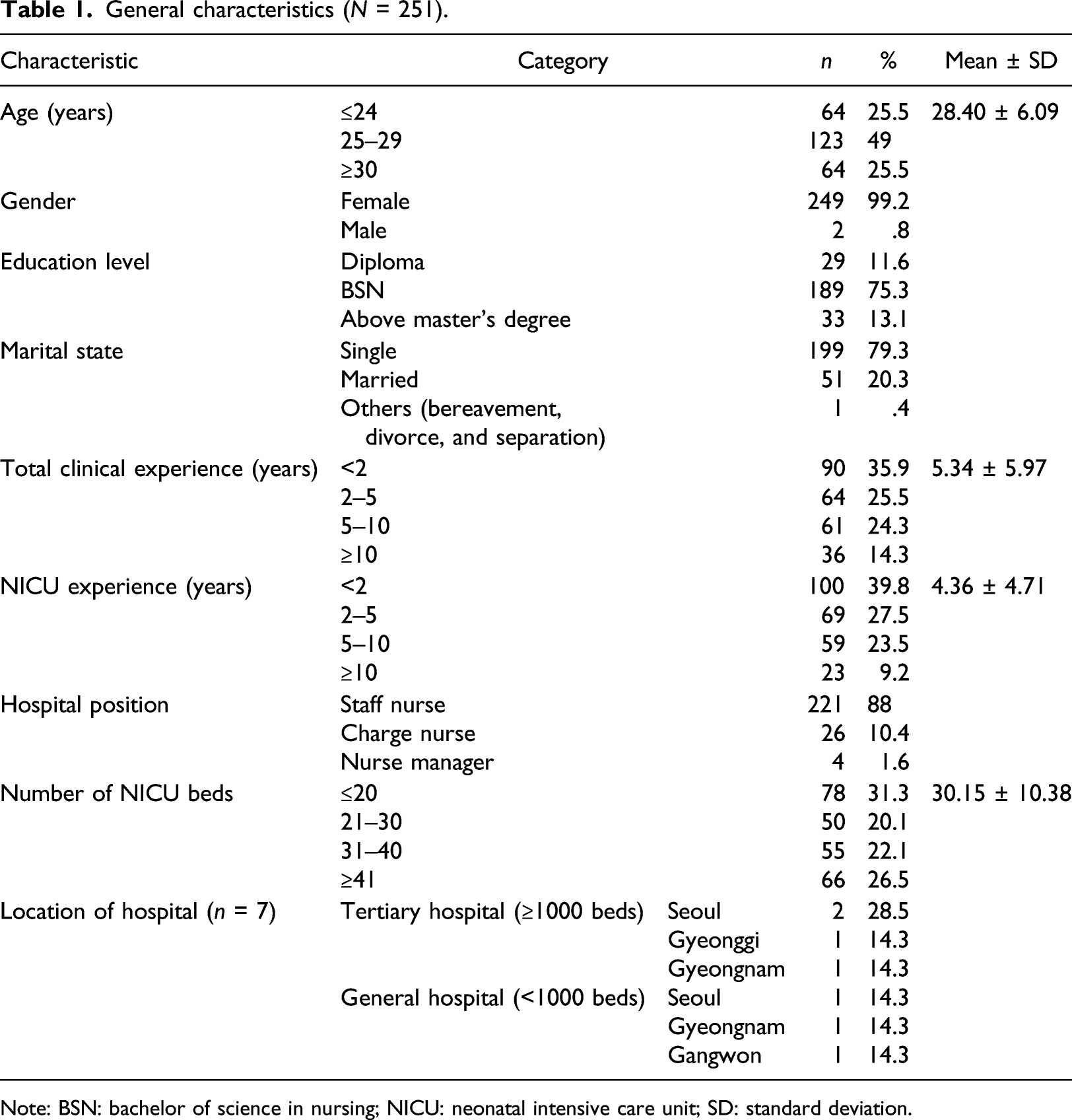
Note: BSN: bachelor of science in nursing; NICU: neonatal intensive care unit; SD: standard deviation.
