
Abstract
Background:
Evidence on associations of remnant cholesterol (RC) and its variability with cognitive function is still lacking.
Objective:
To explore the association of RC and its variability with cognitive function.
Methods:
Participants were recruited from a population-based cohort, the China Health and Retirement Longitudinal Study (CHARLS). Cognitive function was assessed by a standardized questionnaire from CHARLS, with domains of episodic memory and mental intactness. A linear mixed effects model was used to analyze the association of RC with cognitive function, along with its variability (calculated as standard deviation [SD], coefficient of variation [CV], variability independent of the mean [VIM]), with results expressed as β (95%CI). Potential subgroup differences in the association of RC and its variability with cognitive function were also explored.
Results:
4234 participants were eventually included, with mean (SD) age of 57.4 (8.0) years. Each 10 mg/dL increase in RC was associated with 0.053 (95%CI: 0.096, 0.009) points, 0.021 (95%CI: 0.042, 0.000) points, 0.032 (95%CI: 0.064, 0.001) points decrease in global cognitive function, episodic memory, and mental intactness scores, respectively. Compared with the first tertile (T1) group of RC variability (calculated as SD, VIM), T3 showed a lower level in global cognition and episodic memory after multivariate adjustment. The potential modification effects of educational level on RC and its variability in relation to cognitive function were also identified.
Conclusions:
Among Chinese middle-aged and older adults, higher RC level were associated with worse cognitive function. Greater RC variability was also associated with worse cognitive performance, especially in memory function.
Introduction
Cognitive function is an important factor for physical and mental health and normal social function among older adults. Cognitive impairment refers to dysfunction in any cognitive domain such as language, memory, visuospatial ability, attention, and executive capacity due to various causes, 1 and is generally classified as mild cognitive impairment (MCI) and dementia according to the severity of the disease. Cognitive impairment has imposed a great burden on health provision and the economy, as well as having devastating effects on patients and their families. A recent large-scale cross-sectional study showed that, the prevalence of MCI and dementia among population aged 60 years and older in China was about 15.5% and 6.0%, respectively. 2 Meanwhile, the annual cost of treating Alzheimer's disease (AD) in China is expected to reach $507.49 billion in 2030. 3 Although no effective drugs have been developed to treat dementia, improving modifiable risk factors could reduce the incidence of dementia by 40%. 4 With or even without interventions, patients with MCI could also be reversed to a normal cognitive state rather than progressing to dementia. 5 Therefore, early identification of modifiable risk factors is essential for the prevention of cognitive impairment.
Abnormal lipid levels, as one of these modifiable risk factors, have been shown to be associated with cognitive impairment in previous studies. 2 Existing studies have tended to focus more on traditional lipid profiles. For instance, positive associations of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) levels with MCI and dementia have been reported,6–9 whereas associations of high-density lipoprotein cholesterol (HDL-C) and triglycerides (TG) with cognitive function are inconsistent.10–12 Although the association between novel lipid parameters and cognitive function has also been discussed, the evidence is insufficient. Remnant cholesterol (RC) represents the cholesterol content in triglyceride-rich lipoproteins, including chylomicron remnants, very-low-density lipoprotein and intermediate-density lipoprotein in the non-fasting state. 13 As an emerging biomarker, RC has shown its predictive value for cardiovascular disease (CVD) risk beyond LDL-C in recent years, 14 and higher RC variability increases the risk of cardiovascular disease.15,16 Nevertheless, the current evidence on the association between RC and cognitive function is limited to cross-sectional studies.17,18 Furthermore, most studies have focused on lipid levels at a single time point, few studies have explored the associations of dynamic changes in lipids on cognitive function, and the association of RC variability on cognitive performance is still unclear.
Therefore, the aim of this study was to explore the association between RC and cognitive function based on the China Health and Retirement Longitudinal Study (CHARLS) and to investigate the relationship between RC variability and cognitive function.
