
Abstract
Background
Controversies exist around the external validity of clinical trials on disease-modifying treatments for Alzheimer's disease (AD). Detailed information on the clinical characteristics of research participants is lacking, hampering the understanding of their representativeness.
Objective
This study aimed to systematically review the baseline comorbidities and health status of patients with AD enrolled in clinical trials.
Methods
A systematic review of scientific and gray literature was conducted. Randomized controlled trials, enrolling participants in the AD continuum, and testing amyloid- and tau-targeting monoclonal antibodies were selected. Data on the type of study and intervention and the baseline clinical characteristics of participants were extracted. The proportion of studies reporting information on comorbidities, integrative measures of health (e.g., number of chronic diseases and multimorbidity, frailty, and gait speed), and non-neurological concomitant therapies of participants was calculated.
Results
Thirty-six articles, referring to 41 studies (21,952 participants) were included. None of the retained trials provided information on the comorbidities or other integrative measures reflecting the baseline health status of participants. Only three studies reported data on non-neurological concomitant therapies. Five documents providing relevant information were identified through gray literature searches covering the websites of regulatory agencies and pharmaceutical manufacturers.
Conclusions
The health characteristics of patients with AD included in randomized controlled trials are poorly reported. Therefore, the external validity of the study findings cannot be fully appreciated.
Keywords
Introduction
The identification of interventions producing an enduring, favorable change in the clinical course of Alzheimer's disease (AD) is one of the main challenges facing modern medicine. 1 At the beginning of 2023, 187 clinical trials were testing novel treatments for AD, 2 with a significant share consisting of monoclonal antibodies targeting the two main neuropathological hallmarks of AD, namely amyloid plaques and tau tangles. 2 In the last years, three anti-amyloid monoclonal antibodies (i.e., aducanumab, lecanemab, and donanemab) have been approved by the US Food and Drug Administration (FDA) for use in AD.3–5 A new era has thus been ushered into AD therapy. 6 However, the refusal of the marketing authorization for aducanumab and lecanemab by the European Medicines Agency (EMA) has fueled heated discussions around these drugs.
Indeed, the efficacy and safety of these new AD therapeutics are the subject of an ongoing debate in the scientific community together with their affordability for healthcare systems.7–9 Controversies also surround the external validity of the studies investigating these novel compounds, i.e., whether the study findings can be generalized to other clinical settings and reasonably applied in routine practice. 10 The representativeness of the samples enrolled in AD research protocols, regarding for example age, sex distribution, educational level, and ethnoracial diversity, has repeatedly been questioned.11–13 Some studies have suggested that, based on the stringent eligibility criteria adopted in clinical trials, only a limited proportion of people living with AD would have access to recently approved treatments.14–16 Since randomized controlled trials inform prescription guidelines and regulations, poor external validity can result in inadequate treatment decision information, 17 with negative consequences for both patients and the healthcare system.
To date, little is known about the overall health status and clinical characteristics of AD patients recruited in randomized controlled trials. Previous studies focused on research protocols testing AD symptomatic therapies (i.e., cholinesterase inhibitors and memantine) revealed that baseline comorbidities and non-neurological concomitant medications of participants are poorly described.18,19 Nevertheless, there is preliminary evidence that patients with mild cognitive impairment (MCI) and AD dementia included in randomized controlled trials are more robust (or less frail) than those encountered in daily practice.20,21 The availability of detailed information on the health characteristics of individuals with AD participating in clinical trials would be helpful to discuss the generalizability of research findings and better understand the efficacy and safety profiles of the tested interventions, especially in the perspective of their adoption in real world settings. Indeed, individual comorbidities and integrative health measures (e.g., number of chronic diseases and multimorbidity, frailty, gait speed) have consistently been associated with dementia risk, clinical expression, and course.22–24 It is also plausible that some concomitant somatic illnesses as well as the overall clinical complexity of participants may affect the occurrence of adverse events.
The present study aimed to systematically gather the existing evidence regarding the comorbidities and health status of patients in the AD continuum enrolled in randomized controlled trials testing amyloid- and tau-targeting monoclonal antibodies. To achieve this goal, a systematic review of both scientific and gray literature (i.e., repositories of clinical trials and webpages of drug companies and regulatory authorities) was conducted.
