
Abstract
Children with physical disabilities are less physically active than children with typical development. How children’s experiences of using walkers relates to their physical activity has not been studied previously. This study aimed to explore perspectives of walker use and their potential to increase physical activity. Four focus groups were conducted with children aged 7–10 (n = 3; 12.5%), aged 9–12 (n = 4; 16.7%), parents (n = 7; 29.2%) and paediatric physiotherapists (n = 10; 41.7%). Groups were audio recorded and transcribed. Data were analysed using framework analysis. An overarching concept of walkers needing flexibility to accommodate individual, interpersonal and environmental variability was underpinned by three themes: (a) contrasting drivers for use/non-use of walkers, (b) trade-offs, (c) acceptance of technology within walkers to increase physical activity. Participants were motivated by differing drivers: social for children, emotional for parents and professional for physiotherapists. These contrasting drivers create trade-offs, for example between quality of movement and independence. To maximise physical activity, walker prescribers and designers should prioritise drivers that motivate children and parents, ensuring goal setting is family-centred and participation orientated. Involving families in co-designing walkers is therefore important. Individual clinical assessment allows for identification of children’s specific needs and how a child’s, parent’s and physiotherapist’s goals may differ.
Keywords
Introduction
Children with physical disabilities are less physically active than children with typical development (Li et al., 2016) and spend more time sedentary (Ganz et al., 2020). There is evidence that this difference in physical activity levels has widened during the covid-19 pandemic (Activity Alliance, 2021). Benefits of physical activity for children with physical disabilities include social development, motor skills, muscular strength, increased walking/cycling/running speed and improved mobility (Smith et al., 2022). Sedentary behaviour is associated with cardiovascular risk factors in children including obesity and higher blood pressure (Canabrava et al., 2019). Considering benefits of physical activity in the context of a biopsychosocial model of health, recognising that increased involvement in leisure time physical activities also increases participation and fulfilment of social roles, is important (Reedman et al., 2019). Current evidence suggests goal-directed, participation-based interventions, which are family-orientated and take personal, contextual and environmental factors into account, are more effective for increasing physical activity than impairment-focused approaches (Reedman et al., 2019).
Factors which influence participation in physical activity for children with disabilities are complex, and can act as barriers or facilitators (Bloemen et al., 2015). They include self-efficacy, physical fitness, increasing age, availability of equipment and local facilities (Bloemen et al., 2015). A qualitative literature review exploring out-of-school life of children and young people with physical disabilities in the United Kingdom described barriers limiting access to activities, which included training needs, accessibility issues, parental influences and attitudes of others (Knight et al., 2013). The voice of young people was notably absent from included studies.
Finding strategies to increase physical activity for children with neurodisabilities has been identified as a research priority (Morris et al., 2015). Reducing sedentary time is also recommended for children with cerebral palsy (CP) (Verschuren et al., 2016), but there is an evidence gap in relation to the associations between health outcomes and sedentary behaviour for children with disabilities (Smith et al., 2022). Recently published physical activity guidelines for children and young people with disabilities (United Kingdom) state that 120–180 min of aerobic physical activity per week at moderate-to-vigorous intensity should be undertaken, through activities such as walking or cycling (Smith et al., 2022).
Time spent using a walker (an assistive device that supports children with disabilities to move independently) increases physical activity and reduces sedentary time. Children with disabilities may use walkers to mobilise or during physiotherapy. Wheeled walkers include hand held walkers, such as anterior or posterior walkers (Poole et al., 2017), and support walkers. Support walkers (or gait trainers) provide additional support for the trunk, pelvis or head.
Increased physical activity is the most common perceived benefit of walker use (George et al., 2020). Some weak evidence suggests walkers increase walking distance/number of steps (Paleg and Livingstone, 2015). A survey of children who use wheeled walkers and their parents/guardians highlighted that improvements could be made to weight, adjustments and repair/maintenance of walkers (Gudjonsdottir and Gudmundsdottir, 2021). Improving families’ experiences could encourage more frequent walker use and result in increased physical activity.
We were interested in stakeholders’ views on whether using technology to provide feedback about walker use and to deliver behaviour change techniques may increase children’s physical activity. E-Health behavioural interventions to increase physical activity are effective for young adults (Oosterveen, 2017). Also, interventions combining technology and behaviour change techniques such as prompts, cues, self-monitoring and goal setting reduce sedentary time in adults (Stephenson et al., 2017; Oosterveen, 2017). Incorporating active video gaming interfaces into walkers may motivate children to be more active (Glegg and Levac, 2018).
Involving children with disabilities in participatory design of assistive technologies reduces the risk of new technology being abandoned, by ensuring it reflects their priorities (Vasalou et al., 2021; Petrie et al., 2018). We thought that working with children, parents/guardians and physiotherapists, using a co-creation approach (Greenhalgh, 2016), would produce effective and acceptable equipment. Professionals’ perspectives are likely to differ to those of children/parents (Mortenson and William, 2008), and are also important to capture.
Recent surveys exploring parents’ perspectives of children’s use of mobility devices and their impact on participation (Gudjonsdottir and Gudmundsdottir, 2021), and professionals’ use of support walkers in clinical practice (George et al., 2020), highlighted a lack of studies relating to children’s use of walkers. In a systematic review of outcomes of children’s gait trainer use, Paleg and Livingstone (2015) emphasised that existing evidence is mainly descriptive, and is insufficient in offering firm conclusions. No previous studies have consulted children, parents or physiotherapists about how walker design influences children’s participation or whether technology to provide feedback on and to motivate children to do more walking would be worthwhile.
