
Abstract
Alzheimer's disease (AD) is a common neurodegenerative disease characterized by amyloid-β (Aβ) deposition and neurofibrillary tangles formed by high phosphorylation of tau protein. At present, drug therapy is the main strategy of AD treatment, but its effects are limited to delaying or alleviating AD. Recently, non-pharmacologic intervention has attracted more attention, and more studies have confirmed that non-pharmacologic intervention in AD can improve the patient's cognitive function and quality of life. This paper summarizes the current non-pharmacologic intervention in AD, to provide useful supplementary means for AD intervention.
Keywords
Introduction
Alzheimer's disease (AD) is the most prevalent form of dementia, characterized by progressive neurodegeneration marked by neuritic plaques and neurofibrillary tangles.1,2 Currently, there are approximately 50 million individuals worldwide diagnosed with AD, and this number is projected to rise to 152 million by 2050. 3 The primary pharmacological treatments for AD include cholinesterase inhibitors (such as donepezil, rivastigmine, and galantamine) and the N-methyl-D-aspartate (NMDA) receptor antagonist memantine. 4 However, these medications do not halt neuronal impairment or prevent disease progression, 5 highlighting the urgent need for more effective therapies. In recent years, increasing attention has been directed towards complementary and alternative therapies for AD, particularly non-pharmacological interventions.6,7 This review provides an overview of current non-pharmacological treatments for AD, encompassing psychological cognitive interventions, exercise regimens, combined interventions, neurostimulation therapies, artificial intelligence technologies, and other intervention methods. These insights aim to advance non-pharmacological strategies as preventive and therapeutic approaches for AD.
Cognitive intervention
Cognitive decline is the principal clinical manifestation of AD, while the accumulation of amyloid-β (Aβ) peptides in the cerebral cortex is a major neuropathological hallmark. 8 Studies have indicated that synaptic loss is the primary pathological correlate of cognitive decline in AD. Although Aβ, particularly Aβ oligomers, may lead to subsequent synaptic loss, their primary pathophysiological impact involves functional imbalance and inconsistent coordination among specific neural networks. This phenomenon may explain the connection between cerebral amyloid burden and the subtle yet significant cognitive performance variations among cognitively normal elderly individuals. Prolonged dysregulation of Aβ levels results in Aβ deposition. This may couple with abnormal activity within extensive neural networks (manifesting as deactivation defects or task-related hyperactivation across diverse brain regions) and may synergistically reinforce each other and precipitate a self-propagating cycle, thereby exacerbating Aβ burden and neural network dysregulation. 9 This physiological mechanism underpins the rationale for cognitive interventions in AD.
Presently, cognitive interventions are broadly classified into three categories: cognitive training, cognitive stimulation, and cognitive rehabilitation. Cognitive training involves customizing tasks to enhance specific cognitive functions like memory, visual-spatial abilities, attention, and language. 10 Typically conducted at home or with family-based supervision, this intervention stimulates cognitive function through tailored exercises, providing positive reinforcement to bolster confidence and alleviate depressive and anxious emotions. 11 Studies affirm its efficacy in enhancing verbal episodic memory and verbal working memory, as well as improving immediate and delayed memory, including story recall. 12 Conversely, cognitive stimulation employs social activities and group discussions and targets cognitive and social functions. 13 For instance, reminiscence therapy (RT) fosters happiness and improves the quality of life by revisiting past events, while reality orientation (RO) enhances cognitive function by training environmental memory, such as directional awareness, routes, and familial names. 14 Research by Ta'rraga et al. demonstrates improved cognitive function among AD patients following cognitive stimulation therapy. 11 Cognitive rehabilitation aims to enhance daily life abilities through collaborative efforts between medical professionals and family members. It employs personalized strategies, encompassing activities like personal hygiene, dressing, eating, and medication management, with a focus on reinforcing memory, cognition, and intelligence. 15 It has been shown that a 12-week cognitive rehabilitation program can enhance the quality of life for mild AD patients; however, it does not significantly elevate cognitive levels. 16 Notably, interventions combining cognitive training and rehabilitation yield overall cognitive improvement in experimental groups over the long term compared to control groups. 17 In populations at high risk for AD or in those with mild cognitive impairment (MCI), changes in brain activity precede Aβ pathological deposition and cognitive decline. 18 Functional magnetic resonance imaging (fMRI) monitoring post-cognitive interventions reveals heightened brain activity, suggesting that cognitive intervention can modulate cognition by altering brain function. 19 Presently, the majority of neuroimaging studies in cognitive intervention are centered around memory training.
Research has demonstrated that cognitive stimulation can significantly enhance both general and specific cognitive functions in patients with AD. However, most existing psychological interventions rely on traditional cognitive exercises to improve cognitive function, often resulting in low patient compliance. With the increasing prevalence of computer technology, integrating innovations in computer science into psychological cognitive interventions can boost the engagement and appeal of cognitive training, potentially leading to improved patient adherence.
Exercise intervention
There is a growing body of evidence supporting the notion that physical exercise holds the potential to avert cognitive decline and dementia. 20 Diverse modalities of exercise intervention, including aerobic exercise, stretching, resistance training, and combined exercises, exhibit promise in staving off cognitive deterioration among elderly individuals afflicted with AD. 21 Research indicates that aerobic exercise, in particular, can bolster neuroplasticity, mitigate hippocampal atrophy, and even augment hippocampal volume. 22 Appropriate exercise regimens are increasingly recognized as instrumental in both preventing and mitigating abnormal Aβ and tau phosphorylation processes within the body. This is accomplished through mechanisms such as the facilitation of neural signal transmission, modulation of neurochemical functions, suppression of Aβ production, and aberrant phosphorylation of tau proteins.23,24 Moreover, exercise has been shown to stimulate the secretion of neurotrophic proteins, enhance cerebral energy metabolism, and ameliorate cerebral blood flow, thereby fostering neurogenesis and synaptic plasticity. 25 It also upregulates the expression of muscle factor interleukin-6 (IL-6), mitigates the deleterious effects of pro-inflammatory factors on brain tissues, promotes the secretion of anti-inflammatory factors, and impedes the onset of inflammatory responses.26–28 Furthermore, exercise-mediated modulation of neuroglial cell states exerts a discernible influence on the onset and progression of AD pathology, manifesting anti-inflammatory properties and diminishing the risk of neuroinflammation-related ailments, consequently thwarting the emergence and advancement of AD. 29
Animal studies suggest that high-intensity running significantly enhances cognitive function in Tg2576 mice compared to low-intensity running. 30 Similarly, medium-intensity running training shows a greater reduction in Aβ formation in 2×Tg-AD mice relative to low-intensity training, indicating that moderate to high-intensity exercise can positively impact cognitive function. 31 This improvement is primarily achieved through increased lipid metabolism, antioxidant enzyme activities, and the stimulation of neurotrophic factors like brain-derived neurotrophic factor (BDNF), insulin-like growth factor 1 (IGF-1), and vascular endothelial growth factor (VEGF). 32 Conversely, low to moderate-intensity exercise focuses more on reducing highly phosphorylated tau protein levels and extracellular Aβ plaques, thus reducing neuroinflammation and easing the progression of AD. 33 Liang et al. reviewed exercise interventions in AD patients and found that exercise can improve cognitive function, neuropsychiatric symptoms, and quality of life. 34 The duration of exercise is crucial; subgroup analysis shows that interventions lasting 2–5 months yield significant benefits. Short-term (2–5 months) physical activity interventions appear to be more effective at enhancing cognitive function, neuropsychiatric symptoms, and quality of life for AD patients. Notably, no significant differences were observed between different types of physical activities. 34 Studies have demonstrated that combining aerobic interval exercise with running and swimming was employed to examine its effects on behavioral dysfunction and mature neuron regeneration in an AD mouse model. The findings indicate that four weeks of exercise can improve cognitive impairment in these mice, while also reducing anxiety and depression-like behaviors. The combination of metabolites and proteins generated by aerobic interval exercise plays a role in promoting mature neuron regeneration and improving behavioral outcomes following AD pathology. 7 A meta-analysis reinforces the idea that regular exercise has systemic benefits, influencing the nervous, cardiovascular, skeletal, immune, digestive, and reproductive systems. Regular exercise can reduce plasma Aβ concentration and guard against Aβ's neurotoxicity, thus potentially preventing organ degeneration. This underscores the preventive role that regular exercise could play in AD. The meta-analysis also supports the notion that regular exercise may slow AD progression. 35
Although appropriate exercise is beneficial for enhancing brain functions, high-intensity exercise-induced cognitive dysfunction is causing more and more concerns nowadays. Sun et al. found that high-intensity exercise impairs cognitive behavior and hippocampal synaptic plasticity in rats via inflammatory responses and may be related to the upregulation of the JNK/p38/ERK pathway. 36 In a multicenter randomized controlled trial, the effects of moderate to high-intensity exercise training on cognitive impairment in AD patients were investigated. The results showed that the training did not slow cognitive impairment. 37 Therefore, it is essential to focus on the benefits of appropriate exercise.