Methods
The present systematic review was conducted according to the Cochrane Handbook for Systematic Reviews of Interventions 25 and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 26 (Supplemental Material). Based on preliminary searches of PROSPERO, PubMed, and the Cochrane Library Databases, no current or ongoing systematic review on the topic was identified. The final review protocol was registered on PROSPERO (CRD42023429015).
Information sources, search strategy, and selection process
The systematic review included both academic and gray literature searches.
To identify potentially relevant scientific literature, the following bibliographic databases were searched from inception to June 15, 2023: PubMed, the Cochrane Library Databases, and Embase. Articles published by July 31, 2023, were also considered if deemed relevant for the review and if they met the predefined eligibility criteria. The search strategy was developed without restrictions for language, date of publication, and study design, by combining three broad blocks of search terms referring to the following areas of interest: i) Alzheimer's disease, ii) anti-amyloid and anti-tau monoclonal antibodies, and iii) randomized study. The Boolean operator “OR” was used to combine search terms within each interest area. The three areas were then combined with the Boolean operator “AND”. A list of all investigated monoclonal antibodies was created by consulting available systematic reviews27,28 and through preliminary searches on the main registration databases (i.e., ClinicalTrials.gov and EudraCT). Full search terms and strategies are provided in the Supplemental Material.
The final search results were exported into Rayyan, a free screening assisting software, and duplicates were removed. Additional relevant sources were identified by reviewing the reference list of included studies and other published systematic reviews (i.e., snowball search). Four reviewers working in pairs screened titles and abstracts. The full texts of all potentially eligible studies were then independently screened by two reviewers. Inclusion criteria were assessed independently, and inconsistencies were resolved by consensus.
An extensive review of gray literature was also conducted using Google Scholar and navigating databases of interventional clinical studies, repositories of clinical research data, and websites of drug companies and regulatory authorities, using key terms for Alzheimer's disease and monoclonal antibodies. Information sources included, among others, the websites of ClinicalTrials.gov, EudraCT, Alzforum, Yale University Open Data Access, Clinical Study Data Request, Vivli, Food and Drug Administration (FDA), European Medicines Agency (EMA), and Pharmaceuticals and Medical Devices Agency. The gray literature search was updated to July 31, 2023.
Eligibility criteria
Studies retrieved from bibliographic databases were considered eligible if they i) were randomized, placebo-controlled trials, ii) enrolled participants with AD dementia or prodromal AD/MCI due to AD according to international diagnostic criteria,29–31 and iii) tested the safety and/or efficacy of amyloid- and tau-targeting monoclonal antibodies. Studies enrolling healthy participants or participants with MCI or dementia of different etiologies or autosomal dominant AD, and studies investigating any drug other than monoclonal antibodies were instead excluded. Case reports, case series, non-systematic or narrative reviews, study protocols, letters, commentaries, and editorials were also excluded.
Documents and sources identified through gray literature searches were considered eligible if they provided information on the baseline clinical characteristics and health status (i.e., comorbidities, concomitant therapies) of participants enrolled in randomized controlled trials testing anti-amyloid and anti-tau monoclonal antibodies.
Data items and extraction
Data were independently extracted by two reviewers using a standardized data extraction form. Disagreements were resolved by discussion, consensus, or involving a third researcher. The following information was extracted from the retained scientific publications, where available: year of publication; National Clinical Trial (NCT) number; study phase; tested monoclonal antibody; inclusion and exclusion criteria; sociodemographic and clinical characteristics of randomized participants (i.e., age, sex, education, race, APOE genotype, health status, concomitant neurological and non-neurological pharmacological treatments).
The clinical characteristics of participants were extracted from articles’ main texts, supplementary materials, and other reference materials. Special attention was paid to the reporting of information on comorbidities or other integrative measures of health (e.g., number of chronic diseases and multimorbidity, frailty, gait speed). Gait speed was considered among these measures as it has been repeatedly associated with the overall health status and risk profile of the older person. 32 If this information was not available, participants’ characteristics were indirectly deduced by reviewing the eligibility criteria. Exclusion criteria were categorized as “absolute” when the presence of a given clinical condition precluded participation or “relative” when eligibility depended on additional clinical considerations (e.g., on the severity or frequency of the condition) or on the judgment of the investigator. Given the study aims, we focused only on comorbidities, drug therapies, and other clinical conditions not directly related to dementia in evaluating eligibility criteria.
