
Abstract
Pain in hospitalized infants, children, and young people (ICYP) is a well-known phenomenon but remains undertreated. This study aimed to examine documented pain management practices provided for ICYP and compare practices adopted in neonatal and pediatric units. This national retrospective multi-center study was conducted in 40 of the 42 Danish neonatal and pediatric units in November 2020. Data were collected from the medical records of ICYP admitted to a participating unit. We performed a total of 846 medical record audits of which pain was assessed in 51.9% of the ICYP. Pain assessment was documented for more infants (57.8%) than for children and young people (CYP) (47.4%) (p = 0.003). CYP more often received pain treatment (37.7%) than infants (6.9%, p < 0.0001) and more frequently had a pain treatment plan (50.8% versus 10.2%, p < 0.0001). Use of non-pharmacological treatment was documented for 6.3% of the ICYP. Our findings indicate that pain assessment is insufficiently documented in Danish neonatal and pediatric units. Among cases in which pain scores indicated that the patient had experienced pain, pain treatment was documented in a larger proportion of the pediatric population than in the neonatal population.
Background
Pain management (assessment and treatment) in infants, children, and young people (ICYP) is complex and influenced by ICYP and clinicians alike (Whitley et al., 2021). The need for evidence-based pain management for hospitalized ICYP has been stressed (Friedrichsdorf and Goubert, 2019; Hall and Anand, 2014). However, ICYP pain frequently goes undetected and is therefore undertreated and unrelieved (Twycross et al., 2016). This may result in preventable suffering (Birnie et al., 2014; Shomaker et al., 2015). Untreated pain may have several long-lasting negative consequences including needle phobia, procedural anxiety, and healthcare service avoidance (Friedrichsdorf and Goubert, 2019). Pain in preterm infants is associated with increased morbidity and mortality (Anand et al., 1999) and may alter neurological development and pain response later in life (Eccleston et al., 2021; IASP, 2020). To ensure ICYP pain management quality in hospital settings, pain treatment must be continuously assessed and documented.
Pain treatment involves pharmacological and non-pharmacological interventions (Friedrichsdorf and Goubert, 2019), which are administered according to patients’ age and weight. Non-pharmacological interventions for infants include sucrose, breastfeeding, non-nutritive sucking, facilitated tucking, and skin-to-skin contact (Friedrichsdorf and Goubert, 2019). Age-specific non-pharmacological interventions for CYP include distraction with a pacifier, toys, virtual reality glasses, tablets, and sitting with parents (Friedrichsdorf and Goubert, 2019).
Using objective pain scales facilitates identification of pain and thereby pain management and may serve to prevent untreated pain and unnecessary medication (Hall and Anand, 2014). Thus, the objective of documenting pain assessment reaches far beyond simply documenting the presence or absence of pain; indeed, documentation serves to make pain visible for healthcare professionals (HCP) to ensure continuity in ICYP pain management (Manworren and Stinson, 2016). Two Danish National Guidelines on ICYP pain assessment provide recommendations on age-appropriate pain assessment. One guideline, initially published in 2010, covers neonatal infants (Haslund et al., 2015) and recommends using the COMFORTneo scale (Van Dijk et al., 2009). The second guideline, published in 2016, covers infants from 28 days of age, children and young people (CYP) and employs a total of five age-appropriate scales (Pedersen et al., 2016). With the publication of the neonatal guideline, a comprehensive 2-year national implementation program was also initiated (Stenkjaer et al., 2019).
Although evidence-based clinical guidelines aiming to ensure adequate assessment and treatment of ICYP pain are available to clinicians, practice does not always conform to recommendations (Carvalho et al., 2022; Friedrichsdorf and Goubert, 2019). Furthermore, it has been established that younger children receive less pain treatment than older children (Friedrichsdorf and Goubert, 2019; Orovec et al., 2019). Pain management and documentation is customarily undertaken by nurses at Danish hospitals. Previous studies of ICYP pain management were primarily based on data from a single or few hospitals and did not have a nationwide perspective. However, such individual-level nursing practice observations focusing on pain assessment are not a feasible approach in a nationwide study. As documentation of pain management is mandatory in Danish medical records (Dons AM, 2013), a medical record audit seems feasible and the best possible approach in this nationwide study on pain assessment and treatment in Denmark.