Dual-task cognitive-motor combined training
Dual-task training, training that involves undergoing cognitive interventions and physical exercises simultaneously or in sequence, may yield superior effects on cognition and movement compared to utilizing either of them alone. Also, dual-task training may elicit synergistic effects between physical exercise and cognitive training. 38 A study revealed that combined intervention (Dual-task training) significantly enhanced memory compared to groups receiving only cognitive or exercise interventions;39,40 however, this combined approach did not yield significant improvements in overall cognition or executive function. In contrast, other recent findings demonstrated positive effects on overall cognition or executive function. 40 Research suggests that physical exercise fosters neurogenesis, while cognitive interventions bolster the survival of newly formed neurons and facilitate their integration into functional brain networks via activity-dependent synaptic adaptation, thereby sustaining positive plastic changes.41–44 It is noted that some studies offer contradictory results, possibly attributable to the challenges of combining interventions, which include the possibility of inducing excessive stress and attenuates the cognitive benefits of individual cognitive and physical interventions.45,46 Interactions between combined components in interventions may hinder rather than facilitate neuroplasticity, obscuring cognitive enhancements. Furthermore, although combined intervention outperforms single physical exercise in memory enhancement, this superiority is not evident when compared to single cognitive intervention. 46 This discrepancy may stem from the superior efficacy of cognitive intervention in improving memory among MCI patients compared to physical exercise alone. Physical exercise is limited when it comes to enhancing memory and fails to counteract the negative effects of combining both physical exercise and cognitive intervention, thereby resulting in inferior memory enhancement compared to the use of cognitive intervention alone. Conversely, the prominent efficacy of cognitive intervention in enhancing memory counteracts the negative effects of combining both components, yielding superior memory enhancement compared to the use of physical exercise alone. Since MCI represents a critical stage characterized by ongoing cognitive restructuring and neuroplasticity, 47 cognitive intervention should be prioritized to sustain existing neuron survival and enhance plasticity, while the impact of physical exercise on neurogenesis remains insignificant.
Neurostimulation therapy
Transcranial electromagnetic stimulation therapy
Brain electrical stimulation therapy encompasses various modalities such as deep brain stimulation (DBS), transcranial magnetic stimulation (TMS), transcranial current stimulation (TCS), transcranial photothermal stimulation (TPS), and vagus nerve stimulation (VNS). 48 While cognitive and exercise training are prevalent non-pharmacologic interventions for AD, brain electrical stimulation therapy, notably repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS), also demonstrate promising clinical prospects in AD treatment. 49
Deep brain stimulation (DBS)
DBS is an invasive technique that entails implanting electrodes into specific regions of the brain to administer electrical stimulation, which is controlled by an implanted pulse generator. In the context of treating AD, common brain targets for DBS include the fornix, 50 the entorhinal cortex, 51 the vertical limb of the diagonal band, 52 and the ventral capsule/ventral striatum (VC/VS) region, 53 among others.
Chronic DBS of the hippocampus in mammalian models with neurodevelopmental disorders shows an increase in neuronal count, encouraged neurogenesis, reduced neuropathological burden, and improved spatial learning, memory, and object recognition. 54 In clinical studies, six AD patients who received chronic bilateral hippocampal DBS showed enhanced neural activity in memory circuits, suggesting a potential therapy for AD-related memory deficits. 55 However, a double-blind randomized controlled trial (RCT) assessing DBS in mild AD patients did not yield significant differences in cognition or metabolism between the treatment and control groups overall. Subgroup analysis demonstrated slight cognitive improvement among patients aged 65 or older, juxtaposed with cognitive decline in younger patients after 12 months of DBS treatment. 56 While chronic stimulation studies on the human entorhinal cortex are lacking, long-term DBS in rodent AD models targeting the bilateral entorhinal cortex has shown promising outcomes. This intervention has been associated with increased neurogenesis and a reduction in Aβ plaque load, indicative of potential therapeutic benefits. 57 Furthermore, studies investigating olfactory cortex DBS (EC-DBS) have demonstrated its ability to rectify synaptic defects between layers II of the entorhinal cortex and CA1 of the hippocampus in AD mice. 58 This correction has led to hippocampal neurogenesis and improved cognitive function. Notably, EC-DBS has shown efficacy in reducing Aβ plaque burden in various brain regions of early-stage AD mice, suggesting its potential as a treatment strategy in the early stages of the disease. 51 Additionally, vertical diagonal band DBS (VDB-DBS) therapy has exhibited the ability to restore reduced cholinergic neuron synaptic density in the dentate gyrus (DG) of the hippocampus. 52 Targeting the VC/VS region aims to modulate frontal networks and influence executive function in AD patients. It is also noted that neurons in the VC/VS region undergo neurodegeneration following temporal areas of the AD process, potentially rendering them more suitable targets for DBS modulation. 53
Although DBS is generally considered safe and well-tolerated, there are unforeseeable risks associated with the invasive nature of the procedure and the potential for neurological or psychological side effects, such as the occurrence of depression in AD patients undergoing bilateral DBS treatment of the thalamic nuclei for epilepsy. 59 Therefore, caution should be exercised in the use of DBS.