Risk of bias assessment
The Cochrane Risk of Bias (RoB) 33 tool was used to assess the methodological quality of eligible randomized controlled studies regarding the following aspects: random sequence generation, allocation concealment, blinding of participants and health care personnel, blinded outcome assessment, completeness of outcome data, evidence of selective reporting, and other biases. Based on the RoB, the risk of bias was classified as “low”, “high”, or “unclear”.
Data synthesis and analysis
Descriptive statistics were used to present the overall characteristics of the retained studies and documents. Categorical variables were reported as absolute numbers and percentages. Continuous variables were reported as means or weighted means and standard deviations (SD). The proportion of studies reporting information on comorbidities, integrative measures of health, and non-neurological concomitant therapies of participants was calculated.
Results
Search results
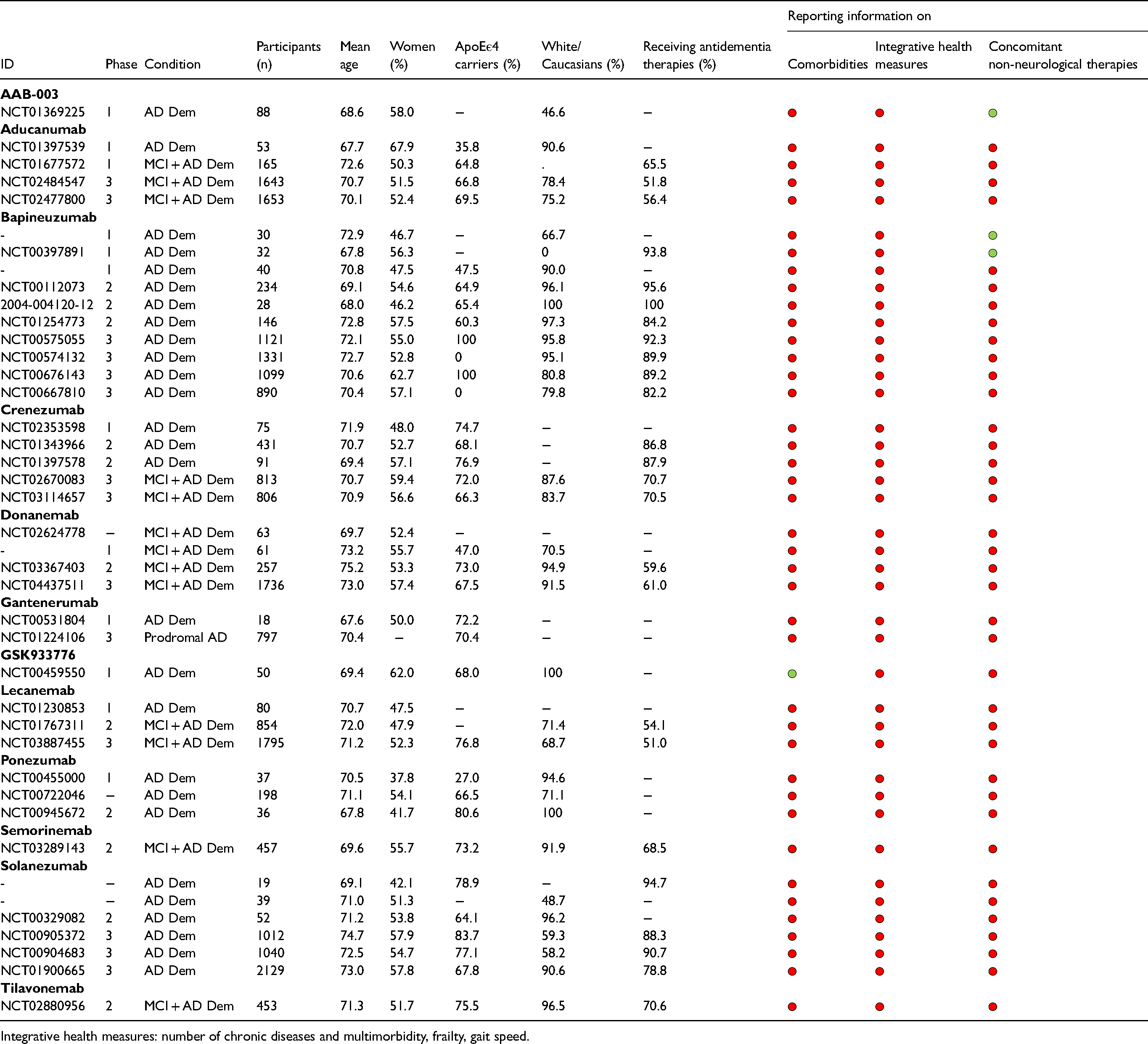
The search on literature databases yielded 1145 results, reduced to 705 records after the removal of duplicates. After the screening of titles and abstracts, 76 records were selected and assessed for eligibility. Of these, 40 were excluded as they did not meet the predefined inclusion criteria. A total of 36 articles were finally included, referring to 41 studies and 12 monoclonal antibodies (i.e., anti-amyloid monoclonal antibodies: AAB-003, aducanumab, bapineuzumab, crenezumab, donanemab, gantenerumab, GSK933776, lecanemab, ponezumab, solanezumab; anti-tau monoclonal antibodies: semorinemab, tilavonemab) (Table 1 and Supplemental Material).
