
Abstract
Background
Mild cognitive impairment (MCI) and mild behavioral impairment (MBI) are both considered potential prodromal stages of dementia, especially Alzheimer's disease. Previous literature has lacked specific information about MBI in individuals with MCI and associations of several aspects of both, MBI and MCI.
Objective
Our aim was to investigate whether associations exist between aspects of MBI and aspects of cognitive performance in certain dimensions of the Montreal Cognitive Assessment (MoCA).
Methods
We used baseline data from the double-blind randomized controlled intervention MCI-CCT-study. Current cognitive performance of individuals with MCI was measured with the MoCA. MBI was assessed with the MBI Shortscale (MBI short), which was administered through a self-report interview. Associations were assessed with Pearson correlations. Sensitivity analyses were conducted for gender and cognition. Group differences were examined with independent samples t-tests or Welch test. Significant correlations were considered in binary logistic regressions under control of covariates.
Results
There was no significant correlation between the current MoCA and MBI short scores in the total sample or in the gender-related analysis. Using dichotomized cognitive performance, significant correlations between MCI and MBI were revealed for individuals with lower MoCA scores. On the task level, several significant associations were identified between MoCA dimensions and MBI dimensions in the total sample and in the sensitivity analyses, also under control of covariates.
Conclusions
Our findings support the hypothesis that with increasing cognitive decline, the association between MCI and MBI becomes stronger. Furthermore, a certain cut-off on the MoCA must be reached to identify a correlation.
Keywords
Introduction
As a result of demographic changes, society is experiencing an increasing burden due to the rising prevalence of dementia, among other diseases. 1 In Germany, there are approximately 1.7 million people living with dementia, and as many as 50 million worldwide.2,3 Due to increases in life expectancy, the number of people with dementia in Germany is expected to rise to 3 million by 2050. Mild cognitive impairment (MCI) thereby represents a transition stage between normal aging and dementia. Thus, MCI is for some considered a precursor to dementia during which appropriate interventions can stop the progression to dementia.4,5 However, the prevalence of MCI increases with age; it ranges from 6.7% in 60- to 64-year-olds to 25.5% in 80- to 84-year-olds. 4
The dementia syndrome is characterized by three aspects: a) cognitive impairment, b) behavioral and psychological symptoms of dementia (BPSDs), and c) limitations in activities of daily living (ADLs). 6 BPSDs are early signs of dementia according to the National Institute on Aging-Alzheimer's Association 7 and their severity is associated with disease progression.8,9 Almost all individuals with dementia experience BPSD during the course of their illness. 10 If individuals with dementia live in a nursing home, over 80% of them show BPSDs. 11 Thereby, BPSDs are particularly likely to affect the quality of life (QoL) and ADLs of people with dementia, without necessarily being associated with cognitive decline. 12 However, according to Forrester et al., 5 BPSDs are associated with more rapid cognitive decline. Furthermore, within MCI cohorts these BPSDs are related to lower cognitive and psychosocial functioning. 13
Mild behavioral impairment (MBI)—consisting of the five dimensions: 1) decreased motivation, 2) affective dysregulation, 3) impulse dyscontrol, 4) social inappropriateness, and 5) abnormal perception or thought content—is a pre-dementia BPSD that occurs in individuals with MCI and normal cognition.13,14 Thereby, analogously to MCI, the concept of MBI represents the transition between normal behavior and BPSD and is considered for some a potential prodromal stage to dementia.12,15 MBI is defined as a syndrome with psychological and behavioral symptoms later-life emergent and persistent, which may manifest in the absence or presence of subjective or objective cognitive symptoms that last six months or longer.1,12–14,16–19 Moreover, MBI is a non-cognitive disease marker of neurodegenerative diseases like dementia,20–22 especially the Alzheimer's disease. 23 Thereby, MBI is related to the intensity and rapidity of the progression of cognitive impairment towards dementia.9,24 Thereby, it should not be ignored that MBI and MCI are complementary constructs, occurring also simultaneously, that should be assessed for along with cognition.25–27 Thus, according to literature, there are two risk axis for progression to dementia, which complement each other 28 : the neurobehavioral risk axis represented by MBI and the neurocognitive risk axis represented by subjective cognitive decline and MCI. If symptoms of both axes occur, the risk of cognitive decline is higher than if symptoms of one axis occur. According to the literature, the MBI dimensions of affective dysregulation and decreased motivation are most common in individuals with MCI.18,29,30 The most common cognitive impairments in individuals with MBI are impairments in attention and working memory. 31 According to Jin et al., 9 the co-occurrence of MCI and MBI is considered critical in terms of progression to dementia, as both are the consequence of the same underlying neurodegenerative disease.17,18,21,26,32
