
Abstract
Anxiety is highly prevalent in Alzheimer's disease (AD), correlating with cerebrospinal fluid/positron emission tomography biomarkers and disease progression. Relationships to plasma biomarkers are unclear. Herein, we compare levels of plasma biomarkers in research participants with and without anxiety at cognitively normal, mild cognitive impairment, and AD dementia stages. We observed significantly higher plasma tau/amyloid-β42 ratio in AD participants with anxiety versus those without, but did not observe differences at other stages or plasma biomarkers. No such relationships were evident with depression. These results support a unique pathophysiological relationship between anxiety and AD that can be reflected in plasma biomarkers, suggestive of heightened neurodegeneration.
Introduction
Neuropsychiatric symptoms (NPS), such as anxiety, depression, and other mood disorders, are common in Alzheimer's disease (AD) and AD-related dementias (ADRD).1–3 In recent years, there have been efforts to formalize NPS as part of prodromal AD diagnostic criteria, most notably as part of the mild behavioral impairment construct, characterized by the presence of NPS or behavioral change as a precursor of progression to AD.4–7 Among NPS, anxiety in particular is highly prevalent in individuals with AD, even at early stages. Anxiety prevalence varies between 10–49% among those with subjective cognitive decline and 10–70% in individuals with mild cognitive impairment (MCI), and is additionally associated with faster disease progression. 8
This relationship between anxiety and AD is also seen at the biomarker level, including structural magnetic resonance (MRI), F-fluorodeoxyglucose positron emission tomography (FDG-PET), and amyloid/tau measured via cerebrospinal fluid (CSF) and positron emission tomography (PET). 8 However, the correlation of anxiety to plasma AD biomarkers is unclear. For example, one recent study found increased plasma neurofilament light (NfL) to be significantly associated with anxiety (among other NPS), 9 while a second found significant correlations of plasma p-tau217 and p-tau181 with appetite, disinhibition, and agitation, but did not find significant associations of the tested biomarkers with anxiety. 10 Given these conflicting results, further study with plasma biomarkers across stages is needed to more properly elucidate this relationship.
Plasma biomarkers confer several potential advantages for evaluating AD pathogenesis. There is evidence that changes in plasma biomarkers may preview changes in CSF or PET biomarkers, thus potentially enabling earlier insight into the relationship of anxiety with disease progression at early stages. In addition, assessment of proteinopathy in the periphery can offer a more in-depth investigation into dynamics leading to amyloid/tau deposition in the brain.11,12 From a practical perspective, if anxiety is to be utilized as a prescreen for further biomarker investigation in vulnerable populations, plasma biomarkers offer a more cost-effective and less invasive means to assess AD risk at a biological level.
In this study, we performed a cross-sectional analysis on a research cohort of older adults to test the hypothesis that plasma AD biomarker levels differ between anxious and non-anxious participants across the AD spectrum. Specifically, given the association between faster progression of AD and anxiety, we further hypothesized that anxious participants would show higher levels of neurodegeneration biomarkers. We leveraged SIMOA technology to acquire high-fidelity measurements of plasma Aβ42, Aβ40, NfL, and total tau. Additionally, we assessed whether potential differences in plasma AD biomarker relationships were unique to anxiety by also investigating their correlations to depression.
Methods
Study participants
A cross-sectional analysis was performed on a deidentified dataset of participants evaluated at the NYU Alzheimer's Disease Research Center (ADRC) between 2006 and 2019. The NYU ADRC study is approved by the New York University Grossman School of Medicine Institutional Review Board. Participants were community-dwelling older adults living in the greater New York City metropolitan area, recruited through community events and physician- or self-referrals. NYU ADRC inclusion criteria were age >50, a study partner, fluency of participant and study partner in English or Spanish, and willingness to undergo phlebotomy and MRI. Exclusion criteria included significant non-AD/ADRD neurological disease, HIV/AIDS, organ transplantation, organ failure, significant autoimmune disease, significant psychiatric disease, malignancy within the last 5 years, and alcohol/drug abuse. The present study includes participants whose study partners gave responses to questions for anxiety and depression on the NPI-Q, and who had data for at least one AD plasma biomarker measured (n = 197).
Clinical measurements
Participants underwent clinical interviews, physical examinations, and were administered psychometric testing and other instruments according to the National Alzheimer's Coordinating Center (NACC) Uniform Data Set, in addition to NYU-specific assessments. These data were synthesized into a consensus diagnosis by ADRC Clinical Core clinicians to determine AD stage (e.g., cognitively normal, MCI, mild AD dementia). Blood was also collected and stored for evaluation of APOE genotype and measurement of AD plasma biomarkers.
