
Abstract
Children often experience hospitalization as stressful. To better understand children’s experiences, this current study involved interviews with and assessments of 17 children who were currently admitted at a U.S. children’s hospital. On average, they reported low levels of distress on the Facial Affective Scale (FAS) (M = .34) and moderate levels of anxiety on the Child Drawing: Hospital (M = 107.01). Results revealed themes in children’s experiences including stressors in the hospital, such as pain, disruptions to normalcy, and uncertainty. Children also reported factors that contributed to coping, including social support from parents and peers, and distractions from the medical routine such as leaving their hospital room. When children were grouped into clusters based on coping, those who were younger and who had received child life specialist services tended to be coping well. Regardless of understanding of diagnosis, those who demonstrated high levels of stress (distress and anxiety) in assessments tended to be categorized as not coping well. The findings inform interventions to support children’s coping during hospitalization.
Introduction
Child hospitalization tends to be stressful for children and their families (Ari et al., 2019; Claridge et al., 2020). Hospitalization is stressful not only because of physical pain and discomfort but also because it involves disruption to routines and exposure to scary or confusing procedures and equipment (Bsiri-Moghaddam et al., 2011). Children tend to report stress related to separation from caregivers and friends (Bsiri-Moghaddam et al., 2011) and report worry related to a lack of information (Lambert et al., 2013) and understanding of what might happen in the hospital (Jepnsen et al., 2019) and lack of participation in decision-making (Coyne and Kirwan, 2012). Taken together, the hospital environment is often stressful for children.
Long term, children tend to report negative memories of their hospitalization (Noel et al., 2017), and some children develop clinical symptoms of posttraumatic stress disorder following hospitalization (Triantafyllou and Matziou, 2019). In order to best support children during hospitalization and reduce long-term negative outcomes, it is important to identify factors that contribute to children’s stress in the hospital as well as resources that may help them cope better in the stressful context. Previous studies have highlighted that children report some positive views of the hospital (Jepnsen et al., 2019), and those positive areas may provide insights into how to best support children during hospitalization.
Factors that contribute to children’s experiences
Chronicity of children’s illnesses may impact their experience of hospitalization, both in terms of their experience of stress and their coping. Children with acute illnesses may struggle to understand their illness, medical terms, and procedures and experience anxiety in the unfamiliar hospital environment (Jepsen et al., 2019). Children’s previous experiences with hospitalizations and length of hospital stay may also contribute to their stress and coping: Children with chronic illnesses often have previous medical experiences that shape their future experiences in hospital settings (Thompson, 2009). They may have more opportunities to gain familiarity in the hospital setting; however, those with previous negative hospital experiences may demonstrate heightened anxiety when re-admitted (Ekra and Gjengedal, 2012). Experience of multiple hospitalizations can also contribute to loss of identity and isolation over time (Griffiths et al., 2011).
Children’s developmental capacities contribute to their experience of hospitalization and their ability to articulate their experiences (Marcinowicz et al., 2016). Young children (4–6years old) tend to value play activities (Lindeke et al., 2006) and report appreciating humor and fun in their interactions with staff (Marcinowicz et al., 2016). They also emphasize the importance of relationships and continuity in caregiving more than older children (Lindeke et al., 2006). When reporting on stressors during hospitalization, young children tend to emphasize pain and discomfort whereas older children highlight confusing communication, isolation, sleep issues (Lindeke et al., 2006), and issues of privacy and security (Marcinowicz et al., 2016).
Taken together, the reason for and length of hospitalization, as well as developmental stage may contribute to children’s hospitalization experiences and later outcomes.
Support for children during hospitalization
To support family- and child-centered care, the healthcare team often includes professionals who are trained to assist children and their families cope with the stress of hospitalization (Coyne et al., 2018). Child life specialists are one such member of the multi-disciplinary healthcare team who provide psychosocial support to children and families (Hubbuck, 2009). These specialists use therapeutic play to learn about children’s anxieties and explain diagnoses, prepare children for procedures, and provide coaching during medical interventions (Nabors and Liddle, 2017). Other hospital staff also play an important role in children’s coping (Farias et al., 2017). When nurses communicate clearly and kindly and are caring and helpful children feel more comfortable (Foster and Whitehead, 2019). Child-friendly and clear communication are related to children’s positive hospital experiences (Clarke, 2019).