Nevertheless, based on our literature search of common databases such as PubMed and PsycINFO, there is no specific information to date on which items from the Montreal Cognitive Assessment (MoCA) are more associated with MBI. Studies that have focused on MBI or BPSD have usually considered three groups: (a) cognitively healthy people or people with subjective cognitive impairment, (b) people with MCI, and (c) people with dementia. However, a differentiated consideration of people with MCI is still missing from the literature, even though it seems to be necessary, as individuals often react with BPSD (e.g., depression or aggression) over the course of cognitive decline. 10 Therefore, our objective was to investigate potential associations between aspects of MBI and aspects of cognitive performance on the MoCA 33 in a MCI cohort from an intervention study in Germany by using a hypothesis-generating approach.
Methods
Design and sample
The data for the analyses were obtained from the baseline data from the double-blind randomized controlled intervention MCI-CCT-study. The study design was previously published as a study protocol. 34 The intervention study tested the effectiveness of computerized cognitive training (CCT) in individuals with MCI in Germany. The randomized controlled trial consisted of one intervention arm that received an individualized CCT as a self-learning system specified for people with MCI. An active control group received a basal CCT, which included simpler tasks with simple strategies (e.g., easy arithmetic operations) or tasks targeting working and long-term memory. The main objective of the study was to examine the effectiveness of the two CCT programs. In the present study, based on the described study design, a secondary data analysis was performed on the baseline data.
To recruit study participants, individuals 60 years of age or older residing in Bavaria were contacted. From the study region, a total of 507 individuals 60 years of age or older were screened for MCI between March 2020 and January 2021. The primary inclusion criterion was psychometric identification of MCI on the basis of MoCA < 25 points and Mini-Mental Status Examination (MMSE) ≥ 24 points. The criterion was met by 100 individuals. Of these individuals, 89 individuals with MCI gave written informed consent to participate in the study and were randomized. Randomization was performed regarding gender. A positive vote from the responsible ethics committee is available (No.: 58_20 B). The study was registered prospectively on the ISRCTN Registry (ISRCTN 14437015; 27/02/2020).
All described studies in humans were conducted with the approval of the responsible ethics committee, in accordance with the national law and the Declaration of Helsinki of 1975 (in the current revised version). Informed consent was obtained from all participants. Approval for the study and the manner in which consent was obtained was granted by the Ethics Committee of the Medical Faculty of the University of Erlangen (Registration Number 58_20 B).
Written informed consent to publish the results was obtained from all participants involved in the study.
Instruments
To assess the current cognitive performance of participants with MCI, we used the MoCA 33 as our psychometric test, as it is one of the most widely used screening instruments for MCI. 35 The MoCA consists of six subscales: Visuospatial Abilities, Executive Functions, Attention, Language, Short-Term Memory, and Orientation. In addition to the cognitive abilities of individuals with MCI, sociodemographic and MBI data were collected from the study participants. Sociodemographic data included age, gender, education, living situation, and employment status. MBI was assessed with the Mild Behavioral Impairment Shortscale (MBI short), 36 which is a newly validated combination of the German Mild Behavioral Impairment Checklist (MBI Checklist) 37 and the Neuropsychiatric Inventory Questionnaire.38,39 The MBI short consists of one item from each of the eight dimensions Night-Time Behavior, Changes in Eating Behavior, Agitation, Dysphoria, Anxiety, Apathy, Irritability, and Aberrant Motor Behaviors. With exception of the dimension Night-Time Behavior the other items originate from the MBI checklist. A four-level response format is available for answering, consisting of 0 (aspect not applicable) and three severity ratings ranging from 1 (mild behavioral impairment) to 3 (severe behavioral impairment). For the total behavioral impairment score, the items are summed (Range 0–24), with higher scores corresponding to more severe behavioral impairment. All data were self-reported by individuals with MCI.