Aim
To 1) examine HCP’s documented pain assessment practices and pharmacological and non-pharmacological pain treatment of ICYP, 2) compare neonatal and pediatric unit practices, and 3) explore and describe pain management characteristics.
Methods
Study design and participating units
This cross-sectional retrospective multi-center study was conducted using audit tools to evaluate pain assessment and pain treatment in hospitalized ICYP. All 42 Danish neonatal and pediatric units in 18 Danish hospitals offering such services were invited to participate. Danish neonatal and pediatric units provide treatment and care to ICYP from birth to 18 years of age.
Population
We collected data from electronic medical records of all ICYP admitted to a participating neonatal or pediatric unit from 3 November to 5 November 2020. Inclusion criteria for medical record auditing were that the ICYPs had been admitted for a minimum of 24 h at the time of their audit. Audit exclusion criteria were ICYP on hospital leave or hospital treatment for less than 24 h during leave.
Data collection tools
We developed both a neonatal and a pediatric audit tool for data collection aimed at the populations constituting the target groups of the two Danish national clinical guidelines on pain assessment (Haslund et al., 2015; Pedersen et al., 2016). The neonatal tool was developed for infants with a postmenstrual age of ≤44 + 0 admitted to neonatal units, whereas the pediatric tool was developed for IYCP admitted to pediatric units.
The neonatal tools included 45 variables; the pediatric tool, 43 variables. The variables included basic information on a 24-h audit day: hospital and unit, date of birth, date of admission, sex, admission for medical or surgical reason (or both), (semi-)intensive treatment, and surgery within the past 7 days. Outcome variables were documented separately for each day, evening, and night shift on audit days and covered: documented pain assessment, highest pain score, documentation of reason why pain was not assessed, individual plans for pain treatment, type of pharmacological and/or non-pharmacological pain treatment, and re-assessment evaluating treatment effectiveness.
The two audit tools differed in options for pain assessment and pain treatment in drop-down menus. Thus, the non-pharmacological treatment options “adjustment of surroundings” and “sucrose” were included only in the neonatal audit tool. In Denmark, sucrose is defined as non-pharmacological treatment that requires no prescription. The pharmacological treatment options nitrous oxide and general anesthetic and the non-pharmacological treatment distraction were included only in the pediatric tool. Data on gestational age were collected only in the neonatal tool.
Both tools were pilot tested by the authors and four nurses from three participating units. While the audit tools were being developed, revisions were made based on the authors’ comments. After pilot testing with nurses, no further revisions were needed.
Study data were collected and managed using Research Electronic Data Capture (REDCap) tools hosted at the Capital Region of Denmark. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture, 2) audit trails for tracking of data manipulation and export procedures, 3) automated export procedures for seamless data downloads to common statistical packages, and 4) procedures for data integration and interoperability with external sources (Harris et al., 2009, 2019).
Data collection
The study was conducted on 3 days; November 3–5, 2020. The medical record for a specific ICYP could be included for one, two, or all three audit days, depending on the time of admission and length of hospital stay. Each participating unit designated a single person tasked with collecting and entering all data into the REDCap database on the three audit days. The designated person received written material with information about the study and guidelines for data entry. The audit tool guidelines provided detailed information that clarified each audit question. If any questions or doubts arose during audit days, members of the study group (the authors of this paper) were reachable by phone. In addition to entering data into the database, the designated person was asked to complete a document on each study day recording the number of ICYP eligible for and the number of ICYP included in the audit.
Ethical considerations
The study was approved by the Knowledge Centre on Data Protection Compliance (P-202–843) and by the Danish Patient Safety Authority (REC no: 31–1521-415). With these approvals, signed consent from the parents and young people (age ≥15 years) was not required under Danish law. The management of each participating unit provided a signed letter of consent permitting data collection from medical records. Data collected from medical records were anonymized for publication.