Children also benefit from social support from parents, siblings, and peers (Farias et al., 2017; Nabors and Liddle, 2017). Children cope best with medical procedures when they are supported by their parents before, during, and after (Foster and Whitehead, 2019). Peers and siblings also play a critical role for providing emotional support and promoting psychosocial adaptation (Griffiths et al., 2011). Social interactions and opportunities for play help to normalize the hospital environment and help children feel more comfortable despite the stressors (Jepsen et al., 2019).
The child’s perspective
According to the United Nations Convention on the Rights of the Child (1989), children have a fundamental right to be listened to and to contribute to decision-making regarding their care. It is important to provide an opportunity for children to share their experiences of the hospital to promote child-centered practices during hospitalization (Clarke, 2019). Although parents can provide an adult understanding of their children and the context of the family, children’s voices offer additional insight into their perspectives and experiences in the hospital (Coyne et al., 2016). Children as young as 4 years old can describe their experiences (Gibson et al., 2010), although young children may engage more fully in creative participatory methods like drawing, and multiple methods of data collection may provide more comprehensive understanding of children’s experiences (Carter and Ford, 2013).
Existing studies have interviewed children about their experiences in the hospital (Bsiri-Moghaddam et al., 2011; Clarke, 2019), many from a quality improvement perspective to inform practices at specific hospitals (Lindeke et al., 2006) and often related to the quality of nursing care they have received (Fletcher et al., 2011).
Aim
To describe children’s experiences of stress, distress, and coping while in the hospital in order to identify factors that either promote stress or coping among children.
Research design and methods
Study design
This study employed a mixed-methods design wherein qualitative and quantitative data were collected concurrently, and the qualitative portion was given more weight (QUAL + quan; Leech and Onwuegbuzie, 2009). The qualitative data were treated as primary in addressing the research aim as the goal of this study was to describe children’s experiences in the hospital, and qualitative reports from children provide the most in-depth description. The quantitative psychosocial assessments and demographic data served to triangulate and contextualize the qualitative themes.
Setting and sampling
Participants were children between the ages of 4 and 15years old recruited as part of a larger study of parents’ and children’ experiences in the hospital. Families were recruited from the inpatient medical/surgical unit at a medium-sized, acute care children’s hospital in the Northwestern U.S. between January and October 2016. Potential participants were identified using a daily roster of all children ages 4–15 admitted at the time of the study. Each day of data collection, cases were randomly selected off the list using a random number generator, to determine the order in which patients were approached.
To be eligible to participate, children had to be currently admitted to the hospital and able to verbally communicate in English. The full study included 40 parent participants, of which 17 (54.8%) of their children agreed to participate in the qualitative interview and child assessments.
Data collection
Data collection began after the hospital ethics board reviewed and approved the study (Multicare Health System #15.23). Parents provided consent, and children provided assent to participate in the study. To maintain children’s confidentiality, they were assigned pseudonyms. Children participated in the interview as their parents were occupied with the parent portion of the larger study, and parents were asked to allow children to respond independently. Interviewers were either faculty or graduate students with expertise in child development, so although they used an interview guide, they used language appropriate for each child’s age, and followed the participants’ lead to make the interviews conversational. Children were assessed using the Facial Affective Scale (FAS) during the interview and were asked to complete the Child Drawing: Hospital (CD:H) task following the interview to assess their anxiety levels. Both assessments are described in detail in the measures section.
Measures
Semi-structured interview
The semi-structured interview had two overarching questions: The first explored the child’s understanding of why they were in the hospital, including questions about how they learned about their diagnosis, their understanding of their diagnosis, and their understanding of what would happen next in the hospital. The second overarching question assessed the child’s current emotional state. Children first indicated their current level of distress on the FAS (described below) and then were asked a series of follow-up questions about the reasons they were feeling that way, times in which they felt differently during their stay in the hospital, and things that would make them feel more comfortable in the hospital. Children provided varying levels of detail in their responses, and the interview portion of the study lasted between 5 and 30min. Interviews were audio-recorded.