Statistical analysis
All analyses (α < 0.05) were performed using IBM SPSS Statistics 28.0. Because this study involved an exploratory analysis of a hypothesis-generating character, we did not correct for multiple testing.
Main analysis
The analysis sample comprised 89 people with MCI. There were no missing values. The correlation between the baseline MCI sum score from the MoCA and the MBI score from the MBI short scale as well as the correlations between the individual items used to measure the two constructs were computed as Pearson or Spearman correlation coefficients. Further, the importance of the significant correlations at item level was checked using multivariable binary logistic regression models (dependent variable: MBI dimension), controlling for socio-demographic covariates (independent variables). Therefore, in the first block, the sociodemographic covariates age, gender, and education were included in the model using Enter method, and in the second block, the MoCA dimension (independent variable), which correlates significantly with the MBI dimension, was also included using Enter method.
Sensitivity analyses
In sensitivity analyses, we also computed a gender-specific analysis and a cognition-related analysis regarding the correlations that emerged significant at item level in the total sample. In the present sample, MCI was defined on the basis of a rather high cut-off in the MoCA score (MoCA < 25). According to Thomann et al., 40 such a high cut-off offers higher sensitivity at the expense of a somewhat lower specificity, and therefore, they prefer to use a cut-off of MoCA < 24 because it offers a better balance between sensitivity and specificity. For this reason, we conducted the cognition-related sensitivity analysis with cut-off MoCA < 24, as the inclusion criterion for MCI in our study was MoCA < 25. In addition to the correlational analyses, gender-related group differences (women versus men) were examined with independent samples t-tests, or, when