Analysis
A 3-day data collection period was estimated to yield a reasonable number of included audits. We conducted no power calculation as we had no a priori hypotheses of the magnitude of any differences between neonatal and pediatric units. The sample was considered representative of Danish neonatal and pediatric units as 95% of all such units participated in the study. Data were analyzed using descriptive statistics. We used the chi-squared test to examine statistically significant differences between variables. ICYP were deemed to have been assessed for pain if any pain assessment was documented during the 24-h audit period; similarly, they were considered to have received pain treatment if any non-pharmacological or pharmacological treatment was documented during the 24-h audit period. Each study day was divided into three working shifts. To analyze if pain scores indicating pain resulted in pain treatment, the highest documented pain score in each shift was categorized as pain/no pain. The cut-off score indicating pain was 14 in COMFORTneo (Haslund et al., 2015). The scales used for pain assessment in CYP was FLACC (face, legs, activity, cry, and consolability) (Merkel et al., 1997), visual analog scale (VAS) (Price et al., 1983), and numeric rating scale (NRS) (Hjermstad et al., 2011). To avoid overestimating pain, we estimated that CYP had pain if they scored >3. Data on ICYP characteristics were missing for less than 2% of the audits, and data were analyzed with the number of responses. Data on pain assessment and treatment were missing for less than 3% of the audits and were considered to be missing completely at random; missing data were interpreted as non-compliant (not pain assessed, not pain treated, and reason for lacking documentation not assessed), and data were analyzed with the total number of audits. Data were analyzed using Statistical Package for the Social Science (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp). A p-value of <0.05 was considered statistically significant. Data are available on request.