Child distress
The Facial Affective Scale (FAS) is an established measure of children’s global distress (McGrath et al., 1996). The scale consists of sketches of nine faces, varying in level of distress, and children were asked to select the face that best represented them in the moment. Each face corresponds to a score between 1 and 9, where higher scores indicate more distress. The scale has previously been used with children age four and up and demonstrated strong convergent criterion validity such that scores on the FAS were correlated with those on the Faces Pain Scale (r = .46) and mechanical visual analogue measures of pain (r = .52–.77; Goodenough et al., 1999) and were also correlated with reports of anxiety and stress (r = .66–.76; Nilsson et al., 2014). The FAS has also demonstrated test–retest reliability with no significant changes in reports over three time points (Nilsson et al., 2014).
Child anxiety
The Child Drawing: Hospital (CD:H) was used to assess child anxiety (Clatworthy et al., 1999a). Investigators gave children a blank piece of paper and asked them to draw a picture of a person in a hospital. Drawings were evaluated using a scoring manual to calculate three subscale scores and a total anxiety score from 15 to 290, where higher scores indicate more anxiety (Clatworthy et al., 1999b). Clatworthy et al. (1999a) reports internal consistency among the subscales (correlations between .18 and .78, p < .10) and strong interrater reliability using the manual (Cronbach’s alpha among six raters for each of the subscales was between .71 and .95). The measure has demonstrated strong construct validity, with similar identification of anxiety in hospitalized children as the Missouri Children’s Picture Series (Sines et al., 1974).
Demographic characteristics
Parents reported their children’s age, gender, and race/ethnicity. The child’s length of current hospitalization and diagnosis were drawn from medical charts. Diagnoses were categorized as acute or chronic by two independent coders based on medical chart information, including diagnosis and number of past hospitalizations.
Data analysis strategy
Interviews were transcribed verbatim and verified by another researcher. Children’s responses to the FAS portion of the interview and their demographic characteristics were noted in the quantitative data set. Children’s drawings from the CD:H assessment were scored by three independent coders (strong interrater reliability; ρ = .84) using the CD:H scoring manual (Clatworthy et al., 1999b).
Investigators used inductive thematic analysis to identify themes and patterns in children’s interview data (Braun and Clarke, 2006). The process involved an open, axial, and selective coding procedure (Strauss and Corbin, 1990). To contextualize interview responses in terms of children’s developmental stage, children’s ages were included on transcripts during analysis. First, both authors became familiarized with the data, and using an open coding approach, authors read through the transcripts and coded everything the participants said using both descriptive and in-vivo codes, independently and one interview at a time. Once consensus in coding scheme was reached, the remaining transcripts were coded independently by one investigator each. In the axial coding phase, investigators independently identified initial higher-level themes that encompassed the open codes in each interview and then met to compile themes across all interviews. Finally, the investigators used selective coding to review and organize the axial themes into overall core themes that represented the central experiences of participants. Presented results reflect themes perceived to be robust and broadly representative.
Based on an inductive thematic analysis framework (Braun and Clarke, 2006), themes should be developed in a process directed by the content of the data. As such, in the process of developing and reviewing themes the authors noticed patterns among those participants who, based on a subjective evaluation, seemed to be coping well versus those who were struggling to cope with the hospitalization. Researchers also noticed that some children had clear understandings of the reason they were in the hospital while others were less clear about their diagnosis or prognosis. As such, participants were sorted into clusters based on the two factors (coping and understanding of diagnosis) to identify whether there were patterns among children who fell into each cluster. Researchers independently categorized children into coping and understanding of diagnosis categories, and when there was disagreement, they each re-read the transcript and discussed the child until a consensus about cluster was achieved. Criteria used to classify children and example quotes are included in Table 3. After children were categorized into clusters, researchers examined demographic characteristics and distress and anxiety assessment data for each cluster. This process resulted in four clusters of participants with varied demographic and psychosocial profiles.
Findings
Participant demographic characteristics.

Qualitative findings
Qualitative themes and additional exemplar quotes.