Methods
Study design and population
The CHARLS is a prospective cohort study conducted in China since 2011. The details of study design have been described previously. 19 Briefly, the baseline survey was performed among around 19,000 individuals aged ≥45 years in 28 provinces of China, with a response rate of 80.5%, and was followed up in 2013, 2015, and 2018. Of note, measurement of lipid profiles was only conducted in 2011 and 2015. In accordance with the purpose of the analysis, participants who had normal cognitive function at baseline (2011) and completed both cognitive tests and lipid measurements were enrolled. The detailed exclusion criteria were as follows: missing lipid measurements (TC, HDL-C, LDL-C) at baseline or 2015; missing cognitive function measurements at baseline, 2015 or 2018; diagnosed with memory-related diseases (Alzheimer's disease, brain atrophy, or Parkinson's disease) or taking related medications (Chinese traditional medicine, western modern medicine, or other treatments) at baseline; diagnosed with stroke at baseline; taking lipid-lowering medications at baseline; missing potential covariates (Supplementary Figure 1).
Ethical approval was obtained from the Biomedical Ethics Committee of Peking University, and written informed consent was signed by all respondents.
Measurement of RC and its variability
Fasting venous blood samples were collected by trained staff from the Chinese Center for Disease Control and Prevention, and blood lipid levels (TC, HDL-C, LDL-C) were examined by enzymatic colorimetric test. RC was estimated using the following equation: RC (mg/dL) = TC-HDL-C-LDL-C. The cutoff point for abnormally high RC level was defined as 30 mg/dL. 20
RC level variability between 2 visits (2011 and 2015) was calculated, with different indices of variability: (1) standard deviation (SD); (2) coefficient of variation (CV), SD/mean × 100%; and (3) variability independent of the mean (VIM), 100×SD/meanβ, where β is the regression coefficient based on ln(SD) on ln(mean). 21
Measurement of cognitive function
Cognitive function was assessed utilizing the CHARLS questionnaire and consisted of 2 domains: episodic memory and mental intactness. 19 Episodic memory was divided into immediate recall and delayed recall. Participants were asked to recall a word list in any order immediately and 4 min later, the score was defined as the average of the two components, with a range of 0–10 points. The domain of mental intactness, which was derived from the Telephone Interview for Cognitive Status (TICS), 22 was measured by orientation, calculation, and visuospatial ability. The respondents were asked “Please tell me today's date, the day of the week, and what is the current season?” In addition, participants were asked to complete successive subtractions of 100 minus 7, and to draw 2 overlapping pictures. The score range was 0–11 points. Global cognition score was the sum of the above 2 domains and ranged from 0 to 21.
Covariates
Socio-demographic information, behavioral lifestyle, disease and medical history were collected from the questionnaire interviewed by trained staff. Residence was divided into rural and urban areas. Educational level was classified as illiteracy (no formal education), primary and middle school, high school, and college and above. Smokers were defined as those who smoke more than 100 cigarettes in their lifetime, drinkers were defined as those who drink any alcoholic beverages more than once a month in the past year, and smoking status and drinking status was categorized into never, ever and current. History of chronic disease (hypertension, diabetes, dyslipidemia, cancer, CVD) was ascertained via a combination of self-reported physician diagnosis, medication history, and physical or biochemical examinations. For instance, history of hypertension was defined as physician-diagnosed hypertension, current use of antihypertensive drugs, or systolic/diastolic blood pressure ≥ 140/90 mmHg. Similarly, history of dyslipidemia was defined as physician-diagnosed dyslipidemia, current use of lipid-lowering drugs, or TC ≥ 240 mg/dL or TG>200 mg/dL or LDL-C>160 mg/dL or HDL-C<40 mg/dL. 23 CVD included heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems. Body mass index (BMI) was calculated as weight (kg)/height (m)2. The 10-item Center for Epidemiologic Studies Depression Scale (CESD-10) 24 was used to evaluate the depressive condition (0–3 points/question, score range 0–30 points).
Statistical analysis
Baseline characteristics of the participants were determined according to either cutoff point or tertile groups (T1, T2, T3) of baseline RC levels. Continuous variables were expressed as mean ± SD (normally distributed) or median (interquartile range, IQR) (skewed distributed), Student's t test or ANOVA or rank-sum test was used for comparison of differences. Categorical variables were presented as frequencies (number, %), chi-square test was used for comparison of differences.
