
Abstract
This study explores the experience of communication regarding the care of children with cancer, from the perspective of family carers, children and health professionals in occupied Palestinian territory. This study employed an ethnographic collective qualitative case study approach, which was applied in one oncology unit in a Palestinian hospital. Participant observation and semi-structured interviews were used. This study only reports the findings of the interviews with the participating family carers. Fifteen interviews were conducted with family carers (n = 14 children), namely mothers (n = 7), grandmothers (n = 7) and a father (n = 1). The findings reveal that styles of information were given to children by their family carers: minimal/practical information, gradual information, false information, reassuring information and several sources of information. The term cancer was avoided in the discussion of the disease to ameliorate the negative effect of this term, which is considered taboo in the studied culture. Despite the recent trend emphasising the importance of parents communicating openly with their children with cancer, the findings of this study suggest that such open communication is not accepted by all parents. Hence, a case-by-case strategy could be adopted to treat each child in a way that is individual to that child and their culture.
Introduction
Located in the Middle East, the occupied Palestinian territory (OPT) consists of the West Bank (including East Jerusalem) and Gaza (WHO, 2017). The political situation within the OPT, especially in Gaza strip impacts on human security, well-being and the general determinants of health (WHO, 2017). Children account for around 50% of the Palestinian population and those living in poor socio-economic conditions represent 25.7% (Palestinian Central Bureau of Statistics, 2012, 2015). Whereas over 80% of childhood cancers are cured in developed countries, just around 20% of childhood cancers are cured in low- and middle-income countries (Gupta et al., 2015; Howard et al., 2018). In 2017, 131 Palestinian children <15 years of age were diagnosed with cancer (Palestinian Health Informatrion Centre, 2017).
Childhood cancer is an exhausting chronic condition compounded by the high frequency of visits to hospital, medication side effects and associated complications. Caring for children with cancer is frequently viewed as a very challenging experience, which affects not only parents and relatives but also the healthcare professionals interacting with children with low survival probability (Graziano et al., 2016; Tang et al., 2020). Communicating with children with cancer can be challenging especially in terms of what information should be given to them at different stages of their illness. Stein et al (2019) noted a lack of evidence-based guidelines to support healthcare professionals and families to communicate with children about their life-threatening and life-limiting illnesses. One of the most challenging issues of communication for parents and professionals is the issue of conveying prognostic diagnosis to children with cancer (Sisk et al., 2016).
Literature review
The volume and content of information given to children with life-threatening and life-limiting illnesses at different illness stages is a complex issue. Inconsistency between the parents and professionals’ perceptions about whether children can comprehend death and children’s actual comprehension (Pfefferbaum, 1982; Pfefferbaum et al., 1982) may play a part. The Piagetian developmental theory proposes that children acquire comprehension about death gradually, acquiring the logic, clarity and structure they need to gain a complete understanding of the fact that death is immediate and permanent between 11–16 years (Beale et al., 2005). Younger children are susceptible to ‘magical thinking’ (Santrok, 2009) and are unable to completely grasp what death implies, thus suggesting they should not be given information or allowed to make decisions regarding their own death. However, several studies have found that children’s knowledge of their terminal status may increase through their experience of being treated in oncology wards and receiving information regarding their disease (e.g. seriousness and treatment) and information about death (Bluebond-Langner, 1978; Clarke et al., 2005; Goldman and Christie, 1993; Patenaude, 2005). The challenges relating to communication with children become even more complicated when the focus is centred more on prognosis rather than diagnosis (Sisk et al., 2016).
Some parents aim to protect their children from potential emotional suffering that might occur if they were given comprehensive details about their condition (Van der Geest et al., 2015; Zelcer et al., 2010). Van der Geest et al. (2015) found that mothers’ lack of confidence about telling their children that they were terminally ill contributed to a protective approach. Cultural background is one of the most significant issues that can affect the degree of openness in communication between children and parents. A study of Jordanian mothers found that they tend to avoid sensitive areas such as delivering bad news, talking about prognosis or death with their children with palliative care needs, especially if they perceived their children did not want to discuss such matters with them (Atout, 2017; Atout et al., 2019). Cultural differences are also seen in healthcare professionals. Parsons et al. (2007) found that 65% of American physicians but only 9.5% of Japanese physicians openly informed children about a cancer diagnosis. Several factors were shown to affect the nature of communication, such as the physicians’ attitudes, patient factors and work culture. Children’s understanding of their illness, is affected by factors like their level of development and their experiences as well as cultural issues (Gray et al., 2014). Most research tends to focus on understanding the parental/health professionals’ perceptions of illness, with less attention being given to consideration of the findings of these studies when devising clinical plans for treating children with cancer in different cultures. Concepts such as cancer stigmatisation have only been studied in a few cultures (Gray et al., 2014), so further exploration of the effect of social stigma on parents’ behaviours such as seeking social support (Smith et al., 2008) could be valuable.