Construct validity: scale performance items
Exploratory factor analysis (N = 251).

Note: KMO (Kaiser–Meyer–Olkin): .887; Bartlett’s test of sphericity: χ2 = 6581.16 (p < .001). B: basic care; E: environmental management; F: feeding management; I: invasive procedure; M: medication; S: skin care; SD: standard deviation; CR: construct reliability; AVE: average variance extracted.
Although we had initially set six factors for infection control, we first performed exploratory factor analysis, which facilitates investigation of the characteristics of the data without any assumptions concerning the number of factors or structuring of the tool (Pett et al., 2003) in generating a model or structure, as the participants’ responses and perceptions concerning the tool may differ according to the participants’ characteristics and clinical situation. To identify the appropriate factors in PCA, the cutoff value was set to an eigenvalue of ≥1.0 and a factor loading of ≥.35 (DeVellis, 2016). As a result, 29 of 72 items were removed, leaving a total of 43 items over five factors: 13 items for invasiveness/medication management, 9 items for basic care, 7 items for skin care, 8 items for environment management, and 6 items for feeding management. The cumulative explained variance of the five identified factors was 53.71% (Table 2).
Difficulty indices and discrimination according to the classical test theory (N = 251).
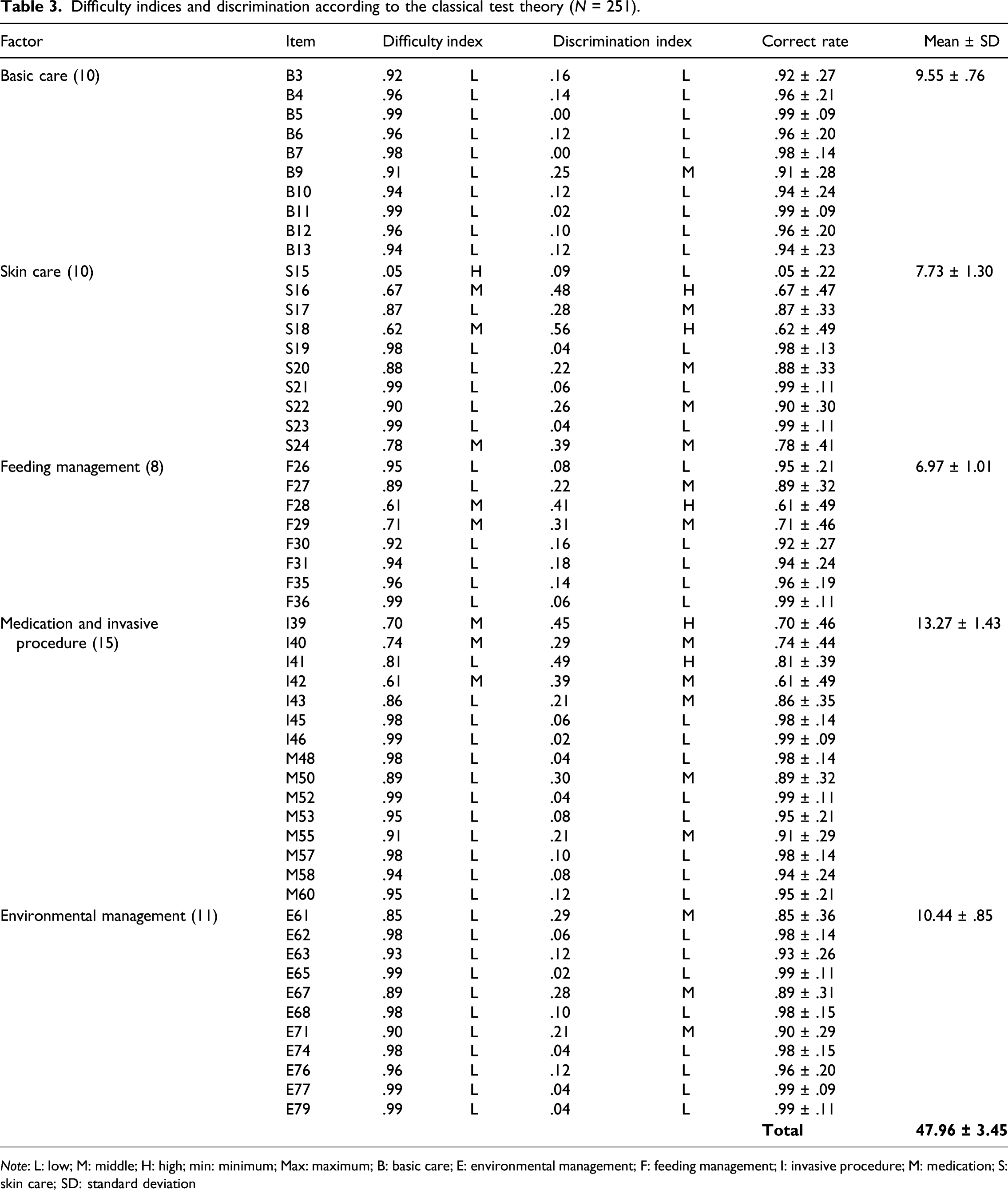
Note: L: low; M: middle; H: high; min: minimum; Max: maximum; B: basic care; E: environmental management; F: feeding management; I: invasive procedure; M: medication; S: skin care; SD: standard deviation
Item analysis: scale knowledge items
To assess item difficulty, the percentage of participants who gave the correct answer was calculated. In the classical test theory, item difficulty refers to the correct answer rate, and we considered a difficulty of ≥.8 as easy items, .2–.8 as moderately difficult items, and <.2 as very difficult items according to Lim et al. (2007). Although there is no absolute criterion for assessing item discrimination (Lim et al., 2007), we divided the responses into two extreme groups and subtracted the bottom 27% correct answer rate from that of the top 27%. A value of <.20 was considered as “almost no discrimination,” .20–.40 