In main analyses, linear mixed-effect models (LMM) 25 were used to evaluate the associations of baseline RC and its variability with cognitive function. Fixed effects of the model included RC (baseline level or variability), time since baseline (0, 2, 4, or 7 years), time × RC (or variability), with adjustment for potential covariates mentioned in the following 2 models. Model 1 included age, gender, residence, marital status, and educational level. Model 2 was further adjusted for smoking status, alcohol use, history of chronic disease (hypertension, diabetes, dyslipidemia, cancer), BMI, and depression. Baseline cognitive function scores for specific domains were additionally adjusted when the correlation between RC variability and cognitive function was analyzed. Random effects included random inter-individual intercepts to account for within-individual differences. Given that the correlation between RC (or its variability) and cognitive decline was not observed (represented by time × RC), our results were expressed as coefficient β with 95% confidence intervals (CIs) of RC (or its variability) to account for their associations with baseline cognitive function.
Subgroup analyses was stratified by age (≤60/60–69/≥70 years), gender (men/women), educational level (illiteracy/primary and middle school/high school and above), and baseline RC (<30/≥30 mg/dL). Interaction analyses were performed among subgroups using likelihood ratio test to compare models with and those without interaction terms, 26 and p for interaction was represented. Sensitivity analyses contained 4 parts: (1) not excluding those taking lipid-lowering medications at baseline; (2) excluding participants with baseline cognitive function below 10%; (3) imputing missing values of covariates using multiple imputation method (Markov Chain Monte Carlo, MCMC); and (4) further adjusting for history of CVD in the model.
The analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC). A 2-tailed p < 0.05 was considered statistically significant.
Results
Baseline characteristics
4234 participants were included in our study, the average age was 57.4 ± 8.0 years, and 46.7% were men. The mean RC level was 26.2 ± 23.7 mg/dL. As presented in Table 1, participants in the T3 group were more likely to be women, to have had a history of hypertension, diabetes, dyslipidemia, and to have a higher BMI, TC, TG, and a lower HDL-C, LDL-C than the other tertile groups. The differences in baseline cognitive function scores among T1-T3 groups were nonsignificant. Baseline characteristics of participants according to the cutoff point of RC level were also demonstrated (Supplementary Table 1).
Baseline characteristics of participants by tertiles of RC level.
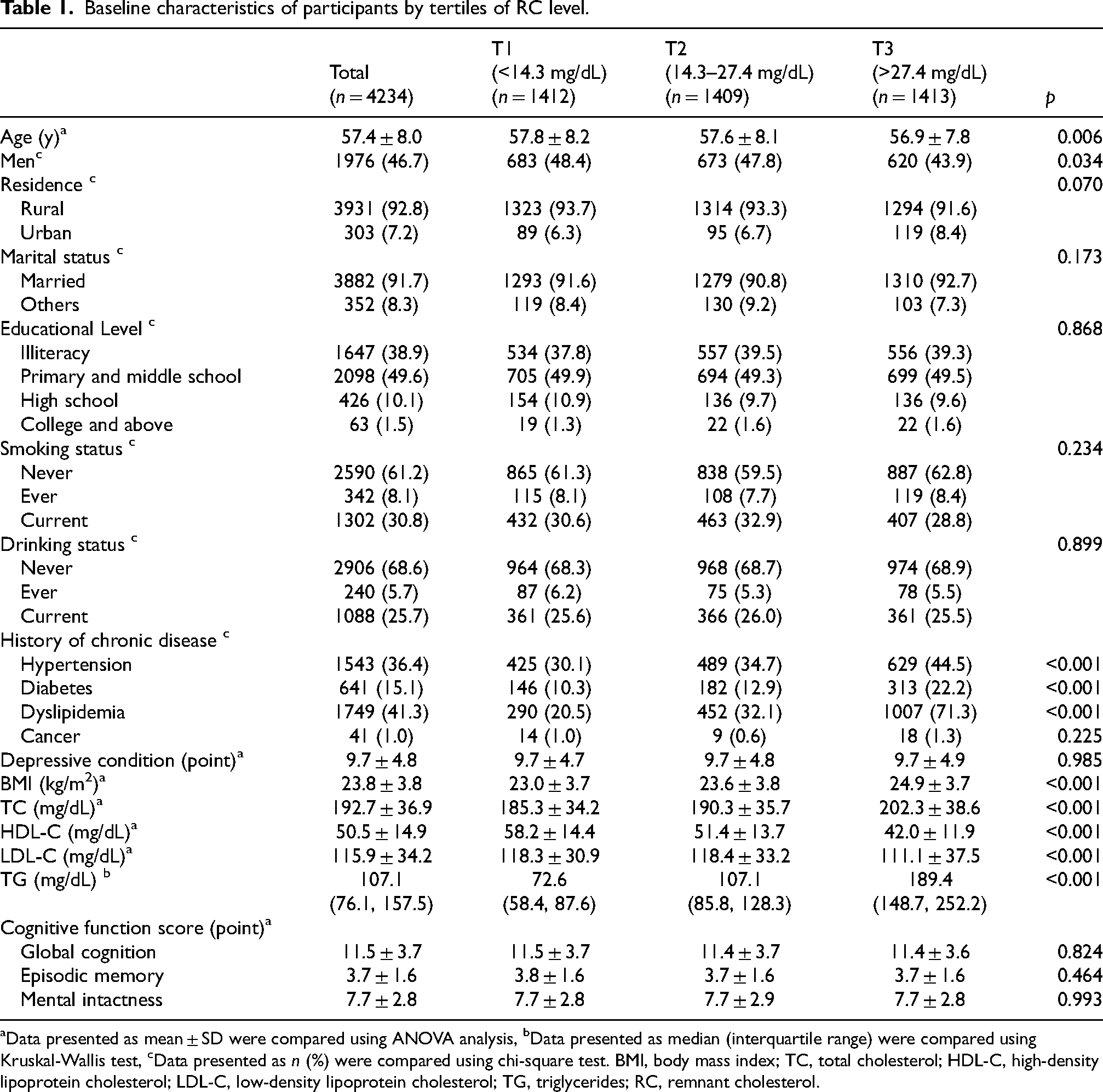
Data presented as mean ± SD were compared using ANOVA analysis, bData presented as median (interquartile range) were compared using Kruskal-Wallis test, cData presented as n (%) were compared using chi-square test. BMI, body mass index; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglycerides; RC, remnant cholesterol.
Baseline RC and cognitive function
The associations of RC level with cognitive function in older adults were shown in Table 2. In the fully adjusted model, RC was negatively associated with each domain of cognitive function, with β (95%CI) of −0.053 (−0.096, −0.009), −0.021 (−0.042, 0.000), and −0.032 (−0.064, −0.001) for global cognition, episodic memory, and mental intactness for each 10 mg/dL increment. Compared with the lowest tertile of RC, participants in the highest tertile group had poorer cognitive performance in global cognition (β = −0.321, 95%CI: −0.568, −0.075) and episodic memory (β = −0.191, 95%CI: −0.310, −0.073), respectively. In the sensitivity analyses, the results were generally consistent with our main findings (Supplementary Table 2).
Associations between baseline RC and cognitive function, β (95%CI).