Most research reflects Western cultural settings and mores which do not align with the Arab parents’ cultural considerations and religious beliefs. In Palestine – a specific Arab culture – the political conflict increases the challenge and complexity of communication between parents and professionals and child cancer patients. For example parents from Gaza find difficulty to get an access to the West Bank for their children to receive the necessary health care which is not offered in Gaza. They need to apply several times before getting a permission which is not guaranteed after the long process (World Health Organisation, 2019).
Aim
This study reports on the findings of the interviews with family carers from a larger study exploring the experience of communication with child cancer patients from the perspectives of family carers, healthcare professionals and children.
Methods
Study design
A qualitative ethnographic case study approach (Pagram, 1999) was used to gain detailed insight into the experience and process of communication in the care of children with cancer.
Study setting
This study was conducted in one hospital in Nablus city in the West Bank. Nablus is the second largest West Bank city and constitutes a centre where more than a million people living in northern villages come to access medical services.
Sampling strategy
Purposeful sampling was used. Children were eligible if they were aged 6–18 years, undergoing care in the paediatric oncology unit (POU) of the study hospital, and the children gave permission/assent for being observed and/or interviewed. Family carers (children’s parents or other close relatives) were eligible if their child was eligible. Children and family carers were ineligible if healthcare professionals considered the child to be too sick and/or distressed, if the family carers was distressed or if there were barriers to communication.
Access and recruitment
A research assistant from the research team made an informal visit to the POU to familiarise themselves with the setting, provide information about the study to the nursing and medical administrative team and determine interest in the study. The head nurses identified the parents of eligible children and subjected to parental and child agreement; they were then approached by the research assistant to discuss the study and answer any questions. Every parent received a written invitation letter and information sheet about study and given around three days to consult with other people and decide whether to consent or not. Children, >6 years were asked to assent (Royal College of Paediatric and Child Health, 2000) to participate.
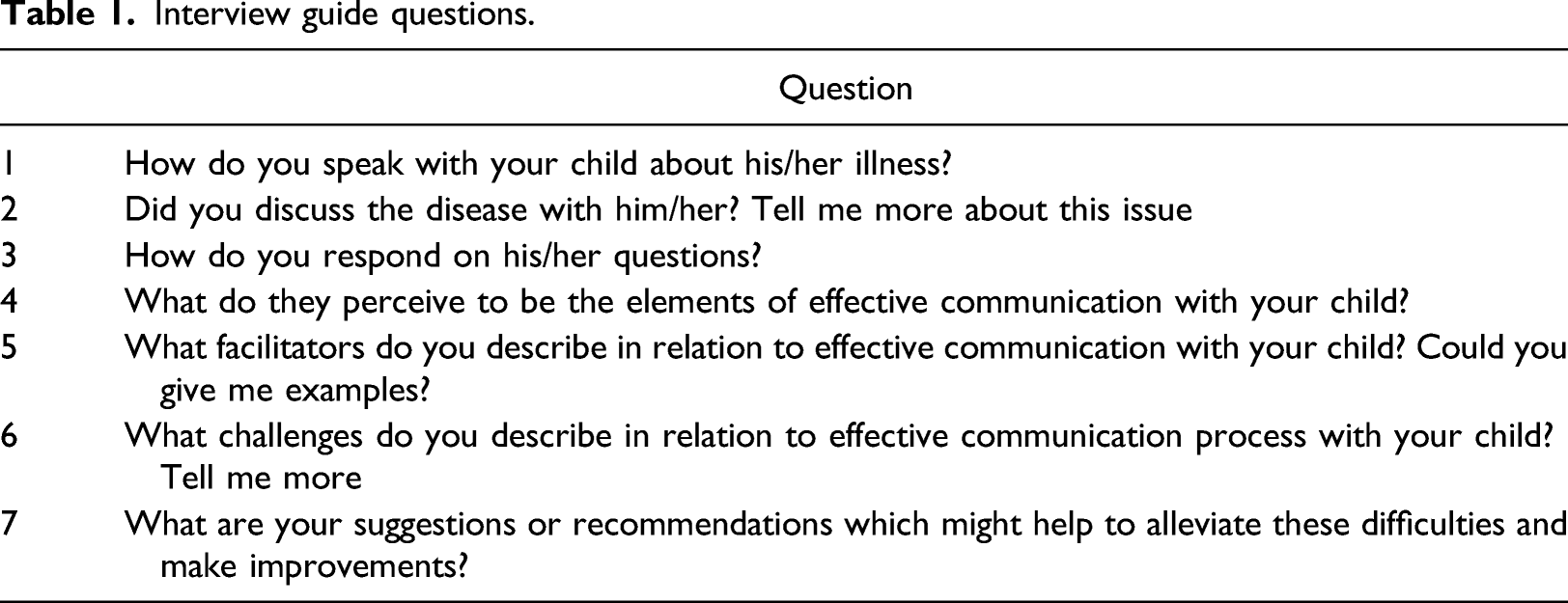
Methods of data collection
Interview guide questions.