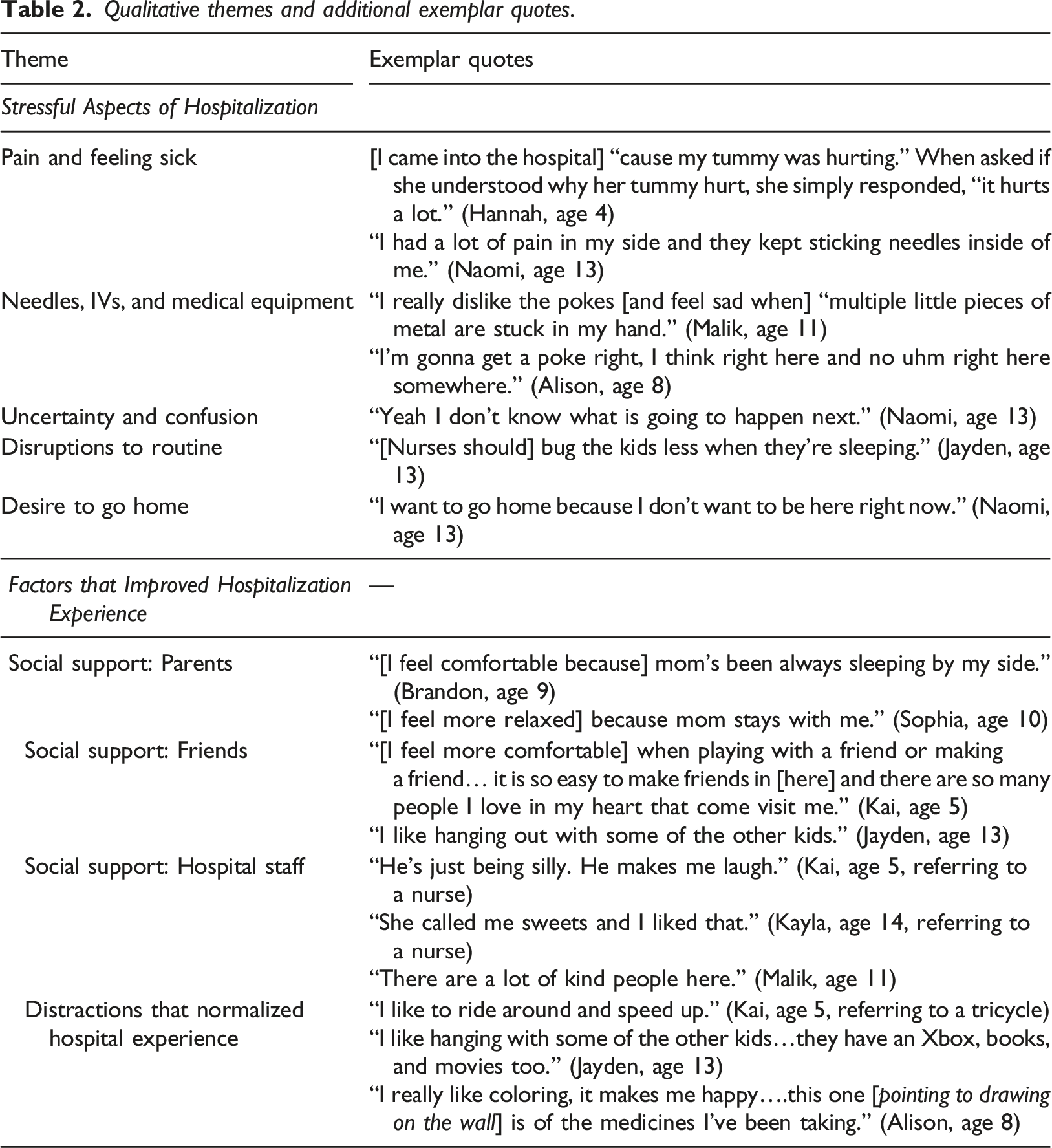
Stressful aspects of hospitalization
Pain and feeling sick
Most children described some level of pain, typically related to their illness or discomfort with needle pokes or IVs. For some of the younger children, pain was described as the reason they came to the hospital or the moments they felt the worst. Other children discussed times when they felt especially bad while hospitalized, typically related to physical symptoms of their illness and painful procedures: (Table 3) “I was crying and stuff like that because my throat and neck hurts.” (Kayla, age 14) Patterns in coping and understanding of diagnosis based on cluster-grouping of participants. Note: Table illustrates patterns. Not all children who fell into each cluster represented all patterns listed.
