
Abstract
Introduction
Alzheimer's disease (AD) is the most prevalent form of dementia in older adults, characterized by chronic, progressive, and neurodegenerative brain disorders. As the global population ages, the prevalence of AD is increasing, leading to significant humanistic and economic burdens. 1 By 2060, the number of individuals affected by AD is projected to reach approximately 13.8 million. 2 Despite ongoing research efforts, the pathogenesis of AD remains poorly understood, and current prevention and treatment strategies are inadequate. Currently, the management of AD primarily focuses on slowing disease progression, improving cognitive symptoms, and controlling psychobehavioral manifestations. 3 In recent years, a growing body of evidence has suggested that acupuncture could be a viable and effective complementary and alternative therapy for treating AD.4,5 However, there remains a lack of comprehensive and systematic research in this field. Therefore, this study aimed to review randomized controlled trials (RCTs), systematic reviews (SRs), and meta-analyses (MAs) to assess the current state of research, identify shortcomings, and address existing issues. Our findings aim to provide evidence-based support for using acupuncture in treating AD and indicate directions for clinical research.
Methods
Search strategy
The electronic databases used for the systematic search from their inception to September 10, 2023, included PubMed, Embase, Cochrane Database of Systematic Reviews (CDSR), Cochrane Controlled Trials Register (CENTRAL), China National Knowledge Infrastructure (CNKI), Chinese BioMedical Literature Database (CBM), Chonqing VIP (CQVIP) and Wanfang. More details on the search strategies are provided in Supplemental File 1.
Literature inclusion and exclusion criteria
The inclusion criteria were: (1) Types of studies: This review included RCTs, SRs, and MAs, whereas network MAs were excluded. Only the journal articles were considered in the review. (2) Types of Participants: Study participants were diagnosed with AD based on various diagnostic criteria, regardless of sex, race, age, education, nationality, or severity. (3) Types of intervention: The experimental group received acupuncture therapy, either used alone or in combination with conventional therapy. (4) Type of control: The control group aimed to evaluate the effects of acupuncture. Participants in the control group received sham acupuncture treatment, placebo acupuncture, no treatment, positive drugs, Chinese medicine, rehabilitation therapy, or other therapies. 6 (5) Types of outcomes: All study results were available without limitations.
The exclusion criteria were: (1) Animal experiments, reviews, case studies or experience reports, or protocols for an RCT. (2) Documents of repeated studies or data. (3) For materials lacking data or information, if contacting the author via e-mail did not yield the necessary information.
Study selection and data extraction
Two authors (Chao Ke and Shengtao Shan) independently screened and examined the features of all articles identified using the PICOS (population, interventions, comparators, outcomes, study design) selection criteria. They then extracted data for further evaluation. After completing this work, a cross-check was conducted, and any disagreements were resolved through the arbitration of a third author (Wei Zhang).
Data extraction from RCTs included the following: general information on the study (authors, article title, journal title and year, grade, register, and funding source), patient demographic characteristics (sample size, severity of condition, and diagnostic criteria), study type, interventions, comparisons, acupuncture prescription, and outcomes.
Data extraction from SRs and MAs included the following: author, year of publication, study type, sample size, number of studies included, quality evaluation tools, interventions, comparisons, and outcomes. The acupoint prescription was pretreated as follows: (1) Unified acupoint name and location: the above acupoints were determined following the Meridian and Acupoint (“Thirteenth Five-Year Plan” textbook). The author's record was used as the standard for unusual acupoints and other special acupoints not included in the book. (2) Prescriptions were divided into two groups, with acupuncture points alternated every other treatment in the intervention group or when different acupuncture treatments were administered in both the intervention and control groups. In cases where multiple acupuncture points were identified through Traditional Chinese Medicine (TCM) syndrome differentiation, only the primary point was chosen. However, the primary and adjunct points were documented when a single syndrome type was present. (3) Each prescription included information on the meridians, acupoints, body parts, and specific points. In instances where an acupoint possesses multiple specific attributes, it was simultaneously categorized under different classifications.
Quality evaluation
The Cochrane Risk of Bias (ROB) assessment tool was used to assess the quality of each RCT. The AMSTAR 2 tool was used to assess the methodological quality of the included SRs or MAs.7,8
These seven items included random sequence generation, allocation concealment, reporting bias, performance bias, detection bias, attrition bias, and other sources of bias. The studies were assessed for bias using the criteria of “high risk of bias,” “low risk of bias,” or “unclear risk of bias.” AMSTAR 2 includes 16 items with three evaluation options for certain items: “yes,” “no,” and “partial yes.” A review with one or fewer noncritical weaknesses is classified as being of high quality; a review with more than one noncritical weakness is classified as being of moderate quality; one or fewer critical weaknesses is classified as low quality, and one with more than one critical weakness is classified as critical low quality. Two authors (Chao Ke and Shengtao Shan) independently evaluated the methodological quality of the included studies. After the above work was completed, a cross-check was carried out, and any disagreements were discussed and resolved under the arbitration of a third author (Wei Zhang).
Data analysis and synthesis
The results are presented using a combination of textual descriptions and charts. Microsoft Excel 2003, Original, Review Manager 5.3, and SPSS Modeller 18.0 software were used for data analysis and synthesis. The Apriori algorithm was initially employed to analyze the association rules between acupoints, meridians, specific points, and body parts using SPSS Modeller 18.0. Subsequently, the degree of support, confidence, and rule support was calculated, and a network map of association rules was generated to assess the compatibility of the core acupoints/meridians/specific points/body parts.
Results
A total of 6003 literature items were retrieved using the search strategy. First, 2951 articles remained after removing the duplicates. Second, 2689 records were excluded after reading the titles and abstracts of the articles. Finally, 117 RCTs, 17 MAs, and SRs were included in this study. Details of the literature screening process are displayed in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart (Figure 1). More details on the included RCTs, MAs, and SRs are provided in Supplemental Files 2 and 3.