Data analysis
Children’s characteristics and interview details.
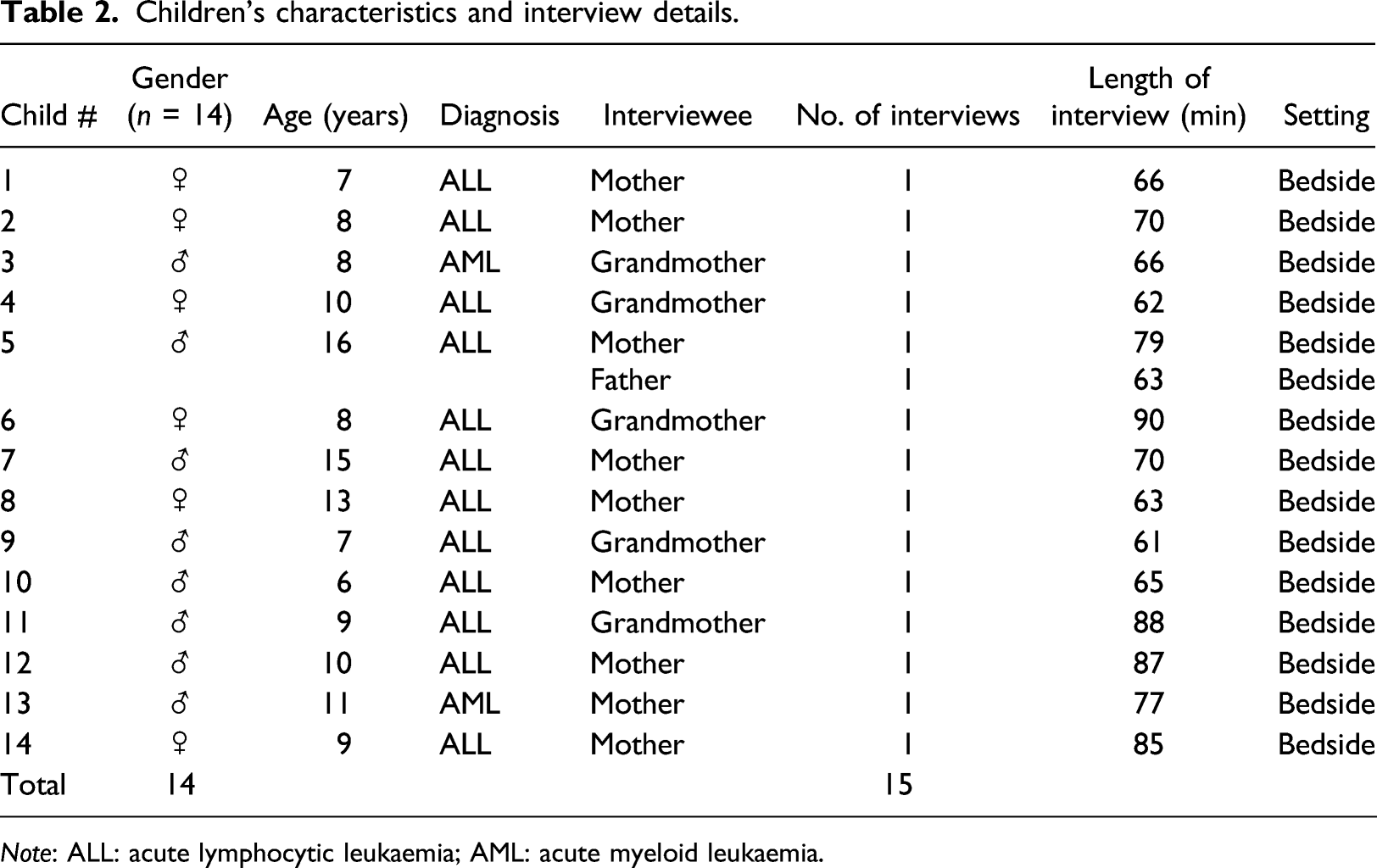
Note: ALL: acute lymphocytic leukaemia; AML: acute myeloid leukaemia.