Neuropsychiatric symptoms were assessed by study partner report via the Neuropsychiatric Inventory Questionnaire (NPI-Q) for anxiety, depression, and other symptoms. Participants were considered anxious or depressed if study partners answered affirmatively to the respective NPI-Q items, which are scored according to presence of the symptom (no = 0, yes = 1) and severity (mild = 1, moderate = 2, severe = 3). Total NPI-Q scores were obtained by summing presence × severity across all domains. 13 Language/semantic fluency was assessed via Animal and Vegetable tests, measuring the number of animals and vegetables participants spontaneously name in one minute. Executive/visuospatial functioning and attention was measured by the Trail Making Test Part A (Trails A), a timed test of connecting numbered circles in order.
Measurement of blood plasma biomarkers
Blood samples were collected in 10 mL EDTA tubes, gently inverted, and centrifuged at 3000 rpm for 15 min at room temperature. The plasma was extracted into propylene low-binding tubes, which were promptly stored at −80°C. Plasma samples were centrifuged 10,000 g for 5 min before use. Plasma biomarker levels of Aβ42, Aβ40, total tau, and NfL were measured using a Quanterix Single Molecule Array (SIMOA) HD-1 Analyzer and related kits. Assays were performed in duplicate using two internal standards and calibrated with an 8-point calibration curve.
Statistical analysis
Statistical analysis was performed using GraphPad Prism. Chi-squared or Fisher's exact tests were used to compare categorical and demographic data, while unpaired t-tests were performed to compare means of continuous variables between anxious and non-anxious (or depressed and non-depressed) groups of participants. A p-value of <.05 was considered to be statistically significant. For statistically significant biomarker findings, multivariable linear regression models were additionally run with single demographic/genetic variables to verify that the significance was maintained. Given the sample size, statistical significance was not adjusted for multiple comparisons.
Results
Demographic, genetic, and psychometric data for the 197 participants are summarized in Table 1. Of 197 participants, 103 were cognitively normal (CN), 53 were at MCI, and 41 were at the AD stage. Anxiety had a prevalence of 14%, 48%, and 24% at CN, MCI, and AD stages, respectively among this cohort.
Demographic and psychometric characteristics of the study population.

Values are reported as means (standard deviation) unless otherwise indicated.
We compared the levels of each plasma biomarker (Aβ40, Aβ42, NfL, tau) and relevant ratios (Aβ42/40, tau/Aβ42) between anxious and non-anxious participants across each AD stage (Figure 1, Supplemental Table 1). The tau/Aβ42 ratio was the only measure to show statistically significance (Figure 1(a), Supplemental Table 1), with plasma tau/Aβ42 ratios elevated by 66% between anxious and non-anxious participants at the AD stage (p = 0.0127). This finding persisted as significant through several multivariable linear regression models that included each demographic/genetic variable individually to adjust the p-value (Figure 1, Supplemental Table 1).
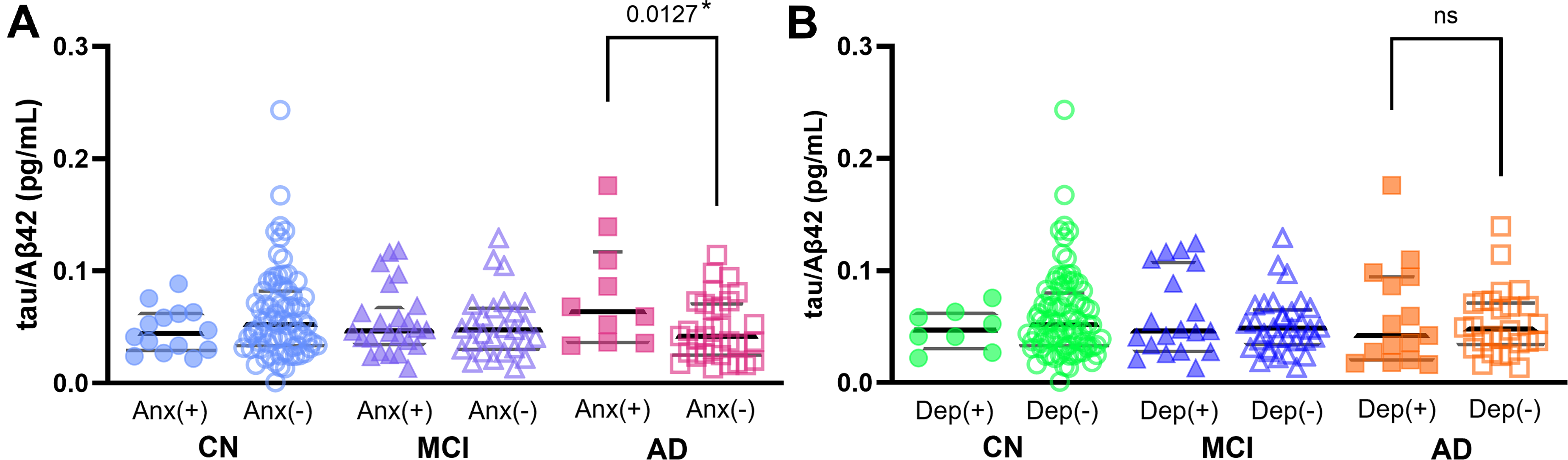
Comparisons of tau/Aβ42 levels in participants with (+, closed symbols) and without (−, open symbols) (a) anxiety (Anx) or (b) depression (dep) across stages. CN: cognitively normal (circles); MCI: mild cognitive impairment (triangles); AD: Alzheimer's disease (squares). *adjusted for age: p = 0.0171, adjusted for sex: p = 0.0222, adjusted for education: p = 0.0160, adjusted for APOE4 carrier status: p = 0.0184, adjusted for race: p = 0.0233.
