
Abstract
Siblings of children with chronic disorders are at increased risk of mental health problems. Predictors of siblings’ mental health require further study to identify children in need of interventions and to design effective intervention programs. Siblings of children with chronic disorders (n = 107; M age = 11.5 years; SD = 2.1, 54.6% girls) and their parents (n = 199; 50.3% mothers) were included in a survey study. Siblings and parents completed questionnaires on mental health. Siblings completed questionnaires on parent–child communication, relationships with parents, and an adjustment measure on the sibling situation. Multiple linear regression analyses were applied to identify predictors of siblings’ mental health. Sibling-reported relationship with parents was a significant predictor of sibling mental health reported by siblings, fathers, and mothers (R 2 = 0.26 - R 2 = 0.46). Siblings’ adjustment was significantly associated with fathers’ report of siblings’ mental health (r = .36), but not mothers’ report (r = .17). Siblings’ relationships (d = 0.26) and communication (d = 0.33) with mothers were significantly better than with fathers. We conclude that the sibling–parent relationship is a significant factor in identifying siblings at risk and that family-based intervention programs should be developed.
Introduction
Chronic disorders (CD) are characterized by the following core features: they are non-communicable (i.e., not passed from person to person), are permanent or long-lasting, and are mostly incurable (WHO, 2014). Chronic disorders in childhood represent a wide range of disorders and conditions, including both somatic illnesses (e.g., cerebral palsy and congenital heart disease) and neurodevelopmental disorders (e.g., autism and intellectual disability). In addition to the child with a disorder, CD also affect family members (Barlow and Ellard, 2006; Kazak, 1989), including siblings, who are often overlooked in both research and clinical services (Fjermestad et al., 2019). The current paper focuses on siblings of children with CD and their parents.
Growing up with a sister or brother with a chronic disorder impacts typically developing siblings (herein, siblings) (Parker et al., 2020; Sharpe and Rossiter, 2002; Smith et al., 2018; Vermaes et al., 2012). Studies have shown that siblings’ psychological experiences can be characterized by feelings of loss, grief, anxiety, loneliness, jealousy, anger, and guilt (Alderfer et al., 2010; Sharpe and Rossiter, 2002). Siblings may witness recurring acute medical situations and may be assigned extra caregiving and domestic chores responsibilities due to the child with CD (Lobato and Kao, 2002). They may also experience differential treatment due to the care needs of the child with CD (Sharpe and Rossiter, 2002). Review studies have shown that siblings are at increased risk of developing mental health problems (Jokiranta-Olkoniemi et al., 2016, 2019; Sharpe and Rossiter, 2002; Vermaes et al., 2012). The risk for internalizing problems (e.g., anxiety and depression) is somewhat higher than the risk for externalizing problems (e.g., conduct problems) (Vermaes et al., 2012). A longitudinal study showed that the increased risk of developing mental health problems for siblings is persistent across childhood and into adulthood (Giallo et al., 2014). In the current study, we examine sibling mental health conceptualized as emotional, behavioral, attention, and peer-related problems (Goodman et al., 2000).
In addition to siblings, CD in children also affect parents and their parenting. Studies have shown that parents of children with CD report significantly greater general stress than parents of children without CD (Cousino and Hazen, 2013; Pinquart, 2018). This is believed to be a result of extra care-taking challenges. Parents have to manage frequent clinical appointments, demanding treatment regimens, and behavioral and psychiatric problems that may occur as part of the CD (Dykens, 2000; Strømme and Diseth, 2000). Parents’ ability to provide adequate developmental support to siblings of the child with CD may be limited due to these extra burdens.
Childhood CD thus have direct effects on siblings and parents, and also on the parent–sibling system. Siblings may be affected by reactions of parental distress (pessimism regarding the future of the child with CD, problems because of excessive time demands, feeling incompetence as a parent or finding the role of parent less rewarding) (Fisman et al., 2000; Houtzager et al., 2004; Knecht et al., 2015; Vermaes et al., 2012). Furthermore, many of the risks are shared between siblings and parents. For example, both siblings and parents have to face worries about the child with CD, including fears associated with medical risks. The joint effect on siblings and parents is particularly evident based on findings regarding family communication. A review study showed family communication in families of children with CD is characterized by less openness and warmth than in other families (Murphy et al., 2017). Hence, there is a need for studies that look beyond sibling status alone and examine which factors may contribute to the potential risk for diminished mental health among the siblings of children with CD. Such knowledge can be applied to better understand the underlying mechanisms of risk and protective factors in order to identify those siblings who need interventions. Mental health problems in siblings may be due to combined risk related to various family factors such as differential attention, parental stress, and parental mental health problems (Incledon et al., 2015; Tudor et al., 2018).