as “moderate discrimination,” and ≥.40 as “high discrimination.” As a result, we removed 17 items with a correct answer rate of 100% or with a single incorrect answer or a correct answer rate of 100% when rounded up. We additionally removed 7 items with a negative discrimination value and one item with an extremely low difficulty, and 54 of 79 items were tested for difficulty and discrimination (Table 3). The results showed that there was 1 item with “high” difficulty, 8 items (14.8%) with “moderate” difficulty, and 45 items (83.3%) with “low” difficulty. Regarding discrimination, there were 5 items (9.3%) with “high” discrimination, 15 items (27.7%) with “moderate” discrimination, and 34 items (63.0%) with “low” discrimination.
Criterion validity
Criterion validity (N = 251).
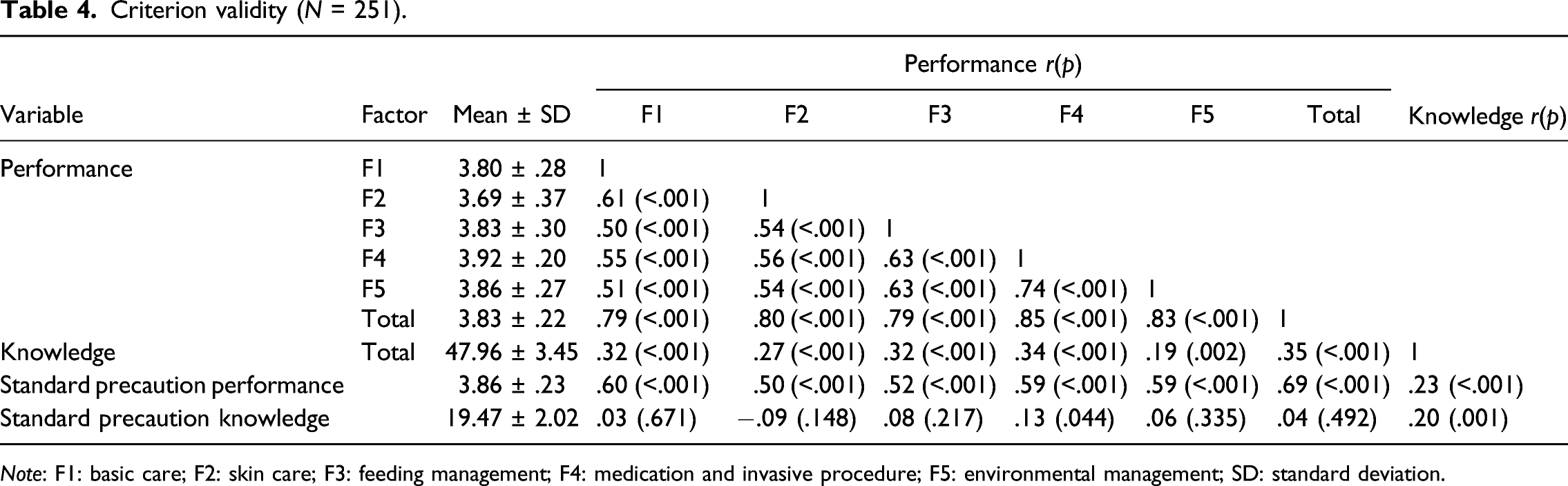
Note: F1: basic care; F2: skin care; F3: feeding management; F4: medication and invasive procedure; F5: environmental management; SD: standard deviation.
Reliability
Cronbach’s α for the entire high-risk neonatal infection control performance section was .95, with values ranging from .81 to .88 across factors. Based on criteria suggested by DeVellis (2016), where Cronbach’s α of between .70 and .80 indicates good internal consistency reliability and that between .80 and .90 indicates high internal consistency reliability; the high-risk neonatal infection control performance component in our study had a high reliability. The knowledge component had low reliability indices for each factor, but reliability of the overall tool was (KR-20) .67 (Supplementary table).
Finalized scale and factor naming
For the main survey, the preliminary scale was reduced to 42 items over five factors for performance and 54 items over five factors for knowledge, after establishing construct validity, reliability, and factor naming. The finalized high-risk neonatal infection control competency scale was divided into a high-risk neonatal infection control competency scale_performance (HirNICCS_P) component and a high-risk neonatal infection control competency scale_knowledge (HirNICCS_K) component. Factors involved in both HirNICCS_P and HirNICCS_K were identical, namely, basic care (factor 1), skin care (factor 2), feeding management (factor 3), medication and invasive procedure management (factor 4), and