Aims
This study aimed to: (1) explore experiences of walker use from the perspective of children with neurodisabilities, their parents and physiotherapists, including physiotherapists’ decision-making processes; (2) seek children’s, parents’ and physiotherapists’ opinions about the potential of improving walkers to increase physical activity, including making educational, sporting and leisure activities more accessible.
Methods
Study design and setting
A qualitative approach was appropriate for this study’s exploratory nature. ‘Standards for Reporting Qualitative Research’ have been followed (O’Brien et al., 2014). Focus groups were held with children, parents and physiotherapists to capture interaction between participants and generate novel ideas (Plummer, 2017). Focus groups are an effective method for involving children in research, if an informal environment that reduces power imbalances can be created (Adler et al., 2019). Data were analysed using framework analysis (Ritchie et al., 2014).
Deciding where to conduct research involving children is context specific and participants’ needs are key (Adler et al., 2019). Clinical settings can emphasise the patient-professional relationship (Adler et al., 2019). Public and patient involvement work during protocol development informed decision-making around holding children’s and parents’ groups at frame football clubs (set up to enable children who use walkers to play football with and against each other).
Study sample and recruitment
Purposive sampling was employed (Plummer, 2017). Children and parents were recruited by physiotherapists working for a community NHS Trust and via two frame football clubs. Physiotherapists attending training hosted by the Association of Paediatric Chartered Physiotherapists were invited to participate.
Inclusion criteria were
(1) Children with neurodisabilities aged 7–12 years who use a wheeled walker, or parents/guardians of children under 18 years of age who have neurodisabilities and use a wheeled walker, or paediatric physiotherapists who prescribe walkers. (2) Appropriate communication skills for participating in a focus group.
Exclusion criteria were
(1) Children under seven and over 12 years of age. (2) Children or parents/guardians of children who use sticks or crutches only, not a wheeled walker. (3) Participants requiring additional support to communicate. (4) Physiotherapists who have not prescribed children’s walkers.
To capture experiences of children with communication difficulties and a broader age range, parents/carers could participate even if their child had not taken part.
Children aged 7–12 years were included because gross motor function plateaus at 7 years of age in children with cerebral palsy and they become more vulnerable to reduced physical activity (Rosenbaum et al., 2002). Younger children can be less confident contributing in a group and older children may have stronger opinions about their equipment as their independence grows.
Small group sizes and narrow age ranges are recommended when conducting focus groups with children (Shaw et al., 2011). As we planned to hold two small groups, recruiting older children would have unacceptably widened age ranges.
Public and patient involvement in protocol development informed the decision that a maximum of 10 participants would attend focus groups for adults.
Data collection methods and procedures
One group was held for each of the following: (1) children aged 7–10, (2) children aged 9–12, (3) parents of walker users, (4) paediatric physiotherapists.
The second children’s group was intended to be for children aged 10 and over, however, recruiting 10–12 year olds was difficult. Time and resources limited the number of groups held. Our aim was not to reach data saturation, but to draw on a range of perspectives. Data collection took place between June and November 2017.
