
Abstract
Standard description of local care provision is essential for evidence-informed planning. This study aimed to map and compare the availability and diversity of current mental health service provision for children and adolescents in Australia. We used a standardised service classification instrument, the Description and Evaluation of Services and DirectoriEs (DESDE) tool, to describe service availability in eight urban and two rural health districts in Australia. The pattern of care was compared with that available for other age groups in Australia. Outpatient care was found to be the most common type of service provision, comprising 212 (81.2%) of all services identified. Hospital care (acute and non-acute) was more available in urban than in rural areas (20 services [9.7%] vs 1 [1.8%]). The level of diversity in the types of care available for children and adolescents was lower than that for the general adult population, but slightly higher than that for older people in the same areas. Standardised comparison of the pattern of care across regions reduces ambiguity in service description and classification, enables gap analysis and can inform policy and planning.
Introduction
Mental disorders are one of the leading causes of burden of disease in children and adolescents (Australian Institute of Health and Welfare, 2020). Several international projects have gathered information on the current state of policies for child and adolescent mental health services, and provided recommendations to strengthen their implementation (Coppens et al., 2015; Hendriks et al., 2019). These projects have found a relationship between higher levels of service availability and lower levels of child and adolescent behavioural problems (e.g. aggressive behaviour) (Hendriks et al., 2019). There is therefore a critical need for planners of child and adolescent mental health services to know the current level of service availability within their jurisdictions, and identify any existing gaps in service provision, to inform appropriate service planning for local need.
This knowledge about local service availability can then enable comparison with systems of care provision in other regions, both national and international. The importance of such comparisons has been underscored by the World Health Organization (WHO), and a series of analytic tools for use at national and regional level have been developed. These include the Service Availability and Readiness Assessment (O’Neill et al., 2013) and the World Health Organization Assessment Instrument for Mental Health Systems (Lora and Sharan, 2015), which has been used to assess child and adolescent mental health services in low- and middle-income countries (Morris et al., 2011). However, terminological ambiguity in mental health services research, including ambiguity in definition and description of services and target population, differences in the structure and complexity of service networks, and the frequent exclusion of non-health-related services, limit the effectiveness of international comparisons (OECD; Eurostat and World Health Organization, 2017).
These methodological limitations are also present at the national level. Despite the uneven distribution of child and adolescent mental health services across Australia, the information currently available is aggregated at state, rather than local, level. It is also focused on public health services (Lawrence et al., 2015). This reduces its reliability and usefulness in informing service planning at the local level. A common assessment method, using a ‘whole system’ approach is required, integrating health, social, education and justice services (Stansfield et al., 2020), and better coordinated with related areas such as drug and alcohol disorders or neurodevelopmental conditions (Brien et al., 2015; Mental Health Commission of Western Australia, 2020). (Lawrence et al., 2015). A common reference framework (Leginski et al., 1989), validated glossary of terms (Montagni et al., 2018) and standardised classification system (Salvador-Carulla et al., 2013) for describing and mapping local services should also be used. This harmonised data can then be used to plan for equitable allocation of care resources, programs and treatments across different health districts, and facilitate the linkage of health networks (Garcia-Alonso et al., 2019).
Local Atlases of Care use an international service classification instrument which addresses the issues described above. They provide a standardised description of local service provision, allow data aggregation without incurring the ecological fallacy (assuming that population means and national averages apply directly to individuals or to local area services), and provide key information about service characteristics and availability to support evidence-informed policy (Rosenberg et al., 2020; Salinas-Perez et al., 2020).
Local Atlases of Care use a Mental Health Ecosystems Research (MHER) approach. This is a novel approach to the study of complex health systems (Furst et al., 2021), which can reduce ambiguity in the analysis of their complexity and diversity, including that arising from their different ecological levels and typologies of care, and their diverse social, economic, demographic and political contexts (Furst et al., 2019). This approach enables envisioning of the structure of the whole service system, showing the pattern of care delivery in a defined area, including gaps and duplications in care, and its relationship with local social determinants of health. This then provides the basis for international, regional, longitudinal or specific population-based comparison with other systems (Romero-Lopez-Alberca et al., 2019).
The need for better comparative data on healthcare provision for children and adolescents has been recently shown by service mapping for Attention Deficit Hyperactivity Disorder in the UK (Price et al., 2019), and the relatively low availability of child and adolescent mental health services when compared to that of adult services in low- and middle-income countries (Morris et al., 2011). There is, however, a gap in the literature related to comparative data available on mental healthcare provision for children and adolescents.