All interviews were transcribed verbatim by the lead author. In the current study, an inductive thematic analysis approach was adopted. The inductive approach indicates that the themes are derived from the data itself (Patton, 1990). With inductive analysis, data are not derived from the researcher’s previous theoretical assumptions. The first step, data familiarisation, occurred during data collection, and it involved forming a preliminary understanding of the dataset (Braun and Clarke, 2006). In step two, initial codes were generated (Saldaña, 2013), and the processes of ‘open coding’ and ‘analytic coding’ were used to identify potentially relevant data (Merriam and Tisdell, 2015; Richard, 2015). For the third step, in which the researcher sought to identify themes, codes were combined in order to establish higher-level themes through ‘axial coding’ (Charmaz, 2014; Corbin and Strauss, 2015). Additionally, the schematic shown in Figure 1 was used to conceptualise the links between codes and themes. In turn, themes were reviewed based on Patton (1990) criteria of homogeneity and external homogeneity. Finally, themes were named based on the participants’ words, the researchers’ perceptions and the literature (Merriam and Tisdell, 2015). The researcher also sought to create short but informative theme names (Braun and Clarke, 2006) Visual representation of a coding map used in the study.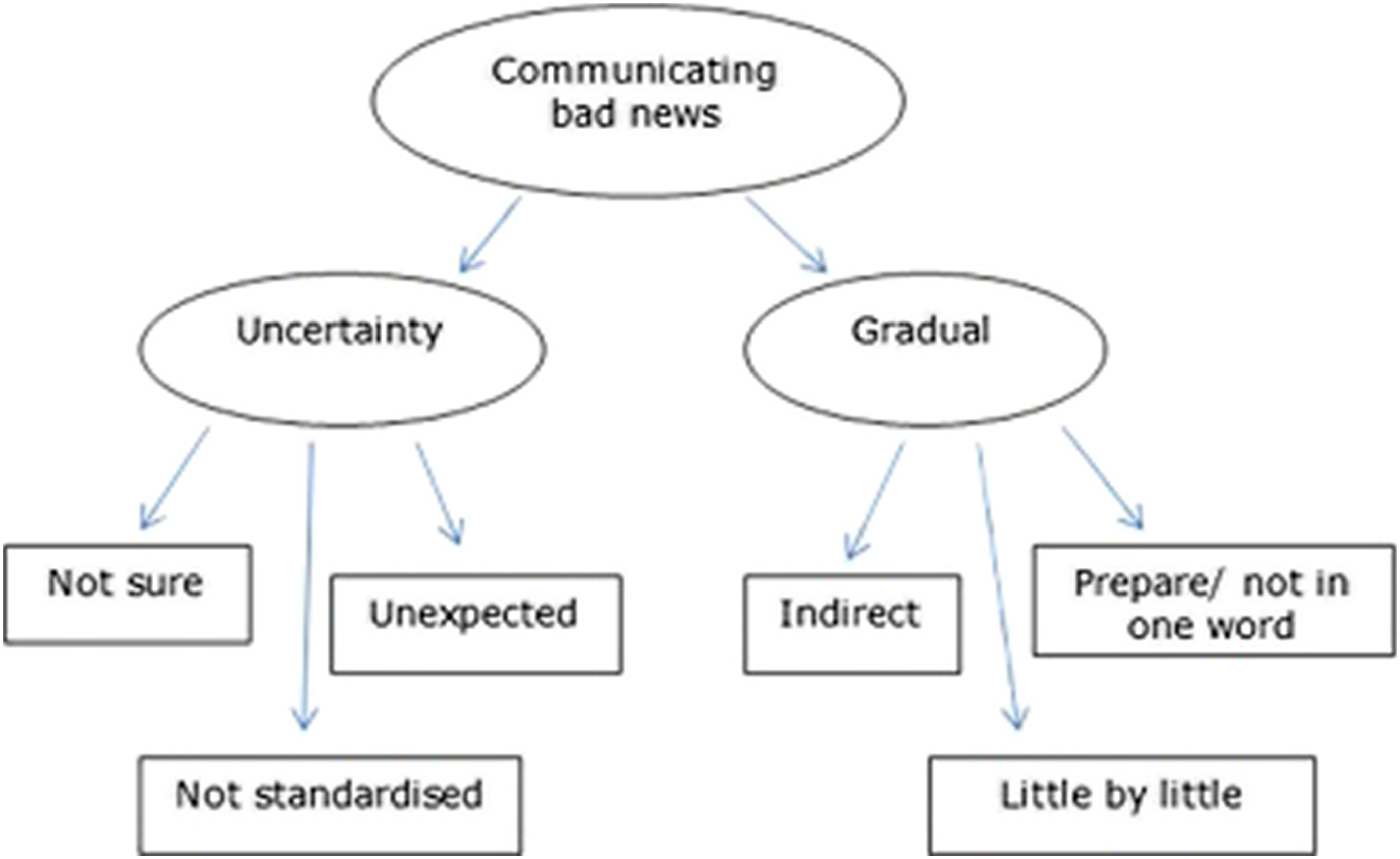
Ethical considerations
Ethics approval for the research was obtained from the hospital’s ethics committee (XXXX). The risks and benefits of research participation and their right to decline or withdraw were discussed with all potential participants. The information sheets and informed consent confirmed that their anonymity would be preserved through the removal of any information that might reveal their identity and the use of pseudonyms or numbers instead of their original names. Informed consent included permission to use anonymised extracts from the interviews.