Levene's test was significant, with Welch test. Because the requirements for parametric tests were not met in the cognition-related analysis (n < 30), we used the Mann Whitney U test as the nonparametric alternative to test cognition-related differences (higher cognitive impairment versus less cognitive impairment).
The importance of the significant correlations at item level was checked using binary logistic regressions accordingly to the procedure in the main analysis.
Results
Sample characteristics
Sample characteristics are reported in Table 1. The mean age of the study participants was 73.46 years, with approximately two fifths female participants, and one fifth lived alone. One in eight was still employed. Participants showed an average MoCA score of 22.15 points. MBI was reported on at least one dimension by 55 individuals (61.8%). Irritability (25.8%), Apathy (22.5%), and Night-Time Behavior (20.2%) were most frequently reported (see Table 1). Aberrant Motor Behaviors were reported least frequently (4.5%).
Sample characteristics.
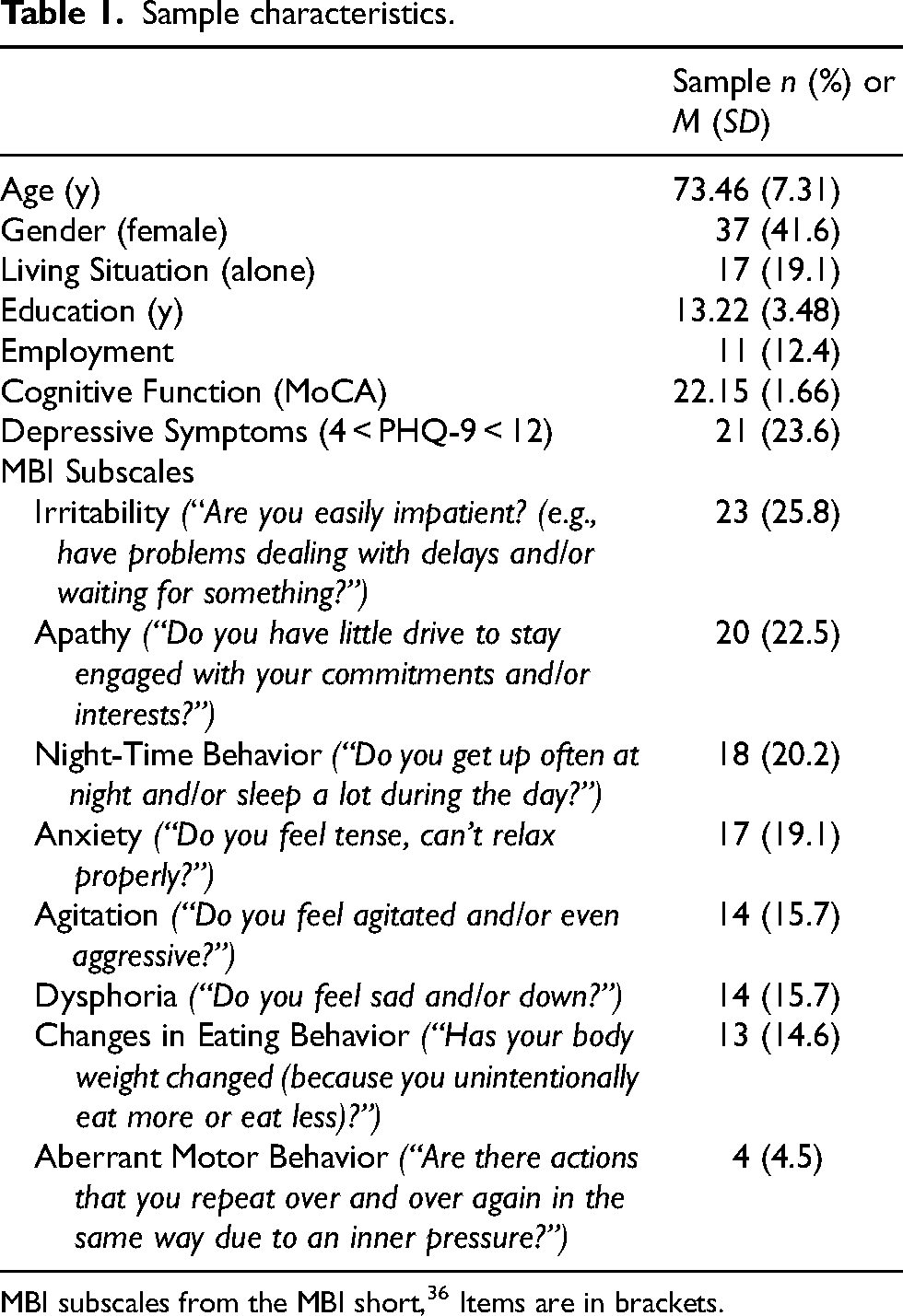
MBI subscales from the MBI short, 36 Items are in brackets.
Association between MCI and MBI
The current MoCA and MBI short scores were not significantly correlated in the overall sample. Only at the task level could correlations with the MoCA tasks be identified for the MBI dimensions Changes in Eating Behavior, Agitation, and Irritability. The MBI dimension Changes in Eating Behavior was significantly correlated with cognitive abilities Attention and Language. The MBI dimension Agitation was also correlated with Attention. The MBI dimension Irritability was significantly correlated with Visuospatial Abilities. A summary of the notable bivariate results and the results of the multivariable regression models is presented in Table 2.
Summary of the correlations between the MBI short and the MoCA—in the total sample and in the gender- (women versus men) and cognition-based subsamples.