Aim
To describe the pattern of mental healthcare provision (availability and diversity) for people under 18 years of age in urban and rural health districts in Australia, and to compare it with the pattern of care delivery reported in other population groups (adults and older people) (Tabatabaei-Jafari et al., 2020).
Materials and methods
Study design and study areas
This is an ecological, comparative and cross-sectional study comprising 10 districts (8 urban and 2 rural) of the 31 Primary Health Networks in Australia. Healthcare in Australia, including mental healthcare, is coordinated at regional level by Primary Health Networks, which are broadly similar geographically to Local Health Districts. Local Health Districts are responsible for management of public hospitals and community mental health centres. This study is part of the GLOCAL (Global and Local Observation and mapping of CAre Levels) project (University of Canberra, 2021) comparing local patterns of mental health care throughout the world. The urban regions include Australian Capital Territory, Eastern Melbourne, Perth North, Perth South, North Sydney, South Western Sydney and Western Sydney Primary Health Networks. South Eastern Sydney Local Health District was mapped within Central Eastern Sydney Primary Health Network. The rural and remote areas include Country Western Australia and Western New South Wales. The same method was used to map all regions. Integrated Atlases of Mental Health are available at the Australian National University Integrated Health Care Atlases repository site (GLOCAL, 2022).
Services
Child and adolescent mental health services within the boundaries of the selected Primary Health Networks were evaluated using the Description and Evaluation of Services and DirectoriEs (DESDE) (Salvador-Carulla et al., 2013). DESDE provides a standard description of all services available in a defined area, using common units of analysis. DESDE has described local care provision in over 35 countries (Romero-Lopez-Alberca et al., 2019), and has been validated in application to adult mental health care (Salvador-Carulla et al., 2000), disability (Salvador-Carulla et al., 2006b;) and chronic care (Salvador-Carulla et al., 2000, 2006, 2013, 2015).
DESDE’s international terminology and multiaxial coding overcomes the problem of terminological ambiguity resulting from variation in the names of services, and in how they are used to describe the type of care provided. Its units of analysis are care teams or Basic Stable Inputs of Care (BSIC). BSICs are the minimal units of care with organisational and temporal stability (i.e. funded for more than 3 years), delivering care to a defined population (Salvador-Carulla et al., 2013, 2015). Care teams are classified using the DESDE multiaxial system. The first axis of the code refers to the ecological level (macro, meso or micro) of the service catchment area (e.g. a municipality, a health district or a region within a country). The next DESDE axis defines the specific target population of the service (age, gender, International Classification of Disease coding, functioning). The following axis code provides the primary activity or Main Type of Care (MTC) provided by the care team. DESDE comprises 108 MTCs, grouped into 6 main branches and described according to characteristics including acuity, mobility and frequency of support: (1) Residential care, both community and hospital, acute and non-acute; (2) Day care, providing structured and unstructured day activities, including work related care; (3) Outpatient care, both centre based (non-mobile) and outreach (mobile); (4) Accessibility to care, including co-ordination of care but not direct support; (5) Information and assessment services that do not provide ongoing support or direct care provision; and (6) Self-help and volunteer care that include any types of care provision by unpaid peers or graduate professionals.
The DESDE taxonomy is described in detail online at http://www.edesdeproject.eu/. See supplementary table (Annex) for DESDE codes for the range of services in Australia.
Service inclusion and exclusion criteria
All services with temporal and organisational stability within the boundaries of the defined Primary Health Networks providing specialised mental health services to people aged less than 18 years were included in this study. Temporal and administrative stability were defined as services with administrative support and own workspace, separate documentation and accountability, and stable ongoing funding. Generic services for the general population (e.g. general practitioners) were not included.
Data collection
Services providing mental health support to young people up to the age of 18 years were identified in each area through a search online and of existing directories, and consultation with local sector and peak body representatives. Data were collected by researchers from the Glocal Integrated Mental Health Atlas project between 2014 and 2017 from interviews with service managers, either face to face, by telephone or through an online survey tool. The Glocal project includes researchers from the University of Canberra, Australian National University, ConNetica, University of Sydney and the University of Loyola Andalucia (Spain).