To better inform the field and design interventions, the empirical research on risk factors for sibling mental health require theory-driven studies. As having a child with CD affects the entire family, it is appropriate to examine potential risk factors within the theoretical framework of family systems theory (Broderick, 1993; Minuchin, 2018). This theoretical framework highlights the importance of understanding the child or a disorder within a family and relational context, in which all members influence each other reciprocally. Tudor et al. (2018) presented an empirically based conceptual model that aligns with family systems theory (Tudor et al., 2018). In this model, siblings’ mental health is described as a function of the interplay between siblings’ relation quality, the symptom severity of the child with CD, and family social support, as well as maternal stress, depression, and differential attention from parents.
The current study builds on the framework proposed by Tudor et al. (2018). We have added three methodological features to advance the field and enhance the interpretability of our findings. First, we focus on a broader range of CDs than autism only. Second, we included both mothers and fathers. This is important because fathers are underrepresented in research on siblings of children with CD (Bogossian et al., 2019; Parent et al., 2017; Phares et al., 2005). Third, we included sibling self-report, and also linked their self-reports to mothers’ and fathers’ reports.
Aim and research questions
To identify predictors of sibling mental health, our first research question was: Do parental mental health, parent–child relationship quality, and/or parent–child communication quality predict mental health among siblings of children with CD? Our second research question was: Do maternal mental health, mother–child relationship quality, and/or mother–child communication quality predict mental health among siblings of children with CD differently from paternal mental health, father-child relationship quality, and/or father-child communication quality?
Methods
Setting and sample population
The population comprised families of children with various disorders, including autism spectrum disorder, cerebral palsy, congenital heart disease, Down syndrome, and rare genetic disorders. Most siblings and parents were recruited from one of two specialist centers, one for rare disorders and one for autism spectrum disorder. The remaining participants were recruited from the national user associations for either autism, cerebral palsy, congenital heart disease, or Down syndrome. Parents received information letters by regular mail. Written informed consent was obtained, and families were informed that participation was voluntary. The participants were not offered any financial incentives to participate. Participants were invited to an open trial of a joint parent–sibling intervention called “SIBS” focused on parent–sibling communication in Norway (Authors’ own). The current study reports questionnaire data from the baseline measurement (i.e., pre-intervention). Parents and siblings > 11 years of age received questionnaires and instructions by regular mail approximately 1 week prior to participating in the intervention. Siblings < 11 years of age completed the questionnaires when arriving at site for the intervention, with assistance of a project assistant if needed. The inclusion criteria were being the sibling (aged 8–16 years) of a child with diagnosed CD and having one parent available to participate. The exclusion criteria were diagnosed CD for the siblings and/or parents or bereavement of the child with CD.
The study was approved by and conducted in accordance with the guidelines of the local institutional review board for medical and health research ethics, the Regional Committees for Medical and Health Research Ethics, REC (proposal number masked for review).
Measures
Measures concerning siblings
The Strengths and Difficulties Questionnaire (SDQ) (Goodman et al., 2000) was used to measure siblings’ mental health. The 25-item SDQ is a measure of emotional, conduct, attention, and peer problems. Siblings, mothers, and fathers rate siblings’ mental health on a 3-point scale from 0 (not true) to 2 (certainly true) (e.g., “I am restless, I cannot stay still for long”). Adequate test-retest reliability, concurrent validity, and the ability to distinguish between community and clinical samples have been reported for the SDQ (Goodman, 2001; Goodman and Scott, 1999; Vostanis, 2006). The SDQ has been validated globally with several informant groups, ranging from normal populations to clinical populations (Deighton et al., 2014). In the current study, internal consistency for the SDQ was satisfactory (sibling α = 0.77; mother α = 0.84; father α = 0.76).