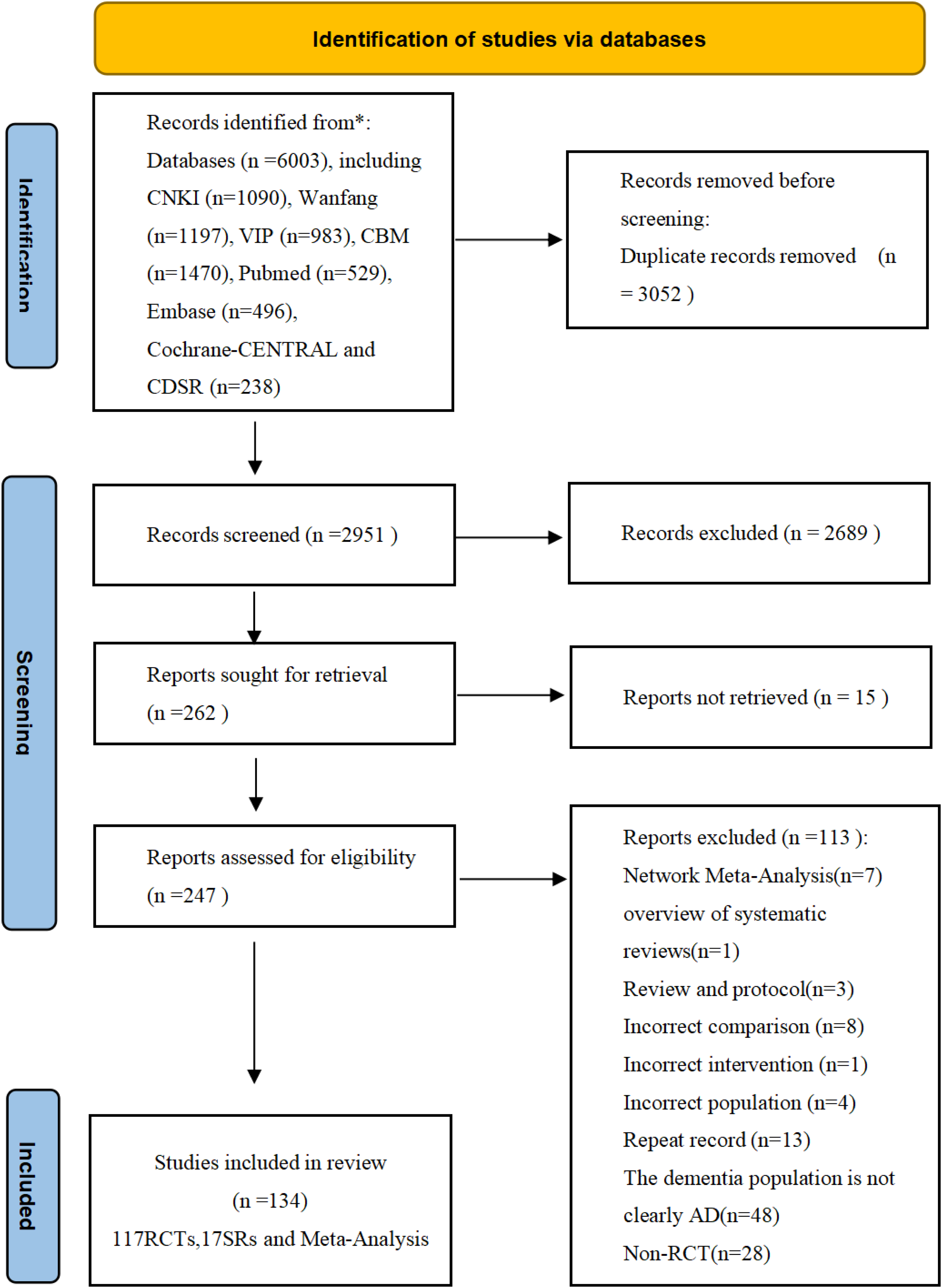
A PRISMA diagram of the literature selection.
Basic characteristics of the included studies
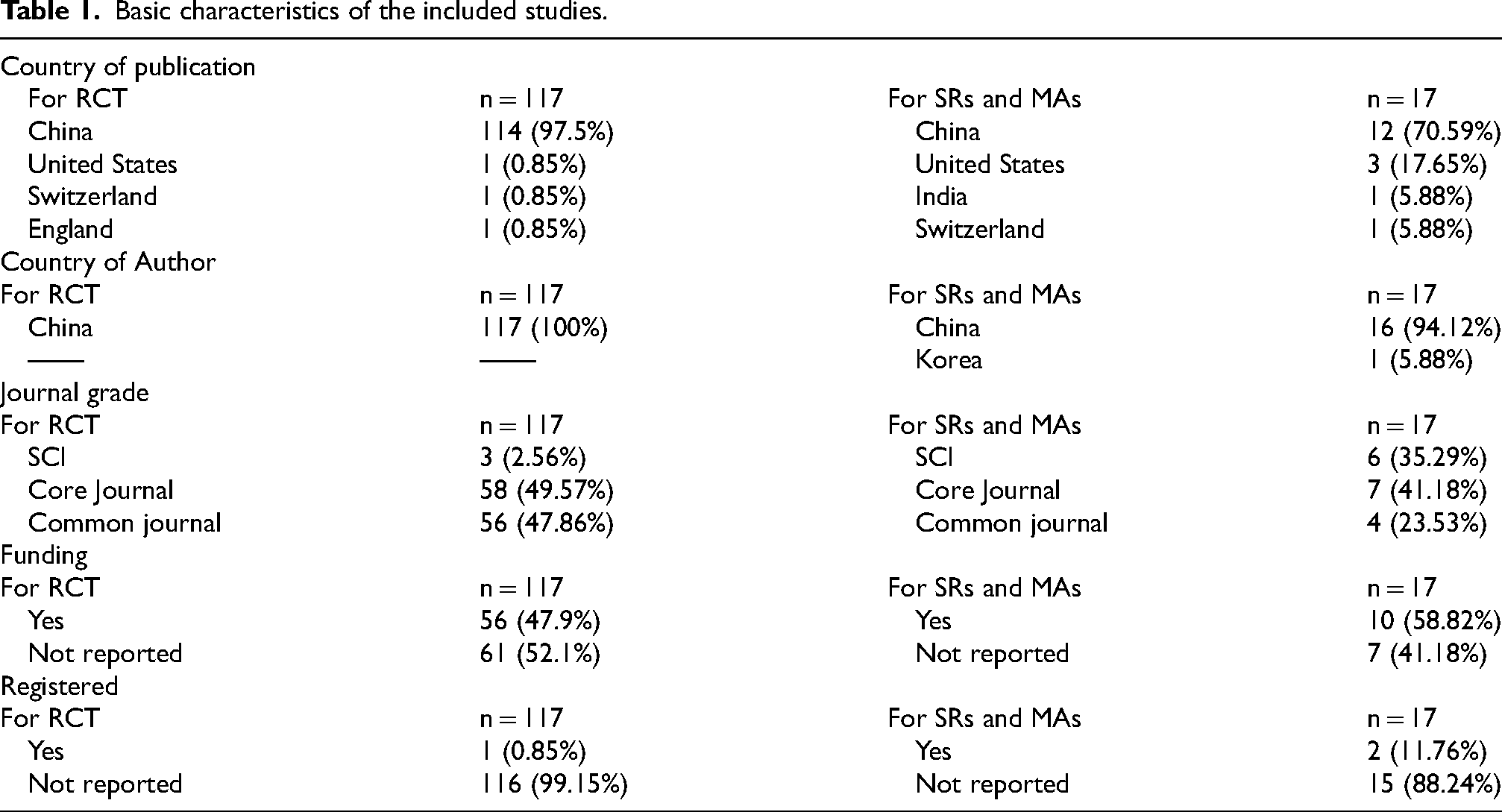
RCTs on acupuncture for AD began in 1999, and 117 RCTs were published between 1999 and September 2023. The annual publication rate of these studies showed an increasing trend, peaking in 2019. The distribution of these studies is shown in Figure 2. The data are presented in Table 1. The included papers were published in journals from five countries, with a significant proportion originating from China (114/117 [97.5%] RCTs and 12/17 [70.59%] SRs and MAs). A total of 117 RCTs were published in 76 distinct journals. Approximately 2.56% of the selected papers were published in Science Citation Index Journal (SCI), 49.57% were published in core journals such as the Chinese Core Journal Criterion of Peking University (CSCD) and China Core Periodicals of Science and Technology (CS TPCD), and the remaining 47.86% were published in common journals. The 17 SRs and MAs included in this study were published in 17 journals. Of these, 35.29%, 41.18%, and 23.53% were published in SCI, core, and common journals, respectively. Half the studies received project funding (56/117 [47.9%] RCTs and 10/17 [58.82%] SRs and MAs). Very few studies reported registration status (1/117 [0.85%] RCTs and 2/17 [11.76%] SRs and MAs).