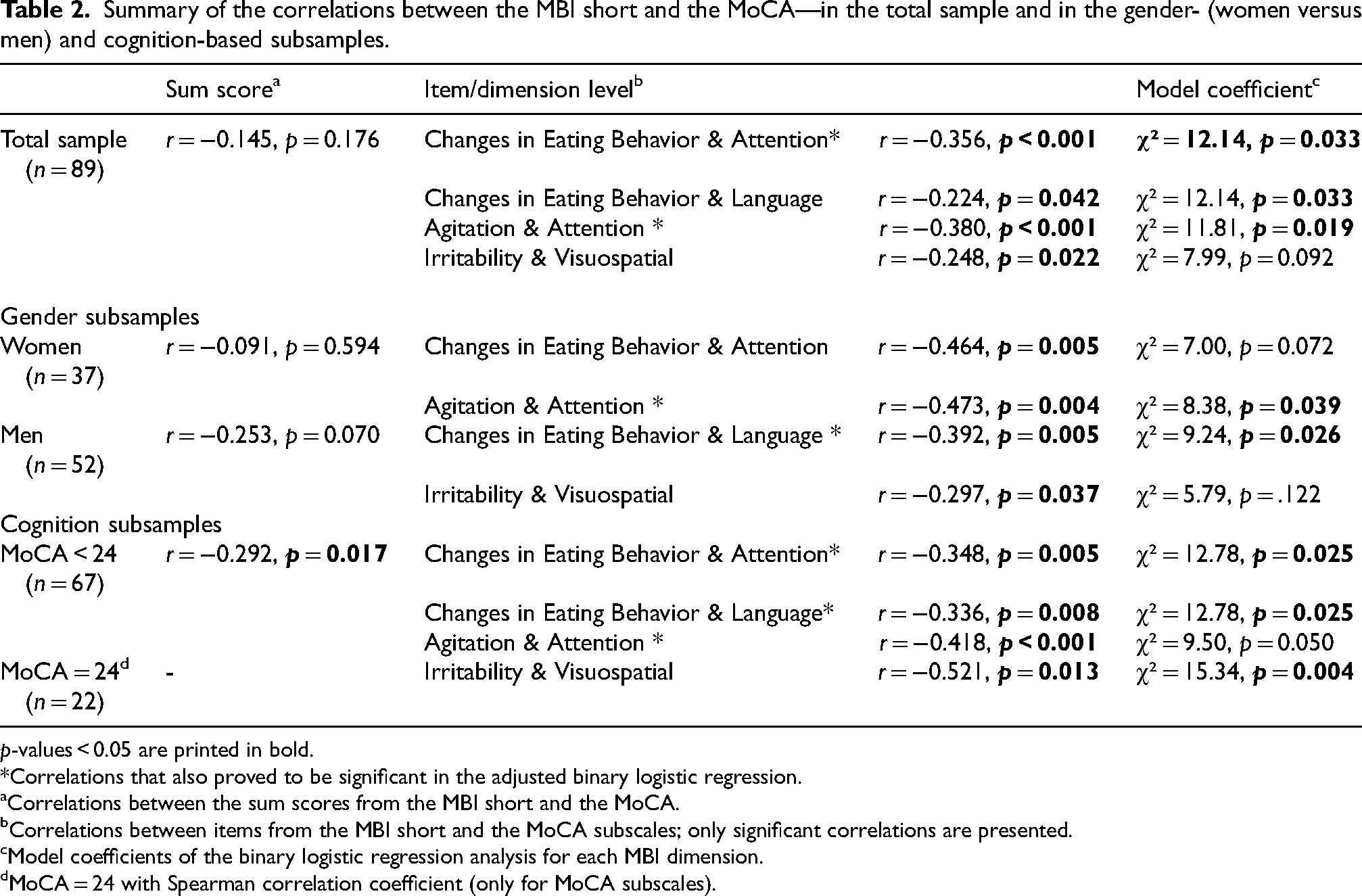
p-values < 0.05 are printed in bold.
*Correlations that also proved to be significant in the adjusted binary logistic regression.
Correlations between the sum scores from the MBI short and the MoCA.
Correlations between items from the MBI short and the MoCA subscales; only significant correlations are presented.
Model coefficients of the binary logistic regression analysis for each MBI dimension.
MoCA = 24 with Spearman correlation coefficient (only for MoCA subscales).
The multivariate, adjusted binary logistic regressions regarding the four identified bivariate correlations, controlling for socio-demographic covariates, showed that the MBI dimension Changes in Eating Behavior (χ² = 12.14, df = 5, p = 0.033; ORAttention = 0.317) and Agitation (χ² = 11.81, df = 4, p = 0.019; ORAttention = 0.282) were significantly negatively associated with Attention in the MoCA. No significance was reached for the MoCA dimensions in the regression models for the other two bivariate correlations identified.