The lead facilitator and second author was a senior research fellow (PhD) with experience of research with children. She was unfamiliar with this subject area. She had no pre-existing relationships with participants. The second facilitator and corresponding author was a paediatric physiotherapist and clinical researcher (MRes). She worked in NHS community services and had undertaken previous research relating to children’s walkers (Poole et al., 2017). Two children, two parents and six physiotherapists who participated had been either on the second facilitator’s caseload, were participants in her previous research or were local colleagues.
To reduce power imbalances between adult facilitators and children participating, researchers dressed casually and sat on the floor (Shaw et al., 2011).
Data collection procedures for each group of participants.
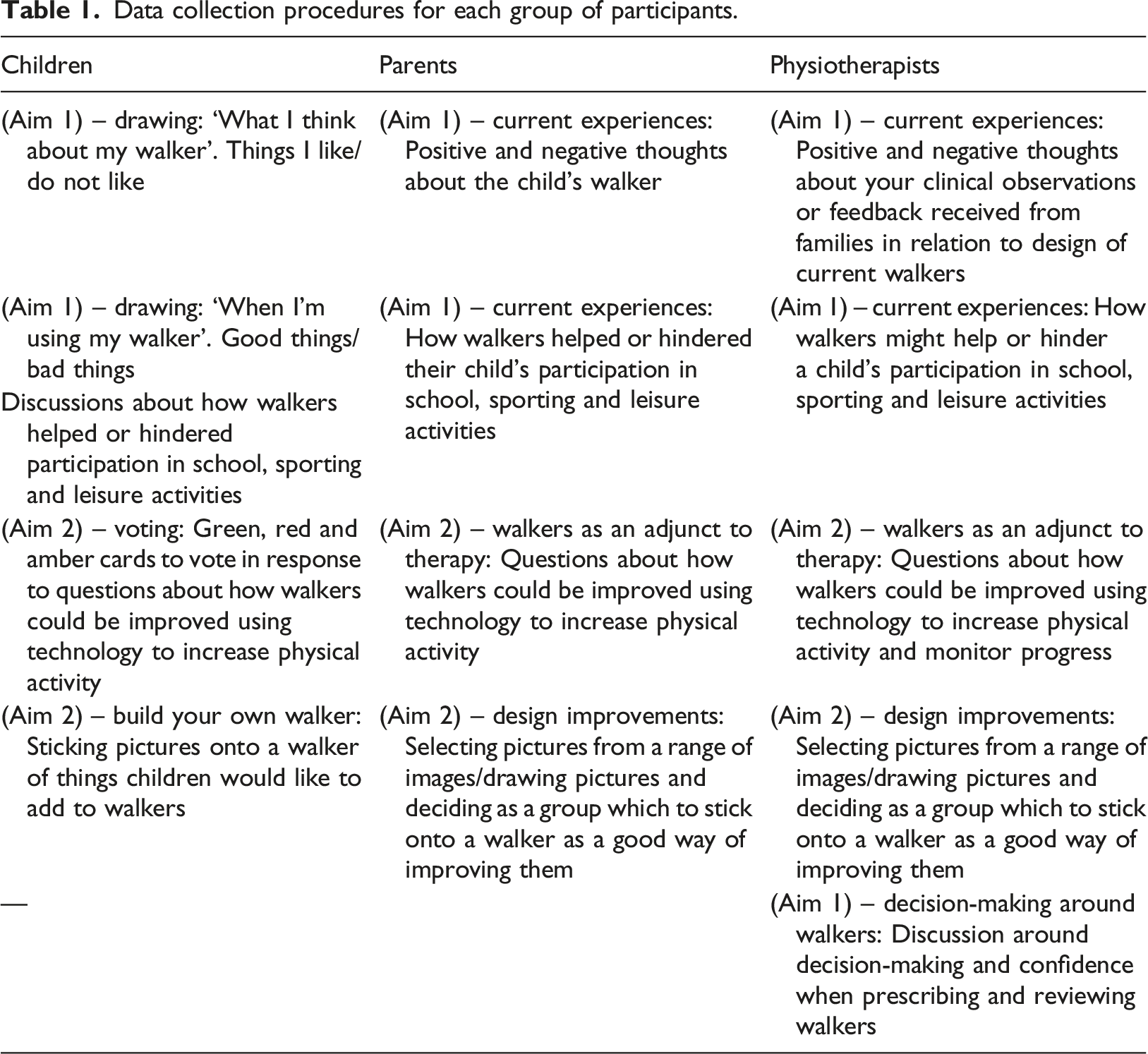
Groups lasting 45–70 minutes were audio recorded and transcribed verbatim. When children voted using coloured cards (Table 1), facilitators verbalised the number of votes for each colour, so this was included in the transcript. Photographs were taken of drawings and ‘build your walker’ activities. Field notes were made to document immediate observations and reflections. NVivo 10 (QSR International Pty Ltd, 2014) was used for data management. Transcripts and photographs were uploaded into this computer programme for analysis.
Data analysis
An ontological position of subtle realism was adopted (Blaikie, 2007). This assumes that an external or objective reality exists, which is independent of individual beliefs or understanding (Ritchie et al., 2014) and recognises that although this external reality exists, it is only known through the human mind and socially constructed meanings (Blaikie, 2007).
Framework analysis was employed as its applied quality suited the study’s objectives (Ritchie et al., 2014; Poole and Hebda-Boon, 2019). Framework analysis is a systematic approach, consisting of five distinct stages: familiarisation, developing a thematic framework, indexing and sorting data, reviewing data and refining the framework, summarising data in charts (Supplement file 2). Abstraction and interpretation follows these five steps. Two researchers were involved and met at each stage of the analysis to review and discuss progress. Photographs were labelled with themes from the thematic framework to ensure visual data within them was represented.
Reflexivity and trustworthiness
Participants were informed that the lead facilitator was not familiar with this topic, which minimised her preconceptions. She was introduced to children as a scientist and to adults as an academic. Her lack of pre-existing relationships with participants made it appropriate for her to lead. The second facilitator was introduced to those she had not met as a paediatric physiotherapist, who was undertaking research. As an advocate of using technology in clinical practice, she was aware of her role and opinions when analysing data. She minimised her influence on data collection by being second facilitator.
Facilitators worked in partnership to code and interpret data, acting as critical friends as recommended by Smith and McGannon (2018).
Exploring different perspectives (children, parents and physiotherapists) in relation to the same aims served as a means of triangulation (Mortenson and William, 2008), enhancing trustworthiness.
To create a psychologically safe environment, participants were reassured that their contributions were valuable and were asked not to discuss conversations they had afterwards.
Ethical considerations
West Midlands – Solihull Research Ethics Committee granted approval for this study to be carried out in the NHS (REC ref 221393). Participants or their parents gave informed written consent; children gave verbal assent. Participants were reminded that they could withdraw without explanation. Asking participants to keep conversations confidential helped to maintain anonymity. Transcripts were anonymised. Pseudonyms are used for participant quotations.
Findings
Participants
Participant characteristics.