Transcranial magnetic stimulation (TMS)
TMS is an established non-invasive method for brain stimulation. Utilizing coils encased in plastic, the TMS apparatus is placed over the patient's scalp and generates electrical currents, creating a magnetic field within cranial tissues to administer targeted brain stimulation. 60 rTMS involves administering a series of pulses with specific frequencies and consistent intensities. Particularly in the motor cortex, rTMS can modulate cortical excitability, inducing enduring neuroplastic changes. 61 Research suggests that rTMS therapy can mitigate the production of Aβ peptides, enhance neuronal plasticity, and reduce neuronal apoptosis, thereby potentially ameliorating cognitive function in AD patients. 62 Low-intensity rTMS (110% average resting motor threshold intensity, 1 Hz, LIMS) have been reported to trigger the activation of BDNF and tyrosine kinase receptor B (TrkB), upregulate synaptic protein marker levels, increase synaptic density and PSD thickening, and further reverse the spatial cognitive dysfunction in aging mice. 63 It has also been reported that rTMS stimulated at a high frequency of 25 Hz improves the cognitive function of AD model mice through the PI3K/Akt/GLT-1 signaling pathway, reduces hippocampal Aβ1–42 level, improves oxidative stress, and improves glucose metabolism. 64
Research indicates that neuropathological abnormalities in AD predominantly localize to the posterior cortical regions of the brain. Specifically, amyloid plaques and neurofibrillary tangles initially appear within the precuneus, posterior cingulate cortex, splenium, and lateral posterior parietal cortices. Consistent findings from FDG-PET imaging studies reveal early regional metabolic reductions in these posterior regions among AD patients. This correlates with alterations in default mode network (DMN) connectivity, which is detectable through fMRI. 62 The precuneus, considered a key hub of the DMN, is prominently affected by tau pathology deposition and neuroinflammation, resulting in diminished functional connectivity or hypoactivation. Reports also indicate interpretative impacts attributed to localized atrophy in the precuneus among patients with mild cognitive impairment. It is noted that disconnection of the precuneus precedes and contributes to localized brain atrophy during the early clinical stages of AD. Precuneal atrophy reflects the consequences of brain disconnection, leading to the transition from mild cognitive impairment to AD. 62 Additionally, AD patients often exhibit reduced cortical thickness, along with abnormal activation and decreased functional connectivity during memory tasks. Given the critical role of precuneal activity in episodic memory retrieval, its impairment signifies typical clinical manifestations of AD. 62 rTMS exhibits varied therapeutic effects across different brain regions. Following rTMS treatment of 94 patients with mild to moderate AD, stimulation of the left dorsolateral prefrontal cortex (DLPFC) was found to yield more pronounced cognitive improvements compared to the right or bilateral stimulation. 65 Another randomized controlled clinical trial indicated that high-frequency rTMS targeting multiple brain regions simultaneously enhances cognitive function in AD patients more effectively than stimulation of a single region. 66
A 24-week trial, comprising a two-week treatment and a 22-week maintenance phase, was conducted on 50 Alzheimer's patients. 67 They were randomly assigned to either active rTMS or sham stimulation. During treatment, the active group received intensive rTMS sessions five times a week for two weeks, while the sham group received simulated treatment. In the maintenance phase, the active group had weekly sessions for 22 weeks. The primary outcome measured was the change in the Clinical Dementia Rating Scale total score, with secondary outcomes including scores on various cognitive assessments. Neurophysiological changes in prefrontal cortex excitability and oscillatory activity were assessed using single-pulse TMS and EEG. Results showed stable scores in the active rTMS group compared to deteriorating scores in the control. The active group also performed better on secondary outcomes. Neurophysiological findings revealed sustained prefrontal cortex excitability and enhanced gamma oscillations in the active group. Another trial combining 20 Hz rTMS with cognitive training showed superior associative memory improvement compared to cognitive training alone. 68 High-frequency rTMS, particularly targeting the bilateral DLPFC, showed promise in AD treatment compared to low-frequency rTMS. These findings highlight rTMS as a potential intervention, especially when combined with cognitive training, emphasizing the importance of frequency optimization.
Intermittent theta burst stimulation (iTBS), a novel time-saving and cost-effective repetitive transcranial magnetic stimulation regime, has been shown to improve cognition in patients with AD. 69 The latest study found that iTBS can reduce oxidative stress, increase antioxidant capacity and decrease reactive astrocyte proliferation in AD model mice. 70 Furthermore, iTBS can upregulate the expression of iron-sulfur cluster assembly 1 (ISCA1, an essential regulatory factor for mitochondrial respiration) in the brain of APP/PS1 mice, regulates mitochondrial respiration and function, and thus alleviates the cognitive impairment and pathology of AD. 71 A randomized clinical trial investigating personalized hippocampal network-targeted rTMS in early AD demonstrated significant improvements in cognitive and functional performance, as well as enhanced hippocampal-cortical connectivity, supporting rTMS as a promising intervention for AD treatment. 72
Transcranial current stimulation (TCS)
Transcranial electric stimulation (tES) involves delivering weak electrical currents (1–2 mA) between two or more electrodes on the subject's scalp. There are two main forms of tES: tDCS and transcranial alternating current stimulation (tACS). tDCS is the most common choice for tES in the treatment of AD. tDCS delivers a current of 1 to 2 mA through electrodes placed on the scalp. Anodal tDCS typically increases excitability in the targeted area and surrounding cortical regions, while cathodal tDCS decreases excitability. tDCS modulates neuronal activity, altering the polarization state of membranes. tDCS is safe, well-tolerated, and cost-effective, leading to its increasing application over recent decades. The DLPFC has been a target of research due to its crucial role in executive functions. tDCS applied to the DLPFC may engage compensatory mechanisms for working memory performance, this can alter neuroplasticity due to prefrontal cortex damage. Some studies have found positive effects of tDCS on memory in AD patients. A double-blind randomized controlled trial found higher cognitive scores in AD patients after repeated treatments compared to a control group, with similar effects for both anodal and cathodal tDCS. 73 tDCS can enhance cognitive reserve effects in mild to moderate AD patients, possibly connected to its effects on neurotransmitters such as acetylcholine and dopamine. tDCS interventions targeting the left temporal cortex (TC) and frontal cortex (FC) also show a trend toward improving memory and executive function decline. Studies have suggested that tDCS treatment of the TC region improved word recognition memory in suspected AD patients. Additionally, tDCS treatment targeting the temporal regions demonstrates potential effects on visual recognition memory. 74
tACS delivers a current oscillating above and below zero with a specified stimulation intensity (i.e., peak-to-peak amplitude) and specific frequency. 75 In contrast to tDCS, where the excitability threshold of neuronal membranes is modulated, 76 tACS directly interacts with ongoing neural activity during cognitive or sensorimotor processes, resulting in the synchronization of brain network oscillations or rhythmic coordination.75,77 In animal studies, tACS stimulation of AD model rats demonstrated improved memory impairment and decreased recognition ability induced by Aβ in the brain, suggesting that tACS can counteract Aβ-induced memory deficits. 78 tACS therapy that targeted the stimulation of bilateral temporal lobes in mild to moderate AD patients for 1 h/day over 4 weeks resulted in significantly reduced phosphorylated tau protein and microglial activation post-treatment. However, there was no significant change in brain Aβ burden, indicating that tACS therapy may only improve certain aspects of AD pathology. 79 Another study that applied tACS therapy to the medial temporal cortex and prefrontal region demonstrated increased scores on the Rey Auditory Verbal Learning Test (RAVLT) total recall, long-delayed recall, and face-name association scores in the treatment group, along with enhanced network connectivity of cholinergic neurotransmission within the cortex, suggesting significant improvement in memory capabilities in AD patients with tACS. 80
In summary, tDCS mitigates neuropathological manifestations of neurodegenerative disorders like AD by modulating neuronal activity and excitability within the cerebral cortex. Conversely, tACS does not directly modulate neuronal excitability but instead integrates substantial neuronal clusters into localized oscillatory networks via entrainment and resonance mechanisms. This process consequently modulates internal computations within specific brain regions and orchestrates broader network activity, thus playing a regulatory role in cognitive functions.