Gender-related analysis
We found significant gender differences in the MoCA sum score (t = 2.055, df = 87, p = 0.043, d = 0.442, 95% CI [0.014, 0.867]; MoCAwomen = 22.57; MoCAmen = 21.85). There were no gender differences in the single tasks in the MoCA or in the MBI score (t = 1.139, df = 87, p = 0.258, d = 0.245; 95% CI [−0.179, 0.667]; MBIwomen = 2.11; MBImen = 1.62).
In the subgroup of women, there were correlations between MoCA items and MBI dimensions (Table 2): Change in Eating Behavior with Attention and Agitation with Attention. The multivariate, adjusted binary logistic regression analysis confirmed the significance of the association between Agitation and Attention (χ² = 8.38, df = 3, p = 0.039; ORAttention = 0.263).
In the subgroup of men, the following correlations were found between MoCA items and MBI dimensions (Table 2): Change in Eating Behavior was correlated with Language, and Irritability was correlated with Visuospatial Tasks. The multivariate binary logistic regression analysis confirmed the significance of the correlation between Changes in Eating Behavior and Language (χ² = 9.24, df = 3, p = 0.026; ORAttention = 0.221).
Cognition-related analysis
The approach with the MoCA cut-off < 24 suggested by Thomann et al. 40 resulted in a sample size of n = 67. Considering the differences in MBI between participants with MoCA < 24 and MoCA = 24 showed, that there were no differences between the two groups in the Mann Whitney U test (U = 723.50; Z = −0.133, p = 0.894).
In the MCI sample with MoCA < 24, the current MoCA score and MBI score were significantly negatively correlated (see Table 2). This means that a lower MoCA score, i.e., more cognitive impairment, is associated with more behavioral impairment. Similarly, at the task level, the following bivariate correlations were identified (Table 2): The MBI dimension Changes in Eating Behavior was significantly correlated with Attention and Language, and the MBI dimension Agitation was correlated with Attention. The multivariable, adjusted binary logistic regression analysis confirmed the significance of all three significant associations: between Changes in Eating Behavior and Attention (χ² = 12.78, df = 5, p = 0.031; ORAttention = 0.228), Changes in Eating Behavior and Language (χ² = 12.78, df = 5, p = 0.023; ORLanguage = 0.305), as well as Agitation and Attention (χ² = 15.34, df = 4, p = 0.004; ORAttention = 0.169).
Considering the group of people with MoCA = 24, Irritability correlated significantly with Visuospatial Abilities (Table 2). Although the multivariate, adjusted binary logistic regression analysis resulted in a significant model (χ² = 14.02, df = 4, p = 0.007), there was no significant variable in the model.
Discussion
In the present analysis, the relationship between MBI and cognitive performance on the MoCA in individuals with MCI was examined at the total score and item levels. Although the newly validated MBI short questionnaire also contained a NPI aspect, only the dimensions corresponding to the MBI construct13,14 or the MBI checklist 37 showed significant correlations with MoCA dimensions on the dimensional level. Most commonly, individuals with MCI reported MBI symptoms of Irritability, Apathy, and Night-Time Behavior. Aberrant Motor Behaviors were mentioned least frequently. These findings go counter to previous findings in which, in addition to the MBI dimension Decreased Motivation, the dimension Affective Dysregulation were also most frequently reported in individuals with MCI.18,29,30 Abnormal Cognition, Social Inappropriateness, and Impulse Control Disorders were cited least frequently.18,30 However, Impulse Control Disorders have also been found to be a common category in other studies. 41 In total, MBI symptoms were reported almost as frequently in the present MCI sample as in the literature,18,29,30,42,43 although we had a smaller sample in our study and thereby less variance.
In the total sample and in the subsamples of women and men in our study, cognitive performance and MBI were not correlated with each other. As Hu et al. 44 had concluded that an increase in cognitive impairment (ranging from subjective cognitive impairment to dementia) was associated with higher MBI scores, perhaps the non-significant association between cognitive abilities measured with the MoCA and MBI can be attributed to the fact that our sample comprised only individuals with MCI. 30 Therefore, only a small range of MoCA values were considered, to which the limited within-group differences can be attributed.