Needles, IVs, and medical equipment
Children often indicated IVs or needle pokes were among the most stressful aspects of hospitalization. Children recalled past experiences of needle pokes as well as stress related to anticipation of future medical intervention. Children also often commented on medical equipment when asked about the most stressful aspects of hospitalization: “I was scared of taking that thingy out.” (Hannah, age 4, referring to chest tube)
Uncertainty and confusion
Children discussed the stressful aspects of uncertainty and confusion regarding their health care experiences. When children were asked if they knew the reason for their hospitalization, some indicated they were not sure why they were in the hospital: “I don’t know why I’m here.” (John, age 12)
Other children described feeling uncertain about the next steps of their hospitalization. Feelings of uncertainty and confusion consistently contributed to stress during hospitalization.
Disruptions to routine
Some children reported struggling with changes in their routine and disruptions to sleep. Children reported being bothered by the nurses who checked their vitals throughout the night and struggling with shifts in bedtime and other daily routines: “I am not used to going to bed at that time…someone woke me up in the middle of the night.” (Brandon, age 9)
Desire to go home
Many children reported feeling a strong desire to leave the hospital and go home. Most children indicated missing aspects of home life: “I really wanna go home. I miss my friends, and my school.” (Alison, age 8)
Others simply expressed a desire to not be in the hospital.
Factors that improved hospitalization experience
Children also described factors that reduced the impact of the stressors and made their hospital experiences tolerable.
Social support
Children described multiple forms of social support that improved their experience in the hospital, including support from parents, friends, and hospital staff.
Parents. Children indicated parents’ presence in the hospital and involvement in their care reduced their stress. Several children indicated their parent being with them in the hospital made them feel more comfortable. Children also indicated parents helped them understand their diagnosis and actively helped them cope with their stressors: “I learned it from the best of the best [pointing at mom]…the most specialist person is my mom.” (Kai, age 5).
Parents’ presence and support was consistently discussed as a factor that helped children cope.
Friends. Many children discussed their friends, both in terms of missing their friends at home and enjoying opportunities to interact with friends in the hospital. Children indicated visits from friends and opportunities to play with other hospitalized children made them feel comfortable: “[I feel best] when people [are] here to play with me.” (Sophia, age 10)
Hospital staff. Several children mentioned the hospital staff when asked about what made them feel relaxed or comfortable in the hospital. Staff made them laugh, built relationships with them, taught them coping skills, and interacted with them in kind ways: “A psychiatrist that uhm that helps me relax all my worries…..She [taught] me breathing exercises. It’s easier for me now.” (Jane, age 10)
Children consistently appreciated positive interactions with hospital staff and felt those interactions made the experience of hospitalization more tolerable.
Regardless of its form, social support seemed to play an important role in almost every child’s narrative of the aspects of the hospital experience that had been comfortable.
Distractions that normalized hospital experience
Children described distractions that made their hospital experience feel more like typical life. Many of the children discussed the playroom, teen room, and other trips outside of their room as important distractions. These opportunities to leave their hospital room were helpful distractions and provided a break from their typical hospital life. Children also discussed enjoying opportunities to engage in activities like art, board games, video games, and movies: “I usually play games with playdough and I really like painting.” (Mariah, age 7) “[It’s better] when I have things to do and having places I can go to take breaks [like] the playroom with the kids [and] the TV room that I go to.” (Sophia, age 10)
These activities seemed to offer children a distraction from the typical routine of their hospital stay and also provided some semblance of normalcy for children.
Cluster patterns
As illustrated in Table 3, participants were fairly evenly distributed among the four clusters: Cluster 1: Coping well, understands diagnosis (n = 5); Cluster 2: Coping well, does not understand diagnosis (n = 3); Cluster 3: Not coping well; understands diagnosis (n = 5); and Cluster 4: Not coping well; does not understand diagnosis (n = 4). After categorizing children into the clusters, quantitative data (demographic characteristics and distress and anxiety assessments) were examined for each cluster. Several differences emerged among the children who ended up in each cluster in terms of their age, reason for being in the hospital, number of days in the hospital, receipt of child life services, and levels of anxiety and distress.
Cluster 1: coping well, understands diagnosis
Of the five participants who were categorized as coping well and understanding their diagnosis, four of the five were between 9 and 11 years old. The majority of the children in this cluster had chronic illnesses and had been admitted two or fewer days. All but one of the participants had received child life services during their current hospital stay, and most reported low distress during the FAS task. There was not a clear pattern in terms of child anxiety in this cluster.