Characteristics of the retained randomized controlled trials. Red dots indicate that the information was not available. Green dots indicate that the information was reported.
The gray literature search led to the identification of a poster presentation on gantenerumab, an EMA briefing document on aducanumab, an FDA briefing document and the prescribing information on lecanemab, and a conference presentation on donanemab.34–38
The flowchart of the records’ selection is presented in the Supplemental Material.
Overall, 12 phase 1 studies, 11 phase 2 studies, and 14 phase 3 studies were identified. In four cases, the study phase was not specified. A total of 21,952 participants were randomized. Twenty-six trials enrolled only participants with AD dementia (of mild to moderate severity), one was restricted to participants with prodromal AD, 39 whereas the remaining ones recruited patients with AD dementia or MCI. The weighted mean age of trial participants was 71.6 years, 51.9% were women, and 81.8% were white/Caucasians. Sixty-three % of participants were carriers of at least one APOE ε4 allele, and 70.5% were receiving antidementia medications (i.e., cholinesterase inhibitors and/or memantine) at enrollment.
The assessment of the risk of bias in each of the include study is presented in the Supplemental Material.
Comorbidities and health status of participants
Scientific literature
None of the retained scientific articles provided information on the comorbidities or other integrative measures reflecting the health status of participants. Three studies reported data on non-neurological concomitant therapies. Based on the available information, 35% of participants in a trial on AAB-003 were on antithrombotic therapies. 40 In one study on bapineuzumab, the most common concomitant medications were paroxetine (15.6%) and calcium channel blockers (15.6%), antithrombotic agents (12.5%), cough and cold preparations (12.5%), ophthalmological agents (12.5%), other hematological agents (12.5%), and influenza vaccines (12.5%). 41 In another study on bapineuzumab, all participants were receiving some concomitant medications, most often analgesics (73%), other central nervous system drugs, including parasympathomimetics (63%), vitamins (53%), anti-inflammatory or antirheumatic products (40%), psycholeptics (37%), serum lipid-reducing agents (37%), and antihypertensives (33%). 42
All the retained studies reported the adopted exclusion criteria. The most adopted absolute exclusion criteria were a history of seizure (31.7% of studies), the presence of liver dysfunction (22.0%), the current use of antithrombotics (17.1%), the presence of blood disorders (14.6%), atrial fibrillation (12.2%), and a history of TIA/stroke (9.8%) (Figure 1). As to relative exclusion criteria, most studies (61.0%) excluded patients with medical conditions that, based on the investigator's judgment, were unstable/not adequately controlled and/or could interfere with the study assessments. Several studies did not enroll participants with TIA/stroke (51.2%), cardiovascular diseases (41.5%), and cancer (41.5%) if they were recent and/or clinically relevant. Patients with uncontrolled hypertension were also often excluded (34.1%).