environment management (factor 5). HirNICCS_P component contained 42 items and was assessed using a 4-point Likert scale (1 for “not at all true,” 2 for “rarely true,” 3 for “almost always true,” and 4 for “always true”), where the scores ranged from 42 to 168, with a higher score indicating higher performance of high-risk neonatal infection control. HirNICCS_K component contained 54 items with “yes,” “no,” or “I do not know” responses. Correct answers were scored as 1, while incorrect answers and “I do not know” answers were scored . The scores ranged from 0 to 54, with a higher score indicating a higher level of knowledge.
Discussion
This study involved the preliminary development of a novel scale to measure infection control competency among nurses caring for high-risk infants in NICUs. First, we first reviewed Korean and international literature and guidelines dealing with the key elements of nurses’ infection control strategies to identify key constructs concerning NICU nurses’ infection control competency. Researchers with both clinical experience and theoretical knowledge in the care of high-risk neonates then extracted preliminary items after several rounds of discussions. These discussions were the basis for a scale development process that reflected both aspects of domestic clinical practice and international recommendations for infection control competency. Next, identified preliminary items were tested for content validity based on expert opinions. We obtained opinions of experts with experience in providing nursing care to high-risk neonates in NICUs in various hospitals, and we found that there were differences in infection control guidelines across institutions. For items that differed in their management across institutions, such as breast milk storage in refrigerators, replacement timing of total parenteral nutrition fluid sets, and usage duration of lipid agents, we used the US CDC standard management guidelines. This was because experts agreed that this would facilitate a general use of the tool throughout Korean hospitals. However, we recommend that a more standardized infection control be established in relation to these items (and in the use of disinfectants that was excluded as an item here due to widely differing management practices), following relevant research.