Transcranial pulse stimulation (TPS)
Transcranial pulse stimulation (TPS) is an innovative noninvasive method for precise neuromodulation using brief, high-intensity ultrasound pulses (∼3 μs), repeated every 200–300 ms. 81 This technique offers superior spatial resolution, allowing it to effectively target deep neural structures within the human cortex. 82 TPS utilizes focused ultrasound frequencies that can penetrate up to 8 cm deep, reaching critical brain regions like the thalamus, positioned between 5 and 6.5 cm beneath the scalp. 83 Computational models indicate that TPS can modify the electrical activity of both cortical and subcortical areas. Unlike transcranial-focused ultrasound stimulation, TPS circumvents issues such as tissue heating and standing wave effects by employing brief pulses without continuous or prolonged ultrasonic sequences.84,85 It has been reported that stimulating areas related to depression (including extended dorsolateral prefrontal cortex) appear to alleviate depressive symptoms and induce functional connectivity (FC) changes in AD patients. 86 TPS is promising in improving cognitive performance and reducing depressive symptoms in patients with AD. Therefore, TPS may be a safe adjunct therapy in the treatment of AD. 87
Vagus nerve stimulation (VNS)
VNS encompasses both invasive and non-invasive modalities. In invasive VNS (iVNS), electrodes are surgically positioned along the left vagus nerve. These electrodes are intricately connected to the left vagus nerve within the brain and are linked to a pulse generator implanted in the left thoracic region. This setup facilitates the delivery of programmable electrical stimulation to the vagus nerve, thereby regulating brain network activity. Studies have demonstrated that iVNS exerts its effects by enhancing synaptic transmission, neural plasticity, and long-term potentiation (LTP) through modulation of the locus coeruleus (LC) and β-adrenergic receptors within the CA3 region of the hippocampal perforant pathway, ultimately leading to cognitive enhancement. 88 A pioneering pilot study conducted in 2002 on AD patients showcased promising results. Following 3 months of treatment, approximately 90% of patients exhibited improvements in Mini-Mental State Examination (MMSE) scores, with 70% demonstrating enhanced performance on the Alzheimer's Disease Assessment Scale-Cognitive Subscale (ADAS-Cog). Remarkably, even after 6 months of treatment, the response rate among AD patients remained consistently high at 70%. 89 After these encouraging findings, the research team expanded their cohort and conducted a comprehensive 12-month follow-up study. Notably, after a year of iVNS intervention, approximately 70% of patients exhibited either stable or improved cognitive abilities. 90
Non-invasive vagus nerve stimulation (nVNS) represents a non-invasive therapeutic approach, utilizing a portable device to administer electrical stimulation to the ear or neck, thereby indirectly activating the auricular branch of the vagus nerve. Research indicates that in cognitively healthy older adults, a single session of nVNS therapy yields improvements in associative memory compared to control groups. 91 While nVNS shows promise for AD treatment, comprehensive clinical evidence remains insufficient. 92 Currently, a double-blind, placebo-controlled crossover study is underway to assess the therapeutic efficacy of nVNS in patients with MCI. 93
Sensory stimulation therapy
Sensory stimulation encompasses a range of techniques and methods designed to activate the senses, aiming to enhance neural activation and mitigate negative emotions. This concept can be divided into two main categories: single-sensory stimulation and multisensory stimulation. Single-sensory stimulation involves targeted approaches such as auditory stimulation therapy, olfactory stimulation therapy, tactile stimulation therapy, and phototherapy. Multisensory stimulation, on the other hand, seeks to boost memory function and emotional well-being by engaging multiple sensory systems simultaneously. Common examples of multisensory stimulation include Snoezelen multi-sensory rooms, therapeutic garden designs, and virtual reality (VR) applications. Table 1 summarizes the results of previous studies on the effects of sensory stimulation therapy on patients with AD.
Sensory stimulation therapy and its impact on AD patients.
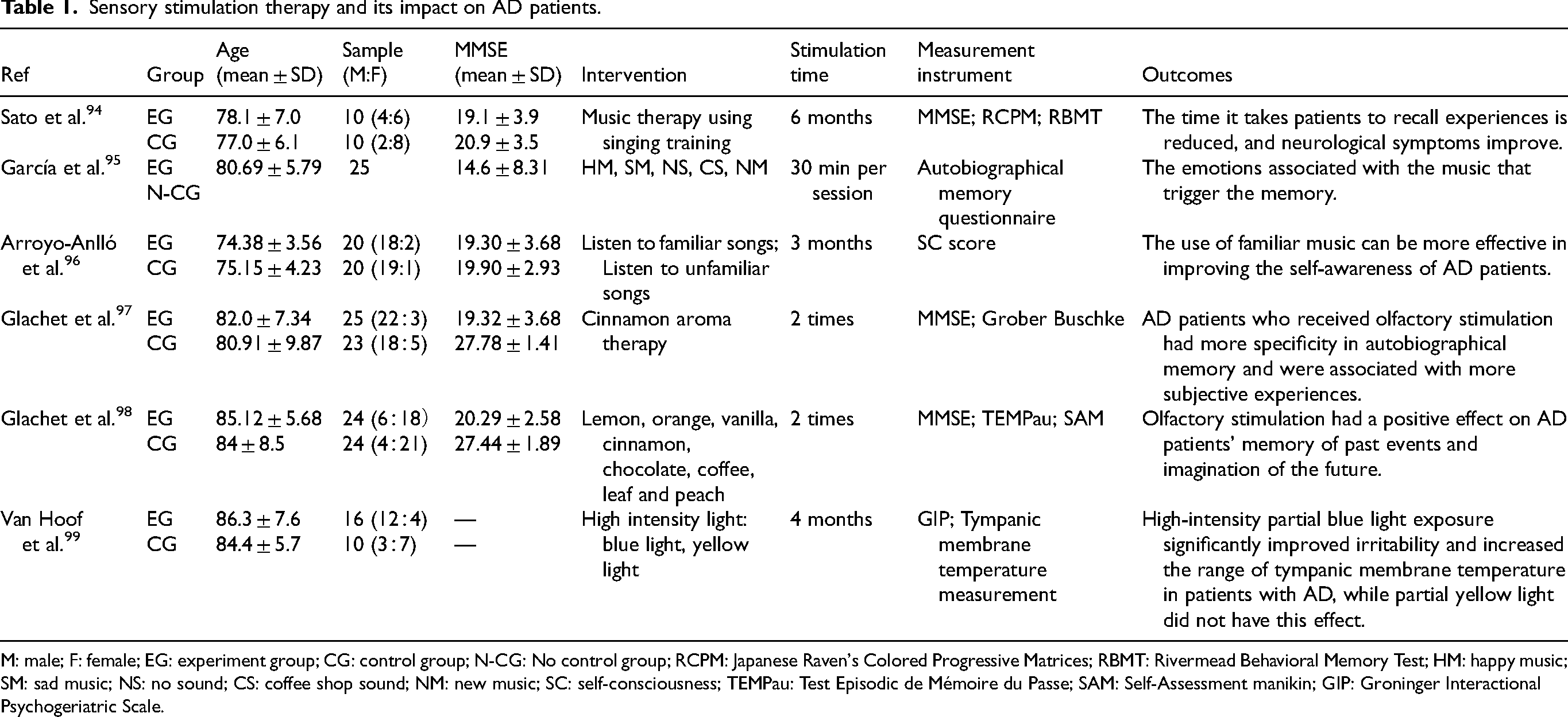
M: male; F: female; EG: experiment group; CG: control group; N-CG: No control group; RCPM: Japanese Raven's Colored Progressive Matrices; RBMT: Rivermead Behavioral Memory Test; HM: happy music; SM: sad music; NS: no sound; CS: coffee shop sound; NM: new music; SC: self-consciousness; TEMPau: Test Episodic de Mémoire du Passe; SAM: Self-Assessment manikin; GIP: Groninger Interactional Psychogeriatric Scale.