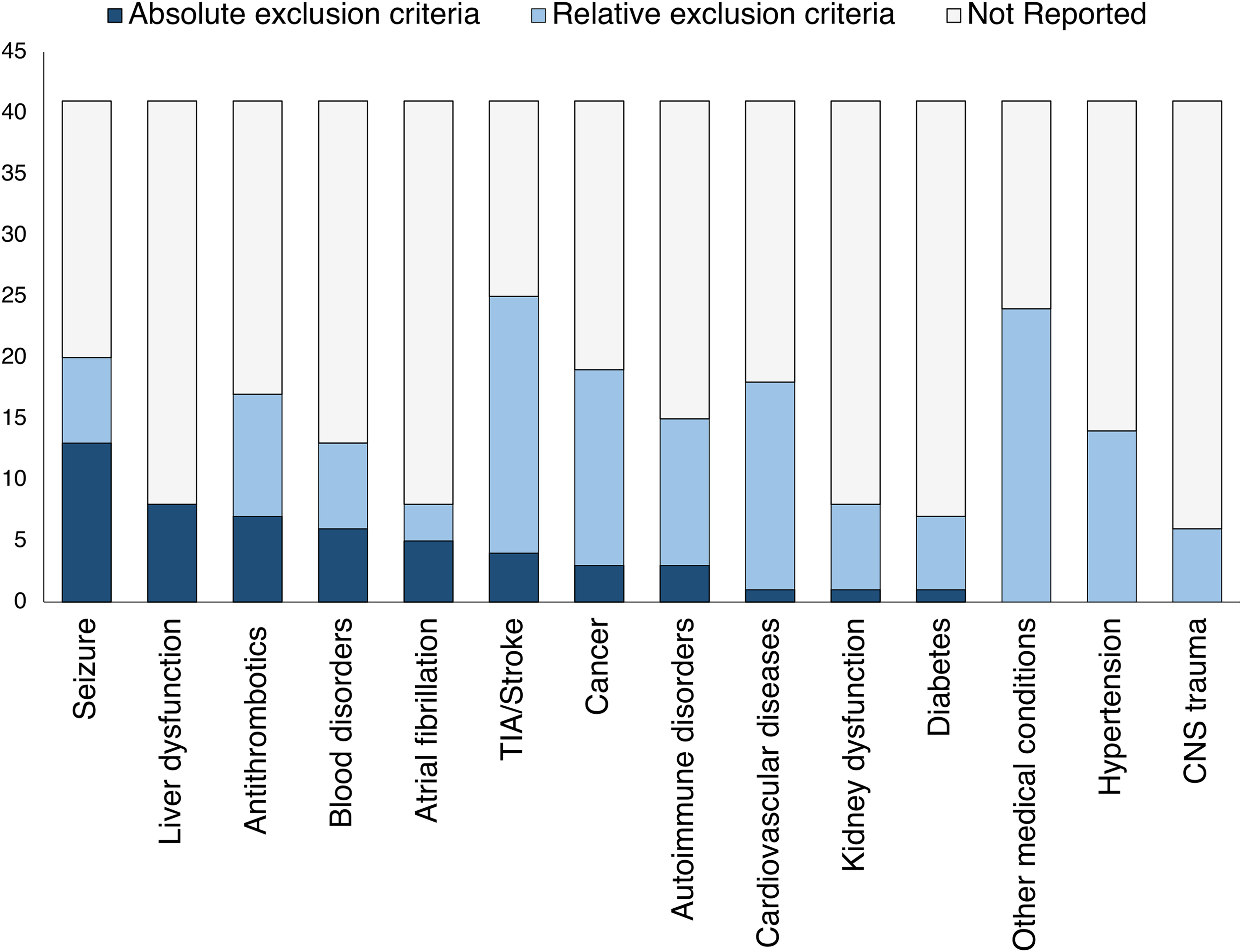
Exclusion criteria adopted in the retained randomized controlled trials. Data are shown as absolute numbers. Absolute exclusion criteria: the presence of the clinical condition precluded participation. Relative exclusion criteria: eligibility depended on additional clinical considerations (e.g., on the severity or frequency of the condition) or on the judgment of the investigator. Not reported: the clinical condition is not mentioned among eligibility criteria.
Gray literature
Based on the information provided in a poster presentation, 34 45.7% of participants in a phase 3 trial on gantenerumab (NCT01224106) had a medical history and baseline characteristics of vascular disorders, 44.7% of metabolic disorders, and 15.1% of cardiac disorders.