Second, to test construct validity, exploratory and confirmatory factor analyses were performed for HirNICCS_P. Exploratory factor analysis led to 43 items over five factors. However, in CFA, a single item for medication and invasive procedure management with a low convergent validity standardized coefficient was removed, resulting in a total of 42 items. There seemed to be a result overlap between medication management domain with invasive procedure and equipment management domain, as most medications are administered via intravenous injections in the NICU. As HirNICCS_K items involved formative indices that cannot be analyzed using factor analysis (Kang, 2013), we examined difficulty and discrimination of items. Most of the items had moderate or low difficulty and discrimination, suggesting that the tool was appropriate for determining an absolute rather than a relative evaluation of the knowledge aspect of infection control competency. Moreover, we examined correlations between compliance with standard precautions and knowledge of standard precautions to test criterion validity of the tool. The results showed that correlation with performance concerning standard precautions was moderate at .69, but that correlation with knowledge concerning standard precautions was low at .20. HirNICCS_P items most likely showed a high correlation due to the external criterion used, which involved the performance of high-risk neonatal infection control as recommended in general infection control guidelines. However, because this study involved nurses working in NICUs, our assessment using knowledge of infection control specific to adult patients might have been less appropriate as an external criterion.
The reliability of HirNICCS_P items was assessed using Cronbach’s α, with a value of .95. The reliability of HirNICCS_K items was assessed using a KR-20 test, with a value of .67.
The finalized scale consisted of five factors for both performance and knowledge scales: basic care, skin care, feeding management, medication and invasive procedure management, and environment management. These factors covered all areas identified in the standard KCDC HAI and general infection prevention guidelines. These include aseptic procedures, hand hygiene, injection practice, and insertion device–related prevention procedures for devices such as ventilators and central venous catheters. Others include environment management in healthcare institutions, with the addition of feeding management, which is a specific aspect of care provided in NICUs, and skin care for high-risk neonates who have a highly vulnerable skin integrity. Factor 1 involves basic nursing pertaining to hand hygiene and the use of personal protection devices at the NICU and includes the most basic and general issues in infection control. However, this factor is distinctive in that the nature of nursing care for high-risk neonates, where all treatments that are required are performed simultaneously to minimize stress on neonates, and emphasizes the critical importance of hand hygiene, given the range of diseases that requires isolation to protect high-risk neonates vulnerable to infection (Bang et al., 2018). Factor 2 involves skin care to prevent infections through skin contact among high-risk neonates. This factor concerns overall skin-related nursing treatments performed at the NICU, comprising umbilical cord care, bathing, skin protection, used diaper removal, and care in relation to ophthalmitis and dermatitis (Lund, 2016). Furthermore, the variety of items involved suggests that skin care provided by nurses is a critical factor in infection control for high-risk neonates. Factor 3 involves feeding management related to management of breast milk and formula and breastfeeding at the NICU. Feeding management is also a major aspect of nursing care for normal neonates but is critical for high-risk neonates who are at a particularly high risk of contracting necrotizing enterocolitis and sepsis due to an immature gastrointestinal system (Boo, 2016). Therefore, accurate knowledge and compliance with breast milk and formula storage requirements as well as appropriate feeding methods are especially important in high-risk neonatal infection control. Factor 4 involves medication and invasive procedure management and relates to the management of central venous catheters, IV agents, and ventilators for high-risk neonates. While essential in NICUs to prevent HAIs, this factor is addressed in KCDC’s guidelines for infection control in ICUs, which argues that management of high-risk neonates does not significantly differ from that of critically ill adult patients, except for an emphasis on lipid agents and IV filters frequently used in NICUs. Factor 5 involves environment management and concerns the management of equipment, supplies, visitors, and staff in NICUs. Based on the NICU setting, scale items addressed regular disinfection of neonatal cribs or incubators, monitoring devices, intravenous pumps, and treatment tables and bathtubs as well as restriction of visitors with infectious diseases, infection prevention education, and nurses’ infectious disease management.