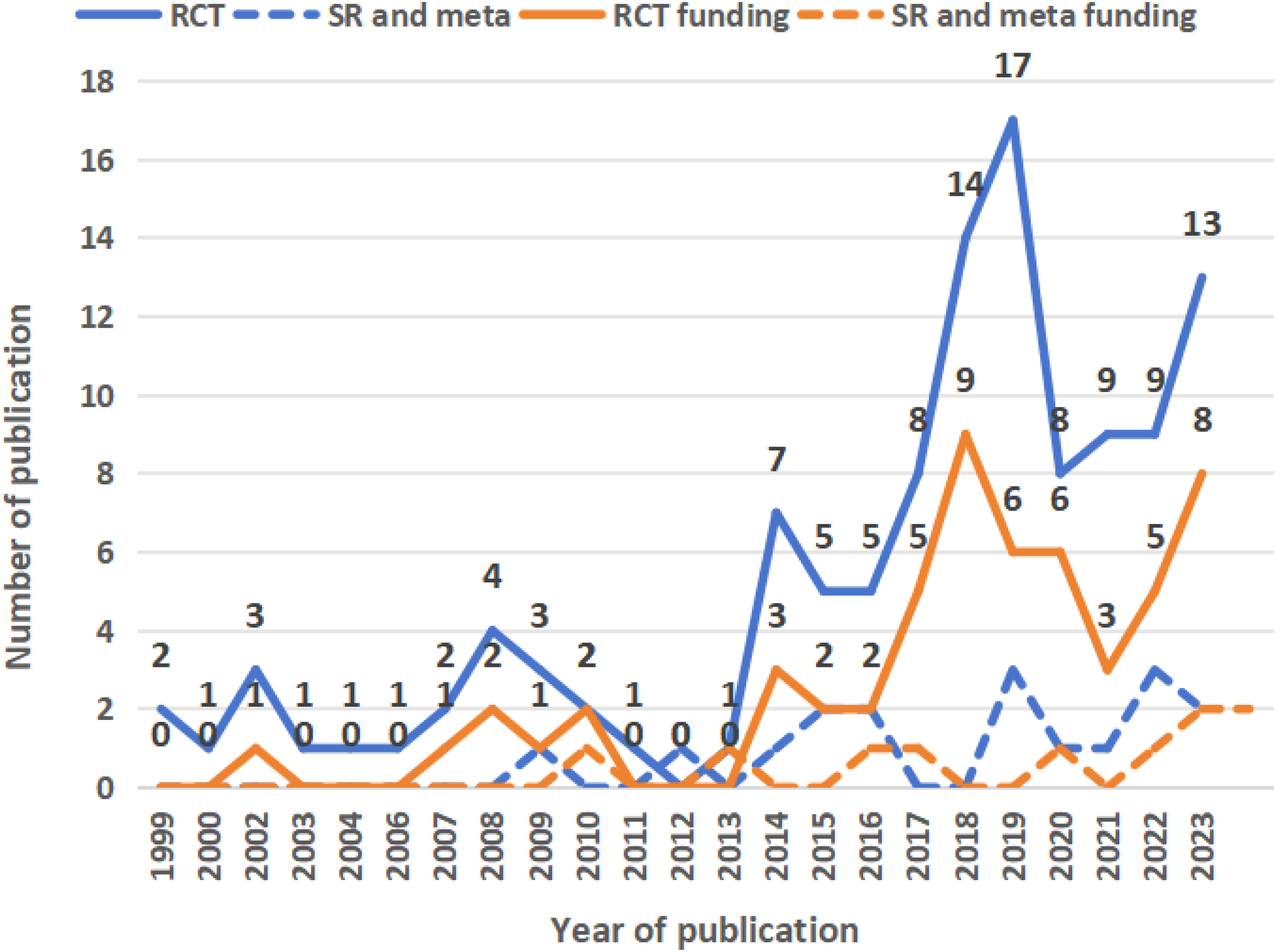
Annual publication trend and funding situation of articles.
Basic characteristics of the included studies.
RCT-related characteristics of the included studies
Characteristics of the study population. The sample sizes of the 117 studies ranged from a minimum of 17 to a maximum of 380. Most studies (68/117 [58.12%]) had sample sizes between 51 and 100. The included studies varied in patient condition severity, with most falling under the mild-to-moderate severity category (38/117 [32.48%]). Most studies reported 1–3 clear diagnostic criteria (95/117 [81.20%]), as displayed in Figure 3. Fourteen Western medicine and nine TCM diagnostic criteria were identified. The specific distributions of each criterion are listed in Figure 4.

Population characteristics of the included RCTs.

Frequency distribution of TCM and Western diagnostic criteria. The right figure represents the frequency of TCM diagnostic criteria; the left figure represents the frequency of Western medicine diagnostic criteria. “Others a” includes seven kinds of indicators, each appearing no more than twice; “Others b” includes seven kinds of indicators, each appearing no more than twice. DSM: The Diagnostic and Statistical Manual of Mental Disorders criteria; NINCDS-ADRDA: American Society of Neurology, Language Disorder, and Stroke-Alzheimer's Disease and Related Diseases Working Group criteria; NIA–AA: National Institute on Aging/Alzheimer's Association criteria; ICD-10: The 10th revision of the International Classification of Diseases; CCMD-3: Chinese Classification and Diagnostic Criteria for Mental Disorders; GDCIC: Guidelines for Dementia and Cognitive Impairment in China; GDTDC: The Guidelines of Diagnosis and Treatment for Dementia in China; GPCRNDCM: Guiding Principles of Clinical Research on New Drugs of Chinese Medicines; ACDDCED: The Assessing Criteria for the Diagnosis, Dialectic and Curative Effect of Dementia.