In addition, we applied a relatively high MoCA cut-off score to define MCI (MoCA < 25). According to Thomann et al., 40 a cut-off of MoCA < 24 offers higher sensitivity but a somewhat lower specificity. As a result, individuals in the transitional range (i.e., between MCI and cognitively healthy) may also have been considered. This idea is supported by our finding that the association between MBI and MCI reported in the literature could be identified with high specificity in the subsample defined by Thomann et al.'s 40 cut-off of MoCA < 24.
Moreover, a lack of correlation between MBI and the objective measure of cognition (i.e., MoCA) can be concluded to indicate the coexistence of the two constructs MCI and MBI. 45 The literature also shows evidence that MBI may be related to subjective measures of cognitive performance but is not necessarily associated with objective measures.30,44,45 Because the two constructs are different but coexisting potential pre-dementia syndromes (neurobehavioral versus neurocognitive), 28 MBI is not necessarily a function of cognitive impairment. 45 However, MBI and MCI are not necessarily competing constructs, but can both occur in the prodromal stage of dementia for some. The two constructs do not have to be a mutual function but complement each other by either preceding each other or coexisting. In this respect, further research is needed to address the question whether MCI and MBI are related because they are both potential prodromal stages of dementia and are both risk factors for conversion to dementia. Therefore, longitudinal studies with big samples are necessary. In addition, there is a need to investigate whether these two aspects should be studied separately with respect to preventing the progression of dementia because of their different neurological bases, although both are consequences of the same underlying neurodegenerative disease.17,18,21,26,32
At item level, the MBI dimension Agitation was negatively correlated with Attention, the MBI dimension Changes in Eating Behavior was negatively correlated with Attention and Language, and the MBI dimension Irritability was negatively correlated with Visuospatial Ability in the total sample. In addition to Working Memory, 31 the cognitive domain of Attention had already been shown to be impaired in individuals with MBI, 19 as Working Memory is involved in both Language and Visuospatial Abilities. Rouse et al. 19 also identified limitations in Language and Visuospatial Abilities over time in individuals with MBI and MCI compared with individuals with MCI alone. Nevertheless, the association between Agitation and Attention seems to be particularly relevant, since it proved to be significant in the regression model of the overall sample as well as the female subgroup and the subgroup with greater cognitive impairment. According to He et al., 46 Agitation is associated with significantly lower Attention. Furthermore, in addition to Working Memory, Attention is the most common cognitive impairment in people with MBI.19,31 This is supported by the significant relationship between Changes in Eating Behavior and Attention. Thus, our results are in line with the current literature, while providing a link to specific MBI dimensions.
Contrary to Hu et al., 44 not every MBI dimension was found to be a significant indicator of cognitive decline in the present study. This difference may be attributable to the different ways in which we measured the two constructs, as we measured MBI with a short self-reported questionnaire and MCI with an objective test.
We found gender differences in the MoCA but not in the MBI short. In the literature, BPSDs are reported more frequently for men.47,48 With the exception of Emotional Dysregulation, MBI symptoms are also reported more frequently for men than for women,49,50 and are considered to contribute to cognitive decline in men. 49 The gender differences were also demonstrated in a MCI sample for Decreased Motivation, Impulse Dyscontrol, and Abnormal Perception. 50 Thereby, MBI symptoms appear to have a greater impact on cognition in men than in women. 49 In the present study, however, there were only small non-significant differences between women and men in the expression of MBI dimensions. Furthermore, some MBI dimensions (like Aberrant Motor Behaviors) had very small case numbers, which may limit the meaningfulness with regard to gender differences.