Results
Distribution of 846 audits and documented pain assessment.

Characteristics of sample in audits.
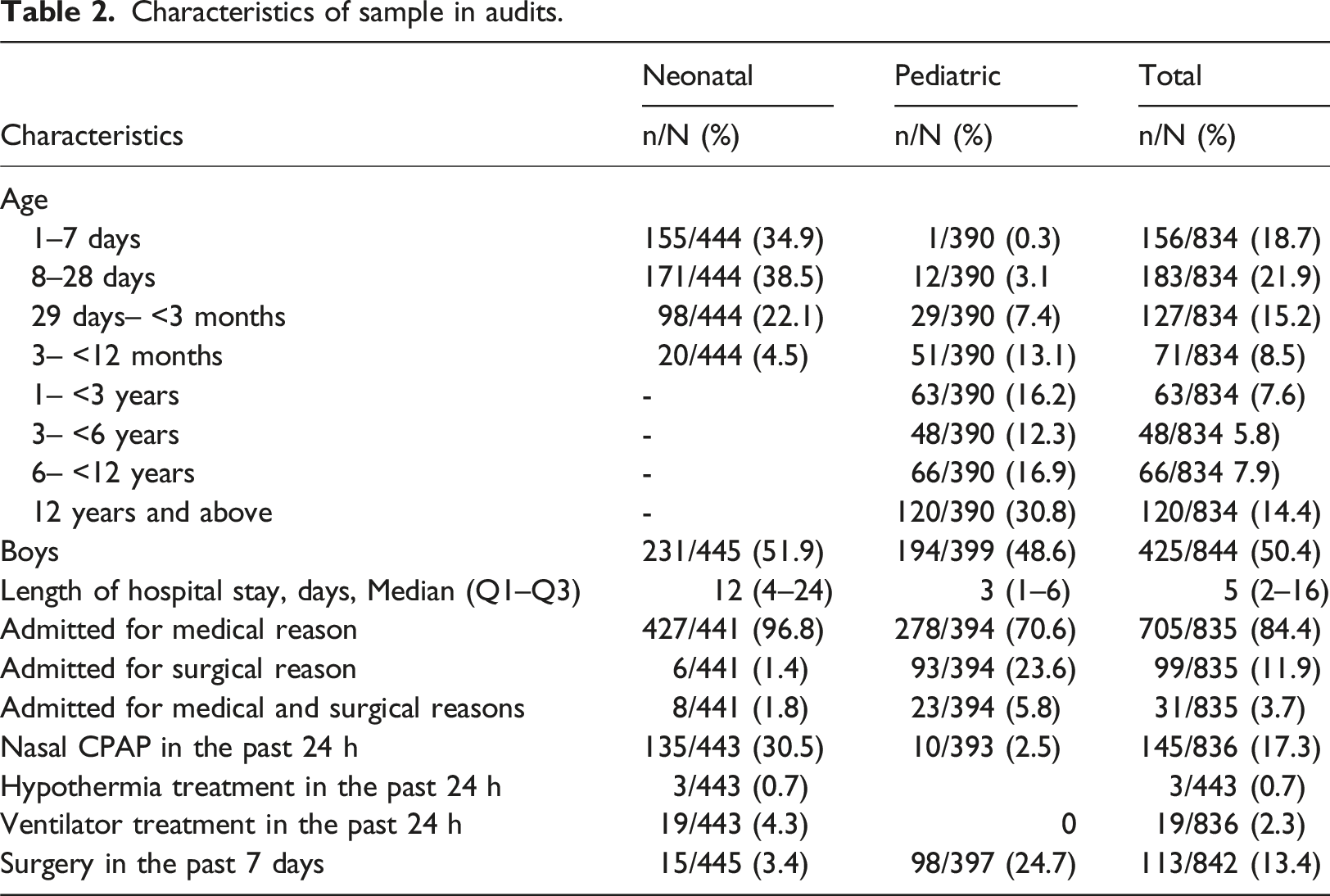
A total of 252/846 (29.8%) ICYP received pain treatment; 198/856 (23.4%) pharmacological, 16/846 (1.8%) non-pharmacological, and 38/846 (4.5%) a combination of pharmacological and non-pharmacological treatment.
Pain assessment and treatment in neonatal units
Pain assessment and management in neonatal and pediatric units.
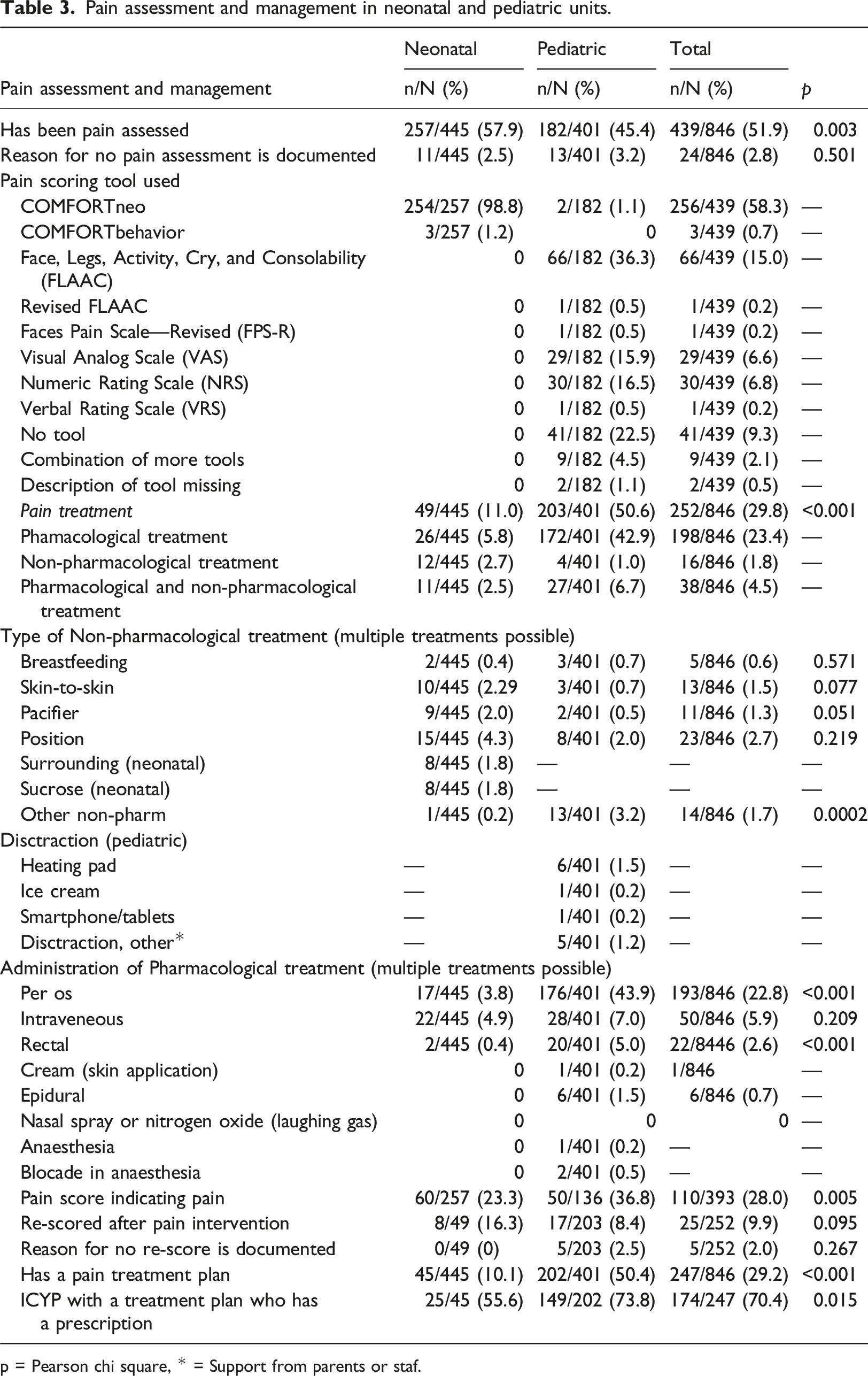
p = Pearson chi square, * = Support from parents or staf.
Pain assessment and treatment in pediatric units
Pain assessment was documented in 182/401 (45.4%) pediatric medical records (Table 3) with clinically and statistically significant differences between all three daily shifts being recorded as follows; day shift 135/401 (33.7%), evening shift 103/402 (25.7%), and night shift 67/401 (16.7%) (p < 0.0001). Reasons for not performing pain assessment were seldom documented. Seven different pain assessment tools were used, with FLACC being the most frequently used tool. The second most frequent choice of pain assessment was to not use a tool. In total, 203/401 (50.6%) of CYP received pain treatment. Per os route was most frequently used as pharmacological treatment (Table 3). Non-pharmacological interventions were rarely documented. Distraction methods not documented during the three audit days included virtual reality glasses, guided imagery, bubble blowing, and use of a hospital clown, play specialist, and kindergarten teacher.