Characteristics of the intervention and the control. As shown in Table 2, acupuncture combined with active drugs was the most commonly used intervention (49/117 [41.88%]), followed by single acupuncture therapy (35/117 [29.9%]). The acupuncture modalities employed in treatment primarily included manual acupuncture, electroacupuncture (EA), acupoint embedding, moxibustion, and acupoint application (Figure 5). EA stimulation typically consisted of continuous or sparse-dense wave patterns, with intensity ranging from 2 to 50 Hz and currents of 0.5 to 5 mA, lasting approximately 30 min per session. Most studies administered no more than 50 acupuncture sessions (68/117 [58.12%]).

Frequency chart of the acupuncture therapies and active drugs.
Interventions, control, and comparison groups of the included RCTs.
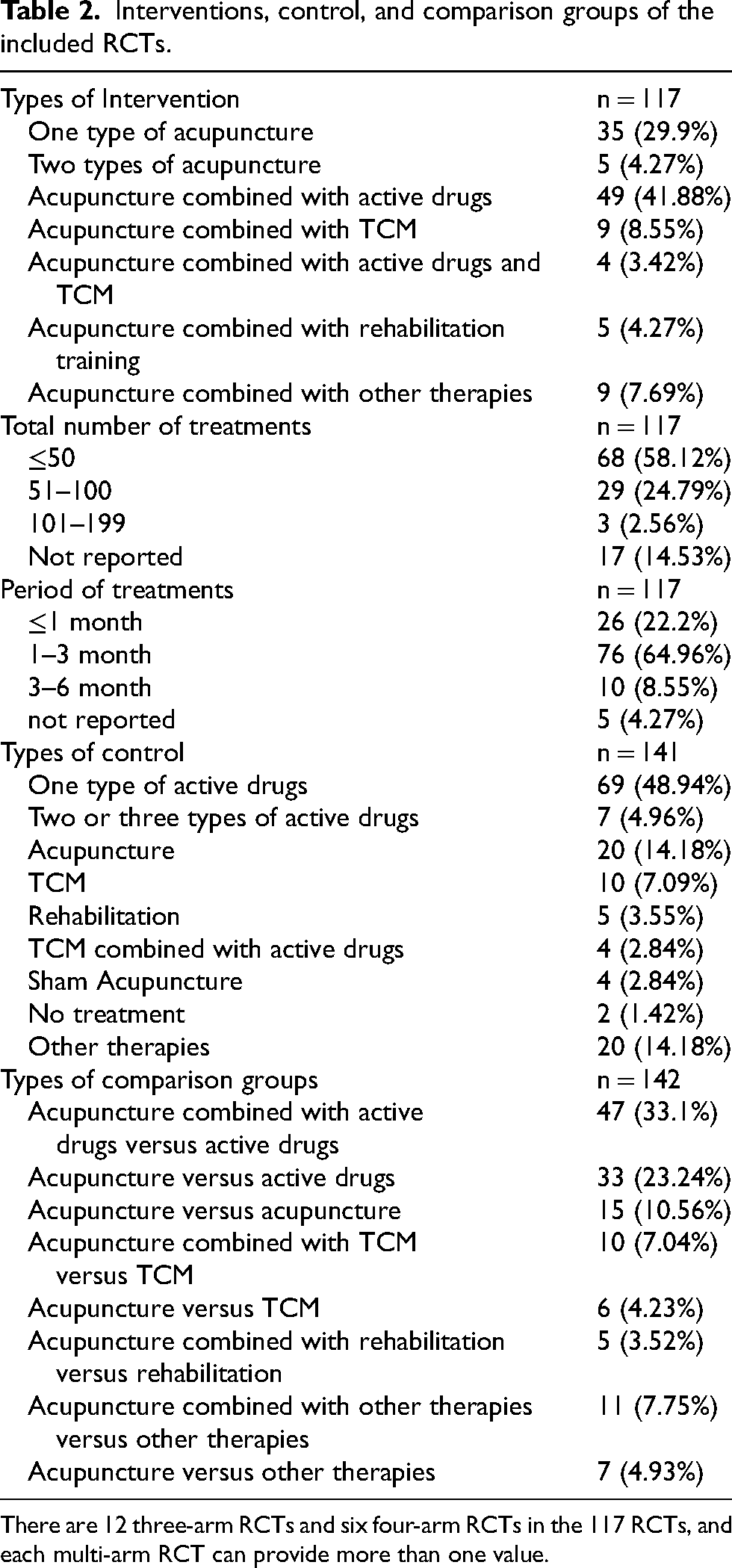
There are 12 three-arm RCTs and six four-arm RCTs in the 117 RCTs, and each multi-arm RCT can provide more than one value.
Regarding the acupuncture courses, most were concentrated in 1–3 months (76/117 [64.96%]). In the control group, the most common was the active drugs group (69/141 [48.94%]), primarily consisting of donepezil hydrochloride tablets, followed by memantine and nimodipine tablets (Figure 5). Acupuncture combined with active drugs versus active drugs (47/142 [33.1%]) and acupuncture versus active drugs (33/142 [23.24%]) ranked in the top tier of comparison.