Cluster 2: coping well, does not understand diagnosis
The three participants in Cluster 2 were younger than those in Cluster 1 (ages 4–8) and were all hospitalized for acute illnesses. They had been admitted longer (between 3 and 10 days), and all three had received child life services. There was not a clear pattern in terms of distress or anxiety scores among this cluster.
Cluster 3: not coping well, understands diagnosis
Four of the five participants in Cluster 3 were adolescents (ages 12–15), and one was 6years old. Each had been admitted two or fewer days, and all but one had not received child life services. They reported high distress during the FAS task and high anxiety during the child drawing task. There was not a clear pattern in terms of illness chronicity.
Cluster 4: not coping well, does not understand diagnosis
In Cluster 4, participants were again primarily adolescents (four were ages 11–14 and one was 6years old) and all but one participant was hospitalized for acute reasons. Each had been admitted two or fewer days. They all reported high distress during the FAS task and high anxiety during the child drawing task. There was no pattern in terms of receipt of child life services.
Summary of cluster patterns
Taken together, the participants who were categorized as “coping well” (clusters 1 and 2) tended to have received child life services during their current hospitalization. Those coping well who understood their diagnosis tended to be older and were more likely to have chronic illnesses than those who were coping well but did not understand their diagnosis. Conversely, participants who were categorized as “not coping well” (clusters 3 and 4) tended to be older children (early to late adolescents) who had been admitted for two or fewer days. They reported high distress and anxiety, which was consistent with their qualitative narratives that led us to categorize them as “not coping well.” The participants who were categorized as “does not understand diagnosis” (clusters 2 and 4) tended to be hospitalized for acute reasons. Those who were categorized as “understands diagnosis” (clusters 1 and 3) tended to be older children (over 9years old), suggesting developmental stage may contribute to understanding and ability to articulate diagnoses.
Discussion
The aim of this study was to describe children’s experiences of stress, distress, and coping while in the hospital. Using interviews and assessments, children in this study were able to identify stressful aspects of their hospitalization experience and also discuss factors that improved their experience. Children reported stress related to pain, fear of medical equipment, disruptions in routine, uncertainty, and missing home. Factors that promoted coping included opportunities to leave their room and social support from parents, friends, and hospital staff.
Existing research has largely focused on the impact of nursing staff on children’s experiences. Foster and Whitehead (2019) highlighted children’s reports of positive, supportive experiences with nurses where they felt safe and listened to as well as negative interactions where children felt excluded and scared. Children in the current study described interactions with nursing staff that were kind, friendly, and made them feel comfortable. In addition to support from nurses, children in this study discussed support and care from parents, peers, and other hospital staff. Existing literature indicates children tend to cope best when parents are present to support them, help interpret the situation, and actively teach their children coping skills (Jepsen et al., 2019). Similarly, children in the current study not only revealed their parents helped them feel comfortable simply by being present, but they also played an important role in educating children about their illness and supporting development of coping skills. In addition to parental support, children in this study indicated the importance of peer support from friends they met at the hospital and friends from home. Similarly, previous studies have highlighted the anxiety and worry that results from disruption to peer relationships (Bsiri-Moghaddan et al., 2011) and crucial role of friendships in providing support (Hicks et al., 2013). Taken together, these findings highlight the value of various forms of supportive relationships for children in the hospital.
Much of what children reported as stressful was consistent with previous literature. In the current study, almost every child discussed some level of pain, discomfort, or fear of medical equipment and procedures. Similarly, Bsiri-Moghaddan et al. (2011) found children reported pain, anxiety about procedures, and dissatisfaction related to the medical environment and equipment. Studies have also highlighted separation and isolation as negative aspects of hospitalization (Clarke, 2019). Likewise, children in this study consistently reported missing friends, school, and home. Children in this study reported both positive and negative aspects of disruptions to their routine: Disruption to routine in the form of activities or leaving their room made the hospital more tolerable. Conversely, disruptions such as vital checks in the night or changes in sleep routine added to children’s stress. Previous literature has indicated lack of control as the source of stress from similar negative disruptions (Jepsen et al., 2019). Perhaps, children gain a sense of control when given the option of participating in positive disruptions of routine and are able to engage in play activities that feel familiar. Having diverse activity options and supplemental rooms designed for different age groups such as the teen room and playroom may give children opportunities to make choices and feel in control.