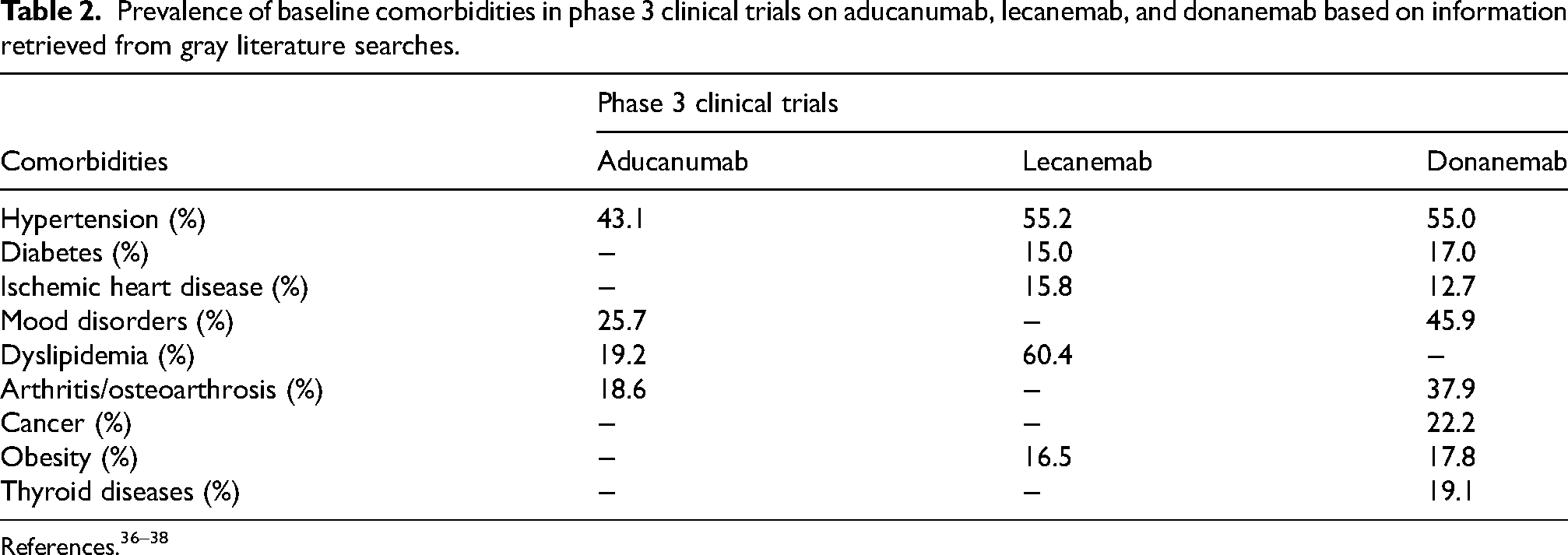
According to an EMA briefing document, 37 the most common comorbidities among participants in two phase 3 studies receiving aducanumab (NCT02484547, NCT02477800) were: hypertension (43.1% of subjects); depression (25.7%); hyperlipidemia (19.2%); hypercholesterolemia (19.0%); and osteoarthritis (18.6%).
Based on the data reported in a briefing document by the FDA Peripheral and Central Nervous System Drugs Advisory Committee, 36 the following baseline comorbidities were reported for the 1795 participants in a phase 3 trial on lecanemab (NCT03887455): hypertension (55.2% of participants); hyperlipidemia (60.4%); obesity (16.5%); ischemic heart disease (15.8%); and diabetes (15.0%). Fifty-one % of subjects had two or more comorbidities, 24.2% had three or more comorbidities, 7.7% had four or more comorbidities, and 1.4% had five or more comorbidities. Concerning concomitant medications, 28.6% of participants were on antidepressants, 27.4% on antiplatelet therapies, and 4.9% on anticoagulants.
As reported in a conference presentation on a phase 3 trial on donanemab (NCT04437511), 38 the following comorbidities were registered at the baseline for 1727 participants: hypertension (55.0% of participants); mood disorders (45.9%); arthritis/osteoarthrosis (37.9%); malignant or unspecified tumors (22.2%); thyroid disease (19.1%); obesity (17.8%); diabetes (17.0%); and ischemic heart disease (12.7%). The most common non-neurological concomitant medications were acetylsalicylic acid (31.5% of participants), cholecalciferol (26.2%), atorvastatin (25.8%), and paracetamol (24.6%).
The prevalence of baseline comorbidities reported for participants in phase 3 clinical trials on aducanumab, lecanemab, and donanemab are reported in Table 2.