Variations in pain assessment and treatment
Among 846 audits, more infants 257/445 (57.9%) than CYP 182/401 (45.4%) had pain assessment documented at least once in 24 h (p = 0.003). More ICYP with a pain treatment plan than without a plan were pain assessed, (154/247 (62.3%) versus 285/599 (47.6%), p < 0.001). Pain assessment was more often documented during a 24-h period for ICYP who had undergone surgery within the past 7 days (25/113 (22.1%) versus 96/729 (13.2%), p = 0.012), who were mechanically ventilated (15/19 (78.9%) versus 106/827 (12.8%), p < 0.0001), or who had nasal continuous positive airway pressure (CPAP) (31/145 (21.4% versus 90/701 (12.8%), p = 0.007) than for patients without these treatment interventions. In addition, we found statistically significant differences in the proportion of ICYP having been pain assessed at least once in a 24-h period between hospitals (5/49 (10.2%) to 28/28 (100%), p < 0.0001) and units (0/23 (0%) to 28/28 (100%), p < 0.0001). During a 24-h audit, CYP more often received pain treatment (203/401 (50.6%) than infants (49/445 (11.0%), p < 0.0001). In those with pain scores indicating pain, pain treatment was documented in more of the pediatric than neonatal medical records (49/50 (98.0%) versus 22/60 (36.7%), p < 0.0001).
Discussion
In this national study, we investigated documentation of pain assessment and treatment by auditing medical records of ICYP admitted to neonatal and pediatric units. Our results show that pain assessment was documented in slightly more than half of the medical records. Pain assessment was more frequently documented in neonatal medical records than in pediatric medical records. However, pain treatment was less frequently documented for infants than for CYP. Non-pharmacological interventions were seldom documented.