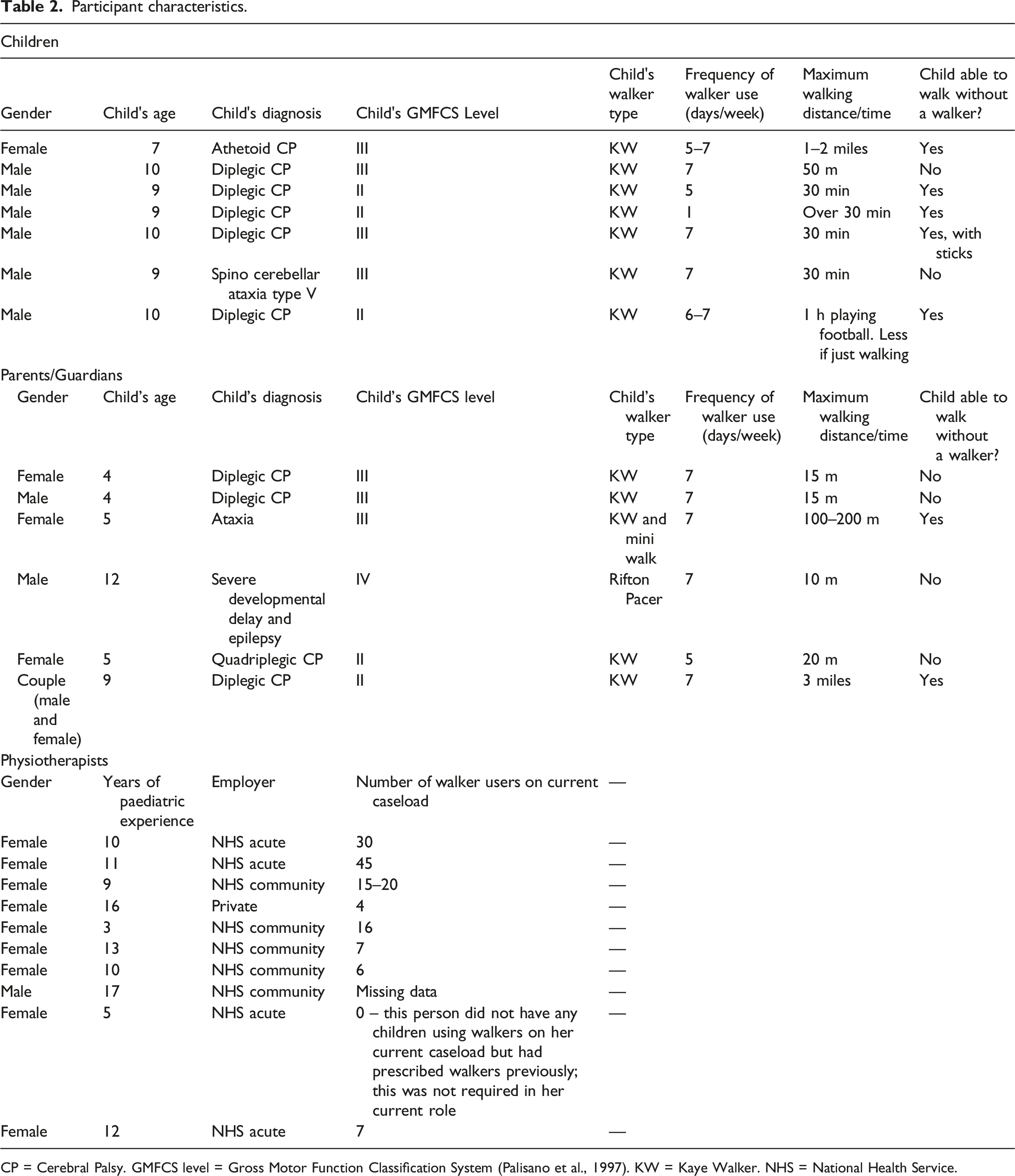
CP = Cerebral Palsy. GMFCS level = Gross Motor Function Classification System (Palisano et al., 1997). KW = Kaye Walker. NHS = National Health Service.
Participants in the first children’s group were strangers; those in the second knew each other. Children only attended one group. Physiotherapists (n = 10) from across England with varying caseloads participated (see Table 2).
Summary of findings
Three themes (with sub-themes) were identified (see Figure 1): (1) drivers for use/non-use of walkers, (2) trade-offs associated with walker use, (3) acceptance of technology within walkers. The overarching concept and themes identified from the framework analysis.
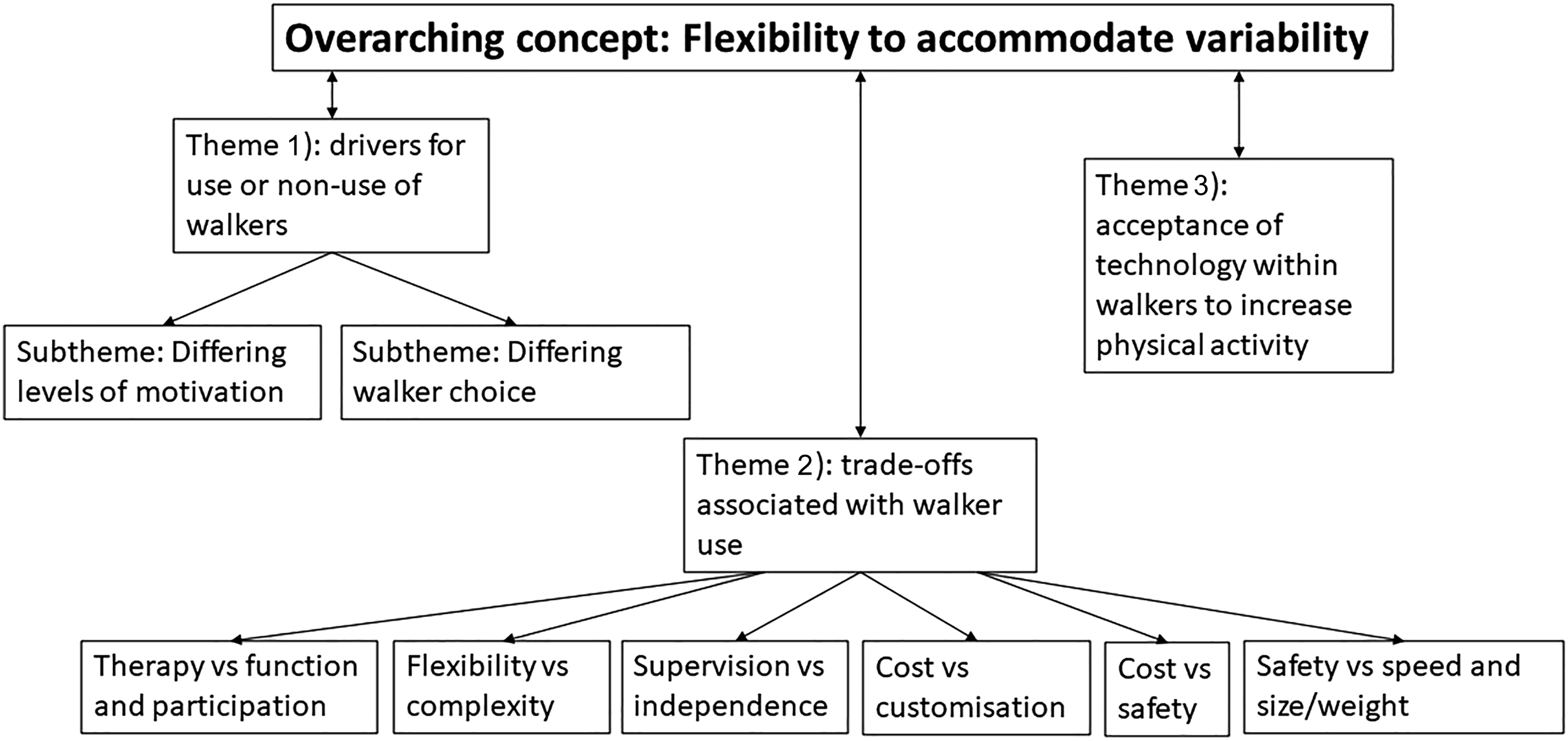
These themes were built into an overarching concept – flexibility to accommodate variability. This overarching concept is described firstly, followed by themes that informed its development.
Overarching concept: Flexibility to accommodate variability
A requirement for walkers to be flexible to accommodate variability at individual, interpersonal and environmental levels was an overarching concept. It reflects how three subsets of participants had different perspectives of what the walker meant to them.
Individually, children needed larger, heavier walkers and more help transferring in and out of them as they grew. Furthermore, as children matured, their sources of motivation, desire for independence, participation in activities, social inclusion, understanding of goal setting and compliance with walking, changed. Interpersonally, children’s physical and cognitive abilities varied widely. Environmentally, participants needed to use walkers indoors or outdoors, on different surfaces, whilst maintaining stability and a safe speed. It seemed difficult to achieve this within one walker. “So wheels that go indoor and outdoor would be the best thing on any one walker because then you don't have to have two walkers.” Kirsty (physiotherapist)
Environments varied between primary/secondary and special/mainstream schools, such as width of doorways and space for manoeuvring. In response to these variations, participants suggested adaptations to walkers were required to increase flexibility and ease of use. Children wanted anti-reverse mechanisms to turn on and off easily to improve manoeuvring, all wheels to swivel when desired, something to stop walkers tipping backwards, small indoor and larger outdoor wheels and a wider opening at the front when playing football. Adult participants also discussed these features, and requested light-weight walkers, combining walkers and seating to minimise transfers between pieces of equipment, easily removable accessories, an additional set of stabilisers to address unsteadiness and more choice in handle styles.
Participants stated that technology added to walkers needed to be flexible and easily removable, to avoid distractions during lessons or in hazardous environments such as roadsides. All groups thought a wide range of modes, games and alert/reward systems were required to suit all ages, abilities and personal tastes: “If they can talk and have understanding that [reward charts] would be brilliant, but mine [my child] don’t have understanding so…” Emily (Parent) “It isn't just one type of game, there's loads. So if someone wasn't sure about [a] game I bet they would be able to find something.” Alex (Child)
Theme: Drivers for use/non-use of walkers
Drivers for use/non-use of walkers.