Findings highlight an important role of child life specialists in children’s experiences in the hospital. Cluster patterns revealed the majority of children who were categorized as “coping well” had received child life services, and many of those children also were categorized as “understands diagnosis.” This clear pattern related to child life specialist services supports existing literature examining child life specialists’ role in helping children cope with specific procedures. For instance, children who receive child life services tend to display less fear when undergoing medical imaging (Tyson et al., 2014) and indicate lower levels of anxiety when they receive preoperative preparation by a child life specialist (Brewer et al., 2006). This study adds to the small but growing literature documenting the positive role of child life services in pediatric hospitals, as much of the previous literature has largely focused on nursing (Fletcher et al., 2011) and hospitalization outside of the U.S. (Marcinowicz et al., 2016) where child life specialists are less commonly employed. The cluster analysis also revealed younger children in the current study tended to be coping better than adolescents. The experience of hospitalization may be more difficult for older children and adolescents (Marcinowicz et al., 2016), who tend to be more peer-focused than younger children who rely more on their caregivers. It is also possible that children’s hospitals are better equipped for younger children and may need to provide more specialized coping support for adolescents.
Limitations
This study was limited in several important ways. Although parents were asked not to participate in their children’s interviews, their presence in the hospital room may have impacted children’s responses. The hospital environment itself was also a difficult environment for interviews with many interruptions and distractions such as loud medical equipment and medical staff interruptions. Many children declined to participate in the study because they were tired or uncomfortable, so it is possible this study did not capture experiences of children in the most distress. Conducting interviews with young children was challenging as children often engaged in the interviews as a back and forth conversation, so it was difficult to capture long narratives, and instead, the presented quotes are statements from the broader conversation with the interviewer. In this way, the interviewers led the interviews more than they would have with adult participants. Future studies may opt to use more participatory methods to engage children (Foster and Whitehead, 2019).
The cluster patterns represented the small group of children in this study and should be considered preliminary and not generalizable. Each cluster only contained a small number of children, and the patterns should be explored in more depth among a larger sample. The results of clustering indicated that most adolescents were categorized as “not coping well” and this could be due to their reluctance to discuss their experiences; many of their interviews were shorter and less revealing than those with younger children. This contrasts previous literature (Lindeke et al., 2006) that suggests adolescents typically provide more detail in interviews than younger children. Also, interviewers only met with the children at one point in time, and this time varied for children in terms of their length of time in the hospital. The variation may have impacted children’s responses.
Finally, the authors’ own identities, experiences, and expertise contributed to these findings. Both authors have training in child development and family systems and may have entered the inductive analysis with assumptions, particularly about typical development and the importance of family and other supports. One of the authors is also trained in child life, and the broader study was originally intended to examine the efficacy of child life services. The inclusion of receipt of child life services as a variable and the author’s experience may have biased the analyses as well.
Implications for practice
These findings have implications for practitioners working in children’s hospitals. Healthcare professionals should regularly ask children directly about factors causing them stress and factors that would make their stay easier. Children in this study indicated enjoying positive distractions from the hospital routine that provided opportunities for them to be in control. Further, adolescents may need more or different intervention as they may be particularly negatively impacted by the hospital environment. Finally, children may benefit from individualized psychosocial care, like that provided by child life specialists, that involves parents and siblings, to help them process their stressful experiences of hospitalization.
Conclusion
The findings of this study indicate children can provide helpful insight into their hospital experiences, and their voices should inform decisions that shape children’s healthcare. Specifically, children can articulate aspects of hospitalization that are difficult and aspects that make their stay easier. It is not always possible to avoid the negative experiences of pain and discomfort related to medical procedures and illness; however, it is possible to implement support strategies to make hospital experiences more comfortable for children. Children in this study highlighted the value of having parents nearby, interacting with peers, having opportunities to leave their room, and receiving care from supportive nurses, doctors, and child life specialists. Based on these findings, children’s hospitals should strive to offer fun, positive disruptions from children’s medical routine, including opportunities for play outside of the hospital room whenever possible.
Footnotes
Acknowledgements
This research would not have been possible without the collaboration and support of the healthcare staff at Mary Bridge Children’s Hospital or the willingness of children and families to participate and share their experiences. Thank you also to Lindsay Montgomery and Brittany Knapp who participated in the collection of this data.
Declaration of conflicting interests
The authors(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by funding from the Central Washington University School of Graduate Studies and Research.