The Negative Adjustment Scale (NAS) (Lobato and Kao, 2002; Sahler and Carpenter, 1989) was used to measure siblings’ adjustment to the CD. The 18-item NAS is a modified version of the Sibling Perception Questionnaire (Sahler and Carpenter, 1989). The siblings rate the adjustment to having a child with CD on a 4-point scale from 1 (never) to 4 (a lot) (e.g., “I think a lot about my brother or sister`s disability or illness”), where siblings report interpersonal relationships, intrapersonal responses, fear, and communication related to the child with CD. Higher scores indicate poorer adjustment to being a sibling of a child with CD. Satisfactory internal consistency has been reported for NAS (α= 0.79) (Lobato and Kao, 2002). The NAS has been validated with siblings of children with various physical and mental disorders (Lobato and Kao, 2002; Orm et al., 2021; Sahler and Carpenter, 1989). In the current study, internal consistency for NAS was satisfactory (α = 0.75).
The Experiences in Close Relationships—Relationship Structures Questionnaire (ECR-RS) (Fraley et al., 2000) was used to measure the quality of siblings’ relationship with fathers and mothers, that is, reported once for each parent. The 9-item ECR-RS is a self-report instrument designed to assess attachment patterns in a variety of close relationships. Siblings rate their relationship with parents on a 7-point scale from 1 (correct) to 7 (incorrect) (e.g., “It is easy for me to trust my mother/father”). Satisfactory reliability has been reported for the ECR-RS (α= 0.88 to 0.92) (Fraley et al., 2011). The ECR-RS was developed based on a large population study with >20.000 adults (Fraley et al., 2011), but has also been used with adolescents in residential care (Costa et al., 2020) and non-clinical school-based child populations (Marci et al., 2019). In the current study, internal consistency for the ECR-RS was satisfactory (about mothers α = 0.78, about fathers. α = 0.76).
The Parent-Child Communication Scale—child version (PCCSc; Conduct Problems Prevention Research Group, 1994) was used to measure the quality of parent–sibling communication. In the present study, the 5-item “parent communication” subscale of the PCCSc was used. Siblings rate openness and problems in parent–sibling communication on a 5-point scale from 1 (almost never) to 5 (almost always) (e.g., “Do you talk with your mother about your problems?”) for both parents; this is reported once for each parent. The reliability of the PCCSc has been reported as being satisfactory (α =0. 75) (McCarty and Doyle, 2001; Pek, 2006). The PCCSc has been validated with high-risk and normative groups within a large child population study (McCarty and Doyle, 2001). In the current study, internal consistency for the PCCSc was satisfactory (about mothers α = 0.80; about fathers α = 0.82).
Measure concerning parents
The Symptom Checklist 90—R (SCL-90-R) (Derogatis, 1992) was used to measure parental mental health. The 90-item SCL-90-R is a self-reported inventory comprising nine symptom dimensions (i.e., somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, psychoticism, and “additional items”). Mothers and fathers rate items on a 5-point scale from 0 (not at all) to 4 (very much) , for example, “During the last week, how much have you been bothered by unwanted thoughts, words, or ideas that won`t leave your mind?”). A wide range of independent studies has shown satisfactory internal consistency for the SCL-90-R, and the scale has been validated with normal and clinical adult populations (α > .79) (Schmitz et al., 2000). In the current study, internal consistency for SCL-90-R (Global Severity Index) was satisfactory (mothers α = 0.96; fathers α = 0.97).
Data analytic plan
Initial analysis of skewness and kurtosis were run to examine data distribution (i.e., normality, and missing data). Further, data analyses were conducted in three main steps. First, we conducted descriptive analyses to identify median and interquartile ranges (IQR). Median and standard deviation were also calculated. Second, we ran correlation analyses between all study variables. Third, we conducted multiple regression analyses predicting siblings’ self-reported and parent-reported mental health (for siblings) from parent mental health and sibling-reported adjustment and relationship and communication quality (enter method; Jaccard et al., 2006). We controlled for the following background variables: sibling age, family economy, and parental education. Across variables, there was an average of 5.9% missing data. Little’s MCAR test indicated data were missing completely at random (X2 = 236.63, p = .149). Listwise deletion was used in all analyses. The data were analyzed using IBM SPSS, version 27.
Results
Background information about 107 siblings of children with CD.