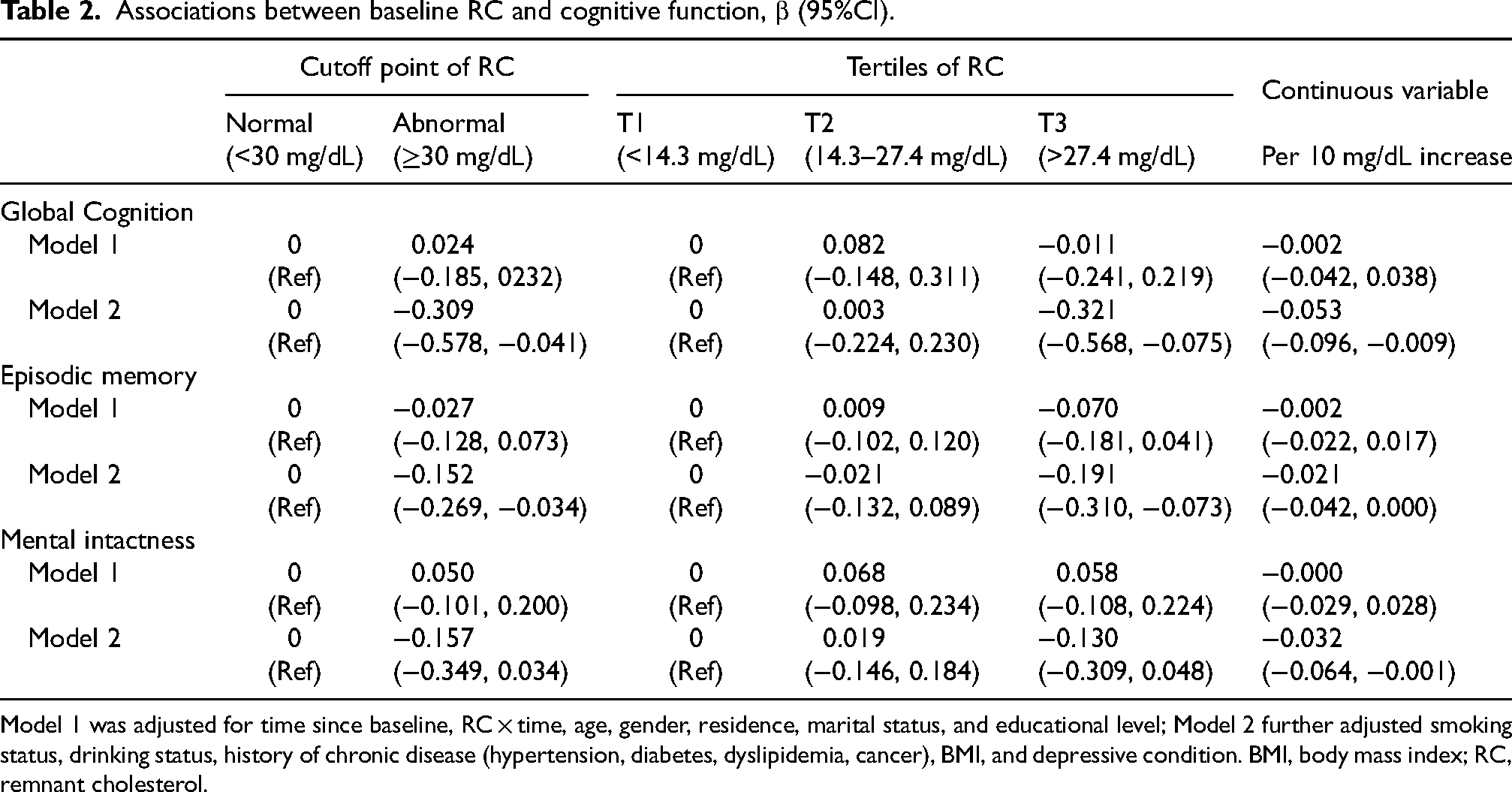
Model 1 was adjusted for time since baseline, RC × time, age, gender, residence, marital status, and educational level; Model 2 further adjusted smoking status, drinking status, history of chronic disease (hypertension, diabetes, dyslipidemia, cancer), BMI, and depressive condition. BMI, body mass index; RC, remnant cholesterol.
Subgroup differences were observed in the relationship between RC and cognitive function by gender, educational level and baseline RC level (Supplementary Figure 2). Elevated RC was significantly associated with lower cognitive level in both global cognition (p for interaction = 0.028) and mental intactness (p for interaction = 0.019), respectively among women. In the subgroup of illiteracy, the negative associations of RC level with the cognitive domains of global cognition and episodic memory were more pronounced (both p for interaction <0.001).