Study rigour
Rigour and the credibility of this study were achieved in several ways, for example participants were given a summary of the main points discussed in the interview to check their responses. Peer debriefing was employed (Lincoln and Guba, 1985) and the principal investigator (MA) sent extracts of the interview transcripts to her co-researcher (BC) for the her input.
Findings
Participants’ characteristics
Characteristics of study participants.
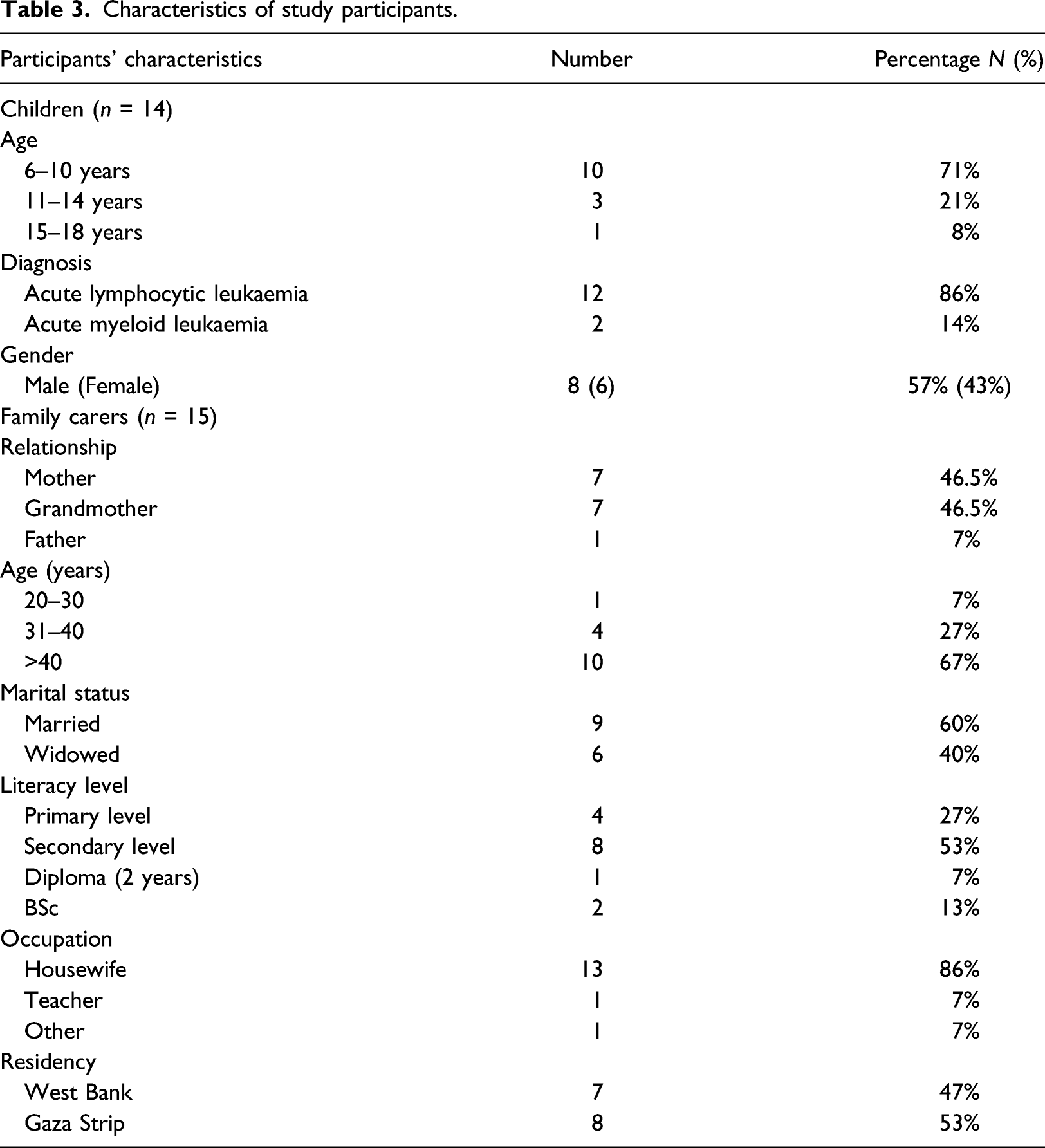
Five major themes reflect the different styles of communication that were adopted by the family carers; minimal/practical information, gradual information, false information, reassuring information and multiple sources of information. A sixth theme, unique to the impact of cultural factors on the style of parent–child communication within the Palestinian context, is also presented.