Data analysis and mapping (data comparison and analysis)
Integrated Atlases of Mental Health for these Primary Health Networks/Local Health Districts are available at the University of Canberra repository of Integrated Health Care Atlases (GLOCAL, 2022). The repository allows comparison of patterns of service provision in areas mapped using the same method and instrument, and checked by the same core group. We followed a heuristic approach to identify patterns of care and gaps in service provision.
We analysed the pattern of care in each region through a description of the Main Types of Care provided by all care teams (BSICs) meeting inclusion criteria according to (i) availability; (ii) the balance of care; and (iii) the diversity of care. ‘Availability’ is defined as the number of MTCs operable upon demand per 100,000 child and adolescent population; ‘balance of care’ is defined as the relative percentage of health and non-health services, and ‘diversity’ as the number of different individual codes representing the types of care in each region.
The availability and diversity of services for children and adolescents were compared to that of services for the other two main age groups: adults aged 18 years and over, and older people, using data collected following the same method. Full information is available at the repository site (GLOCAL, 2022).
Ethics approvals
Ethical approval was secured from the requisite institutions.
Except for Perth North, Perth South, and Central Western Australia which were considered as ethics review exceptions by North Metropolitan Health Service Mental Health Human Research Ethics Committee (NMHSMH HREC- QI 2016_05), for other study areas data collection was approved by the relevant ethics committees using the same standards of consent and confidentiality. Ethical approval institutions and numbers are as follows: Australian Capital Territory-ACT Health ETHLR.16.094; Western Sydney-Human Research Ethics Committee at the University of Sydney 2013/678 (extension of Project 2015/778); South West Sydney-SWS Local Health District LNR/14/LPOOL/467; Sydney North- Sydney North Local Health District HREC LNR/16/HAWKE/338; Western New South Wales- The Greater Western Human Research Ethics Committee LNR/17/GWAHS/19 (GWAHS 2017-018); South East Sydney- CH62/6/2015-126 ; South East Melbourne- Monash Human Research Ethics Committee 11116.
Information was stored in the respective research institutions in password protected computer files for a period of 10 years. Only the researchers had details about who participated in the study. Data files included name of service, but not interviewee.
Results
Description of study areas
Key demographic and socioeconomic factors in study areas.

Sources: Social Health Atlases of Australia, 2019 (Public Health Information Development Unit (PHIDU), 2019); and Australian Bureau of Statistics, 2016 (Australian Bureau of Statistics, 2016a, Australian Bureau of Statistics, 2016b).
The range of study areas is characteristic of Australia’s particular pattern of settlement, which includes areas of high urbanisation along with areas of considerable remoteness (Parliament of Australia, 2019). Central and Eastern Sydney Primary Health Network had the highest population density of the study areas (more than 2600 people per square kilometre); and South Western Sydney, Australian Capital Territory and Perth South Primary Health Network the lowest (fewer than 200 people per square kilometre). Rural areas were slightly more socioeconomically disadvantaged than the Australian national average, while the urban areas were slightly less disadvantaged than the Australian average.
Overview of services in urban areas
Two hundred and six Main Types of Care delivered by 192 care teams were identified, or 126.86 MTCs per 100,000 children and adolescents under 18 years. The most common type of care was health related with 147 (71.3%) services. The other 59 (28.7%) types of care available were mostly social support. One hundred and fifty-nine (77.2%) were outpatient services, of which 110 (69.2%) were hospital- or community-centre based and 49 (30.8%) were mobile (outreach) services. This was followed by 20 (9.7%) hospital and community residential care, 10 (4.9%) accessibility to care, 9 (4.4%) information for care, and 2 (1.0%) self-help and volunteer services.
Diversity, pattern and balance of child and adolescent’s mental health main types of care in the study areas.