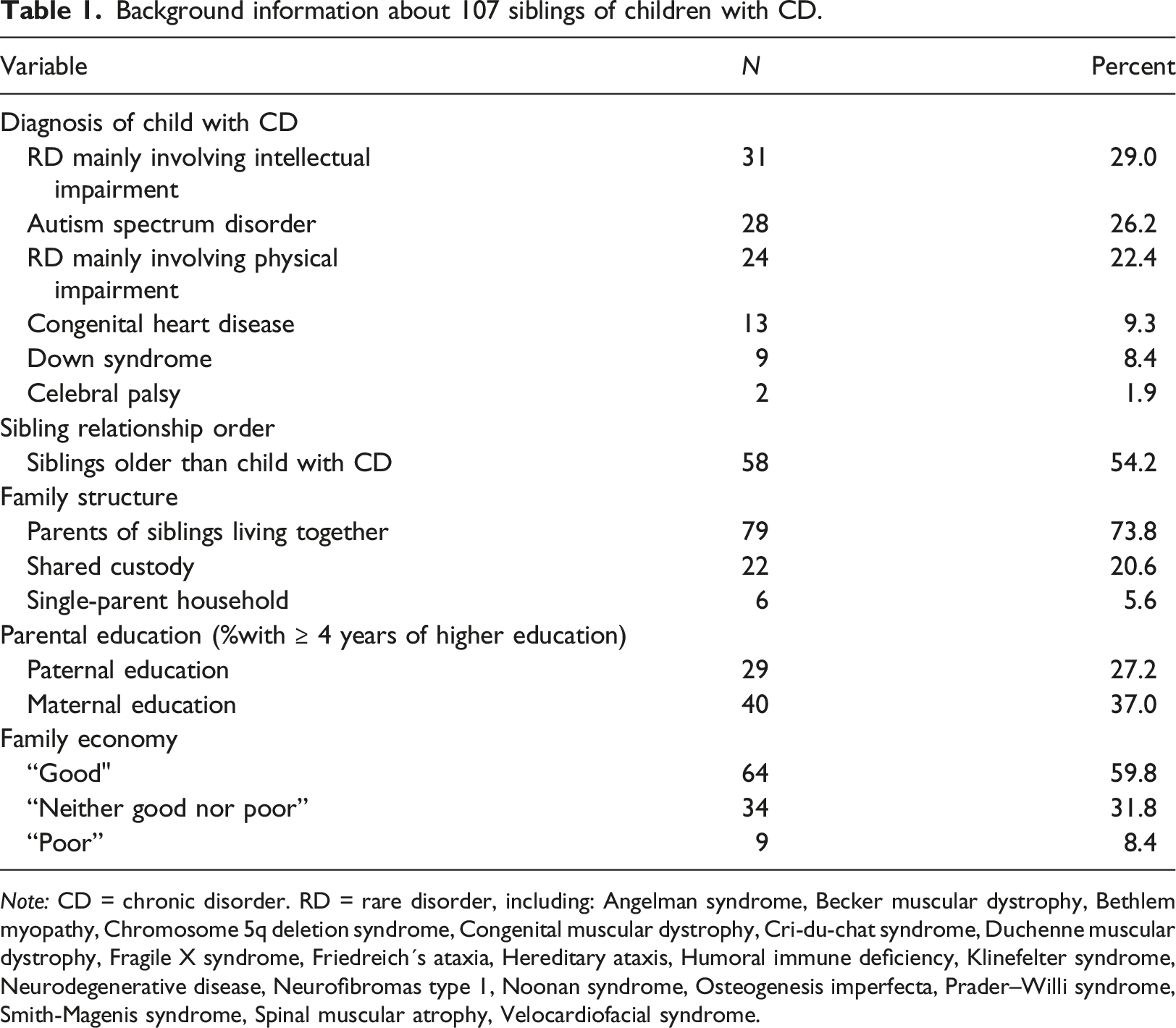
Note: CD = chronic disorder. RD = rare disorder, including: Angelman syndrome, Becker muscular dystrophy, Bethlem myopathy, Chromosome 5q deletion syndrome, Congenital muscular dystrophy, Cri-du-chat syndrome, Duchenne muscular dystrophy, Fragile X syndrome, Friedreich´s ataxia, Hereditary ataxis, Humoral immune deficiency, Klinefelter syndrome, Neurodegenerative disease, Neurofibromas type 1, Noonan syndrome, Osteogenesis imperfecta, Prader–Willi syndrome, Smith-Magenis syndrome, Spinal muscular atrophy, Velocardiofacial syndrome.
Study measures for 107 siblings of children with CD and their parents.