Acupuncture prescription
A total of 117 RCTs were included in the analysis, encompassing 145 acupuncture point prescriptions utilizing 124 acupoints 861 times. As shown in Figure 6, the top ten acupoints identified were Baihui (GV20), Yintang (EX-HN1), Zusanli (ST36), Taixi (KI3), Shenmen (HT7), Shenting (GV24), Shenshu (BL23), Fengchi (GB20), Fengfu (GV16), and Dazhui (GV14). The top ten meridians were identified as Governor Vessel (GV), Stomach Meridian (ST), extra Points (EX), Gallbladder Meridian (GB), Conception Vessel (CV), Kidney Meridian (KI), Bladder Meridian (BL), Spleen Meridian (SP), Heart Meridian (HT), and Pericardium Meridian (PC). Regarding body parts, the top ten areas targeted were the head, thigh or crus, foot or ankle, back, arm, abdomen, wrist, waist, neck, and sacro-coccyx. Additionally, the top ten special acupoints included Crossing Points (CP), Back-Shu Points (BSP), Shu-Stream Points (STP), Yuan-Source Points (YSP), He-Sea Points (HSP), Luo-Connecting Points (LCP), Lower He-Sea Points (LHSP), Eight Influential Points (EIP), Front-Mu Points (FMP), and Eight Confluence Points (ECP). The core acupoint association network for acupuncture in patients with AD is shown in Table 3. The most frequently used acupoint combinations were GV20
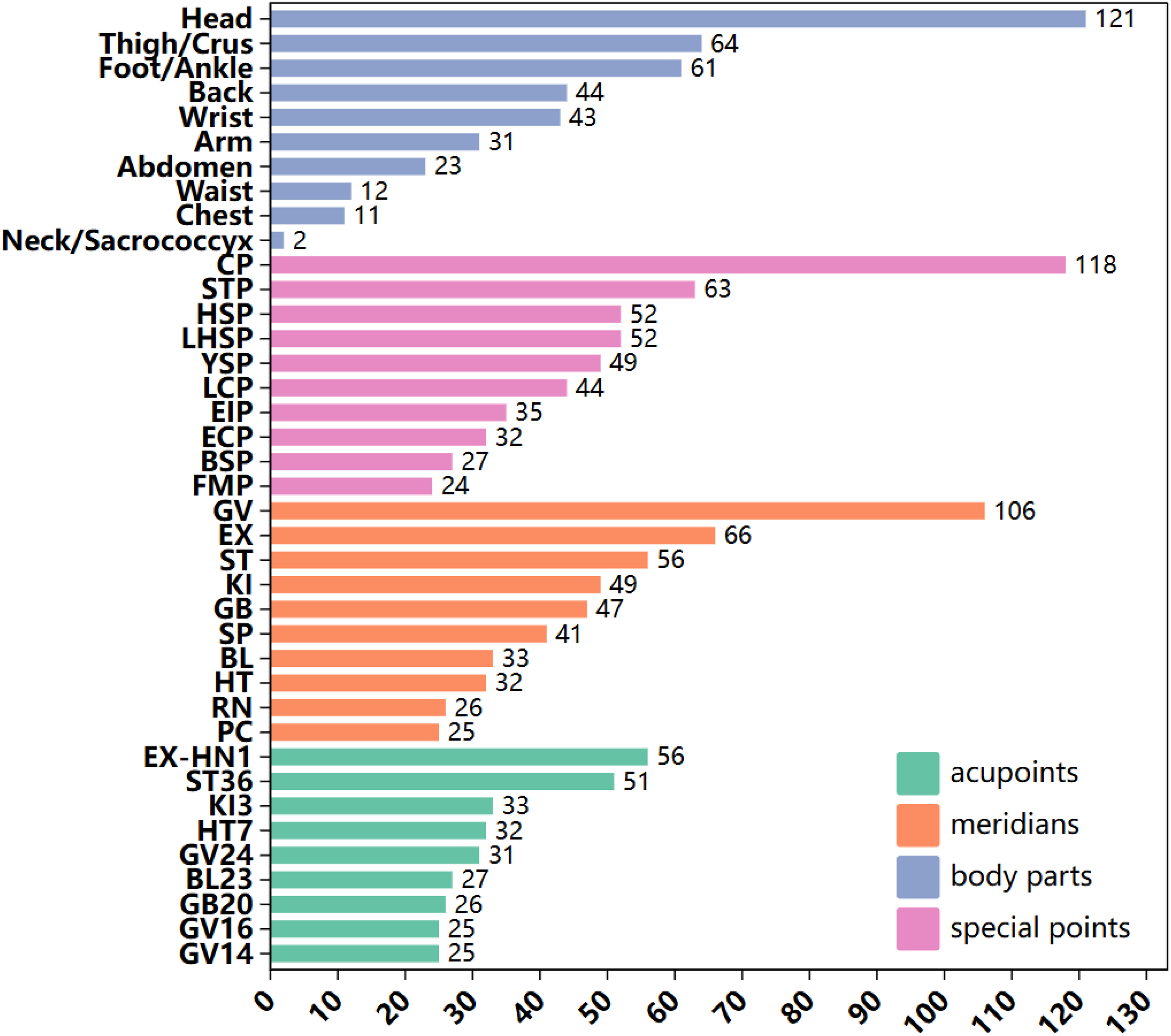
Summary of acupuncture programs. LU: Lung meridian of hand-taiyin; LI: Large intestine meridian of hand-yangming; ST: Stomach meridian of foot-yangming; SP: Spleen meridian of foot-taiyin; HT: Heart meridian of hand-shaoyin; SI: Small intestine meridian of hand-taiyang; BL: Bladder meridian of foot-taiyang; KI: Kidney meridian of foot-shaoyin; GB: Gallbladder meridian of foot-shaoyang; PC: Pericardium meridian of hand-jueyin; TE: Triple energizer meridian of hand-shaoyang; LR: Liver meridian of foot-jueyin; CV: Conception vessel; GV: Governor vessel; EX: Extra points; CP: Crossing points; LHSP: Lower he-sea points; XCP: Xi-cleft points; EIP: Eight influential points; ECP: Eight confluence points; FMP: Front-mu points; YSP: Yuan-source points; LCP: Luo-connecting points; JWP: Jing-well points; YS: Ying-spring points; STP: Shu-stream points; JRP: Jing-river points; HSP: He-sea points; BSP: Back-shu points.
Analysis of the association rule of the combinations of common acupoints/meridians/body parts/special points in the treatment of Alzheimer's disease with acupuncture.