Prevalence of baseline comorbidities in phase 3 clinical trials on aducanumab, lecanemab, and donanemab based on information retrieved from gray literature searches.
Discussion
To the best of our knowledge, the present study is the first attempt to systematically collect and discuss the available evidence on the overall clinical characteristics of participants recruited in randomized controlled trials testing candidate disease-modifying treatments for AD. Overall, there is a dearth of reported information on the health status, comorbidities, and concomitant non-neurological medications of research participants.
Our findings are supportive of the well-established underreporting of the clinical characteristics of older people enrolled in research protocols already observed for other major diseases such as diabetes, heart failure, chronic obstructive pulmonary disease, and stroke. 43 None of the published randomized controlled trials on amyloid- and tau-targeting monoclonal antibodies provided data on baseline comorbidities of participants, and only a striking minority reported data on concomitant therapies. This information can only be obtained through an extensive gray literature search that covers the websites of regulatory agencies and pharmaceutical manufacturers. Although the detailed description of inclusion and exclusion criteria may help delineating the clinical profile of who was eligible for the trial, it is essential to know the clinical characteristics of those who were actually included. 44 The lack of this information strongly limits the possibility of inferring the external validity of the trials. Likewise, it results in the lack of knowledge about the efficacy, safety, and tolerability of the studied treatments in people with AD seen in clinical settings who often have comorbidities and exhibit high levels of clinical complexity and polypharmacy. 45 Yet, data on comorbidities and concomitant therapies are routinely collected at the baseline of interventional studies. Investigators and drug companies are encouraged to make this data available to the communities of researchers and clinicians to support evidence-based reflections and choices. Reaching consensus on a minimum core set of clinical variables to be consistently reported in publications (even in the appendix/supplementary material) would also be important. Measures reflecting the overall health status of participants should also be considered as secondary or exploratory endpoints in clinical trial protocols.
Based on the few available data from gray literature, the prevalence of individual comorbidities observed in AD clinical trials seems to coincide with that documented in clinical settings. Indeed, based on a recent systematic review of observational studies, 30.2%-73.9% of patients with MCI and AD dementia have hypertension, 6.0%-24.3% have diabetes, 10.0%-14.4% have ischemic heart disease, 19.8%-32.3% have mood disorders, and 26.9%-38.9% have dyslipidemia. 46 However, disparities across studies in terms of patient age, study setting, ascertainment of comorbidities, and staging of AD dementia (responsible for the wide variations in the estimates) 46 prevent a straightforward comparison with the data from trial participants. Moreover, no information is available on the severity of these somatic conditions in trial settings and, thus, on participants’ overall health status and risk profile. Rather, according to the adopted eligibility criteria, subjects with severe/unstable medical conditions were mostly excluded. This suggests that patients with AD included in clinical trials are generally healthier than their counterparts in clinical settings. Accordingly, a relevant discrepancy has already been documented between trial eligibility criteria and the characteristics of real-world patients with dementia14–16 as well as between the prevalence of comorbidity in clinical trials and in the community. 47
Beyond individual comorbidities, integrative health measures like frailty may be helpful to appreciate the overall clinical complexity of trial participants and, thus, their representativeness. For instance, robust frailty indexes can be computed from trial baseline assessments covering medical history, laboratory tests, physical/neurological examination, and activities of daily living.20,21 Frailty has already been used to tentatively evaluate the external validity of AD clinical trials. 20 It has also been shown to influence the occurrence of serious adverse events and attrition in randomized controlled trials for dementia or MCI. 21 The adoption of frailty or other integrative health measures may, therefore, enhance the interpretation of the research findings and their translation in the clinical arena. 20