Minimal/practical information
Six family carers provided their children with minimal information about their illness. Some thought that, due to their limited cognitive abilities, children might not understand their condition:
They will not understand the word…. for example what is the meaning of cancer or leukaemia or something like this …. they will not understand it (Mother, Child 10, Boy 6 yrs, ALL).
In some cases, parents felt that their children did not want to speak about their anxieties or concerns, despite their efforts to encourage their children to communicate. Some mothers tried to motivate their children to speak about their suffering:
My son is from the type that if he has pain…he does not like to complain ….…I know this during his disease…I tell him…‘No you should speak…what the thing that hurt you…tell me mum…what wrong with you’ …‘No no nothing mum’….you feel that he puts in his heart…although I am his mother but he puts in his heart…(Mother, Child 13, Boy 11 yrs, AML).
Some mothers (n = 7) provided their children with only the practical information they thought was necessary to ensure compliance with treatment, especially chemotherapy, but did not provide information about the prognosis:
I tell her you need to take this treatment chemotherapy…this is its name chemotherapy…and I know the treatment has its effects many effects…and you will also take cortisone and the cortisone affects …when she was walking she was not able to hold her leg I was telling her… this means telling her how every treatment affects…I discussed about how everything might affect (Mother, Child 14, Girl 9 yrs, ALL)
Gradual information
Some mothers provided their children with gradual information, one step at a time, according to the stage of their illness. These mothers considered that children should be informed about their diagnosis gradually to prevent their psychological status being affected in a way that might negatively impact their response to treatment:
When the girl ask me ‘Mum what is the problem that I have?… when doctors told me she should know .. …I was telling them ‘No I do not want her to know now, I am scared if the girl knows, her body will reject the treatment….reject the treatment…something [bad] will happen to her …let me tell her using my own way….little, little in order for her to accept it’ (Mother, Child 14, Girl 9 yrs, ALL)
False information: changing the nature of the illness
Some parents and grandmothers hid the illnesses from their children by changing the nature of the illnesses. For instance, one grandmother mentioned that her grandson was told he had a blood infection rather than cancer or leukaemia:
His father told him that he has an infection in blood…...… (Grandmother, Child 9, Boy 7 yrs, ALL).
Another mother explained that her 6 -year old son with ALL knew he had a ‘virus’ and that ‘he takes doses but he does not know why’. A grandmother whose child did not know she had cancer avoided the use of the word cancer, even though she was prepared to use other medical language:
She sees those children and she asks …‘My grandma do they have cancer’?...I say ‘No’…I say ‘Weakness in blood…decrease in immunity…decrease in platelets, when it arises, you will be good’ (Grandmother, Child 4, Girl 10 yrs, ALL)
Concealing the nature of the disease aimed to prevent the children from being negatively affected. Additionally, some mothers considered that children could not understand their disease or would have been less able to tolerate associated pain if they had known the true nature of their disease.
Reassuring information
Some mothers ‘knew’ that their children had knowledge about their illnesses and that they even thought about death; this knowing came either from the result of their children’s behaviours or from what other relatives noticed. When mothers knew that their children started thinking of death, they initiated a discussion to provide reassurance and support and to motivate them to talk about their worries. However, some felt that their children did not want them to know that they were aware of and thought of death. One mother mentioned that her son had been looking at a television series in which a character got cancer and died but she thought that her son did not know about his prognosis. However, his older sister told her that she felt that he understood his possible prognosis despite his family concealing the nature and prognosis of his illness from him:
I noticed him watching that series he was looking on a snapshot of that girl [who has the disease]… as soon as I walked near him, he closed his mobile… this means that he understands and does not want to let us understand that he understands…. There was another time …I was with him in the hospital, he was opening the internet and watching these diseases etc.…as soon as I came, he closed the mobile, …I took the mobile from him …he did not want me to know that he knew what he has [the disease] (Mother, Child 12, Boy 10 yrs, ALL)
Multiple sources of information
Following referral from a general hospital in Gaza (without a POU), parents from the Gaza strip had to travel with their children to the POU in the study hospital in Nablus on the West Bank. Political restrictions on travel meant that eight parents from the Gaza strip were unable to accompany their children; prohibitions on travel for young parents from Gaza to the West Bank meant that the responsibility for support and communication lay with the older carers (e.g. grandmother or aunt). This exacerbated the sense of separation and isolation for the children and their parents. The discontinuity of care caused by the requirement for relatives other than parents to accompany children upon admission to a different clinical centre increases the complexity of communication. Although it was clear from the study findings that all grandmothers demonstrated a high level of compassion and responsibility towards their grandchildren, some lacked not only the skills and knowledge but also the experience to communicate with them. The attachment between children and mothers is not necessarily compensated by the presence of their grandmother or other carers. This was clear with one child who refused to speak to his mother to show his anger at her for not accompanying him:
He was calling [phoning] me to speak to me…then he was refusing to speak to me saying ‘You did not travel with me’. But you know you know the coordination here [prohibition on travel] …even though he knows this thing is over my hand…still he did not want to speak to me… He call me but keeping silent, he does not want to speak to me…then he said ‘I will not forgive you…I will not forgive you to the day of judgment …do not think if I return [to Gaza] I will forgive you’ (Mother, Child 7, Boy 15 yrs, ALL)
Cultural perspective
The word cancer was considered a taboo word, with the majority of the mothers refusing to mention it at all because of the negative impact the word had on them and on their children:
It was a shock…shock….I did not expect this….I expect anything else…anything might happened with the girl… this means the word cancer [Glory be to Allah]…this means it is a hard word… even if you know God might cure her…if she cure from it, still this word considered a shock for human (Mother, Child 14, girl 9 yrs, ALL)
Participants did not speak directly about cancer but referred to it as ‘that disease’, even when their children were not present. One of the mothers mentioned avoiding reading about cancer or mentioning its name:
No I did not read about it…this disease …we do not dare to mention its name…its name is hard …to have it [cancer]… and all people are the same ….this lady is the same [the mother whose child near her child’s bed]…she told you ‘I’am saying leukaemia in order not to say cancer’…it is challenging to say cancer (Mother, Child 1, girl 7 yrs, ALL).
The perceptions that the family carers had regarding the disease influenced their interactions with their children, particularly in highly sensitive situations such as response to initial diagnosis, conveyance and reception of unfavourable information. Their Arab-Islamic culture impacted on the perceptions that the majority of parents formed about the significance of their child’s illness. For instance, a large number of carers perceived the illness as a way in which God was testing them to see how patient and accepting they were of the situation or as payment for sinful behaviour. One mother explained she was being tested through her child’s illness either to assess her patience or punish her for sins she had committed. Another mother believed that her daughter became ill because God willed it so and she was convinced that God would either heal her daughter or repay her in another manner if her daughter died or suffered for a long duration:
I know that my child’s illness is a plague of God…my God wants to examine my patience…I have certainty of God … or may[be] I did something wrong and He want to remind me to return..[to right place]…Why to be sad?...I am always feels thankful to God….sure that God will compensate me, if it not by my health, He will bless me in different ways, blessing my family or maybe [providing me with] psychological peace or He will compensate me later in life after life (Mother, Child 2, Girl 8yrs, ALL)
Discussion
This study reports on the findings from the interviews conducted with the family carers to identify the nature of information they provided to their children with cancer. Almost all family carers (n = 15) adopted a protective approach, regardless of the child’s age, in terms of the type and nature of information they gave their children. Overall, the way in which the family carers chose to communicate was neither planned nor intentional; it reflected their natural desire to protect their children from the psychological and physical harm caused by cancer, possibly reflecting a concern that too much information would cause their children anxiety. This tendency of family carers to act protectively has been confirmed by several other studies (Arruda-Colli et al., 2015; Van der Geest et al., 2015; Varkula et al., 2010). This study reveals that adopting a protective approach was a core consideration among all of the family carers; none of them openly discussed any negative prognosis, especially death, with their child.
This study revealed that the family carers provided their children with ‘minimal/practical’ information to ensure their cooperation during their treatment journey. However, provision of information was often ‘gradual’ and triggered by events such as hair loss, when carers were prompted to provide children with ‘practical’ information to prepare them and help them accept the changes happening to their body.
In terms of diagnostic information, ‘false’ information about the illness was given to a few children, with some children being told that they had a blood infection rather than cancer or leukaemia. This finding is congruent with a UK study Clarke et al. (2005) conducted with 55 parents whose children (mean age, 4.24 years) were newly diagnosed with ALL. Seventeen parents gave their children only minimal information, such as that they had blood problems, without revealing the severity of the disease, feeling that too much information would cause the children anxiety.
The findings of this study show that some mothers (n = 5) avoided open discussion with their children, as the children themselves did not want it. Similar to previous work (Van der Geest et al., 2015), parents and caregivers in this study avoided discussion with their children about death, as the children themselves refused to talk about it. However, when one mother became aware of her child’s negative thoughts about his illness (based on her awareness of his special interest in a movie in which a girl had a similar illness and died), she talked to him about this and provided protective ‘reassuring’ information to him, affirming he was going to get better.