Sound and light therapy
Gamma (γ) waves, the fastest brainwaves within the human cortex, are orchestrated by the synchronized firing of a multitude of neurons, yielding a resonance frequency spanning from 25 to 100 Hz. Of these frequencies, there is an emphasis on the 40 Hz frequency due to its extensively investigated impact on cerebral function. Empirical findings show a prevalence of gamma rhythms within the hippocampus, hinting at its pivotal role in mediating the representation of human objects, facilitating visual feature integration, and orchestrating higher-order cognitive processes. This reveals the pivotal role of gamma-band synchronization in orchestrating a myriad of cognitive operations. 100 One randomized controlled trial allocated individuals with mild to moderate AD into either an active treatment cohort (n = 14) or a sham surgical intervention group (n = 8). The active treatment arm received 40 Hz visual and auditory stimulation for one hour daily over six months, while the sham surgical cohort was exposed to high-frequency stimulation exceeding 90 Hz. Notably, the outcomes demonstrated that 40 Hz stimulation therapy reinstated cortical gamma oscillations, thereby culminating in significant enhancements in sleep architecture and functional independence among individuals afflicted with mild to moderate AD. 101
Using invasive optogenetic methods, researchers implanted optical fibers into the visual cortex of 5×FAD/PV-Cre mice, subjecting them to light stimuli of varying frequencies for one hour daily over seven days. Results revealed that 40 Hz light stimulation prompted the microglial transition to a phagocytic state, reducing Aβ1–40 and Aβ1–42 levels by 53.22% and 44.62%, respectively, in the visual cortex. Conversely, 8 Hz or random frequency stimulations showed no reduction in Aβ levels, indicating frequency-dependent therapeutic effects. 102 Morphological changes induced by 40 Hz stimulation, such as shortened microglial processes and enlarged soma diameter, were observed, enhancing phagocytic activity as evidenced by doubled Aβ co-localization. 103 Non-invasive 40 Hz light flicker stimulation in AD mice for one hour daily over seven days induced gamma oscillations, decreased amyloid plaques and phosphorylated tau, boosted neuroprotective factor release, and mitigated neuronal damage and microglia-induced inflammation. Similarly, 40 Hz auditory stimulation was administered to P301S (Tau model) mice aged 8 months and CK-p25 mice aged 6 to 9 months, for 22 and 42 days respectively, results demonstrated improved synaptic function, reduced DNA damage in neurons, and alleviated inflammatory responses, suggesting its efficacy in neurodegenerative disease alleviation. 104 Furthermore, 40 Hz flicker light stimulation enhanced mitochondrial ATP-sensitive potassium channel structure and function, mitochondrial respiratory chain enzyme activities (Complex I and IV), mitochondrial membrane potential (ΔΨm), and reduced mitochondrial reactive oxygen species (ROS) production, thus affecting mitochondrial potassium channels and respiratory chain. 105 Additionally, 40 Hz auditory stimulation induced a 40 Hz auditory steady-state response and gamma oscillations, aiding cognitive functions and language learning memory capabilities. 106 In 5×FAD mice experiments, seven days of 40 Hz auditory stimulation for one hour daily significantly reduced both soluble and insoluble Aβ1–42 in the auditory cortex and hippocampus, increased microglia number and dendritic branching, and improved recognition and spatial memory capabilities. 107 Similarly, 40 Hz auditory stimulation increased reactive astrocytes in the auditory cortex and hippocampal CA1 region of APP/PS1 mice, enhanced blood vessel diameter, and reduced amyloid protein load. 108 Furthermore, 40 Hz auditory stimulation reduced highly phosphorylated tau tangles in tau pathology, 5×FAD, and APP/PS1 mouse models, indicating its broad efficacy in improving tau protein deposition.109,110 In clinical trials, ten consecutive days of 40 Hz light flicker stimulation twice daily in mild to moderate AD patients did not reduce cortical amyloid protein load significantly, suggesting the limited efficacy of short-term visual stimulation. 111 However, 40 Hz auditory stimulation interventions showed significant improvement in mental symptoms for mild to moderate AD patients, with cognitive abilities increasing with prolonged treatment duration, as assessed by the Saint Louis University Mental Status (SLUMS) test, emotional evaluation scale, and behavioral observation. 112
Research has shown that combining 40 Hz visual and auditory stimuli therapy yields better results than using either stimulus alone. This combined therapy enhances microglial cell responses, clears amyloid plaques, and leads to significant cognitive improvement. 108 In mouse models, this therapy increased microglial cell count, reduced plaque numbers and volume, lessened brain atrophy, and boosted cognitive function. 107 Cognito Therapeutics has developed a portable device for this therapy, where AD patients receive 40 Hz audiovisual stimulation for an hour daily for six months. Compared to a control group, treated patients showed reduced brain white matter atrophy, which has the potential to slow AD progression because white matter connects different brain regions. Analysis of AD patient data from the Cognito device treatment and the Alzheimer's Disease Neuroimaging Institute (ADNI) database revealed that treated patients experienced increased white matter volume, while those in the ADNI database had decreased volume during the same period. This suggests that the therapy may effectively reduce white matter atrophy. 113 Dr Mihaly Hajos from Cognito Therapeutics highlighted the device's safety, tolerability, and effectiveness in maintaining cognitive function, reducing brain atrophy, and improving sleep quality. The therapy's benefits extend beyond sensory areas, significantly reducing plaques in the medial prefrontal cortex. 113 Studies also found that continuous 40 Hz audiovisual stimulation for three months in mild AD patients improved brain network connectivity, sleep quality, memory, and slowed brain atrophy. 108 Another trial showed decreased levels of certain proteins associated with AD and improved brain network connectivity after two months of therapy. 114
In summary, the ameliorating effects of AD pathological symptoms induced by 40 Hz gamma oscillations primarily stem from heightened microglial phagocytic activity, augmented vasodilation, and enhanced trans-endothelial cell phagocytosis. These mechanisms facilitate the clearance of pathological proteins, thereby decelerating AD progression and alleviating memory deficits. Additionally, the therapeutic efficacy of 40 Hz audio-visual stimulation surpasses that of singular visual or auditory interventions. Evidence from studies conducted on both AD mouse models and human patients suggests that undergoing 40 Hz audiovisual stimulation therapy yields decreases in neurodegeneration and brain atrophy, alongside increases in synaptic density and normalization of circadian rhythms. These beneficial effects culminate in improved cognitive function, underscoring the potential of 40 Hz audiovisual stimulation intervention as a promising avenue for AD therapy.
Music therapy (MT) represents a cost-effective and efficacious intervention for enhancing neurological, cognitive, and social functioning in patients. Through the stimulation of various brain regions, MT facilitates neuroplasticity, thereby promoting improvements across the aforementioned domains. Notably, research indicates that AD patients experience activation in supplementary motor areas and heightened connectivity among disparate brain regions following exposure to preferred musical stimuli.115,116 Furthermore, music's ability to synchronize neural oscillations associated with learning and memory suggests its potential to foster enduring musical memories.116,117 Moreover, musical stimulation elicits the release of diverse neurotransmitters, including excitatory agents and hormones such as cortisol, testosterone, and estrogen. 117 These biochemical responses influence the expression of receptor genes and associated proteins, potentially ameliorating the condition of AD patients. 118 For instance, estrogen plays a role in reducing Aβ deposition, demonstrating a neuroprotective effect. Additionally, music induces the release of dopamine, a neurotransmitter linked to emotional responses, which can contribute to the therapeutic impact of MT.116,117 Empirical evidence, such as the study conducted by Satoh et al., underscores the efficacy of six months of MT in enhancing memory recall and alleviating neurological symptoms. Furthermore, the emotional valence of music, ranging from cheerful to poignant, elicits varied effects on AD patients’ cognitive and emotional states. 94 Notably, Garcia et al.'s findings suggest that emotionally evocative music can evoke memories in AD patients. 119 Additionally, familiar or preferred musical selections can enhance memory and linguistic capabilities. 120 Arroyo-Anllo et al.'s research highlights the role of familiar music in augmenting self-awareness among AD patients. 96 Importantly, MT demonstrates efficacy in mitigating symptoms such as anxiety, depression, and agitation, fostering a more positive behavioral repertoire in affected individuals. By promoting engagement in activities and reducing negative behaviors, such as wandering or aggression, MT cultivates a sense of accomplishment and belonging among AD patients. 95
Olfactory stimulation therapy
In individuals afflicted with AD, olfactory dysfunction manifests across a spectrum of severity. In the early stages of AD pathology particularly, degenerative processes target key olfactory structures such as the olfactory bulb and piriform cortex, notably impacting the anterior olfactory nucleus, where a proliferation of neurofibrillary tangles is observed. This degeneration disrupts the intricate connectivity between the hippocampus and cerebral cortex, impeding the transmission of crucial signaling factors necessary for complex olfactory processing. 121 It is also noted that this impairment is correlated with declines in linguistic learning and memory retention capabilities.