In comparison to anxiety, depression had a higher prevalence of 37% at the AD stage in our cohort. Despite this increased prevalence, however, we did not observe a significant difference in tau/Aβ42 ratio associated with depression at any stage (Figure 1(b), Supplemental Table 1). Depression was also not associated with stage-specific differences in Aβ40, Aβ42, Aβ42/40, NfL, or tau (data not shown).
Lastly, we evaluated whether the higher tau/Aβ42 in the anxious AD group was associated with worsened cognitive performance (Table 2). We compared psychometric performance on global (Mini-Mental State Examination) and domain-specific tests (Animals/Vegetables, Trails A), and found no significant difference between anxious and non-anxious AD groups.
Comparisons of psychometric instrument scores between non-anxious and anxious AD participants (values reported as test scores ±SD).

Discussion
Our finding that plasma tau/Aβ42 was significantly elevated in anxious AD subjects is consistent with previous findings in CSF. In one longitudinal study of CN individuals, higher CSF tau/Aβ42 levels predicted a higher degree of anxiety and other NPS at 2-year follow-up. 14 In a prior cross-sectional study, it was observed that anxiety was significantly associated with lower levels of CSF Aβ42 and higher levels of t-tau, findings consistent with a larger tau/Aβ42 ratio. 15 Similarly to our findings, these results were not replicated in participants with depression.
Higher total tau levels are known to correlate with increased neurodegeneration, 16 thus one interpretation of elevated tau/Aβ42 ratio is a greater degree of neurodegeneration at a given level of amyloidosis. This suggests that neurodegeneration takes place more quickly at a given disease stage for individuals with anxiety, and associates with a higher level of decline. Broadly, this is in agreement with previous literature. In one 3-year longitudinal study, among participants with MCI, the presence of anxiety led to an almost 2-fold increase in conversion to AD compared to non-anxious participants, and 30-fold in comparison to cognitively normal non-anxious participants. 17 Subsequent longitudinal studies have further confirmed these findings, with one study of 812 Alzheimer's Disease Neuroimaging Initiative participants demonstrating NPI-Q reported anxiety at baseline significantly predicted MCI to AD conversion, 18 and another study of 376 amnestic MCI participants observing significantly increased conversion to AD in anxious participants (with conversion increasing in line with anxiety severity). 19 In addition, plasma tau/Aβ42 ratio has been shown to strongly correlate with increased brain tau deposition, with high sensitivity and specificity for prediction of PET amyloid status. 20
We have observed that this effect appears to be specific to anxiety, as our findings were not duplicated in participants with depression. This may suggest a pathophysiological mechanism or biomarker signature that is specific for anxiety. Alternatively, a recent review summarizes the evidence in the literature that depression in AD, in contrast to anxiety, may potentially arise more from psychosocial factors surrounding the disease, rather than a physiological mechanism. 21 Interestingly, we found that cognitive testing did not significantly differ between anxious and non-anxious AD participants, despite the significant difference in plasma tau/Aβ42. This finding adds further support to the theory that AD-related anxiety may not, in fact, be solely a psychosomatic response to the knowledge of cognitive decline, but instead perhaps has some heretofore undescribed physiological mechanism that is observable via biomarkers. Another possibility is that the rate of decline from the MCI stage to AD is increased in participants with anxiety, 22 such that similar cognitive performance is reached over a shorter period of time.
