
Abstract
From a global perspective, low helmet-wearing rates in children are an ongoing concern. International studies show adult helmet-wearing rates are consistently higher than those of children. Research also shows parents are highly influential in promoting healthy behavior in their children. Parent-focused helmet-wearing campaigns are a practical way to actively feature parents influencing helmet-wearing in children. The current study obtained anonymous parent-focused survey data on parent and child helmet-wearing practices, perceived affects of helmet use on children’s health, and beliefs about brain injury prevention from a sample of Vietnams parents. Findings from this study are consistent with previous international research that shows adults wear helmets at higher rates than children. Data from this study may help those responsible for child helmet safety campaigns develop more effective child helmet-wearing campaigns, particularly in Southeast Asian countries.
Introduction
Low helmet-wearing rates in children is an ongoing global concern (World Health Organization [WHO], 2022a). A recent 28-year meta-analyses of international research on adult and child helmet use found 44% of studies reported low helmet-wearing rates in children (Hoye, 2018). In the United States, child safety concerns have led to helmet-wearing laws for children in 22 states (Bicycle Helmet Safety Institute, 2020). Relatedly, research supports that wearing bicycle and motorcycle helmets reduces head injury and injury severity odds during serious road traffic accidents (Singleton, 2017; Strotmeyer et al., 2020).
In South-East Asia, motorized two- and three-wheel vehicles account for 43% of all road traffic fatalities (WHO, 2018). In Vietnam, motorcycles are a primary mode of transportation and road-traffic crashes are the second leading cause of death for children aged 5–14 and first among young adults aged 15–29 (McDonnell et al., 2017; WHO, 2012, 2018).
In June 2007, it became mandatory for motorcycle drivers and passengers to wear helmets on all roads in Vietnam (Government’s Resolution No. 32/2007/NQ-CP, 2007). Ten years later, more than 90% of adults and 30–40% of children over age six were reported by Vietnamese Government officials to be in compliance (Vietnamese Decree 04/CT-TTg, 2018). That same year, results from an independent study found 64% compliance rates in adults and 35% in children (Bao et al., 2017). Reasons given in Bao et al.’s study for not making children wear helmets included no perceived safety need, child resistance, and fear of hurting a child’s neck. More recent research shows helmet-wearing rates for children in Vietnam continues to be lower than in adults (Li et al., 2020; Nhan et al., 2019). Current Vietnamese helmet law (Socialist Republic of Vietnam, 2021) exempts children under age of six from wearing a helmet.
Since 2007, child helmet-wearing in Vietnam has received ongoing attention from policy makers and researchers (AIP, 2017; Nhan et al., 2019). Additionally, several nationwide campaigns have been organized to raise awareness about wearing helmets (Nhan et al., 2019). According to Trinh and Le (2016), these campaigns failed to clearly identify key audiences or indicate that non-helmeted children can sustain a severe brain injury during an accident. More importantly, they report most campaigns did not encourage parents to take an active role in assuring children wear a helmet. Trinh and Le (2016) suggest doing so is essential as “parents exert sway over their children’s helmet usage behaviour” (p. 11).
International studies have shown parents can be highly influential in promoting healthy behavior and habits in children and fostering their understanding of health risks (Eyre et al., 2015; Rodrigues et al., 2018; Song et al., 2012; Varkula et al., 2010; Wiese and Freund, 2011; Wymore et al., 2020). This may be especially true in Southeast Asian countries like Vietnam, where Confucianism-influenced filial piety values dictate that children must obey parents without question (Nguyen, 2016).
To date, most helmet-wearing safety campaigns in Vietnam have not featured parents actively influencing helmet-wearing in children (Trinh and Le, 2016). For example, in one media campaign, children were used in public service announcements to remind their parents of their parental responsibility to guide and educate children on helmet-wearing (Nhan et al., 2019). In order to effectively feature parents actively influencing child helmet-wearing in safety campaigns, it would be beneficial for campaign developers to understand how parents view helmet-wearing in children.