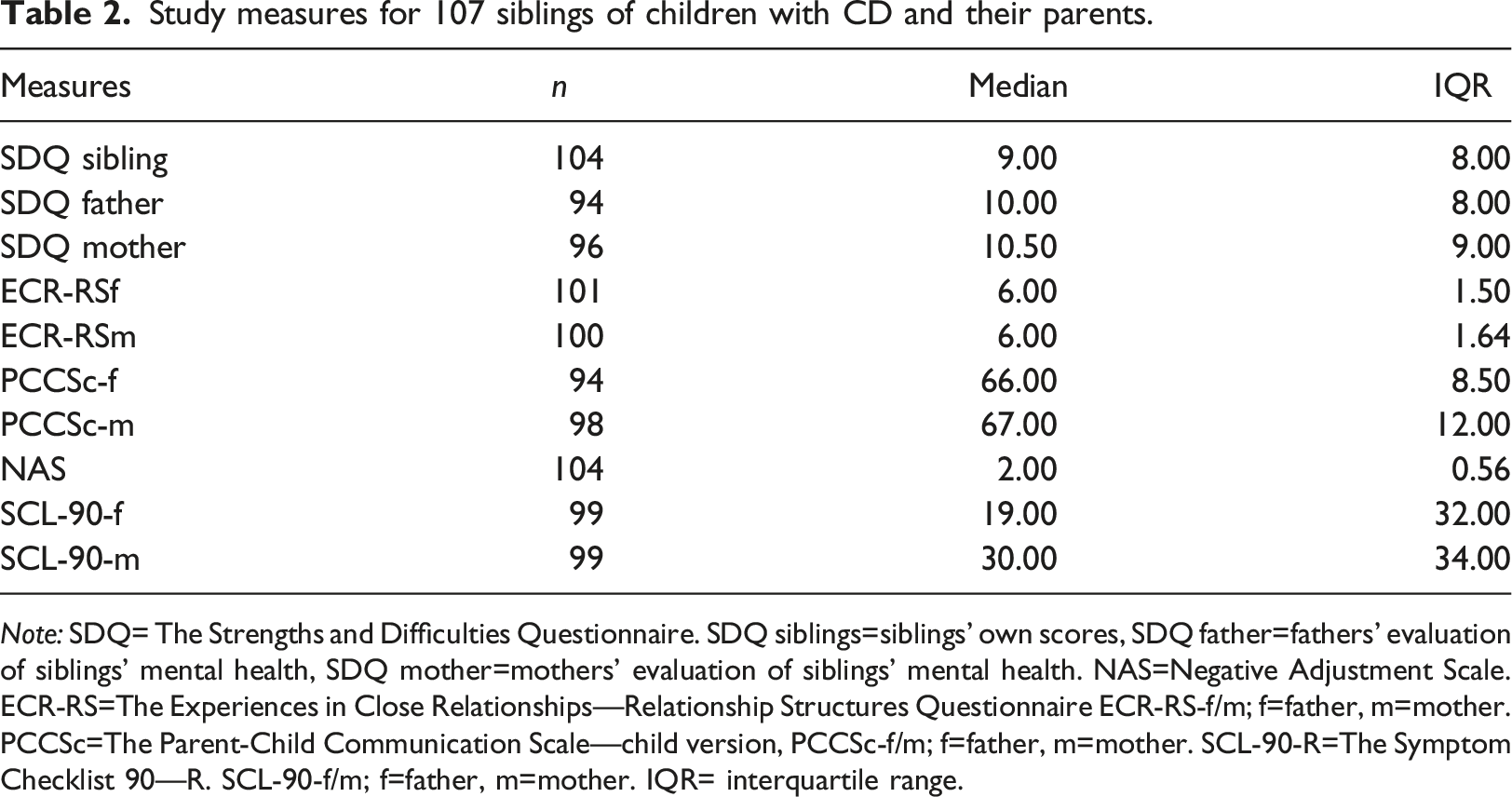
Note: SDQ= The Strengths and Difficulties Questionnaire. SDQ siblings=siblings’ own scores, SDQ father=fathers’ evaluation of siblings’ mental health, SDQ mother=mothers’ evaluation of siblings’ mental health. NAS=Negative Adjustment Scale. ECR-RS=The Experiences in Close Relationships—Relationship Structures Questionnaire ECR-RS-f/m; f=father, m=mother. PCCSc=The Parent-Child Communication Scale—child version, PCCSc-f/m; f=father, m=mother. SCL-90-R=The Symptom Checklist 90—R. SCL-90-f/m; f=father, m=mother. IQR= interquartile range.
Correlations between variables among 107 siblings of children with chronic disorders and their parents.