RC variability and cognitive function
We also explored the associations of various variability measurements of RC with cognitive function (Table 3 and Figure 1). After multivariate adjustment, each SD increase in RC variability measured by SD and VIM was associated with lower cognitive level in episodic memory of 0.057 (95%CI: 0.004, 0.111) and 0.054 (95%CI: 0.001, 0.107) scores, respectively. Compared with T1 group, the T3 group showed lower levels in global cognition and episodic memory, but not mental intactness, as RC variability was calculated using SD and VIM. Similar results were also obtained, and the association between higher RC variability and worse global cognition was amplified when not excluding those taking lipid-lowering medications or excluding the participants with the lowest 10% cognitive function scores (Supplementary Table 3 and Supplementary Figure 3).

Associations between RC variability and cognitive function.
Associations between RC variability and cognitive function (per SD increase).
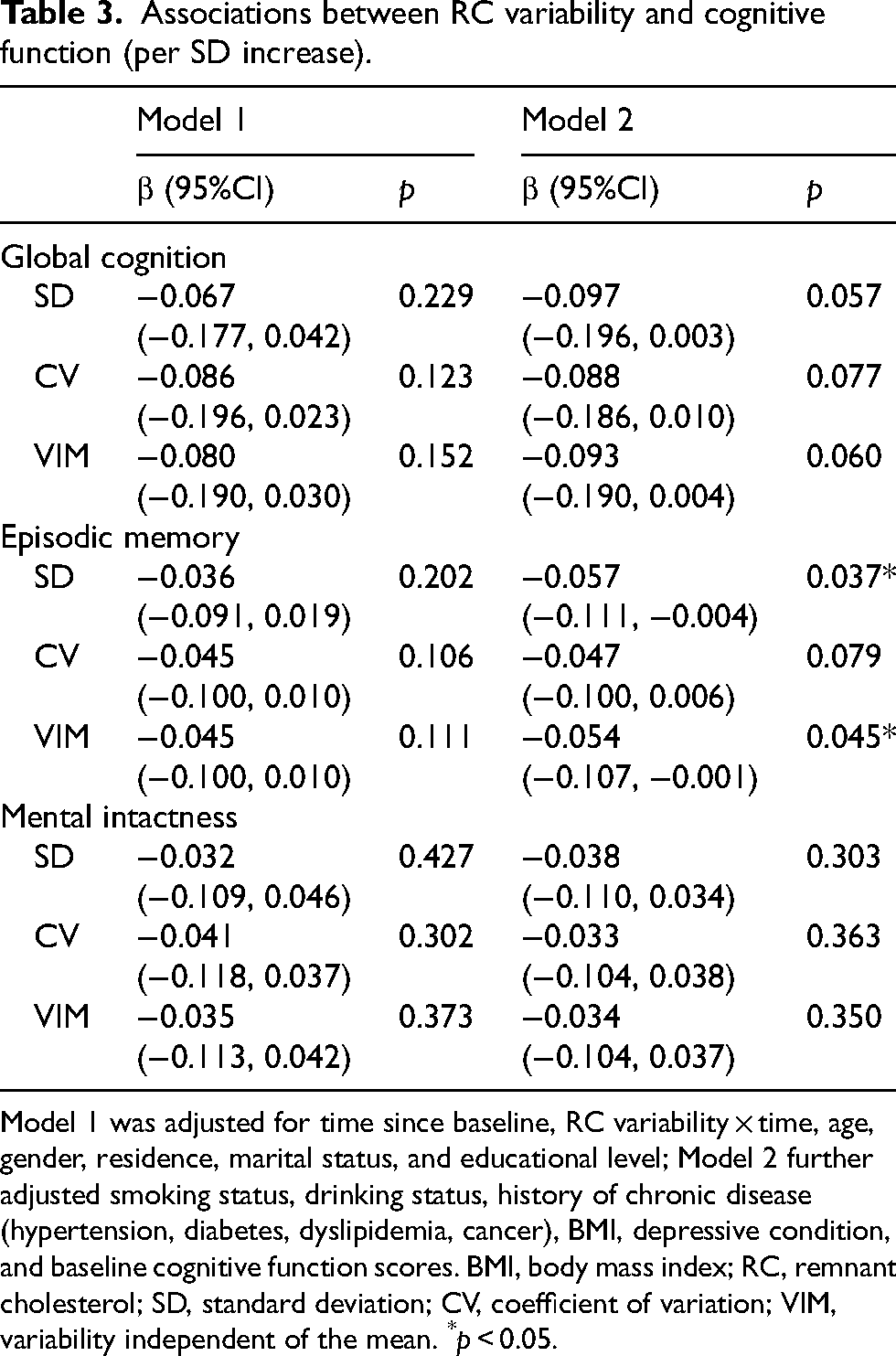
Model 1 was adjusted for time since baseline, RC variability × time, age, gender, residence, marital status, and educational level; Model 2 further adjusted smoking status, drinking status, history of chronic disease (hypertension, diabetes, dyslipidemia, cancer), BMI, depressive condition, and baseline cognitive function scores. BMI, body mass index; RC, remnant cholesterol; SD, standard deviation; CV, coefficient of variation; VIM, variability independent of the mean. *p < 0.05.
As shown in Figure 2, educational level was a potential effect modifier in the association between RC variability and decreased cognitive function of each domain (p for interaction = 0.045 for global cognition; p for interaction = 0.004 for episodic memory; p for interaction = 0.029 for mental intactness). There was also a noticeable trend of differences in the association of RC variability (measured by SD) with episodic memory among age subgroups, with β (95%CI) of −0.063 (−0.126, −0.001) in the participants aged60 years (Figure 2). The subgroup analyses using other measurements as RC variability (CV and VIM) generally generated similar results (Supplementary Figures 4 and 5).

Effect size of RC variability on cognitive function in subgroups (measured by SD).
Discussion