Child helmet-wearing studies in Vietnam have mostly been observations of street traffic compliance rates (Hung et al., 2008; Nguyen et al., 2013; Nhan et al., 2019; Li et al., 2020) or analysis of hospital road traffic injury or death prevalence rates (McDonnell et al., 2017; Silverman and Billingsley, 2016; WHO, 2018). Research studies collecting survey information on child helmet-wearing practices have involved interviewing adult participants (Bao et al., 2017; Pervin et al., 2009). This may have resulted in response bias (West and Blom, 2017). Research has suggested people tend to give more honest responses when answering questions anonymously (Muhlenfeld, 2005). To our knowledge this is the first anonymously administered parent survey on child helmet-wearing practices in Vietnam.
Aim
To explore parent/child helmet-wearing practices, perceived affects of helmet use on children’s health, and beliefs about brain injury prevention from a parent perspective.
Method
Ethics
This study was approved by Texas State University’s Institutional Review Board (6476). Each survey contained an informed consent coversheet and respondents gave consent by completing the survey. No incentives were given for participation. No individually identifiable information was collected that could tie a respondent to a survey. The right to withdraw and protection of anonymity through use of participant codes was explained in information sheets. Coded results were entered into an aggregate database and stored anonymously in accordance with Texas State University data management policy.
Sample and recruitment
This study sought to survey parents. Therefore, adults were approached in parking areas at elementary schools and invited to participate while picking up children or when leaving end-of-term parent-teacher conferences. Those adults who gave consent were handed a survey to complete. Researchers were available to answer questions and their contact information was in the survey cover page. To become a study participant, an individual had to state they were a child’s “mother” or “father” when asked: “What is your relationship with the child that you take to school?”
Data collection and survey
Data were collected using a paper and pencil survey. Participants placed completed surveys in a locked ballot-type box. Survey content consisted of demographic questions regarding participant residency, adult-child relationship, parent and child age, highest level of education, and child helmet-wearing practices. Following review of existing surveys used in Vietnam, clinical judgment was used by the study’s researchers to write a 25-item survey consisting of 12 true–false items, six yes–no items, and five demographic questions. Items were designed to examine information missing in previous surveys addressing parental beliefs regarding the affect of wearing a helmet on a young child’s health, child compliance with wearing a helmet, and injury prevention. Two questions, allowed respondents to write clarifying statements (“Do you wear a bike helmet while riding motorcycle? – Why” and “In your opinion, at what age should children started to wear a helmet while riding a motorcycle. –Why?”). In an attempt to reduce bias, two independent researchers with knowledge on survey preparation, Vietnamese culture, and helmet safety provided feedback on items; which was incorporated into the final survey (see supplementary materials).
Analysis
Data from surveys were entered into an Excel spreadsheet and aggregate results were imported into IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp, 2017) for frequency analysis. Non-normally distributed variables are reported as median and interquartile ranges. Percentage frequency distributions are provided for categorical data and item responses. Of the 511 completed surveys, any missing data was coded so as not be included in data analysis. When data were missing, number of missing respondents were indicated in tables as “Missing.”
Results
Study population
Sample size by residence, relationship to child, highest level of education, and parent/child age (N = 511).