Strengths and limitations
Strengths of our study include a robustly phenotyped cohort, consensus diagnoses, and evaluation of plasma biomarkers via an ultrasensitive protein detection method. However, there are also limitations to this study. First, our study evaluated NPS via the NPI-Q, which is partner-based, and thus results may differ from participant-based assessments. Second, the study cohort was modest in size and largely non-Hispanic White. Smaller cohort size comes with risk of the study sample results not being generalizable to the population at large. Also, given the relative lack of biomarker research in underrepresented populations and known social and cultural factors that affect AD risk, there remain potentially underexplored biomarker associations with anxiety that might not be well addressed by the current study.23–26
Future directions
Although the present study results suggest a significant association between anxiety and tau/Aβ42, a longitudinal study is necessary to determine causal directionality. Future work must focus on plasma biomarkers collected at different timepoints, as well as determining whether biomarker changes occur when non-anxious individuals with AD progress to having anxiety.
In addition, given demographic shifts which will increase the percentage of individuals who identify as non-white, the relative lack of studies in the AD field which focus on underrepresented minority populations, and the higher prevalence of AD in these communities, a focus on greater diversity is needed moving forward. 27 Future studies should have a more racially-diverse cohort, one which should increase the generalizability of the results and more closely resemble the changing population. 28 Lastly (and related to the previous point), continued recruiting efforts should lead to an increased cohort size, one which will more accurately reflect the population at large. 29
Conclusion
In summary, this work demonstrates that anxiety is associated with unique plasma biomarker levels in AD, potentially related to increased neurodegeneration. This supports longitudinal investigation on the association of anxiety with biomarker changes and further study of the pathophysiologic relationship between anxiety and AD.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241295324 - Supplemental material for The relationship between anxiety and levels of Alzheimer's disease plasma biomarkers
Supplemental material, sj-docx-1-alz-10.1177_13872877241295324 for The relationship between anxiety and levels of Alzheimer's disease plasma biomarkers by Mark A Bernard, Allal Boutajangout, Ludovic Debure, Wajiha Ahmed, Anthony Q Briggs, Carolina Boza-Calvo, Alok Vedvyas, Karyn Marsh, Omonigho M Bubu, Ricardo S Osorio, Thomas Wisniewski and Arjun V Masurkar in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Mark Anthony Bernard (Conceptualization; Data curation; Formal analysis; Investigation; Validation; Visualization; Writing – original draft; Writing – review & editing); Allal Boutajangout (Formal analysis; Investigation; Resources; Validation; Writing – review & editing); Ludovic Debure (Formal analysis; Investigation; Methodology; Resources; Validation; Writing – review & editing); Wajiha Ahmed (Formal analysis; Investigation; Methodology; Resources; Validation; Writing – review & editing); Anthony Q Briggs (Writing – review & editing); Carolina Boza-Calvo (Writing – review & editing); Alok Vedvyas (Data curation; Resources; Software; Writing – review & editing); Karyn Marsh (Writing – review & editing); Omonigho M Bubu (Writing – review & editing); Ricardo S Osorio (Supervision; Writing – review & editing); Thomas Wisniewski (Supervision; Writing – review & editing); Arjun V Masurkar (Conceptualization; Formal analysis; Investigation; Methodology; Project administration; Supervision; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NIH P30AG066512 and the Louis J. And June E. Kay Foundation. OMB additionally receives funding support from NIA (L30AG064670, K23AG068534, R01AG082278, RF1AG083975), Alzheimer's Association (AARG-D-21-848397), American Academy of Sleep Medicine (AASM-231-BS-20), and BrightFocus Foundation (BrightFocus-ADR-22-924755), TW receives additional funding from NIA P01AG060882. AQB receives additional funding from Alzheimer's Association (AARF-D-24-1243696). RSO is additionally funded by NIH R01AG072644, R01AG056031, R01AG056531, and R21AG067549.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Arjun V. Masurkar is on the council for the Alzheimer's Association International Research Grants Program and the steering committee for the Alzheimer Disease Cooperative Study, both unpaid positions. All other authors have no conflict of interest to report.
Data availability
The data supporting the findings of this study are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.