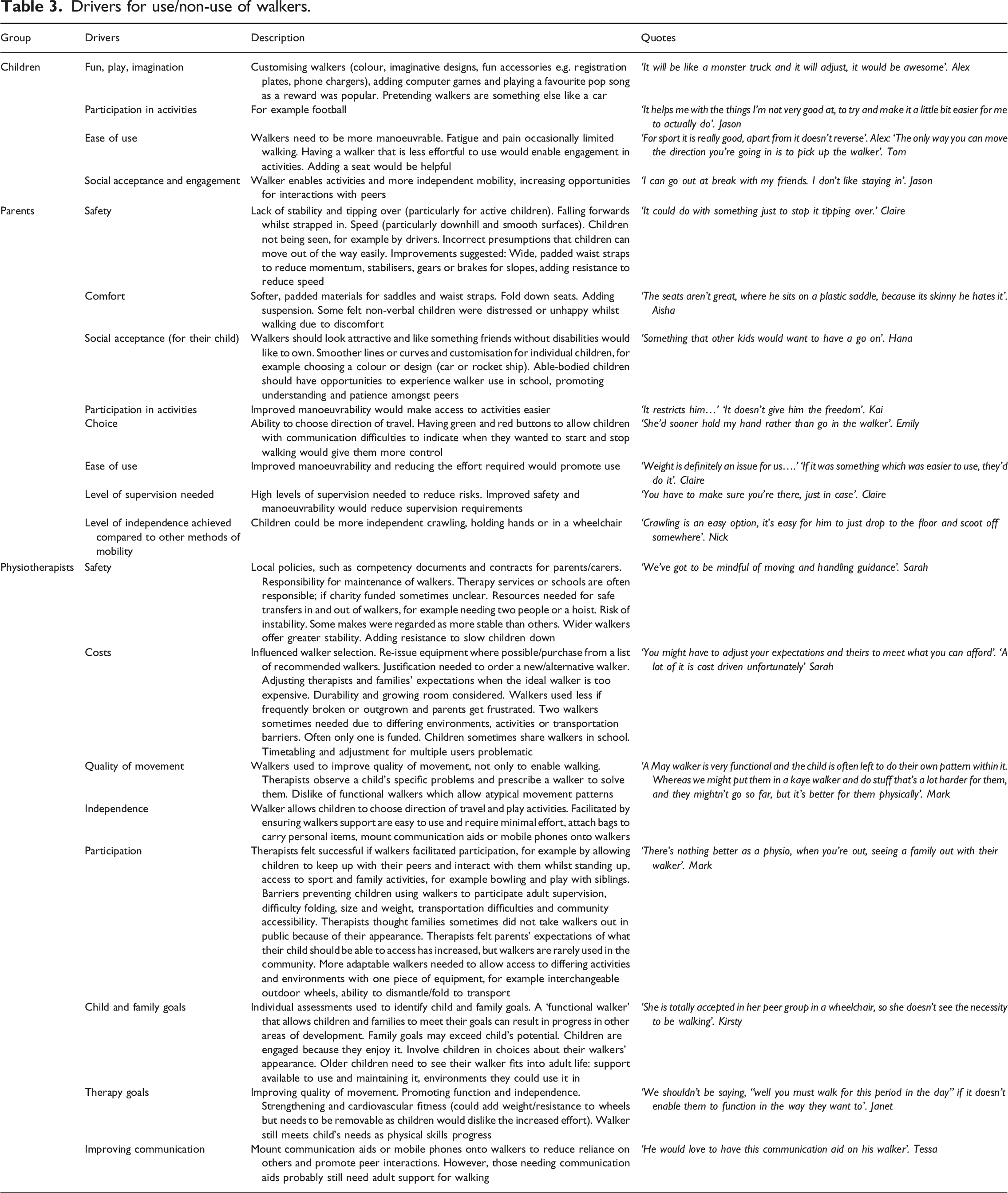
Children’s focus on fun, imagination and play was highlighted when they discussed accessories. They wanted walkers to be like cars, requesting headlights, registration plates, docks and chargers for phones/tablets, drinks bottle holders, a horn, satellite navigation, book bags and seats (see Table 3).
The following sub-themes expand on this idea of drivers.
Differing levels of motivation
Examples of children, parents and physiotherapists having different levels of motivation in relation to walker use included children wanting to walk but adults not being engaged, parents wanting children to walk but children preferring their wheelchair (to conserve energy/facilitate peer interactions) and physiotherapists seeing potential for walking but children and/or families not sharing this goal. Physiotherapists felt walking would be limited if families did not recognise its importance.
Differing walker choice
Children’s, parents’ and physiotherapists’ differing drivers (Table 3) meant families were sometimes prescribed a walker that did not meet their expectations: “…when you aren’t able to provide the thing they [families] want that can be quite difficult.” Kirsty (Physiotherapist)
Some parents felt their child’s walker was uncomfortable, unsafe or difficult to use due to weight or poor manoeuvrability. Safety and comfort were key drivers for parents (Table 3), so these concerns could result in lack of engagement.
Cost could also contribute to the gap between users’ expectations and their prescribed walker.
Theme: Trade-offs associated with use/non-use of walkers
Children, parents and physiotherapists having differing drivers could create conflict. Sometimes one group’s needs were subsumed by those of another. These trade-offs are described in the following sub-themes.
Therapy versus function and participation
Whether walkers were for therapy, or for function and participation, was discussed. Participation is defined as involvement in a life situation (Carmargo et al., 2019). Physiotherapy involves helping people affected by injury, illness or disability through movement, exercise, education and advice (Chartered Society of Physiotherapy, 2018). Some physiotherapists saw therapy and participation as separate constructs. They felt two walkers were often needed, because activities undertaken and support needed to achieve good quality movement, meet therapy goals and provide long term benefits differed to activities and support needed to maximise function and participation. Walkers facilitating function and participation were popular with families and more likely to be used. Walkers prescribed for therapy may not be suitable for participation in sport, creating a barrier. Only one walker can usually be prescribed. When a second is required, private or charity funding is needed.
Tessa (physiotherapist) observed children to identify which movement skills they lacked, then prescribed a walker that supported development of those skills. The child’s perspective was a secondary consideration. However, Sally (physiotherapist) felt quality of movement did not matter if children were unable to experience walking any other way.
Flexibility versus complexity
Designing flexible walkers to meet therapy and functional demands would be beneficial. However, adding flexibility produces increasingly complex equipment and a potentially overwhelming number of options to consider. Participants suggested that multiple accessories and adjustable features could make learning to use walkers difficult. Furthermore, physiotherapists noted parts were more likely to get lost, moved accidently or broken, and that walkers become cumbersome and expensive as features are added.