Olfactory stimulation therapy emerges as a promising intervention with neuroprotective properties, attenuating the deleterious effects of Aβ accumulation in the brain and serving as an efficacious strategy for ameliorating neurological dysfunction. 122 During such therapy sessions, a network of interconnected brain regions including the olfactory cortex, hippocampus, amygdala, lateral cortex, olfactory bulb, and piriform cortex is directly engaged and activated. 123 Notably, fMRI studies demonstrate robust activation within the amygdala and hippocampus, regions integral to memory processing. Given the amygdala's role within the limbic system as a pivotal hub for emotion regulation and memory consolidation, its involvement underscores the emotional resonance evoked by olfactory stimuli. Moreover, research indicates that olfactory cue memory elicits activation within the limbic system and temporal lobe structures, encompassing regions such as the middle temporal gyrus, bilateral superior temporal gyrus, temporal-parietal cortex, anterior olfactory cortex, cerebellar tonsil, and right insula, among others. 124 Consequently, odors wield a potent capacity to evoke vivid memories. Glachet et al.97,98 conducted a seminal investigation probing the impact of olfactory stimulation therapy on the autobiographical memory of past events and the imaginative faculties regarding future scenarios in AD patients. Employing a diverse array of aromas tailored to individual patient preferences, the study demonstrated that olfactory stimulation therapy significantly enhanced the vividness and clarity of both memories and future projections. This observed augmentation is attributed to the unique ability of odors to enhance autobiographical specificity, facilitated by the close anatomical proximity of neurons linking the olfactory bulb and limbic system. 125 Furthermore, the activation of the amygdala-hippocampal complex underscores its pivotal role in retrieving emotionally laden memories, 124 thus elucidating the mechanisms underpinning odor-induced autobiographical memory enhancement.
Photothermal therapy
In the realm of therapeutic interventions for AD, photothermal therapy (PTT) has garnered increasing attention owing to its precise temporal and spatial control. Leveraging photothermal materials hold promise in modulating Aβ aggregation, thereby presenting therapeutic avenues for AD. 126 These materials utilized in PTT encompass various nanomaterials adept at absorbing photon energy and converting it into heat. The research underscores the efficacy of long-wave near-infrared light (NIR) in targeting deep-seated Aβ pathology within the brain. 127 Given the temperature-dependent nature of Aβ formation, localized temperature fluctuations wield considerable influence over Aβ aggregation dynamics. Consequently, a spectrum of photothermal materials has been scrutinized for AD intervention, of which gold nanoparticles are one of the most prominent. 128 Gold nanoparticles, spanning gold nanospheres (AuNSs) and gold nanorods (AuNRs), epitomize the preeminent plasmonic nanomaterials underpinning PTT research. 128 Formulated Aβ-AuNPs conjugates, synthesized by coupling AuNPs with truncated Aβ peptides, exhibit a propensity for precipitating Aβ aggregates. Subsequent exposure to intense femtosecond laser pulses swiftly increases the temperature of AuNPs, inducing the formation of vapor nanobubbles (VNBs) around the surfaces of AuNPs. These VNBs undergo rapid collapse, unleashing high-pressure shock waves that disrupt Aβ aggregates. 129 Distinguished by reduced cytotoxicity and heightened surface plasmon resonance effects, polyethylene glycol-coated AuNRs (AuNRs-PEG) wield superior efficacy compared to AuNPs. 126 Under 800 nm femtosecond laser irradiation, transient mechanical forces acting upon AuNRs-PEG surfaces impede pre-formed Aβ fibrils, prompting their fragmentation into smaller entities marked by diminished β-sheet structures. 130 Moreover, lipid-stabilized AuNRs, endowed with negative charges, fulfill dual roles: selectively binding to cationic Aβ sequences via electrostatic interactions facilitated by anionic liposomes, thereby thwarting Aβ fibrillogenesis, and fostering thermal dissolution of mature Aβ fibrils into smaller fragments through localized hotspot generation upon exposure to 800 nm near-infrared light. 131 Additionally, near-infrared light-responsive AuNSs have been utilized in modulating fibrous Aβ formation and disassembling Aβ deposits. Ruthenium-complex-modified penetration (Pen) peptides, loaded onto PEG-stabilized AuNSs (Ru@Pen@PEG-AuNSs), not only inhibit Aβ aggregation but also disrupt Aβ fibrils effectively. This dual-action mechanism mitigates Aβ-induced cell apoptosis while facilitating the restoration of neuronal dendritic growth and branching. 132 Furthermore, metal nanomaterials endowed with plasmonic photothermal properties, including silver triangular nanoplates and Fe3O4 nanoparticles, have emerged as potent agents for the rapid dissolution of Aβ fibrils. Noteworthy investigations highlight the capacity of silver triangular nanoplates to degrade Aβ fibrils within a remarkably short timeframe under near-infrared light irradiation. 133 The process of anchoring carbon nitride (C3N4) nanodots onto Fe3O4@mesoporous silica nanoparticles and modifying them with benzothiazole aniline has yielded an intelligent nanosystem boasting metal ion chelation capabilities and targeted therapy potential. This sophisticated platform orchestrates Aβ aggregation induction and facilitates the decomposition of mature Aβ fibrils under near-infrared light irradiation, showcasing promise for AD intervention at the nanoscale level. 134
Body temperature stands as one of the earliest documented metabolic metrics, and its modulation plays a crucial role in the paradigm of healthy aging. Across the aging continuum, individuals frequently encounter disruptions in body temperature regulation, manifesting as a progressive decline in average body temperature. This physiological shift results in diminished heat generation and compromises the organism's capacity to uphold its core temperature, indicative of a gradual attenuation in the efficacy of the thermoregulatory mechanism. The waning proficiency in temperature regulation among older demographics can be attributed in part to the age-related decline in the metabolic activity of brown adipose tissue (BAT). 135 Compelling research underscores a potential nexus between the incremental emergence of metabolic perturbations and the onset of AD within the aging population. 136 Moreover, the exponential rise in AD incidence among individuals grappling with temperature regulation anomalies underscores the tantalizing prospect of temperature modulation interventions as a potential avenue for ameliorating AD pathology.