Phase 1 to phase 3 clinical trials mostly deal with internal validity (i.e., the extent to which the observed between-group differences can be correctly attributed to the tested intervention). Study populations are deliberately selected to avoid drug-drug and drug-disease interactions and properly assess the efficacy and safety/tolerability of the intervention. These studies are usually inadequately powered to investigate outcomes in subgroups and test effect modification even for common variables (e.g., age, sex, APOE genotype). Accordingly, the reporting of these trials is mostly restricted to the primary and key alpha-controlled secondary endpoints. Nevertheless, providing information on major clinical variables (e.g., highly prevalent comorbidities, functional status, concomitant therapies) from the early stages of drug development can consent to better design phase 4 post-marketing surveillance studies and clinically relevant post-hoc analyses. This approach would allow the identification of the clinical variables associated with more favorable efficacy and safety profiles and those predictive of poorer outcomes. Specifically, these analyses could explore whether and how AD treatment effects differ according to the extent of comorbidities for which prior hypotheses exist about potential effect modification.43 The reporting of clinical variables reflecting the overall health and functional status of participants is also pivotal in pragmatic randomized controlled trials, aiming to inform decisions and generate evidence directly applicable to clinical practice, whose conduction is increasingly advocated in the field of AD and dementia. 48
The scarcity of information on the influence of concomitant somatic diseases and medications is reflected in the prescribing information of the recently approved monoclonal antibodies (i.e., aducanumab and lecanemab). Indeed, in the FDA prescribing information for ADUHELM® (aducanumab-avwa) and LEQEMBI®, comorbidities are not mentioned.35,49 Despite the lack of clear published evidence, caution is instead suggested when considering the use of lecanemab in patients on anticoagulant therapy as this may increase the risk of intracerebral hemorrhages. 35 Providing clinicians with clear, evidence-based appropriate use recommendations (AUR) is also fundamental. Robust data on the management of special clinical situations (e.g., patients taking anticoagulants or in the need of receiving thrombolytics) are still needed to corroborate the AUR so far developed by expert panels.50,51
The present study has some limitations that are worth mentioning. We focused only on anti-amyloid and anti-tau monoclonal antibodies, thus not extending our analysis to all the compounds in the AD pipeline. However, these drugs are at the forefront of the drug development process and have garnered significant attention from the scientific community in recent years. Despite being exhaustive, the gray literature review may not have intercepted some relevant information on the topic. Still, the choice to review the gray literature arose from the need to obtain some information on the characteristics of the trial participants, otherwise not available from the analysis of published trials. Moreover, the few and heterogeneous literature data on comorbidities in AD prevent direct comparison of the characteristics of trial participants with those of clinical patient populations.
In conclusion, the comorbidities and health status of patients with AD included in randomized controlled trials are poorly reported. This precludes to fully understand the external validity of these research protocols. It appears crucial that drug companies and investigators conducting AD clinical trials adequately ascertain, describe, and report the clinical characteristics of participants and address their effect on treatment outcomes. Sharing this information with the scientific community would sustain important advancements in drug development, improve the clinical use of new therapies, and reduce safety concerns.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241289549 - Supplemental material for Reporting of comorbidities and health status of participants in clinical trials testing amyloid- and tau-targeting monoclonal antibodies for Alzheimer's disease: A systematic review
Supplemental material, sj-docx-1-alz-10.1177_13872877241289549 for Reporting of comorbidities and health status of participants in clinical trials testing amyloid- and tau-targeting monoclonal antibodies for Alzheimer's disease: A systematic review by Marco Canevelli, Antonio Ancidoni, Martina Valletta, Marco Toccaceli Blasi, Alba Rosa Alfano, Simona Buscarnera, Martina Salzillo, Filippo Nuti, Francesca Zambri, Annachiara Di Nolfi, Eleonora Lacorte, Giulia Grande, Nicola Vanacore and Giuseppe Bruno in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Marco Canevelli (Conceptualization; Data curation; Investigation; Methodology; Writing – original draft); Antonio Ancidoni (Investigation; Writing – review & editing); Martina Valletta (Investigation; Writing – review & editing); Marco Toccaceli Blasi (Investigation; Writing – review & editing); Alba Rosa Alfano (Investigation; Writing – review & editing); Simona Buscarnera (Investigation; Writing – review & editing); Martina Salzillo (Investigation; Writing – review & editing); Filippo Nuti (Investigation; Writing – review & editing); Francesca Zambri (Investigation; Writing – review & editing); Annachiara Di Nolfi (Investigation; Writing – review & editing); Eleonora Lacorte (Investigation; Methodology; Writing – review & editing); Giulia Grande (Conceptualization; Supervision; Validation; Writing – review & editing); Nicola Vanacore (Conceptualization; Supervision; Visualization; Writing – review & editing); Giuseppe Bruno (Conceptualization; Supervision; Visualization; Writing – review & editing).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
Marco Toccaceli Blasi is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Data availability
All data relevant to the study are included in the article or uploaded as supplemental information.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.