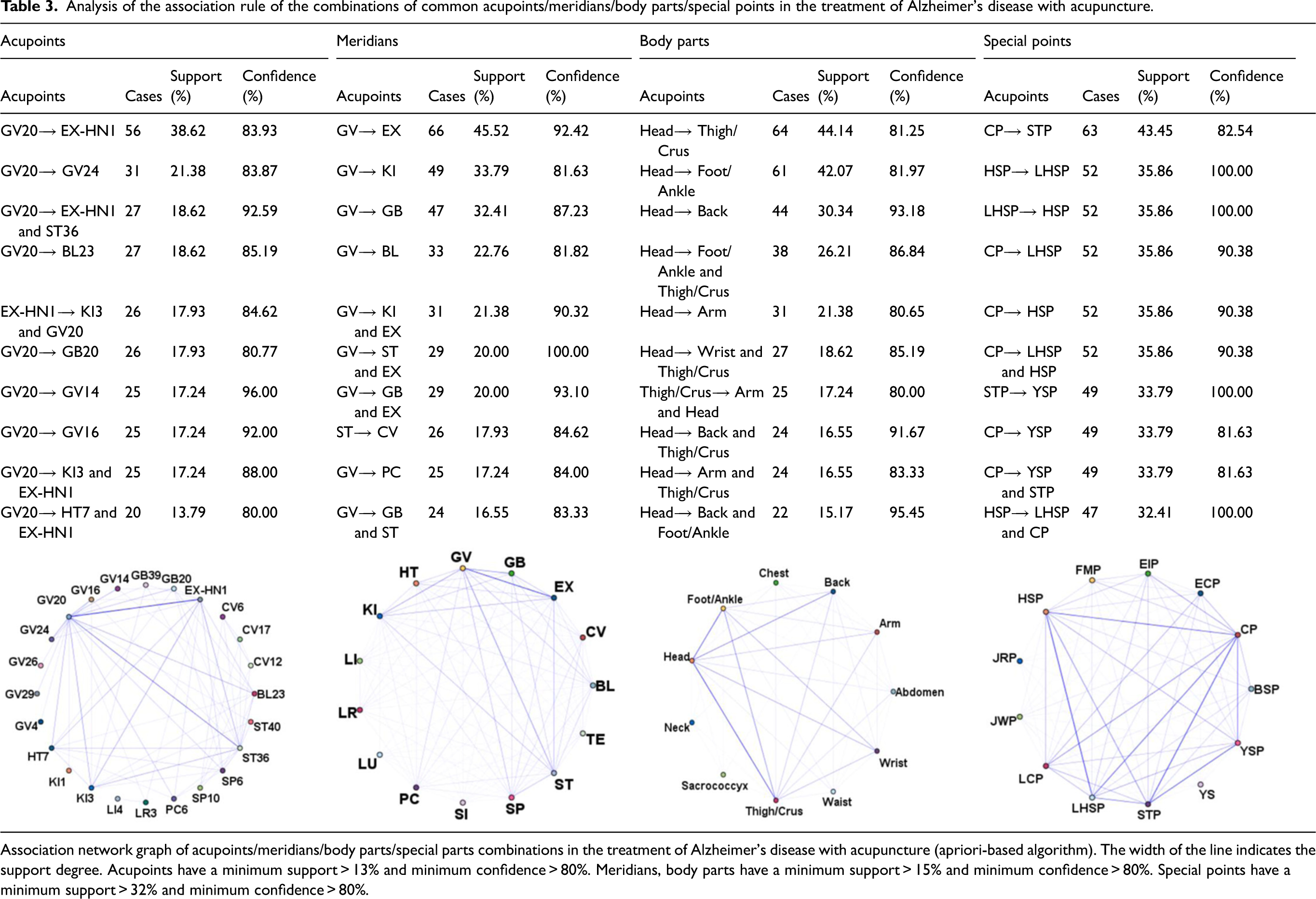
Association network graph of acupoints/meridians/body parts/special parts combinations in the treatment of Alzheimer's disease with acupuncture (apriori-based algorithm). The width of the line indicates the support degree. Acupoints have a minimum support > 13% and minimum confidence > 80%. Meridians, body parts have a minimum support > 15% and minimum confidence > 80%. Special points have a minimum support > 32% and minimum confidence > 80%.
Outcome characteristics
The clinical outcome indicators in the 117 RCTs primarily encompassed eight categories, as detailed in Figure 7(a). (1) Different scales were used to assess chief complaints by comparing improvements in memory and cognition. A total of 103 RCTs reported these indicators, totaling 170 frequencies. The Mini-Mental State Examination (MMSE), AD Assessment Scale-Cognitive Section (ADAS-Cog), and Montreal Cognitive Assessment (MoCA) were the scales most frequently used in these studies. (2) Various scales evaluated the accompanying symptoms, including sleep and emotions. Twelve RCTs reported such indicators, totaling 16 frequencies. These scales predominantly include the Pittsburgh Sleep Quality Index (PSQI) and the Hamilton Depression Scale (HAMD). (3) The quality of life scale was employed to assess health situation by scales such as the activity of daily living scale (ADL), Barthel Index, or modified Barthel Index (BI or mBI), etc. Sixty-five RCTs described such indicators, a total of 68 times. (4) TCM syndrome outcomes were evaluated in seven articles using dependency scales such as the TCM syndrome score, classification of dementia syndrome in traditional Chinese medicine (SDSD), and syndrome of the sea of marrow insufficiency score. (5) Objective metrics like laboratory, imaging, ultrasound, and electrophysiological examinations revealed that 48 of the 117 papers reported these indicators. Specific laboratory examinations were categorized into pathological factors, biological factors of neurological diseases, oxidative stress-related indicators, blood lipids, hemodynamic indicators, vascular-related factors, apoptosis-related factors, immune function indicators, and sleep and ageing factors (for details, see Supplemental File 4). Imaging examinations included functional magnetic resonance imaging (fMRI) and proton magnetic resonance spectroscopy (1HMRS). Ultrasound examinations included three-dimensional arterial spin labeling (3D ASL) and Transcranial Doppler (TCD). Electrophysiological examinations included electroencephalography (EEG), event-related potential (ERP), electromyography (EMG), or evoked potential. (6) Treatment effective rate: Seventy RCTs reported this rate. (7) Safety evaluation: The details of this item consisted of all uncomfortable symptoms and adverse reactions post-treatment, vital signs (heart rate and blood pressure), laboratory examinations (routine examinations of blood or urine, liver and kidney functions), and scales such as the Treatment Emergent Symptom Scale (TESS) and Rating Scale for Extrapyramidal Side Effects (RSESE). (8) Patient satisfaction: Only one RCT reported this item.

Outcome characteristics of the included RCTs. (a) Morus chart left represents eight categories; Morus chart right represents specific indicators under the categories. (b,c) Annual frequency analysis chart of the major evaluation indices of chief complaints, health situation, and objective metrics. Other indicators include different kinds, each appearing no more than three times. MMSE: Mini-Mental State Examination; ADAS-Cog: Alzheimer's Disease Assessment Scale-Cognitive Section; MoCA: Montreal Cognitive Assessment; HDS/HDS-R: Hasegama's Dementia Scale-Revision; NPI: Neuropsychiatric Inventory; BEHAV-AD: Behavioral Pathology in Alzheimer's Disease; CDR: Clinical Dementia Scale; DS: Digit span test; BPRS: Brief Psychiatric Rating Scale; GDS: Global Deterioration Scale; WMS: Wechsler Memory Scale; CGI: Clinical Global Impression Scales; AD-PES-11: Patterns and Elements of Alzheimer's Syndrome Scale; PSQI: Pittsburgh Sleep Quality Index; HAMD: Hamilton Depression Scale; CSDD: Cornell Scale for Depression in Dementia; SDS: Self-Rating Depression Scale; AIS: Abbreviated Injury Scale; ESS: Epworth Sleepiness Scale; ADL: Activities of Daily Living scale; BI/mBI: Barthel Index/ modified Barthel Index; FAQ: Functional Activities Questionnaire; BADL: Basic activity of daily living scale; QOL: quality of life; ADAS-ADL: Alzheimer's Disease Assessment Scale-Cognitive Section-Activities of Daily Living Scale; SDSD: Syndrome in Traditional Chinese Medicine; TCM: Traditional Chinese Medicine.
We further summarized the annual frequency analysis chart of the evaluation indices for chief complaints, health situation, and objective metrics. The frequency of MMSE, ADL, and laboratory examinations was high and increased year by year. Since 2008, ADAS-Cog, MoCA, and Neuropsychiatric Inventory (NPI) have been introduced successively. Since 2014, BI/MBI and electrophysiologic examinations have emerged. From 2018 onwards, the frequency of ultrasound examination has increased (Figure 7(b) and (c)). More details on the outcome characteristics are provided in Supplemental File 4.