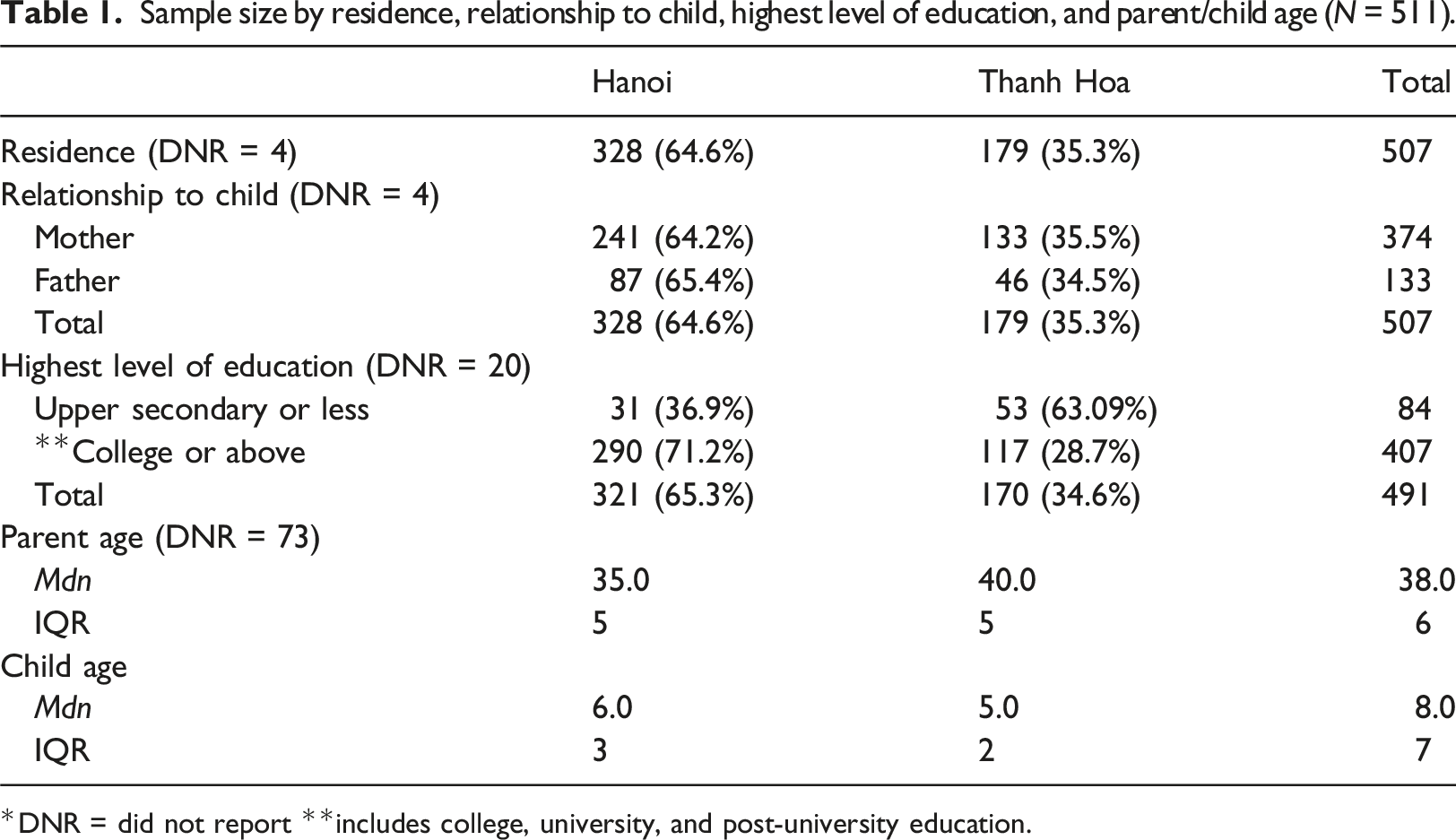
*DNR = did not report **includes college, university, and post-university education.