In pediatric units, pain was mostly assessed without using a particular tool. Opposite, in neonatal units, COMFORTneo was consistently used for pain assessment. This difference between pediatric and neonatal units may reflect the comprehensive national implementation of the Danish guideline for neonatal pain assessment. Furthermore, as from 2016, pain assessment during the first 24 h after admission has served as a quality indicator in the Danish Newborn Quality Database (Database, 2021). Hence, both of these initiatives may have contributed to boosting the frequency of pain assessment in neonatal audits and ensuring consistent use of a single tool. This is in line with Reavey and colleagues who reported that quality improvement projects increased pain assessment documentation (Reavey et al., 2014; Ozawa et al., 2017). The implementation of pain assessment in pediatric units has not received the same national focus and a variety of tools were used in those cases where pain assessment was conducted. Other studies have documented gaps between the clinical practice of pain assessment and guideline recommendations (Olsen et al., 2020; Melia et al., 2019). Furthermore, whereas the national clinical guidelines on CYP pain assessment do provide suggestions for tools and ages, the guidelines lack specific recommendations. Similarly, the Danish national guidelines (Pedersen et al., 2016; Haslund et al., 2015) recommend regular neonatal and pediatric pain assessment but fail to stipulate how often ICYP should be pain assessed during hospital admission. Additionally, several participating hospitals reported having developed local add-ons to the national guidelines that recommended no further pain assessment if no pain was detected at admission. Hence, national clinical guidelines should provide distinct recommendations to establish a firm basis for a nationwide pain management.
We found that in cases where pain scores indicated pain, more CYP than infants received pain treatment. A similar finding was previously reported (Shomaker et al., 2015) indicating that awareness of the need for pain treatment is higher among CYP than among infants. Overall, more CYP than infants received pain treatment, and fewer CYP than infants were pain assessed Another explanation for our finding may be that COMFORTneo measures both pain and distress (Van Dijk et al., 2009). The high scores observed may therefore indicate distress rather than pain. Nevertheless, distress should be treated with non-pharmacological interventions. Evidence shows that a variety of non-pharmacological interventions may effectively manage pain response to painful procedures in preterm infants, term newborns, and older infants (Cignacco et al., 2007; Pillai Riddell et al., 2011). In the present study, non-pharmacological treatment was documented at a surprisingly low rate of 6.4%. We therefore suspect that non-pharmacological treatment is heavily under-documented. Other studies have also reported low documentation of non-pharmacological interventions (Birnie et al., 2014; Carvalho et al., 2022), and they have shown that compared with other infants, immature and sick infants receive fewer pain-reducing interventions (Orovec et al., 2019). In a previous Danish study including children and parents from four hospitals, many reported the use of non-pharmacological interventions (e.g., 34% caregiver participation, 18% breastfeeding/sucrose, and 13% distraction) (Walther-Larsen et al., 2017). This study did, however, not comprise documentation of these interventions in medical records. Even so, the findings by Orovec et al. do support a wide use of non-pharmacological interventions in ICYP and the presumption of under-documentation of non-pharmacological interventions in our study. The lack of documentation of support from hospital clowns and play specialists during painful procedures may possibly be explained by restricted access to hospitals during the Coronavirus disease 2019 (COVID-19) pandemic. Under normal circumstances, hospitals clowns are everyday partners to clinical staff in pediatric units in Denmark. Moreover, Denmark has no tradition for documenting either non-pharmacological interventions such as sucrose during painful procedures in infants or the use of distraction in CYP. To prevent procedural pain in the neonatal population, sucrose is used consistently. Furthermore, sucrose use is implemented to the extent that even parents and medical laboratory scientists are trained in its administration during procedures, which may potentially lead to a less consistent and systematic documentation.
Although HCPs report that they would use non-pharmacological treatment (e.g., distraction), they are often challenged when needing to balance the many agendas, rights, and priorities. Therefore the child’s voice and rights are often ignored and the measures therefore fail to benefit children’s long-term outcomes (Bray et al., 2018). This may potentially also explain the minimal documentation of non-pharmacological interventions observed in the audits. With non-pharmacologic treatment documented in only approx. Six percent of the medical records, a potential exists for increased awareness among HCPs of the need to improve non-pharmacological treatment and documentation in neonatal and pediatric clinical practice.