There was evidence that some of the children hid their fears and concerns as a means of protecting their parents. A study conducted by (Atout, 2017) to understand the experience of communication with children with palliative care needs from the perspectives of Jordanian parents and health professionals found that the protective approach demonstrated by children might originate from the protective environment in which children live (Atout, 2017). The current findings substantiate previous qualitative studies (Atout et al., 2019; Van der Geest et al., 2015) that show that children at a certain developmental age and experience are aware of the expected prognosis of death, but they hide this from their parents as a result of their knowledge of how painful this topic is to their parents.
Cancer is a taboo topic in Palestinian culture and is rarely talked about openly, as revealed by the results of this study. The participants referred to cancer as ‘that disease’ rather than use the actual term, confirming what previous research has reported (Khoury et al., 2013; Parsons et al., 2007; Varkula et al., 2010; Yin and Twinn, 2004). This study has uncovered new knowledge about how participants found support in their cultural background in accepting the situation and being patient, and this was linked to the significance of the disease. Furthermore, the way in which the carers communicated with healthcare professionals was influenced by the widely held belief that their child’s disease was God’s way of testing their patience and acceptance, as well as way of redeeming sinful behaviour. Typically, one mother considered that healthcare professionals were only capable of treating her daughter, not curing her. Consequently, she believed that every medical intervention was just a treatment, while only God could determine whether her daughter would be cured, as also seen in Silbermann and Hassan’s (2011) work. Despite this, the mother believed that medical science had an active part to play in her daughter’s treatment and was firm that every intervention that might make cure more likely should be performed on her daughter.
This study has two key strengths. The population from which the participants are drawn is unique in terms of a study on the experiences of communication with children with cancer in the Palestinian context. Challenges of separation and isolation are likely to have been exacerbated for the eight children whose parents were unable to accompany their children. The process of getting a permit to access health care outside Gaza can be stressful and unpredictable process, and multiple applications may be required before permission to exit. Even then, some parents are never able to secure the permits they need to access care (World Health Organisation, 2019). This is a unique element in this study. Communication was explored in detail in its real-life setting (Broussard, 2006; Malterud, 2001; Miles and Huberman, 1994; Willig, 2001), and the qualitative research approach employed here was appropriate for gaining insight into the experience of communication, which is a topic of great complexity (Creswell, 2013; Cridland et al., 2014).
However, this study is not without limitations. The sample lacks variability, as participants were sampled according to availability, so this might affect the findings. Furthermore, the sample was dominated by children with cancer from Gaza (n = 8); however, at the time of the data collection, there was no specialised paediatric oncology centre in Gaza, so a high proportion of children were referred to the chosen oncology centre, further diminishing sample variability. In terms of financial issues, the majority of the carers who participated in the study came from poor families and had not been educated to the undergraduate level. Therefore, given their low level of education and low economic status, the carers might have paid more attention to secure the basic needs of children and their families, making communication a second priority to them. Thus, future studies might include parents with a higher educational level to understand their perspectives and experiences of communication. Although the study findings may be limited as they cannot be generalised, the participants’ experiences and insights appear to be transferable to other families who live in similar situations in the Palestinian context.
Implications for practice
The findings of the current study have several implications for clinical practice. Greater awareness of cultural factors is needed in order to improve clinical practice in cancer oncology (Aziz and Rowland, 2002; Gray et al., 2014). Mothers were unhappy about and avoided using the word cancer when discussing the disease, even in cases where the children were aware of their illness. Despite the recent trend emphasising the importance of parents communicating frankly with their children with cancer (Jalmsell et al., 2015; Wangmo et al., 2017), the findings of this study suggest that such frank communication is not accepted and embraced by all parents, particularly in cases where the children are terminally ill. Hence, aspects related to parental autonomy and cultural background should be considered in the communication strategies devised in the future. Nevertheless, the input of healthcare professionals must also be taken into account, particularly in cases where parents are not aware of how much their children know about their own illness. Therefore, parents and children can be helped to communicate better by making parents more aware of the protective tendency of the children and how the latter are mentally and psychologically impacted by such a tendency.
Conclusion
This study focused on understanding the experience of communication with children with cancer in one oncology unit in Palestine. Fifteen interviews with family carers of children with cancer were analysed, and the findings were discussed. The uniqueness of this study stems from the population from which the participants were recruited. The Palestinian context with its many political challenges added a new layer of complexity to the issue of communication with children with cancer. The findings demonstrated that the way in which carers communicated with children with cancer was dominated by the carers’ desire to protect the children. Given the medical advances currently being made, especially regarding the growing survival rates of childhood leukaemia, a reassessment of the optimal communication approach on a case-by-case basis is needed, taking into account the effect that carers’ cultural background has on such communication.
Footnotes
Acknowledgements
We would like to thank all of those who helped us during the completion of this research. This study could not have been accomplished without the contribution of the parents and their children who agreed to take part in this study. Their contribution is highly appreciated.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.