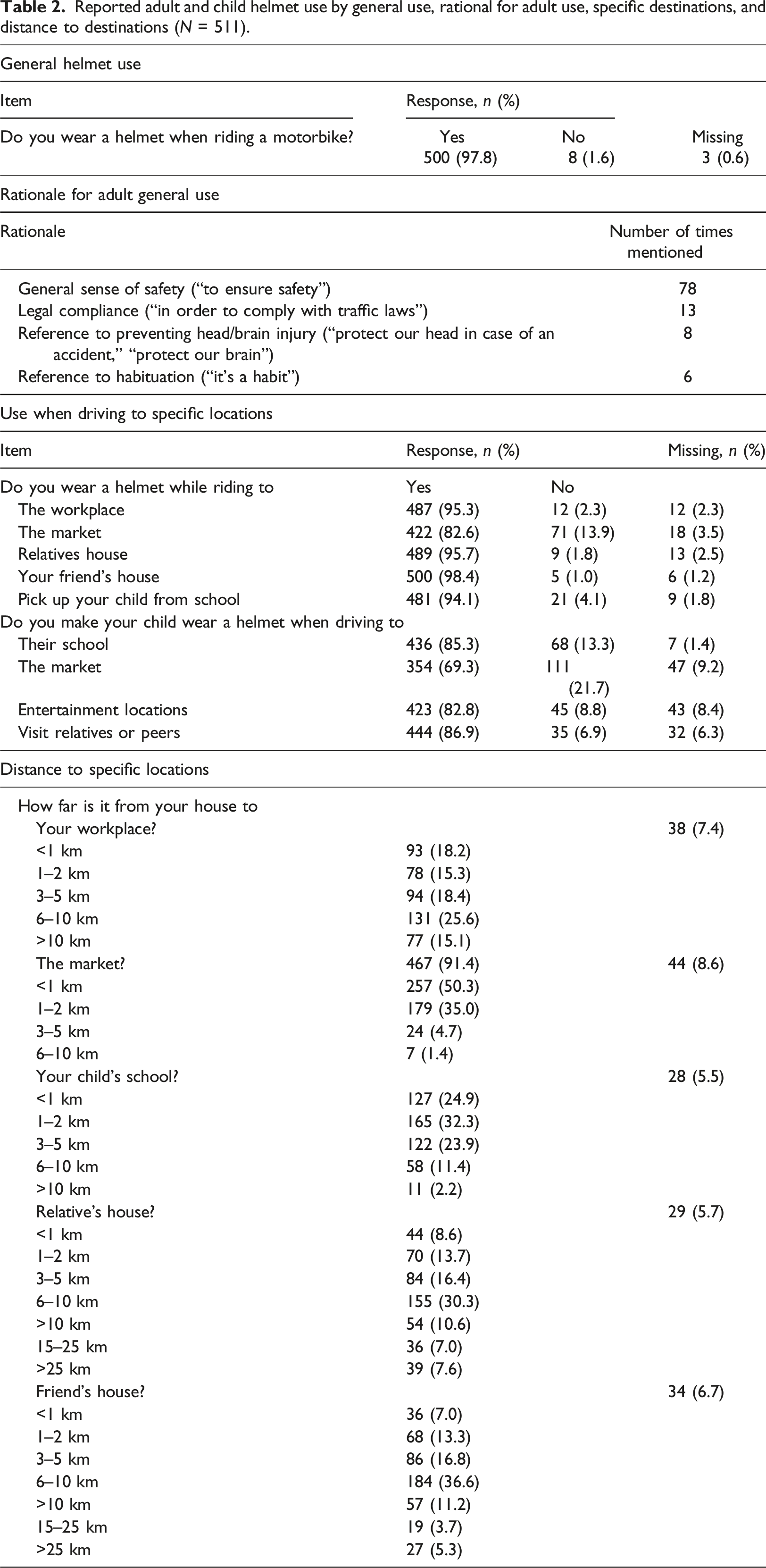
Helmet use
Reported adult and child helmet use by general use, rational for adult use, specific destinations, and distance to destinations (N = 511).
Age at which a child should begin wearing a helmet
Age a child should begin wearing a helmet when riding a motorbike and general rationales (N = 504).

Beliefs regarding helmet use and child health, child helmet-wearing compliance, and injury prevention
True/false response frequency percentages for beliefs regarding helmet use and child health, child helmet-wearing compliance, and injury prevention (N = 511).