This study indicated that higher RC was associated with lower baseline cognitive level in the middle-aged and older population. Additionally, greater RC variability was also associated with poorer cognitive performance, especially in episodic memory, suggesting that a more stable RC level is optimal. Using data from a large-scale cohort, we first examined the associations of RC variability with cognitive function. Furthermore, various measurements of RC variability were implemented to make our final conclusions more robust. While MCI cannot be diagnosed solely from worsening performance in one or more cognitive domains, 27 identification of risk factors of cognitive impairment may still be important for early screening and management of MCI and even dementia.
Xie et al. found that higher RC levels were associated with worse verbal learning and memory function in the older adults in the US. 17 To the best of our knowledge, our study is the first to examine the association between RC and cognitive function using repeated measurements, and the results were in line with that cross-sectional study. Previous studies have mostly focused on the associations between traditional lipid profiles and cognitive function, although results have been inconsistent. Most of the available studies claimed a positive association of TC and LDL-C with cognitive function in the middle-aged and older individuals7–10,28; however, a negative association,29,30 or no association,31,32 has also been found. Furthermore, current findings on the correlation between HDL-C and TG and cognitive function are inconsistent.9,10,33 A meta-analysis integrating 6 studies observed that high TG levels significantly increased the risk of AD (RR = 1.10, 95% CI: 1.04, 1.15). 34 Although TG levels mirror RC levels, and elevated levels of both are associated with an increased risk for CVD, 35 more prospective studies on the effect of RC level on cognitive function are still needed.
Prior studies have explored the association between visit-to-visit variability of traditional lipid profiles and cognitive function, with most findings suggesting a positive correlation.36–39 A UK study included 4428 subjects and with 4 postbaseline LDL-C measurements indicated that, independently of mean LDL-C levels and statin use, higher LDL-C variability was associated with lower immediate and delayed memory function. 38 Grasset et al. 39 found that HDL-C variability was inversely correlated with processing speed and memory function in the older population. In recent years, studies have underscored the adverse effect of great RC variability on cardiovascular diseases.15,16 Our findings further extend these relationships to cognitive outcomes. Specifically, greater variability in RC was associated with poorer performance in episodic memory. Therefore, along with prior studies, ours provides evidence for the clinical benefits of reducing lipid variability.