Supervision versus independence
Parents hoped a walker would increase their child’s independence and access to activities. However, some children required considerable help and supervision when walking. Parents needed to be physically close for safety and helping with transfers, reversing, turning and opening doors. Hence, they commented that children had more freedom when crawling or holding hands than using their walker.
Physiotherapists appreciated that using walkers could be slow and impractical unless children only needed minimal support. They thought children who could transfer into a walker independently were more likely to use it than those who required help. When two adults were needed to transfer a child into their walker, it limited use. Physiotherapists felt these barriers could make using a wheelchair or holding hands faster, easier options: “…if they put them in a wheelchair they can whizz down with the rest of their class and it’s not taking a member of staff out necessarily to walk with them.” Janet (Physiotherapist)
Reducing these burdens through environmental adaptations or improved walker designs may increase frequency of use. Prescribing walkers that are less challenging to use may increase independence and reduce parental burden, but reduce therapeutic benefits.
Cost versus customisation
Children were enthusiastic about being able to customise walkers but lacked insight into cost implications: “It would be nice if it was yellow…I would want it to play a song….” Tom (Child)
Parents and physiotherapists realised giving children more choice about appearance of walkers and accessories could be expensive. They felt families or charities should fund non-essential features.
Cost versus safety
Physiotherapists had safety concerns around sharing and reissuing of equipment. They were uncertain whether there was national guidance in relation to this, as practice seemed to vary: “…we've been talked to about whether [walkers] can actually be reissued….. they've got a shelf life and they're only kind of meant to be single patient. And infection control if people stick stickers and things on them.” Janet (Physiotherapist)
Some also felt making one walker appropriate for multiple environments to save money could be unsafe.
Safety versus speed and size/weight
All groups wanted children to be able to keep up with their peers and family. Children wanted to go quickly. Parents and physiotherapists had reservations about excessive speed reducing stability and increasing risk of falls and injuries. They suggested designing braking systems, which could be automatic or activated on slopes and smooth surfaces.
All groups wanted walkers to be smaller and lighter to improve manoeuvrability. Parents and physiotherapists said this would also make transportation easier. However, physiotherapists highlighted that narrow walkers could be unstable.
Theme: Acceptance of technology within walkers
Adding technology to walkers to promote physical activity was appealing. Children were excited about accessing digital games via their walker: “You can play a game at school when nobody else is allowed to play a game and it will encourage you to walk to play that game.” Sam (Child)
They discussed incorporating games that could encourage walking (Fifa, Football, Pokemon). Most children wanted feedback about their walking and goal setting functions. They related this to popular wearable devices (e.g. Fitbits) and wanted alerts/rewards to be included. They enjoyed discussing reward celebration options (announcements, vibrations, playing music). They felt a digitally enhanced walker would give them kudos amongst their peers and could be used to draw positive attention at school: “Disturb everyone else and then their [the teacher] is like oooh, listen children, [child’s name] has got a goal………just make sure the volume is up really loud”.” Jason (Child)
Parents were concerned about children going too fast and games or alerts distracting them. They wanted to be able to disable games when appropriate: “…he'd start concentrating on that, way too much than actually where he's going.” Kai (Parent)
Parents thought devices attached to walkers could be damaged, so uploading data to nearby devices was preferable. They thought having information about their child’s walking at school would be useful: “So when they’ve done it at school you’ll be able to see exactly how much they’re doing, and you can see if they’re doing enough exercise, which would be really beneficial, because they don't always tell you.” Claire (Parent)
Physiotherapists worried that creating a culture of self-monitoring might limit play, fun and exploration. They recommended monitoring activity over limited time periods. They discussed how existing digital interventions to promote physical activity are often inappropriate for children with disabilities and were positive about making them more inclusive: “It's finding the ones [games] at the right level isn't it, so it's achievable rather than having the frustration.” Mark (Physiotherapist)
Discussion
We explored experiences of walker use from the perspective of children with physical disabilities, their families and physiotherapists. They identified benefits and drawbacks of/barriers to using walkers, which we encompassed within an overarching concept – flexibility to accommodate variability. We sought participants’ opinions on adding technology to walkers to promote physical activity. Participants prioritised basic improvements above addition of technology.
We identified drivers that influence physiotherapists’ decision-making processes when prescribing walkers, including the tension between participation versus therapy. Some physiotherapists viewed therapy and participation as separate constructs, despite the ultimate goal of therapy being to enable participation (Schwellnus et al., 2020). We propose that therapy and participation are inseparable and intertwined. Therefore, any intervention that facilitates participation is part of physiotherapy, regardless of whether, historically, it would have been viewed in that way.
As children, parents and physiotherapists have differing drivers, family led goal setting is important. Seyhan et al. (2020) found parents and children were more satisfied with family-centred, goal-directed approaches, which can be achieved by children and families working collaboratively with professionals to improve goal performance, satisfaction and attainment (Schwellnus et al., 2020). The influence children’s drivers have on physical activity, particularly fun, play, imagination, participation and social acceptance cannot be underestimated. Walker colour, appearance and presence or absence of technology upon it may not be prioritised by adults involved in decision-making. However, if these aspects help children to feel confident, accepted and motivated to walk, it is more likely that they will increase their physical activity and participation, and reduce their sedentary time. Increased physical activity, participation and inclusion are all associated with improved quality of life for children with disabilities (Bloemen et al., 2015; Shikako-Thomas et al., 2012; Knight et al., 2013).