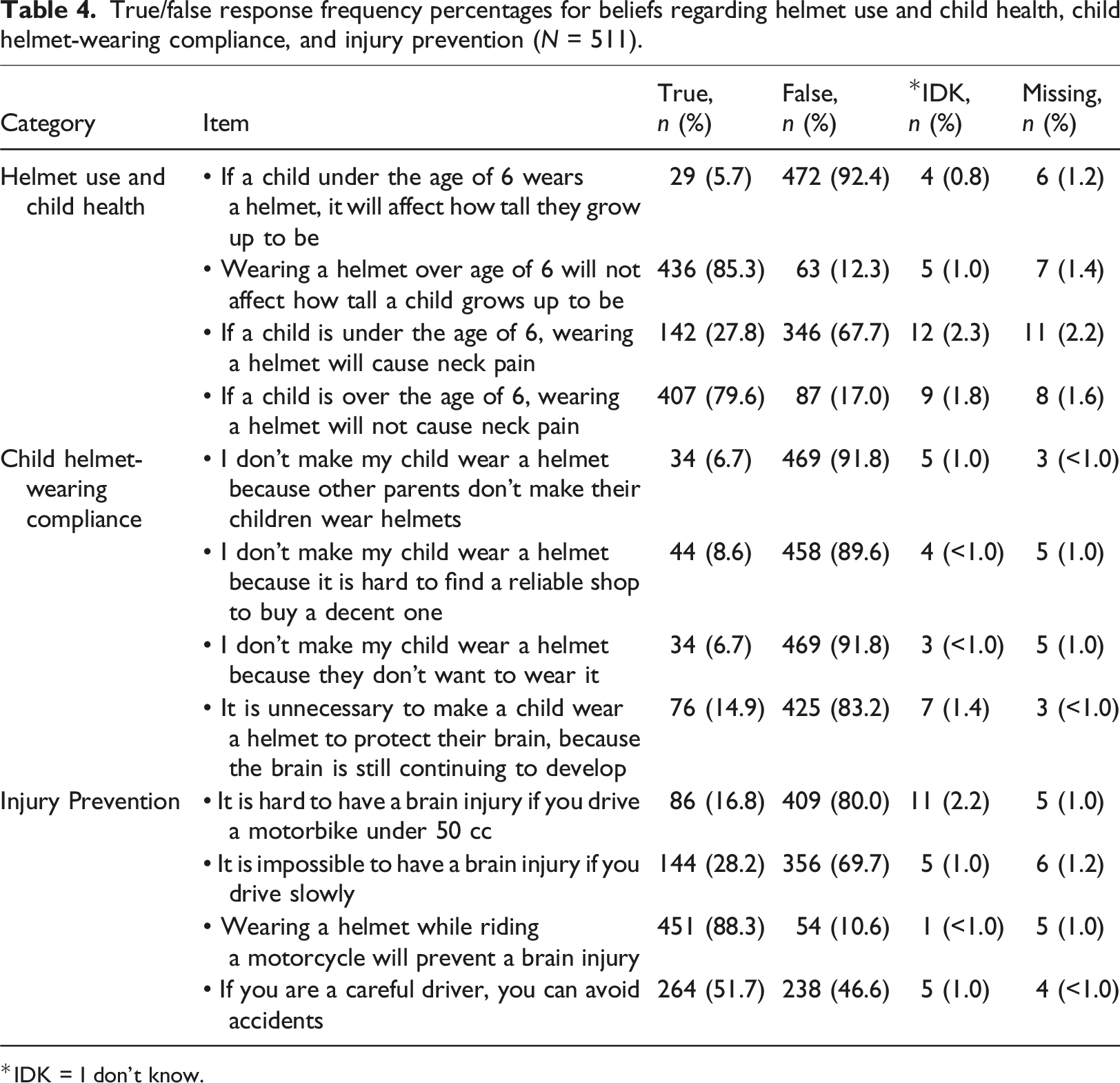
*IDK = I don’t know.
Discussion
This anonymous survey was administered to obtain anonymous parent-focused survey data on perceived affects of helmet use on children’s health, parent/child helmet-wearing practices, and beliefs about brain injury prevention. Our goal was to obtain data that could be used by child helmet safety campaign developers to create campaigns featuring parents actively influencing their children to wear helmets. Findings are discussed below.