For women, both Changes in Eating Behavior and Agitation were negatively correlated with Attention, while the latter remained significant also in the adjusted regression model. For men, Changes in Eating Behavior were negatively correlated with Language, and Irritability was correlated with Visuospatial Abilities. In the adjusted regression model, merely the association between Changes in Eating Behavior and Language remained significant. Thereby, higher MBI values indicate greater impairment of the corresponding cognitive domain. 44
There were no differences in MBI between the groups that had more versus less cognitive impairment, a finding that is consistent with Mallo et al., 45 who found that MBI and MCI are two separate prodromal stages of dementia and are unrelated due to their different neurological natures. However, MBI and MCI are not competing or mutually exclusive constructs. They can be two coexisting constructs that can occur simultaneously, whereby they do not have to be mutually dependent, but rather complementary. 28
Nevertheless, the results of our hypothesis-generating approach revealed that in the subgroup of individuals with MoCA < 24, 40 there was evidence of a moderate 51 association between the MBI short sum score and the MoCA sum score. In addition, at item level, the three regression models that were significant either in the total sample or in one of the two gender samples proved to be relevant in this subgroup of individuals with MoCA < 24. Presumably, only with significant progression of cognitive impairment in MCI during the progression to dementia could MBI be considered to be related to cognitive decline. 24 Furthermore, it is possible that MBI symptoms represent a continuum across the course of MCI that increases in intensity as cognitive impairment progresses. In this regard, as a result of the cognition related sensitivity analysis, the MoCA cut-off suggested by Thomann et al. 40 seems to be a crucial threshold for detecting correlations between MCI and MBI. This finding supports the results of the review by Jin et al. 9 in which they found that MBI usually occurs in the preliminary stage of Alzheimer's disease after the onset of MCI.
It should be taken into account that MBI can occur in all stages of pre-dementia,1,9 even in cognitively healthy individuals. Still, future studies should clarify whether MBI is a prodromal stage 12 or a marker of disease risk.21,22
Strengths and limitations
The strengths of the present analysis include the use of validated instruments (i.e., an internationally validated instrument, the MoCA, and the just currently validated MBI short). Furthermore, it is the first analysis to provide detailed information about correlations between several cognitive domains and MBI.
Nevertheless, the present analysis has some limitations. The present study is limited by the small sample size, the educational level of the sample, the missing gender balance, the requirement of the willingness to use technical devices and the availability of appropriate technical devices. In addition, because we analyzed secondary data from an intervention study on MCI, the results are not representative but merely hypothesis-generating. Furthermore, the individuals with MCI gave self-reports on aspects of MBI, and we did not include external ratings (e.g., from spouses). Therefore, biases due to subjective assessments of their abilities or due to socially desirable response tendencies cannot be fully avoided. In future research, external ratings should also be included in order to avoid socially desirable response tendencies. In addition, current cognitive abilities were assessed using only objective measures of cognitive performance, without including subjective measures. Further, with this correlational cross-sectional analysis at the item level, no causal inferences can be drawn.
Conclusion
Based on the detailed examination of MCI and MBI in this cross-sectional study, the present findings appear to support previous findings that have suggested MCI and MBI are complementary constructs, occurring also simultaneously, that are two risk axes for progression to dementia, which complement each other. Thereby, there is a certain MoCA cut-off that must be reached before a correlation between MoCA dimensions and MBI dimensions can be identified. Consequently, the hypothesis can be generated from the results that the stronger the cognitive impairment develops toward the dementia stage, the stronger the association of MCI with MBI. Therefore, longitudinal data should be collected on the association between MCI and MBI and on symptom improvement, worsening, or constancy.
Footnotes
Acknowledgments
We would like to thank all study participants for participating in the study. Special thanks go to Reinhard-Frank-Foundation, whose support made the study possible. We also thank our English language editor, Dr Jane Zagorski.
Author contributions
Julia-Sophia Scheuermann (Conceptualization; Formal analysis; Investigation; Methodology; Resources; Visualization; Writing – original draft); Elmar Graessel (Conceptualization; Funding acquisition; Methodology; Project administration; Supervision); André Kratzer (Methodology; Visualization; Writing – review & editing); Petra Scheerbaum (Methodology; Visualization; Writing – review & editing).
Funding
This study was funded by the Reinhard-Frank-Foundation. The funding body played no role in the study design, the collection, analysis, or interpretation of the data, or in writing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data presented in this study are available upon reasonable request from the corresponding author. The data are not publicly available due to privacy.