Note: Edu = education level. f= father. m = mother. SDQ= The Strengths and Difficulties Questionnaire. NAS=negative adjustment scale. ECR-RS=The Experiences in Close Relationships—Relationship Structures Questionnaire. PCCS=The Parent-Child Communication Scale. SCL-90-R=The Symptom Checklist 90—R. *significant at the p <.05-level. **significant at the p <.01-level.
Multiple regression models predicting mental health among 107 siblings of children with CD.
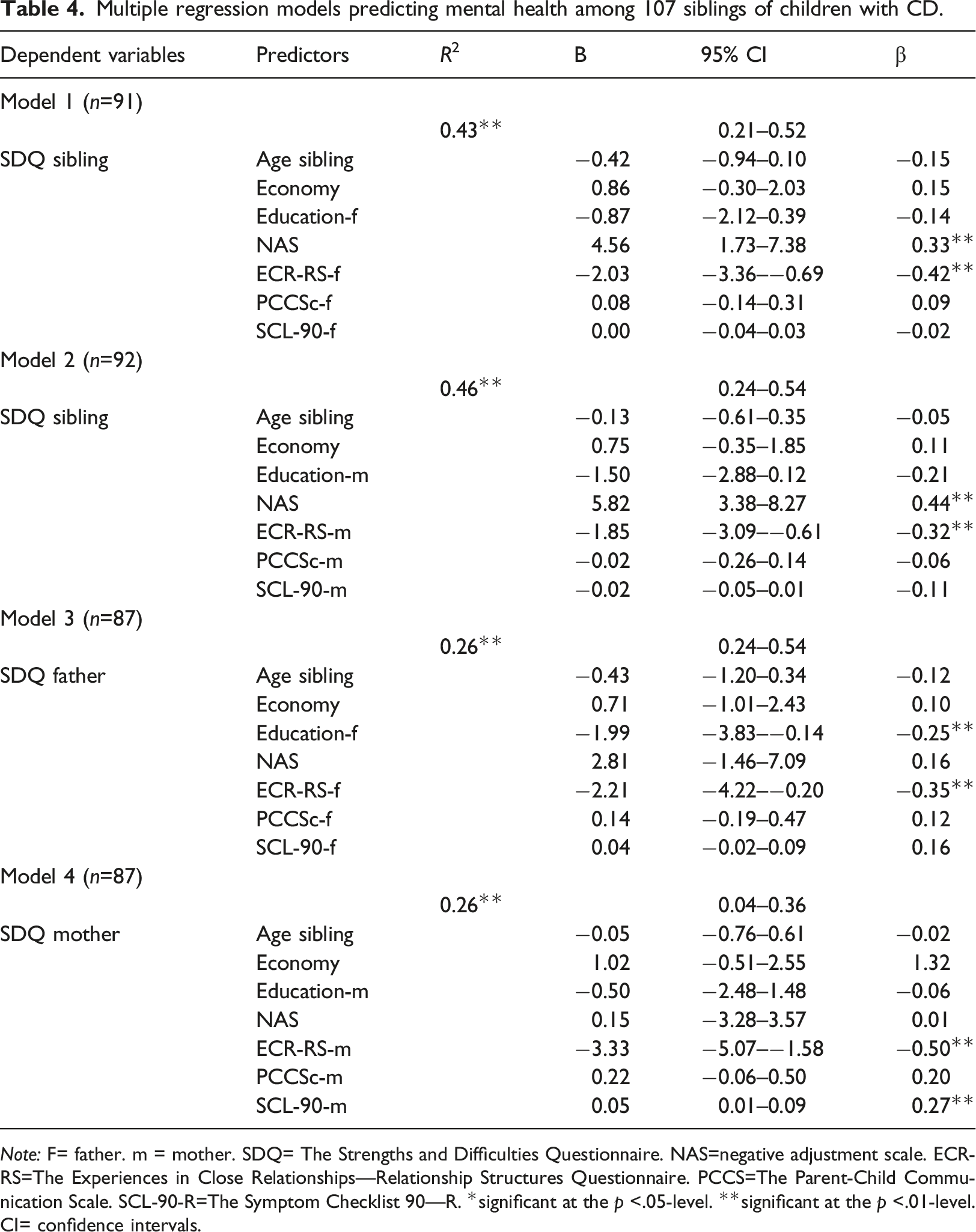
Note: F= father. m = mother. SDQ= The Strengths and Difficulties Questionnaire. NAS=negative adjustment scale. ECR-RS=The Experiences in Close Relationships—Relationship Structures Questionnaire. PCCS=The Parent-Child Communication Scale. SCL-90-R=The Symptom Checklist 90—R. *significant at the p <.05-level. **significant at the p <.01-level. CI= confidence intervals.