Helmet use
Compared to Vietnamese interview/observation studies and data reported by Vietnamese Government officials (Bao et al., 2017; Li et al., 2020; Nhan et al., 2019; Nguyen et al., 2013; Vietnamese Decree 04/CT-TTg, 2018), our anonymously administered parent survey found differences and similarities in helmet-wearing practices. In contrast to previous studies (Bao et al., 2017; Nhan et al., 2019; Pervin et al., 2009), our study found higher helmet-wearing rates for adults. This may reflect stricter Vietnamese helmet law enforcement, a reported general sense of safety that wearing a helmet provides, a belief by respondents that wearing a helmet will prevent a brain injury, ongoing helmet-wearing campaigns targeting adults (AIP, Foundation 2017; Nhan et al., 2019), respondents’ level of education (Table 1), and/or the anonymous survey format.
Consistent with previous findings in Vietnam and globally (Hoye, 2018; Nhan et al., 2019; Li et al., 2020; Vietnamese Decree 04/CT-TTg, 2018), children in this study are reported to wear a helmet less often than adults. Although reported child helmet-wearing frequencies are lower than adults, reported compliance frequency was approximately one-third greater than previously reported (Bao et al., 2017; Nhan et al., 2019; Vietnamese Decree 04/CT-TTg, 2018). This increase may be related to reasons stated above and/or from questions asking about use in specific situations (market, peers, school).
Effect of wearing a helmet on a child’s health
Given that Vietnam helmet law does not require wearing a helmet prior to age six, an interesting finding is that nearly half of parents surveyed believe a child should wear a helmet before age of six. They also believe doing so would not have an adverse effect on a child’s health. This is in contrast, however, to approximately one quarter of parents in this survey, and those in previous studies (Bao et al., 2017; Nhan et al., 2019), who believe doing so would have an adverse effects on a child’s health. This discrepancy may be result of this study’s overall higher respondent educational level.
Child compliance with wearing a helmet
When it comes to enforcing helmet use in children, most parents in this study do not appear to be unduly influenced by previously identified common helmet-wearing deterrents (Bao et al., 2017; Pervin et al., 2009). This does not mean that deterrents do not exist. It means deterrents examined in this study (parent peer pressure, child resistance, lack of helmet availability, no perceived need) were only endorsed by a few parents. Barriers identified in studies conducted outside of Vietnam (Lajunen, 2016; Safe Kids Worldwide, 2017; WHO, 2022b; Wymore et al., 2020) should be explored in future studies.
Injury prevention
Findings about injury prevention were mixed and reveal common misconceptions (McKinlay and Buck, 2019; O’Brien et al., 2019; Ogunfolaji et al., 2021). Regarding misconceptions, an alarming number of respondents believe that wearing a helmet will prevent a brain injury (Table 4). There is little doubt that properly wearing well-constructed helmets is associated with lower rates of severe head/brain injury during serious accidents (Abbas et al., 2012; Chalya et al., 2014; Liu et al., 2008; MacLeod et al., 2010; Olsen et al., 2016; Rice et al., 2016; Singleton, 2017). Nevertheless, there are many injury-inducing biomechanical physics occurring within milliseconds of a head impact (Martin, 2016), and helmets cannot always prevent these from occurring. That is, a major function of any helmet is to absorb and displace impact energy during an accident (Fernandes and de Sousa, 2013; Rice et al., 2017). Although a helmet may displace enough linear force energy to prevent skull fractures, it is significantly less efficient at reducing angular/rotational acceleration energy responsible for diffuse axonal shearing/twisting injuries (Singleton, 2017). It is true that in minor head impacts a helmet may absorb and displace enough energy to only induce a concussion; however, a concussion is still considered to be a brain injury (Menon et al., 2010). Therefore, maintaining a perception that helmets prevent brain injury may give a false sense of invulnerability and lead to reckless/careless driving or driving at higher speeds.