Neutral thermal refers to the condition where, within a certain range of environmental temperatures, animals do not require additional heat production to maintain core body temperature beyond the energy generated by basal metabolism. For example, the core temperature of mice is approximately 28 °C, while the core temperature of humans ranges between 36.5 to 37.5 °C, with rectal measurements most closely reflecting core temperature. In the neutral thermal zone, mammals can generate enough heat through metabolism to counteract temperature decreases, thereby maintaining a stable body temperature even without physical activity. By maintaining a neutral thermal environment, cognitive function and neuropathology can be improved in AD mice and AD patients. Research has found that exposing 3×Tg-AD mice to a warm environment of 28 °C for 7 days resulted in an average increase of 0.95 °C in rectal temperature. 137 Furthermore, intervention with a neutral thermal environment was found to restore their recognition memory function as observed through object recognition tasks and light-dark box experiments. 137 Another study exposed type 2 diabetes db/db mice to temperatures of 34 to 35 °C for 1 h and found that rectal temperatures of the mice returned to levels comparable to the control group, with a significant improvement in phosphorylation sites of tau protein. 138 For elderly individuals experiencing skeletal muscle function decline, thermotherapy can enhance their function and mitochondrial energy metabolism. A clinical study demonstrated that pulsed short-wave diathermy could increase muscle temperature, thereby reducing muscle atrophy and preventing mitochondrial dysfunction. 139 Additionally, passive heating can improve reduced cerebral blood flow and blood-brain barrier dysfunction in AD patients. A study found that thermotherapy can improve skin microvascular function, increase pulse wave velocity, and reduce vessel wall thickness, thus aiding in maintaining cerebral blood flow and blood-brain barrier function. 140 Moreover, sauna bathing has been found to increase core body temperature, lowering the risk of dementia such as AD.141,142 Research on Drebrin protein suggests that a neutral thermal environment can increase its expression. 137 Drebrin protein plays a significant role in synaptic plasticity by influencing dendritic spine morphology and structure, thereby regulating memory function.143,144 The increase in temperature in a neutral thermal environment can also increase the expression of LRP1 transport protein, thereby reducing insoluble Aβ42 levels in the cerebral cortex, which is beneficial for improving the pathological process of AD.145,146
Moreover, a decrease in core body temperature can trigger excessive phosphorylation of tau. 137 BAT serves as the principal thermogenic tissue in mammals. By stimulating BAT thermogenesis to uphold body temperature, it can rectify thermoregulatory and metabolic aberrations, thereby impeding cold-induced tau hyperphosphorylation. 136 In a study involving aged C57BL6/129SvJ mice exposed to 4 °C cold for 24 h, a significant increase in tau phosphorylation was observed in the cortical region of their brains, accompanied by markedly elevated levels of soluble tau pThr181 and pThr231. 136 Similarly, subjecting 3×Tg-AD mice to 4 °C cold for 24 h led to heightened tau phosphorylation increased soluble Aβ protein concentration, and synaptic protein loss in the cortical region of their brains. 137 Furthermore, aged (15-month-old) 3×Tg-AD mice that were subjected to 4 °C cold exposure for 4 h per day, 5 days per week, for 4 weeks demonstrated that repeated short-term cold exposure could augment BAT thermogenesis, ameliorate glucose tolerance, and shield mice from cold-induced tau hyperphosphorylation. Notably, in mice exposed to repeated short-term cold, the expression of silencing regulatory protein 3 (SIRT3) in BAT increased. SIRT3, expressed in BAT mitochondria under fasting or cold exposure conditions, effectively stimulated BAT thermogenesis during repeated short-term cold exposure. 147 Additionally, when AD mice were exposed to 4 °C cold for 3 h per day for 3 days, it was discovered that cold exposure could counteract AD-induced lipid metabolism changes, indicating the potential protective effect of brief cold exposure intervention against AD. 148 In summary, a thermoneutral environment primarily increases Drebrin content and reduces insoluble Aβ in the cerebral cortex, while repeated short-term exposure to 4 °C induces BAT thermogenesis, improves thermoregulation and metabolic defects, and blocks cold-induced tau hyperphosphorylation. This suggests that correcting thermoregulatory defects may have therapeutic implications for AD.
Multisensory stimulation has shown promise in enhancing cognitive and emotional well-being among individuals with AD, while also mitigating psychological symptoms such as depression and anxiety, thereby improving overall quality of life. The design of multisensory environments, exemplified by Snoezelen rooms and therapeutic gardens, integrates visual, olfactory, tactile, and auditory elements, potentially playing a pivotal role in the daily care of AD patients. The Snoezelen approach, tailored for AD patients, focuses on directly stimulating the senses rather than simply providing environmental enrichment for patient activities. Conversely, therapeutic gardens encourage physical interaction with natural elements. 149 Research supporting the effectiveness of Snoezelen interventions suggests a moderate impact in reducing various challenging behaviors associated with AD. However, studies, such as the one conducted by Goto et al., 149 have demonstrated varying effects on AD patient behavior between Snoezelen activity rooms and therapeutic gardens. While the therapeutic gardens have shown positive changes, Snoezelen rooms have sometimes elicited more negative responses from participants. Investigations by Rivasseau et al. 150 have delved into the therapeutic effects of different sensory stimuli in therapeutic gardens, highlighting their potential to enhance cognitive function and alleviate psychological symptoms in AD patients, ultimately fostering interpersonal connections and communication. Additionally, Gueib et al. 151 have observed enhancements in self-awareness among AD patients engaging in multisensory therapeutic garden activities. In our study, we explored the effects of a multifaceted intervention involving voluntary wheel running, involuntary treadmill running, and auditory and visual stimuli on neuroregeneration and behavioral outcomes in an AD mouse model. The findings revealed a significant reduction in toxic proteins and promotion of neuronal regeneration following the four-week intervention, underscoring the potential of multifaceted interventions as non-invasive therapeutic strategies against AD oligomer neurotoxicity. 6
VR technology facilitates the creation of a richly immersive, dynamic, and interactive virtual environment that closely mirrors real-life experiences. In their work, Park et al. 152 leveraged VR technology for game-based training in dementia patients. Comparative analysis of pre-and post-treatment outcomes demonstrated notable enhancements in balance, emotional well-being, and overall quality of life among participants with cognitive decline who underwent VR-based therapy. MT holds promise for augmenting the emotional well-being of individuals with AD, and when integrated with VR technology, it offers enhanced focus and improved training and therapeutic outcomes. Incorporating calming music into VR training sessions can assist patients in immersing themselves more deeply into the virtual environment. In a study by Optale et al., 153 36 patients engaged in VR visual and auditory training, followed by a six-month intervention featuring soothing background music. Evaluation of participants’ linguistic proficiency, cognitive function, and depressive symptoms indicated that VR training significantly bolstered cognitive function, language proficiency, and memory among those in the treatment cohort.
An increasing body of research has confirmed the benefits of utilizing sensory and multisensory stimulation in enhancing memory and alleviating behavioral symptoms in AD patients. These approaches have been validated in AD patients, with studies demonstrating their safety and efficacy. However, the mechanisms underlying the improvement of memory and behavioral symptoms through sensory stimulation are still being explored. Moreover, these treatment modalities have garnered significant attention in clinical trials, particularly in their potential to enhance patients’ quality of life.
The lymphatic and meningeal lymphatic system
The recent discovery of the lymphatic pathway and the meningeal lymphatic system as crucial drivers of central solute clearance represents a significant advancement in understanding AD pathogenesis. 154 Research has highlighted the critical roles these systems play in the disease process. Furthermore, evidence suggests that nutritional supplementation, 155 non-invasive brain stimulation, 156 traditional Chinese medicine, 157 and exercise 158 can enhance lymphatic and meningeal lymphatic function, thereby improving the pathophysiology of AD. 159 Wang et al. used near-infrared light to regulate lymphatic drainage, which significantly improved cognitive ability in elderly and AD mice, and alleviated AD-associated pathology by reducing Aβ deposition, neuroinflammation, and neuronal damage. Moreover, light modulation can improve mitochondrial metabolism and the cellular junction of meningeal lymphatic endothelial cells (mLECs). 160 This suggests that light-enhanced lymphatic drainage promotes pathological remission and cognitive enhancement in aging and AD mouse models, which offers a potential amelioration strategy for neurodegenerative disease.
Recent experimental evidence suggests a link between physical exercise and increased glymphatic function in both healthy animals and AD animal models. Voluntary wheel running for 6 to 8 weeks enhances cerebrospinal fluid (CSF)-interstitial fluid (ISF) exchange dynamics in both healthy middle-aged animals (7–8 months old) and an animal model of AD. 161 In middle-aged animals, aerobic exercise boosts CSF glymphatic influx and meningeal lymphatic outflow to the deep cervical lymph nodes, improving ISF solute clearance. This leads to reduced extracellular Aβ deposition, decreased astrogliosis, enhanced structural and functional neural plasticity, and improved cognitive performance compared to sedentary controls. 162 Therefore, enhancing the central clearance system by increasing lymphatic or meningeal lymphatic function can be used as an adjunct to the treatment of AD.