With high-risk neonates, it is essential for NICU nurses to accurately understand and strictly comply with infection control requirements. In this study, the distribution of the overall infection control performance level shows evidence of competent and proficient practice and is similar to the findings of previous studies that showed right skewness or a high-performance level in nurse competence scales (Dos Santos et al., 2019; Meretoja et al., 2004). Even newly certified nurses appeared to have a high-performance level that was indistinguishable from that of more experienced nurses. Therefore, it appears that HirNICCS_P has the potential for wider application in clinical practice and management in this regard (Meretoja et al., 2004).
In summary, previous studies have investigated nurses’ standard precautions for infection control and organizational standardization of infection control for hospital personnel (KCDC, 2017; Kim et al., 2010). This standardization, however, is limited in its applicability to NICU nurses, who provide highly specialized infant care. Thus, this study met the need for a unique objective scale to evaluate the infection control competency of nurses responsible for providing quality care to high-risk neonates in the challenging NICU environment.
Limitations
Three study limitations should be noted. First, the explanatory power of this tool was moderate at 53.7%, which was less than the recommended explanatory power of approximately 60–70% (Lee et al., 2009). Thus, we suggest recruiting participants with more diverse characteristics to refine and modify the tool and reconfirm its explanatory power. Second, this tool was developed for nurses working in some NICUs in Korea and therefore, has limited generalizability. Further studies are recommended to validate the tool using a larger sample. Third, with respect to scale reliability, no test–retest procedure was used to assess scale stability. Therefore, future research should include a test–retest procedure to examine the stability of the tool.
Implications for practice
A high-risk neonatal infection control competency scale was developed in this study to assess infection control competency among NICU nurses. Two types of competencies—performance and knowledge—were addressed, as nurses must have accurate knowledge about infection control and be able to apply it in practice. Therefore, this scale can be used to assess the performance and knowledge aspects of infection control competency, and its application can lead to strengthening of infection control education for nurses who score low on performance and knowledge competency. Also, the scale will be useful in identifying any performance challenges in a particular NICU and in strengthening aspects of practice among nurses who obtain high scores for knowledge but low scores for performance.
Conclusion
Through a literature review and with consideration of clinical situations pertaining to high-risk neonates in Korean NICUs, an objective scale was developed to specifically assess the infection control competency of NICU nurses. The scale captures aspects of infection control performance and knowledge that are crucial for quality care of high-risk neonates, and it can be used to evaluate the effectiveness of educational programs aimed at increasing NICU nurses’ infection control competencies. This scale can also be used in nursing education studies to identify means of instilling infection control competencies in future NICU nurses. Finally, the scale can be used to generate evidence for nursing practices and strategies that are effective in reducing HAIs among high-risk neonates.
Supplemental Material
sj-pdf-1-chc-10.1177_1367493520943772 – Supplemental Material for The predictors, barriers and facilitators to effective management of acute pain in children by emergency medical services: A systematic mixed studies review
Supplemental Material, sj-pdf-1-chc-10.1177_1367493520943772 for The predictors, barriers and facilitators to effective management of acute pain in children by emergency medical services: A systematic mixed studies review by Gregory A Whitley, Pippa Hemingway, Graham R Law, Arwel W Jones, Ffion Curtis and Aloysius N Siriwardena in Journal of Child Health Care
Footnotes
Acknowledgements
We acknowledge all participants of this study. Also, we would like to thank Jon Mann (Academic Specialist and Instructor, Academic Center of Excellence, University of Illinois at Chicago, USA) for English language editing.
Author Contributions
Study design: Mi Yu
Data collection and analysis: Mi Yu, Hyunju Kang, Jisun Park, Miran Yang
Manuscript writing: Mi Yu, Hyunju Kang, Jisun Park, Miran Yang
Ethical Approval Information
Ethical approval was obtained from the Gyeongsang National University Institute Review Board (IRB No. GIRB-A19-Y-0001).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science, and Technology (NRF-2018R1D1A3B07045408).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.