Risk of bias assessment
We assessed the risk of bias using the Cochrane risk-of-bias tool (Figure 8). It can be seen that a few studies reported the allocation concealment methods and blinding, indicating the quality of included studies was generally low.
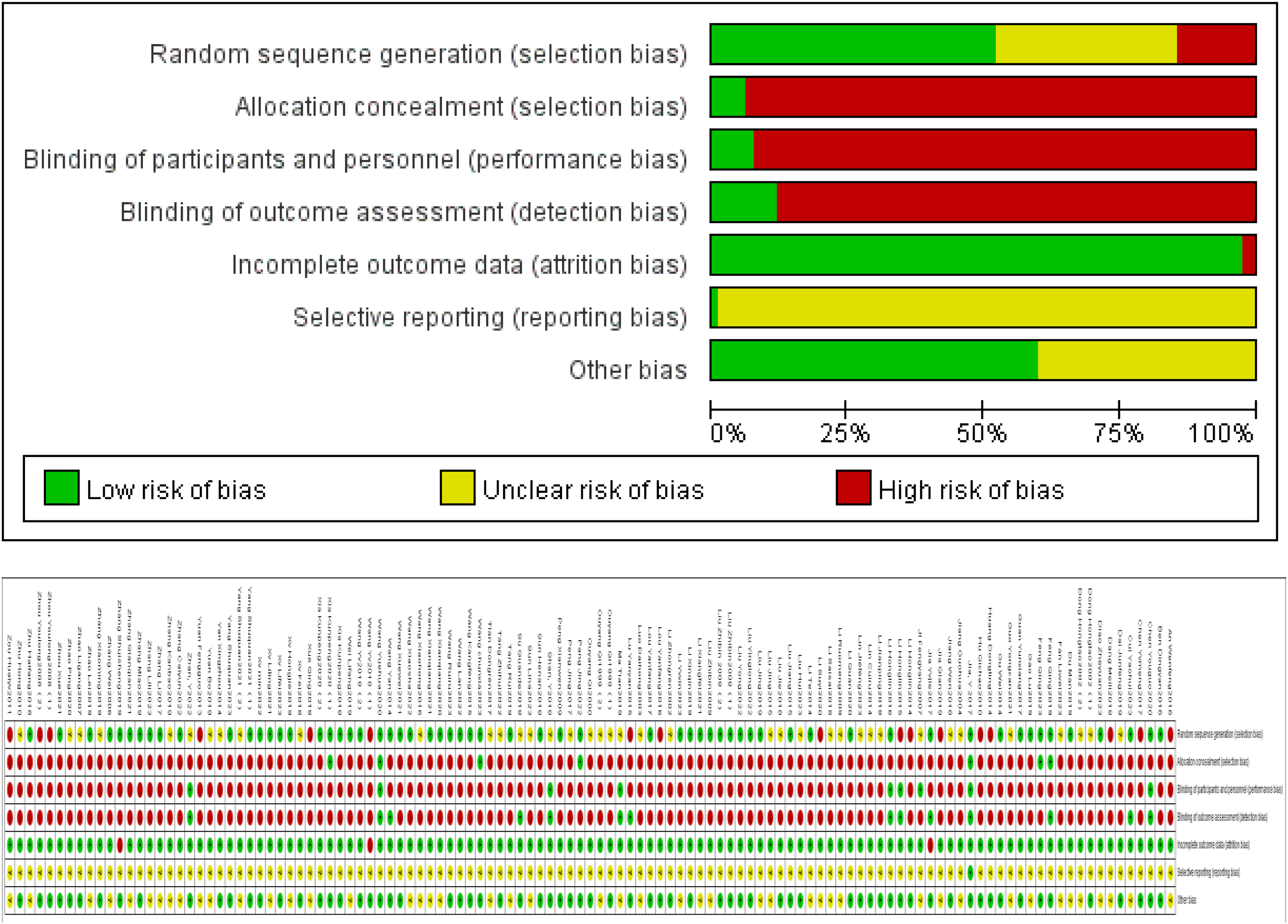
Cochrane bias risk analysis diagram.
Srs and MAs-related characteristics of the included studies
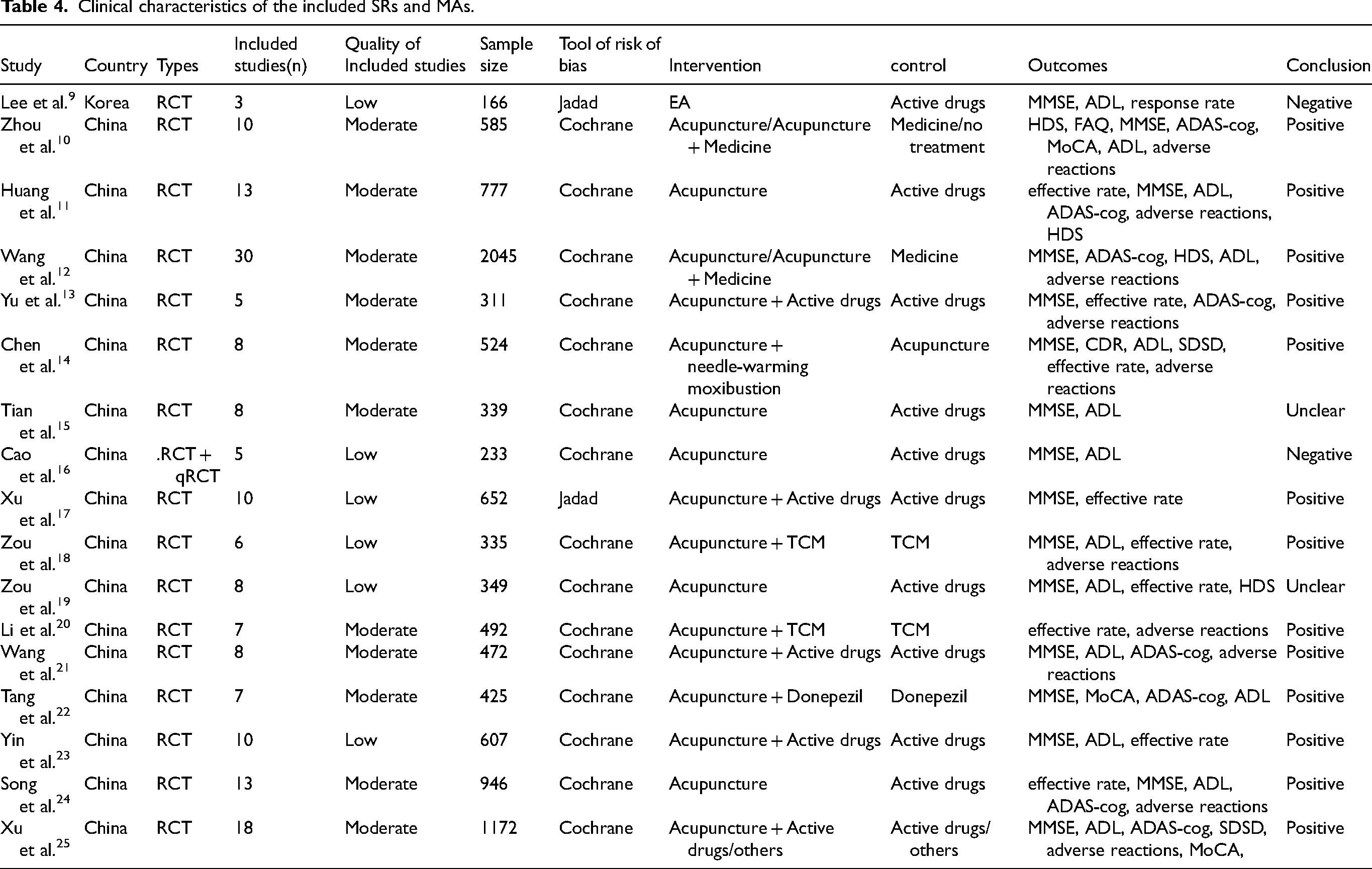
SRs and MAs’ clinical characteristics. The SRs and MAs included in this analysis were published between 2009 and 2023 and were all RCTs. The number of studies conducted per year varied from 3 to 30, and the average number of articles included was 9.94. The total sample size ranged from 166 to 2,045, with a mean of 613.53. The quality of the trials was assessed using the Jadad score system (2/17 [11.76%]) and the Cochrane risk bias tool (15/17 [88.24%]). The RCT quality was moderate (11/17 [64.71%]) or low (6/17 [35.29%]). The interventions in the experimental group included acupuncture, acupuncture combined with active drugs, acupuncture combined with Chinese medicine, or acupuncture combined with other therapies. The