Inadequate pediatric pain management may be caused by a lack of knowledge, understanding, or training (Eccleston et al., 2021). Myths, misunderstandings, and practical barriers may also contribute to this suboptimal clinical practice (Harrison, 2020). Studies have shown that HCPs lack theoretical knowledge regarding ICYP’s perception of pain (Marseglia et al., 2019; Manworren, 2015).
Strengths and limitations
This national study was conducted with a robust participation of 95% of the neonatal and pediatric units in Denmark and all eligible ICYP were included. To ensure consistency and quality of data, each participating unit allocated a person to identify IYCP for the audits and for collect data.
Despite the robust participation, some limitations need to be considered. The intention with the two audit tools was that they should be used according to ICYP age, but in practice, the choice of tool seemed to be guided by the type of hospital unit, not the age of the recipient. As the non-pharmacological treatment options “adjustments of surroundings” and “sucrose” were present only in the neonatal tool, they may have been under-reported in the pediatric audits. However, the pediatric tool allowed HCPs to record other types of non-pharmacological treatments.
Another consideration is that local hospital guidelines may have influenced how often pain was assessed and which ICYP underwent pain assessment. Local recommendations may potentially run counter to the provisions of national clinical guidelines, that is, by stipulating that CYP suffering from functional disorders should be excluded from systematic pain assessment. Guidelines have suggested cut-off scores for pain interventions that we used to estimate CYP with pain. However, it is a limitation that VAS and NRS are subjective self-reported scales and pain is a subjective experience. The cut-off values for FLACC, VAS, and NRS are ≥ 2–4 in the local guidelines. To avoid overestimating pain in CYP, those with scores >3 were considered to be in pain.
Thus, the proportion with pain who received pain treatment may have been underestimated. Furthermore, data were collected during the COVID-19 pandemic, and some of the participating units prohibited use of hospital clowns who are otherwise regularly used as distraction during procedures in pediatric units. Therefore, the normal use of distraction might have been underestimated.
Even though some activities related to pain assessment and treatment may not be entered into the ICYP’s medical records, we assume that the documentation reflects actual practice and may serve to provide insights into the current pain management of ICYP in Denmark.
We made an effort to avoid collecting personal data on the ICYP, such as names or social security numbers. Therefore, we were unable to trace data back to the individual ICYP or identify how many ICYP were audited 1, 2, or all 3 days during the study period. Finally, it needs to be stated that this type of study presents only the documented practice of pain assessment; discrepancies may exist between our collected data and current clinical practice.
Implications for clinical practice
Despite national and regional clinical guidelines, pain assessment remains underdocumented in medical records. Therefore, an enhanced focus is needed on documentation of pain management in daily clinical practice to ensure continuity of pain management during treatment and throughout the care trajectory. Furthermore, findings from this study indicate that some ICYP do not receive pain management even though their assessment indicates that they are in pain. Local guidelines may run counter to national guidelines thereby increasing the risk that hospitalized ICYP’s pain goes undetected, thereby causing undertreatment. Clinical practice must therefore ensure that local guidelines are rooted in evidence-based national clinical guidelines.
Conclusion
This national study on pain management in Danish neonatal and pediatric hospital units revealed that pain assessment is unsatisfactory in these settings. Pain assessments were more frequently documented in neonatal than pediatric medical records. However, in records with pain scores indicating pain, CYP received pain treatment more frequently than neonates did. Furthermore, documentation of non-pharmacological interventions was sparse, indicating that these interventions are under-documented in the hospital medical records of IYCP.
Further studies using field observations and interviews are warranted to further describe current practices in documenting neonatal and pediatric pain management and thereby facilitate development and testing of implementation strategies aiming to optimize neonatal and pediatric pain management.
Footnotes
Acknowledgements
The authors would like to thank all the participating units and a special thanks to the people in the units reporting data for the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Knowledge Centre on Data Protection Compliance (P-202-843) and the Danish Patient Safety Authority (REC no: 31-1521-415). With these approvals, signed consent from the parents and young people (age ≥15 years) were not required. The management of each participating unit provided a signed letter of consent permitting the collection of data from medical records. Data collected from medical records were anonymized for publication.