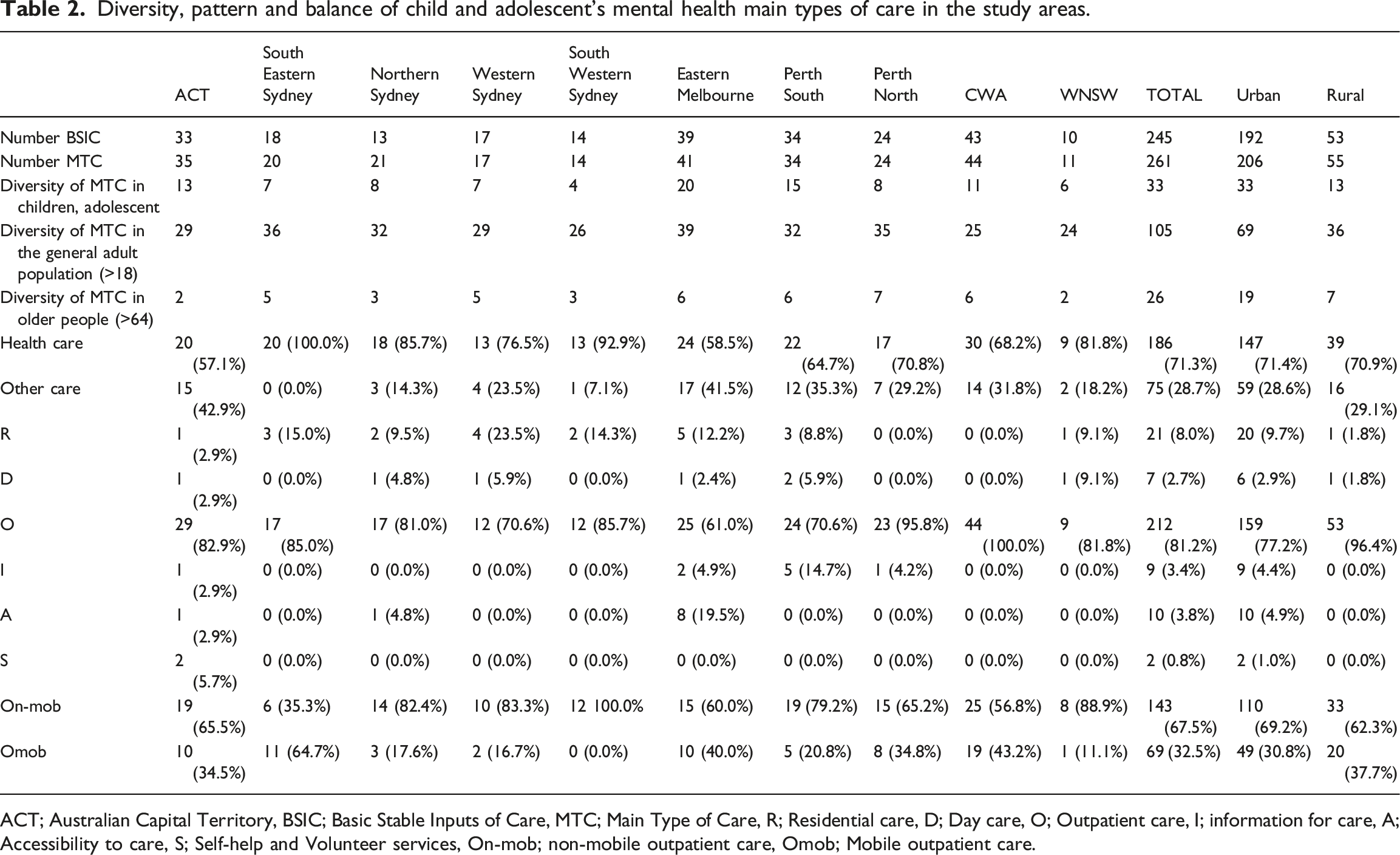
ACT; Australian Capital Territory, BSIC; Basic Stable Inputs of Care, MTC; Main Type of Care, R; Residential care, D; Day care, O; Outpatient care, I; information for care, A; Accessibility to care, S; Self-help and Volunteer services, On-mob; non-mobile outpatient care, Omob; Mobile outpatient care.