Most respondents recognize a brain injury is still possible when riding a smaller (<50 cc) motorbike and driving slowly will not prevent a brain injury. That said, more than half of respondents believe careful drivers can avoid accidents (Table 4). Erroneously believing skillfull driving can prevent accidents and thereby absolve drivers from wearing helmets has been previously identified in research on helmet use (Hung et al., 2008). Although our study’s rate is significantly below respondents in Hung et al.’s 2008 sample, it is still a dangerous misconception to maintain. Careful driving may reduce a person’s odds of causing an accident, however, it does not prevent those who are not careful drivers from involving a careful driver in an accident. Beyond possible deadly consequences of believing that careful driving provides immunity from accident involvement, this misconception can reinforce noncompliance with child helmet-wearing.
Limitations
The following are limitations. This study involved a convenience sample of urban-dwelling Vietnamese adults in which the majority of participants were highly educated individuals. This may limit generalizability of results to those living outside Vietnam, to individuals who have not acquired post-secondary educations, and to those who live outside urban areas. Mothers outnumbered fathers in this study by nearly three to one. Therefore, results may not accurately represent views of fathers. Future research efforts should seek to address this imbalance. This study’s small sample size should also be considered when interpreting results and larger samples should be sought in future studies. The use of self-report is subject to bias and over-/under-reporting. Social desirability may have increased respondents reported helmet compliance rates in order to appear to comply with helmet laws and/or practice socially desired healthy behaviors. Although adult views on helmet-wearing practices are important and informative, so are those of children. A clear limitation of the current study is that no children were surveyed to corroborate what parents were endorsing. Furthermore, children’s perceptions of the value/use of helmets were not explored. Thus, future research should include a direct exploration of children’s attitudes/perceptions toward helmet-use (from their perspective), as well as, explore factors influencing their helmet-use. Additionally, helmet-wearing campaign developers should involve appropriately aged children as member on their campaign development committees and use results of child-focused surveys when developing future helmet-wearing campaigns. Finally, this exploratory study’s survey was not piloted nor validated, which limits its generalizability. Further refinement and validation of the survey questions would increase overall generalizability of future results.
Implications for practice
Findings from this study can help campaign developers in Southeast Asian countries like Vietnam create effective child helmet safety campaigns that take advantage of known parental influence over children’s healthy practices. More specifically, developers can use this study’s findings to create campaigns featuring parents actively engaged in educational conversations with other parents about benefits associated with child helmet-wearing practices, perceived affects of helmet use on children’s health, and misconceptions about brain injury prevention, while at the same time encouraging parents to helmet their children when riding as passengers. This approach may be particularly effective in Southeast Asian countries with Confucianism-influenced filial piety values, as this value may be a keystone to successful attempts to increase helmet-wearing compliance in children.
Although this study’s findings suggest many parents would respond positively to child helmet-wearing campaigns that encourage helmet-wearing in children under age six, it may be challenging to find quality helmets designed for this age group. Finally, future research on children’s perspectives about helmet-wearing is warranted.
Conclusion
In this article, we reported findings of an anonymous qualitative study of parent/child helmet-wearing practices, perceived affects of helmet use on children’s health, and beliefs about brain injury prevention. Our findings suggest helmet-wearing practices in adults has increased in Vietnam; however, as in other countries worldwide, child helmet-wearing rates remain consistently below that of adults. Moreover, our findings suggest misconceptions about helmet injury prevention and driving safety practices, which exist in other countries (McKinlay and Buck, 2019; O’Brien et al., 2019; Ogunfolaji et al., 2021), prevail in Vietnam. We believe findings from this study may be used globally to develop helmet-wearing campaigns actively featuring parents influencing their children to wear helmets; especially in Confucianism-influenced societies in which filial piety dictates that children must obey parents (Nguyen, 2016). These campaigns could also focus on correcting misconceptions related to helmet injury prevention and safe driving practices.
Footnotes
Author contributions
All authors contributed to the study conception and design, data acquisition, analysis, interpretation, and writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.