Discussion
The current study aimed to identify predictors of mental health in siblings of children with CD to point out which siblings may be at risk and to inform what types of clinical services may benefit them most. The predictors were selected based on family systems theory and included a uniquely tailored measure of sibling-reported adjustment (NAS) as a possible predictor. Our first research question was whether parental mental health, parent–child relationship quality and parent–child communication quality were significant predictors of siblings’ mental health. We identified two sibling-reported predictors of siblings’ mental health: Adjustment and relationship with parents. The finding that adjustment to the sibling situation was a significant predictor, implies that this specific measure on how siblings adapt to being a sibling as next of kin is an appropriate tool in identifying those in need of interventions. Because the adjustment measure used in the current study is tailored for siblings, it is not possible to compare scores with children who do not have a brother or sister with a CD. However, siblings reported only slightly elevated scores on the adjustment measure compared to possible maximum and minimum scores. The level of adjustment problems in this sample is equivalent to what was found in a comparable study (Lobato and Kao, 2002). Results indicate that the majority of the current sibling population adjusts sufficiently to the situation of being a brother or a sister of a child with CD.
The quality of parent–child relationship was a statistically significant predictor of siblings’ mental health across all study models. This finding aligns with other studies focusing on relational factors in understanding siblings’ needs (Deavin et al., 2018; Giallo and Gavidia-Payne, 2006; Incledon et al., 2015; Tudor et al., 2018). As demonstrated in Incledon et al. (2015) review, emotional support, particularly from parents, plays a protective role for sibling`s mental health
Parent–child communication was not a significant predictor of siblings’ mental health after other variables, such as parent–child relationship quality, were included in the model. This is in contrast to previous findings (Murphy et al., 2017). A possible explanation is that presently used questionnaire may capture dimensions beyond communication with items such as “Does your mother/father know how you are without having to ask you?” and “Do you talk about your problems with your mother/father?”. Such items may reflect the quality of the relationship more than (i.e., beyond) the communication quality. The correlations between the communication and the relationship scales were statistically significant and medium-sized to large. Also, the communication scale was highly correlated with the siblings’ self-reported mental health, which indicates that the questionnaire about parent–child communication was relevant to understanding siblings’ family functioning, although it was not a significant predictor in the regression models.
Our second research question was to examine whether maternal mental health, mother–child relationship quality, and/or mother–child communication quality predicted mental health among siblings of children with CD differently from paternal mental health, father-child relationship quality, and/or father-child communication quality. Mothers’ mental health predicted their reports about siblings’ mental health, whereas fathers’ mental health did not predict siblings’ mental health. A possible understanding of this finding is that fathers’ perceptions of siblings may be less biased by their own mental health compared to mothers. Since mothers tend to be the parent who does most of the follow-up tasks connected to the child with CD (Parent et al., 2017), fathers may spend more time with the siblings and thus be better able to see their functioning and needs. This speculation should be considered with caution, however, since the cross-sectional nature of our study means we cannot infer the causality of these associations. Furthermore, it is important to note that fathers reported significantly lower level of mental health problems than mothers. This lack of variance may explain why father-report was not a significant predictor. The siblings reported their communication and relationship with their mothers as significantly better than with their fathers. This may indicate that mothers, whose report about siblings’ mental health was predicted by their own report about mental health, are more emotionally attuned to the siblings compared to fathers. Further studies are needed to disentangle how mothers and fathers may play different (or similar) roles for siblings’ psychosocial health.
Our results highlight the importance of extensively exploring the aspects related to fathers and, therefore, including them in both further research and intervention programs. Another important issue to consider is that there are significant differences in how parental stress is manifested in mothers and fathers and not in the actual level of stress. This was found in a recent review of the literature on father`s parenting involvement and parental stress in families with a child with neurodisability (Bogossian et al., 2019). The difference in the manifestation of stress may affect children in different ways.