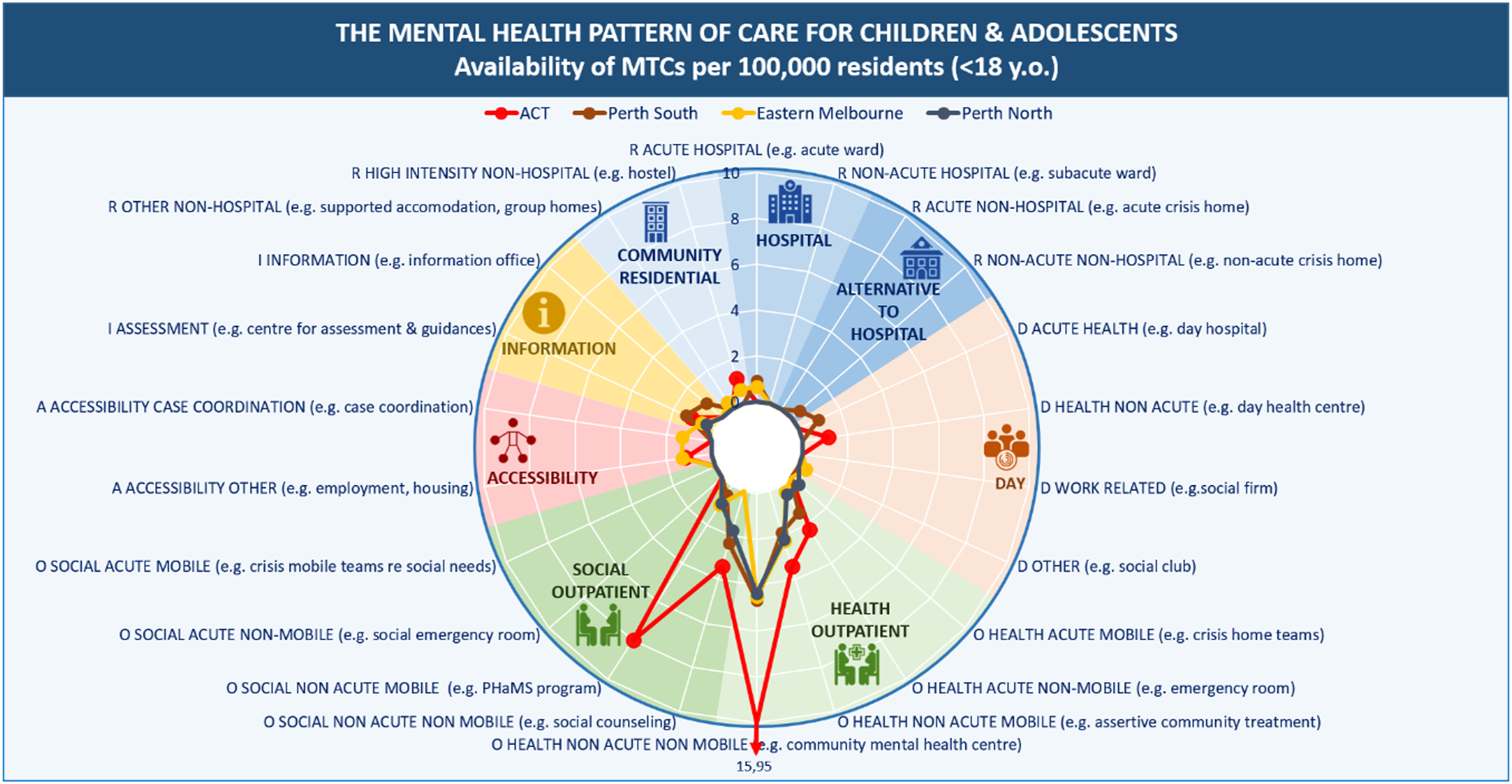
Outpatient and residential care were the most common types of care in all urban areas. In the Sydney catchment areas (South Eastern Sydney, Western Sydney and South Western Sydney), they were the only types of care available. North Sydney Primary Health Network was the only Sydney region to provide day care and accessibility services (Figure 1). A wider variety of services were identified in other regions outside of Sydney (Figure 2). Australian Capital Territory and Eastern Melbourne had the highest diversity of services and availability per 100,000 children and adolescents. Pattern of care of child and adolescent services in Sydney health districts: main types of care per 100,000 inhabitants aged 17 years and less. Pattern of care of child and adolescent services in Australian Capital Territory (ACT), Melbourne and Perth health districts: main types of care per 100,000 inhabitants aged 17 years and less.
Overview of services in rural areas
Fifty five Main Types of Care delivered by 53 care teams were identified, or 27.15 MTCs per 100,000 children and adolescents under 18 years. Health-related care was most common, with 39 (70.9%) services, with other types of care such as social care comprising the remaining 16 (29.1%) available services. Fifty-three services (96.4%) in rural areas were classified as outpatient. Of this, 33 (62.3%) were hospital or centre based and 20 (37.7%) were outreach. Hospital or community residential care and day care each accounted for 1 (1.8%) service. There were no services available for information for care, accessibility to care, and self-help and volunteer care in rural areas. There were 13 different types of care in the rural areas (Table 2), which represented less diversity than that for the general adult population, but slightly higher than that for older people in the rural areas studied.