Our subgroup analysis revealed that women were more susceptible to the association of high levels of RC with cognitive function, which was roughly consistent with previous research.10,17,29 The potential gender difference might be explained by different hormone levels between sexes. 7 Furthermore, our findings also suggested that the negative associations of both RC level and its variability with cognitive function were stronger in the subgroups with lower educational attainment who also have less access to cognitive training. Consequently, in the management of lipid profiles, additional benefits in maintaining cognitive function may be derived from focusing more on less educated populations. Since high educational level is beneficial to preserve cognition, 40 it is also essential to achieve a higher level of education, or at least minimize the rate of illiteracy.
The role of RC in cognitive function has not been elucidated, but in the light of traditional lipid markers and the impact of RC on cardiovascular disease incidence, the following line of argument may be proposed. Elevated RC is associated with impaired vascular endothelial function, reflected by abnormal release of vasodilators such as endothelial nitric oxide (NO).41,42 Deficiency of NO in the cerebrovascular endothelium leads to increased expression of amyloid-β protein precursor (AβPP) and β-site APP-cleaving enzyme 1 (BACE1), resulting in increased secretion of amyloid-β (Aβ), and subsequent neurodegeneration. 43 Moreover, it has also been suggested that both high levels of lipid markers and their variability might reduce cerebral blood flow and increase white matter hyperintensity load, thereby causing cognitive decline.38,44,45
Several limitations should be addressed. First, only 2 measurements of lipid levels were conducted due to study limitations, which was cruder than that with 3 or more time-points. However, an interval of 4 years between these 2 measurements could also well represent the changes in RC levels in the mid-to-long term. Second, RC was only indirectly calculated using values of TC, HDL-C, and LDL-C. Direct and accurate assessment of RC is technically challenging, since remnant particles are synthesized by both endogenous and exogenous pathways. 13 Third, cognitive function was assessed from CHARLS questionnaires rather than standardized cognitive screening scales, thus, all cognitive domains cannot be fully explored. However, the 2 domains of our study were comparable to commonly used questionnaires due to similar test questions. 22 Furthermore, the available data did not allow us to determine whether the participants developed MCI or AD subsequently, and future studies with definitive diagnostic information are needed. Fourth, the modifying effect of educational level was identified among our older respondents with generally low educational attainment, which might not be generalized to the population with higher educational level. Future prospective studies are needed to confirm its role in the high-income regions with greater accessibility to education. Fifth, residual bias could not be ruled out since we did not adjust some potential confounders due to insufficient data, such as physical activity, dietary intake, air pollution, APOE ε4 alleles and so on.
In conclusion, the present study suggested that both higher levels of RC and their variability were associated with worse global cognition, especially in episodic memory domain. In addition, the association between RC variability and cognitive function was potentially modified by educational level. Our findings provide additional evidence for the beneficial effects of maintaining RC levels at a stable level and appropriate range on cognitive health and may help to suggest prevention strategies for cognitive impairment in older individuals.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241284200 - Supplemental material for Remnant cholesterol and cognitive function: Evidence from the China health and retirement longitudinal study
Supplemental material, sj-docx-1-alz-10.1177_13872877241284200 for Remnant cholesterol and cognitive function: Evidence from the China health and retirement longitudinal study by Hanrui Liu, Lili Luo, Juan Xia, Xiaonan Wang and Yanxia Luo in Journal of Alzheimer's Disease
Footnotes
Authors contributions
Hanrui Liu (Data curation; Formal analysis; Investigation; Methodology; Writing – original draft); Lili Luo (Data curation; Methodology; Supervision; Validation; Visualization; Writing – review & editing); Juan Xia (Project administration; Supervision; Writing – review & editing); Xiaonan Wang (Funding acquisition; Project administration; Software; Supervision; Writing—review & editing); Yanxia Luo (Conceptualization; Project administration; Resources; Supervision; Writing—review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (Grant number 81903408).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.