Other interventions
Additionally, various theories have been proposed regarding the influence of diet on the progression of AD. While research suggests that diet may indeed play a role in AD, the optimal dietary approach for providing maximal neuroprotective effects remains uncertain. The ketogenic diet has been a focal point of research, particularly in the realm of neurodegenerative diseases. Yet, similar benefits to those of the ketogenic diet can potentially be attained through the consumption of a regular diet supplemented with ketone precursors. The findings suggest that supplementation with both a ketogenic diet and exogenous ketone supplements could offer therapeutic benefits to individuals with AD. 163 Furthermore, a prospective study evaluating the MIND (Mediterranean-DASH Intervention for Neurodegenerative Delay, MIND) diet score provided compelling evidence that greater adherence to holistic dietary patterns may mitigate the onset of AD. 164 Zheng et al. also delved into the feasibility of royal jelly as an adjunctive measure in both preventing and treating AD. 165
The simple twelve-minute meditation technique of Kirtan Kriya (KK) has been shown to have profound positive effects on brain function, memory retention, cellular health, genetic expression, and overall well-being. Additionally, KK has demonstrated the ability to reverse memory loss in individuals experiencing subjective cognitive decline and MCI. 166 Moreover, researchers have explored the efficacy of reminiscence therapy as an intervention for AD patients. Reminiscence therapy involves evoking memories through various stimuli such as photographs, recordings, objects, and videos, encouraging patients to reminisce about their childhood and youth while expressing emotions. This therapeutic approach helps alleviate emotional distress, maintain identity consistency, reduce agitation, facilitate social adaptation, and minimize disruptive behaviors in AD patients. 167 Numerous studies have underscored the cognitive benefits, mood improvement, and enhanced subjective well-being resulting from reminiscence therapy in AD patients.168,169 Additionally, emerging evidence suggests that oxygen therapy holds promise in ameliorating multiple pathological aspects of AD, encompassing amyloid-β metabolism, tau phosphorylation, neuroinflammation, neuronal survival, oxidative stress, neurotrophic support, mitochondrial function, cerebral blood flow, and protein synthesis. 170
Traditional Chinese medicine, encompassing practices like acupuncture, Tai Chi, fitness Qigong, and acupressure, holds considerable importance in the non-pharmacological management of AD due to its widespread acceptance and practicality among the general population. Li et al. randomly divided 70 AD patients into a control group and a treatment group with 35 cases each. The control group received routine treatment, and the treatment group received acupuncture combined with Baduanjin exercise based on the treatment of the control group, to evaluate the effects of acupuncture combined with Baduanjin exercise on cognitive behavior, activities of daily living, anxiety level, and sleep pattern of AD patients. Research results showed that acupuncture combined with Baduanjin exercise can significantly improve the cognitive function, daily function, anxiety level, and sleep quality of AD patients. 171
Therapeutic ultrasound is an alternative strategy for clearing amyloid by transiently opening the blood-brain barrier (BBB) and allowing for the uptake of blood-borne factors and therapeutic agents. 172 Ultrasound approaches are also being developed for AD interventions, including repeated scanning ultrasound (SUS) for cognitive improvement, as well as focused ultrasound (FUS) for enhancing drug delivery. In APP23 mice aged 12 and 22 months, repeated opening of the BBB with the SUS approach has been shown to activate microglia, thereby reducing amyloid and improving memory performance.173,174 Studies have shown that this relies on the opening of the BBB, rather than simply applying microbubble-free ultrasound to induce neuromodulation. 175 The underlying mechanism of ultrasound-mediated BBB opening has not been fully dissected but is involved in facilitated paracellular and intercellular transport. 176 FUS particularly when combined with microbubble infusion (FUS-MB), is being researched as a noninvasive method to temporarily disrupt the BBB. This approach allows targeted delivery of therapeutic agents into the brain, which has shown promise in reducing amyloid-β and tau pathology, promoting neurogenesis, enhancing neural plasticity, and improving cholinergic function in preclinical models of AD.177–179 Additionally, FUS stimulation alone, even without microbubbles, has demonstrated benefits such as inducing neurogenesis, modulating neural activity, and triggering immune responses, all of which are associated with cognitive and memory improvements in AD models.180–182 Clinical studies have reported no adverse effects and observed improvements in both cognitive and motor functions in patients with AD and Parkinson's disease following FUS stimulation. 183 Overall, FUS-based techniques show potential for enhancing therapeutic outcomes in AD by targeting pathological mechanisms and promoting neurological health. 184
Conclusions and future perspectives
Pharmaceutical treatment currently stands as the primary approach to managing AD, albeit with limitations, primarily only delaying or mitigating symptoms, often at a considerable expense, which significantly affects patient adherence to therapy. Consequently, enhancing the cognitive abilities of AD patients, fostering self-care proficiency, and slowing disease progression have emerged as pivotal challenges in contemporary clinical research. While non-pharmacological interventions targeting AD's pathological mechanisms are still in their infancy, mounting evidence underscores their indispensable role in future AD care. Studies have underscored that non-pharmacological interventions not only ameliorate cognitive function in AD patients but also bolster their psychological resilience and physical activity levels. Compared to singular intervention methods, the amalgamation of various non-pharmacological approaches yields superior outcomes. Moreover, non-pharmacological interventions typically entail fewer adverse effects and offer a more cost-effective alternative to pharmaceutical options, thus charting novel therapeutic pathways in AD management.
Several non-pharmacological interventions proposed in this article have been shown to benefit AD patients. However, in clinical intervention experiments, factors such as cognitive impairment, prolonged intervention duration, and low engagement hinder patients’ compliance, thereby impeding the effective achievement of intervention goals. Consequently, most clinical trials tend to select subjects biased towards patients with mild cognitive impairment. These trials mostly result in conclusions favoring the preventive effects of non-pharmacological interventions on only cognitive disorders, with studies on the effect of non-pharmacological interventions on AD progressing slowly. This slow progress in improving AD through non-pharmacological interventions is exacerbated by differences in gender, sample size, and age of subjects during interventions, resulting in inconsistent experimental results. Presently, clinical studies primarily rely on neuropsychological test outcomes, lacking physiological indicators and standardized measurement criteria for evaluating non-pharmacological improvements in pathological symptoms. To address these limitations, future interventions could utilize artificial intelligence technology to design diverse and engaging interventions, enhancing patient compliance and ensuring intervention sustainability to achieve desired outcomes. At the same time, pharmacological and non-pharmacological interventions can be combined to improve their specificity and cost-effectiveness. Additionally, conducting hematological and imaging examinations alongside neuropsychological tests can validate the objective effects of interventions on patients.
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Min Tang (Formal analysis; Resources; Writing – original draft); Jie-jie Guo (Investigation; Writing – original draft; Writing – review & editing); Rong-xia Guo (Resources; Supervision); Shu-jun Xu (Conceptualization; Formal analysis; Resources); Qiong Lou (Investigation; Validation); Qiao-xia Hu (Funding acquisition; Resources); Wan-yi Li (Writing – original draft); Jing-bo Yu (Investigation; Methodology); Qi Yao (Conceptualization; Project administration); Qin-wen Wang (Conceptualization; Project administration; Supervision; Writing – review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (32171035), Zhejiang Key Research and Development Project (2024C03101), Ningbo Key Research and Development Project (2023Z173), Basic Public Welfare Research Program of Zhejiang(LGF22H090008), Zhejiang Medical and Health Technology Project (2023KY284, 2021KY1228), Science Foundation of Ningbo Rehabilitation Hospital (2022KY02). This project was also sponsored by K.C. Wong Magna and funded at Ningbo University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.