The only type of care available in Country Western Australia was outpatient care. In Western New South Wales, outpatient, residential and day services were available. Despite this, Country Western Australia provided greater diversity of care, with both centre-based social type care and community outreach care most commonly available (Figure 3). Pattern of care of child and adolescent services in Western New South Wales and Central Western Australia rural areas: main types of care per 100,000 inhabitants aged 17 years and less. WNSW; Western New South Wales, CWA; Country Western Australia.
Discussion
The importance of complementing top down information with bottom up data using standardised methods and tools to facilitate comparability and aggregation has been highlighted by limitations identified in the WHO Atlas of MH (World Health Organization, 2021) and the Canadian Mental Health Commission (Canadian Mental Health Commission, 2016).This is related to the problem of ambiguity of official names of services and the lack of a reliable relationship between these names and the actual activity of the service. For example, a recent study in Europe identified that fewer than 25% of mental health services provide a clear description useable for health economics and resource allocation (Gutierrez-Colosia et al., 2022). Under these conditions, the use of a standardised method of describing the system of service availability at the local level is critical to evidence-informed policy.
Local patterns of healthcare provision for people under 18 years of age were investigated from a whole system perspective using the DESDE classification system. The higher ratio of outpatient care identified in this study replicates patterns previously described in low- and middle-income countries (Morris et al., 2011). The availability of other types of services vary across areas, from being completely absent in Country Western Australia to a limited availability in Australian Capital Territory. Since a system of care should consist of a wide range of services (Bickman, 2020), this imbalance may affect the efficiency of the whole system. Of the types of service missing, day care and residential (community, hospital and alternative to hospital such as crisis home) care services are of the most significance (Kennair et al., 2011). The lack of information for care services across all areas may be less significant due to the availability of online self-help tools and programs (Santana et al., 2011).
As expected, there was less diversity in the types of services available in rural than in urban areas. Rural and remote areas already have greater socioeconomic disadvantage and higher rates of mental ill health than urban and regional areas (Van Spijker et al., 2019), and the limited availability and diversity of services could add to the mental health burden and contribute to poorer outcomes in these regions (Lawrence-Bourne et al., 2020). There was no age-specific inpatient care available for children and adolescents in country Western Australia, a region that represents one third of the continent. Western New South Wales had acute hospital care and day care social support, but a limited diversity of types of outpatient care. Inadequate availability of outpatient support could arguably decrease the efficiency of inpatient services, with fewer services available to divert people from admission and limited discharge support options.
Rural access to quality mental health care has been recognised as an urgent issue by a 2018 Senate enquiry into ‘Accessibility and quality of mental health services in rural and remote Australia’ (Australia Senate, 2019). Whether this should be better achieved through the provision of more specialised services or through the augmenting of general care by specialists in rural and remote areas is a matter of ongoing debate (Perkins et al., 2019). Concerns about an over-reliance on hospital care and on specialist services in rural areas have been raised in the Orange Declaration on Rural and Remote Mental Health (Perkins et al., 2019). There is an urgent need to identify rural and remote patterns of service provision in Australia and to compare these at national and international level, to inform the development of models of care for these areas.
Limitations
Generalisation is always a challenge in bottom-up studies on health service and health system research. First, there is the problem of small numbers. There are only 31 PHNs in Australia. We have mapped mental healthcare provision in 11 of these (32%). To overcome the small number problem, we have followed a heuristic approach. A heuristics approach helps decision makers stop searching before the point where collecting more information provides no additional benefit: known as the ‘satisficing’ threshold (Djulbegovic et al., 2018). This approach also allows experts’ consideration in the analysis of complex problems such as mental health care (Marewski and Gigerenzer, 2012; Wolpert and Rutter, 2018). The 10 areas described in this analysis include both well resourced, and less well resourced, areas in urban and rural care in Australia and show a consistent pattern of care provision. Information from an 11th health district in Melbourne which showed a similar pattern of care to the other urban areas (CIT, personal comms) was not included in this analysis as the relevant Primary Health Network has not released its mental health atlas. Taking into account the proportion of the total number of Primary Health Networks that we have included in the study, and the repetition of patterns that we identified within these, we consider that this analysis provides a reliable representation of child and adolescent mental healthcare provision in Australia.
Second, there is a problem of local variation across areas and over time that is core to local health ecosystems research. This requires an approach based on systems thinking and organisational learning where the focus is on improving our knowledge base to optimise local planning more than in identifying a general pattern.