Factors and drivers that determine frequency of walker use and those that introduce variability can be categorised according to the socioecological model (McLaren and Hawe, 2005), illustrating that there are influences at a range of levels: individual, interpersonal, environmental and system wide. For individuals, cognitive and motor ability, growth and development introduced variability. Interactions with peers, parents, teachers, healthcare professionals and carers influenced walker use at an interpersonal level. Home and school environments were relevant, as was environmental accessibility for sports participation and leisure time. At a system wide level, models of and attitudes towards disability were relevant in relation to cultural and societal influences on barriers and facilitators for walker use that were described. Mehtälä et al. (2014) advocated use of multilevel and multicomponent interventions to increase children’s physical activity. Considering how our findings relate to the socioecological model provides an opportunity to identify which levels interventions should target; for example whether interpersonal interactions to identify shared goals, changes in walker design, environmental adaptations or raising awareness of disability and accessibility in society would be most effective to increase physical activity.
Self-determination theory (Ryan and Deci, 2008) is another useful lens for considering our findings. It focuses on the process through which an individual is motivated to initiate and maintain new health-related behaviours. It argues that ‘developing a sense of autonomy and competence are critical to the processes of internalization and integration, through which a person comes to self-regulate and sustain behaviours conducive to health and well-being’ (Ryan and Deci, 2008; page 2). Applying this theory to walker use, physical activity will be maximised when children and parents are intrinsically and autonomously motivated and feel successful. This is more likely to occur when their goals are prioritised, with less emphasis on therapy outcomes.
Parents described how their child’s walker created burdens. George et al. (2020) found the most common precaution for use of support walkers was supervision requirements and the most common problem was getting in and out of the walker. Both issues were raised by parents in our study. Prescribing walkers that can be used more independently, and providing guidance and equipment to assist with transfers in and out of them, would help to reduce these barriers to undertaking physical activity.
Gudjonsdottir and Gudmundsdottir (2021) found mobility devices are important facilitators of children’s participation and they may need multiple types of mobility equipment, because they are used in differing environments. We found physiotherapy potentially created a barrier to participation when children were prescribed a ‘therapy walker’ that is not sufficiently robust for sport. Physiotherapists can promote participation and physical activity by supporting families to obtain funding for additional walkers, or prescribing walkers with sufficient flexibility to meet both needs.
Balancing the gap between expectations of families and the equipment prescribed is an important part of healthcare professionals’ roles. Mortenson and William (2008) found negotiation was required to resolve conflicts between professionals prescribing wheelchairs and their clients in relation to desired outcomes. A power sharing model was advocated, led by client-prescriber interaction, as both have expert knowledge.
Some of the features children and parents requested are already available, for example larger wheels for outdoor use (Kaye Posture Control walkers, Nimbo Posterior Posture Walker), or ability to turn off anti-reverse (R82 Crocodile). Further research could identify whether lack of provision of these features is due to the need not being identified, lack of knowledge of their availability or cost.
Limitations
Recruiting via the Frame Football Association introduced risk of over-representing physically active children and resulted in more boys with diplegic CP taking part. Most parents who participated were recruited via the NHS Trust, so it was not a concern for their group.
Children who participated had lower Gross Motor Function System Classification System (GMFCS) levels and therefore greater capacity for physical activity than the majority of the parents’ children. This must be taken into consideration when comparing their perspectives.
A high number of female physiotherapists participated. However, as approximately 76% of physiotherapists in the UK are female (Health and Care Professions Council, 2018) this is representative.
GMFCS levels, used to classify functional mobility, are only validated for children who have CP (Rosenbaum et al., 2002). Currently, no alternative to GMFCS levels are available for children with other diagnoses. We applied the GMFCS to all participants, regardless of diagnosis.
Children in GMFCS level V (severely limited motor function) were not represented. This means the research may not have captured barriers faced by families of children with complex disabilities (Ghaffari et al., 2020).
Implications for practice
A family’s experiences could be improved by modifying basic features of walkers, to improve manoeuvrability, safety, ease of outdoor use and comfort. Data from our focus groups suggested this was a higher priority than adding technology that provides feedback. To maximise physical activity, walker prescribers and designers should prioritise drivers that motivate children and parents, ensuring goal setting is family-centred and participation-orientated. Involving families in co-designing walkers is important. Longer assessments would allow families to experience using walkers in multiple environments.
Conclusions
To accommodate wide individual, interpersonal and environmental variability, walkers need to be designed to offer flexibility. Children, parents and physiotherapists expressed contrasting drivers for walker use/non-use, which created trade-offs. To increase physical activity, child-centred clinical assessments to identify specific needs and goals are important.
Supplemental Material
Supplemental Material – Perspectives of children with physical disabilities, parents and physiotherapists on use of walkers and their potential to increase physical activity. A qualitative exploration
Supplemental Material for Perspectives of children with physical disabilities, parents and physiotherapists on use of walkers and their potential to increase physical activity. A qualitative exploration by Marilyn Bradburyand Stephanie Tierney in Journal of Child Health Care
Footnotes
Acknowledgements
The authors would like to thank the Frame Football Association and the Association of Paediatric Chartered Physiotherapists for hosting our focus groups. We would like to thank all the children, parents and physiotherapists who shared their views with us during focus groups.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chartered Society of Physiotherapy Charitable Trust (PRF/16/B11), Birmingham Community Healthcare NHS Foundation Trust (Pump Prime Funding).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.