It is important to also consider the level of mental health problems identified in the current population. For the majority of participants, the mental health scores were reported below clinical cut-off. However, more than one in six siblings and almost one in three parents reported siblings’ mental health as being at least in the borderline clinical range. Previous studies also show that siblings report fewer mental health problems than parents do (about the siblings) (Sharpe and Rossiter, 2002; Vermaes et al., 2012). There are several possible interpretations why parents reported a higher level of mental health problems in siblings than siblings did. One possibility is that that siblings tend to underreport negative adjustment. If so, this could be due to a need to protect themselves and/or their parents (Malcolm et al., 2014). This may reflect problems in expressing emotions (Long et al., 2013) or be a result of a coping strategy of hiding emotions (Haukeland et al., 2015). The finding may also reflect young people`s general limitations in mentalizing their own situation (Dumontheil et al., 2010). Conversely, the finding may also indicate that parents overemphasize siblings’ problems. However, informant discrepancies between children and parents are the norm rather than the exception in child mental health studies (De Los Reyes et al., 2013; Korelitz and Garber, 2016). Thus, our findings underline both the importance of identifying relational predictors of mental health problems in siblings based on family systems theory and the necessity of using multiple informants in research on siblings.
This study`s strengths include a large sample with a considerable portion of fathers and siblings’ self-report on multiple measures. In addition, having both fathers’ and mothers’ report on how they perceive the siblings’ mental health, gives us a unique possibility to study cross-informant information. Furthermore, this study focuses on relational variables that are potentially malleable through intervention (e.g., The circle of security intervention, Hoffman et al., 2006, The SIBS intervention, Haukeland et al., 2020; Tuning in to Kids Havighurst et al., 2010). Such factors are especially important considering the aim of identifying factors that could be incorporated in preventive interventions.
Limitations
This study has some limitations, including the lack of a control group. The current study was an open pilot trial of a new sibling intervention, for which a controlled trial was the next step. However, even with a control group for the baseline measures used herein, we would not have been able to include sibling-tailored measures in a controlled design. This would have limited the value of control data. Second, the participants were recruited from specialist centers and user organizations. Thus, they represent families who actively seek support. This may have led to a bias toward families already concerned with and conscious of how their situations may affect the children without CD. That being said, all research requiring participant consent involve potential selection bias. Third, the families have relatively high socioeconomic statuses, which might also affect generalizability. This is likely to partly be a consequence of the study setting (i.e., user associations and a specialist center). Our invitations went out widely, and we aimed to reach participants across a wide socioeconomic range, However, just over half of those approached consented. Finally, the sample is a non-patient population. Using clinical questionnaires with this population may underestimate rather than reveal participants’ challenges. At the same time, however, the recruitment of families outside clinical settings might provide more representative data from a broader range of families of children with chronic disorders.
Implications for practice
This study has several implications for practice. First, as the parent–child relationship`s quality was the most consistent predictor of siblings’ mental health in the current study, we argue that interventions should target the relationship between siblings and parents. This can be done through targeted interventions, such as the SIBS intervention, which involves parents and is focused on family communication (Haukeland et al., 2020) or other family-oriented intervention programs (Besier et al., 2010; Lobato and Kao, 2002). Second, both parents should be involved in research on siblings’ mental health and sibling interventions. The results indicate that the mothers are more influenced by their own mental health than the fathers in their perception of the siblings’ mental health. Hence, mothers may potentially benefit from emotional support interventions such as support groups or individually focused psychotherapy. Within the framework of family systems theory and the consistent knowledge about maternal mental health as a predictor of child mental health (Goodman et al., 2011), promoting mothers’ mental health could affect siblings’ mental health positively. Different individual focused psychotherapeutic programs may be effective (Cuijpers et al., 2008) or alternatively more attachment theory-informed interventions like the Child–Parent Psychotherapy (Guild et al., 2021). Due to several links between siblings’ self-report and how their fathers report siblings’ mental health, we argue that fathers should be included both in further research on siblings and in interventions. Third, based on this study and other research aiming to assess siblings’ mental health, further studies should include questionnaires tailored specifically for the sibling population. Measures of siblings’ adjustment should be included in clinical practice to serve as a tool to promote siblings’ specific experiences, and to customize interventions in a way that acknowledge and show acceptance of siblings’ challenges. Together, these findings suggest at least two distinct factors that should be included in interventions toward siblings. Structure-wise, both parents should be involved in interventions. Content-wise, there should be a focus on relational quality and functioning in the family.
Conclusion
The relationship quality between siblings and parents together with adjustment to the sibling situation were significant predictors of siblings’ mental health and should therefore be applied to identify siblings who are in need of interventions. The relationship quality should also be addressed in interventions aiming at preventing mental health problems in siblings of children with CD. Mothers and fathers may influence sibling mental health in different ways. Hence, both mothers and fathers should be included in interventions as well as in further research on siblings’ mental health.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.