Data in the Atlases were not contemporaneous, but collected over 4 years, between 2014 and 2017. Nevertheless, comparisons of service availability over a similar time period and using the same method have been demonstrated in previous longitudinal studies (Fernandez et al., 2017). In Australia, we have conducted the longitudinal analysis of psychosocial services in Western Sydney and Australian Capital Territory pre and post introduction of the National Disability Scheme, a major reform to the provision of psychosocial care in Australia (GLOCAL, 2022).
We have included only those services for which there is little or no cost to the service user at the point of care. Services requiring significant out of pocket cost or access to private insurance are therefore not included. We have also excluded services providing generic rather than specialist mental health care, such as general practitioners. Separate mapping of these other levels of service provision could be conducted using this method.
Implications for policy and practice
The standard description of local service availability is essential for monitoring the implementation of new plans and strategies. It is as important as the description prevalence and incidence to assess unmet needs and to address the related care gaps. This information is also relevant for establishing care pathways, trajectories and costs, to assess the applicability of recommendations from clinical guidelines to the local context (Sullivan et al., 2018), and to adapt interventions to the local context (Rosalind Raine et al., 2016).
Future steps
This information could be used to inform planning at local, state and federal, and provide recommendations at every level of the mental health system (macro, meso and micro).
Importantly, this is the first step in an analysis of the whole system. Next steps should include analysis of placement capacity (e.g. number of beds), workforce (number, rate and professional composition), service utilisation including pathways of care, and assessment of service quality.
Future studies are needed to compare the pattern of child and adolescent mental health services over time and with other age groups, and to analyse generic child and adolescent mental health services (e.g. primary care, paediatrics) as well as subspecialised services such as services for eating disorders, transitional services and services for neurodevelopmental disorders. Another key area for research is the comparison of core child and adolescent services and transition to adulthood services.
Conclusions
The socioeconomic, geographic and demographic diversity of the areas included in the study enabled us to identify patterns of mental health care for children and adolescents across Australia. The findings of this study indicate that (1) outpatient care is the mainstay of service provision across all study areas in Australia for this population, with an overall lack of other types of service; (2) while health-related and social-support outpatient services are available in most areas, availability and diversity is greater in the former than the latter; and (3) in both urban and rural areas, hospital care is limited to acute hospital care. Service availability and diversity is lower in child and adolescent mental health services than in adult services, but higher than in services for older people.
These findings improve our knowledge and understanding of local child and adolescent mental healthcare ecosystems in rural and urban areas and enable further national and international comparison. This knowledge can be used to assist policy makers and inform decision making in policy planning and resource allocation at local and national levels.
Footnotes
Acknowledgements
CHECK This study used data from the research projects developed by the Glocal Integrated Mental Health Atlas project composed of researchers from the Australian National University (the mental Health Policy Unit), ConNetica Consulting Pty Ltd, University of Sydney and Universidad Loyola Andalucía. Authors wish to thank Western Australia Primary Health Alliance (WAPHA), Western New South Wales Primary Health Network (Western NSW PHN), and Eastern Melbourne PHN for the support in the development of the Integrated Mental Health Atlas in their jurisdictions. Especially to Learne Durrington, Daniel Rock, Linda Richardson, Frances Casella, Elaine Paterson, David Axworthy, David Naughton (WAPHA) and the project reference group; Janine Dennis and Jim Herbert (WNSW PHN), Susan Daly (Far West LHD) and Jason Crisp (WNSW LHD) and the project reference group; and Kieran Halloran (Mental Health Manager Severe and Enduring, EMPHN) and Anne Lyon (Executive Director Mental Health and AOD, EMPHN) and the project reference group.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Several authors of this paper participated in the development of DESDE-LTC (LSC, JAS, MRGC). These authors do not have any commercial interest in this instrument.
Funding
This research uses data from the Integrated Mental Health Atlases of Western Sydney (funded by Western Sydney Partners in Recovery, 2014); South Western Sydney (funded by South Western Sydney LHD, 2014); Sydney North (funded by Sydney North PHN, 2016); Central Eastern Sydney (funded by the University of Sydney, University SPARC Funding, and PIR East and South East Sydney, 2015); Australian Capital Territory (PHN Canberra ACT, 2016); Eastern Melbourne (funded by Eastern Melbourne PHN, 2018); Perth North, Perth south and Country Western Australia (funded by Western Australia Primary Health Alliance, 2018); and Western New South Wales (funded by PHN Western New South Wales, 2016).