control group received active drugs, Chinese medicine, or other therapies. The most frequently reported outcomes in SRs and MAs were the MMSE score (16/17 [94.12%]) and ADL score (14/17 [82.35%]), with adverse events reported in 10/17 (58.82%) SRs and MAs (Table 4).
Clinical characteristics of the included SRs and MAs.
Quality assessment of the SRs and MAs. Most SRs and MAs were positive (13/17 [76.48%]), suggesting the effectiveness of acupuncture intervention. Assessment according to AMSTAR 2, among the 17 included SRs and MAs, seven had moderate methodological quality, seven had low methodological quality, and three had critically low methodological quality (Figure 9).
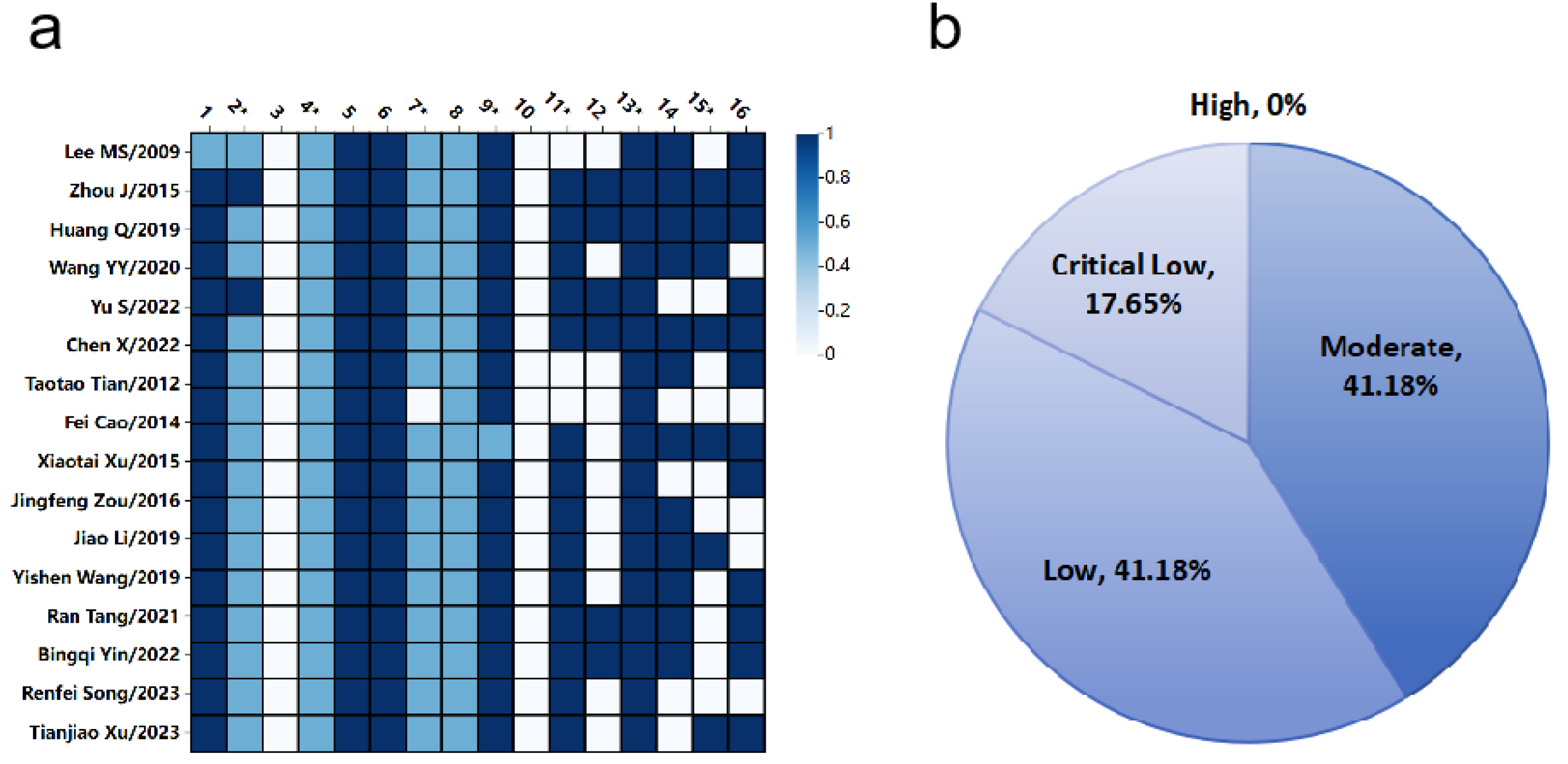
Quality assessment of the SRs and MAs.
Research problems and research gaps suggested by SRs and MAs
We summarized the evidence gaps in the SRs and MAs and classified them as follows: methodological (risk of bias, report quality, sample size) and clinical evidence gaps (population, acupuncture intervention, control group, outcome indicators, time point, and setting). The categories and frequencies are presented in Figure 10.
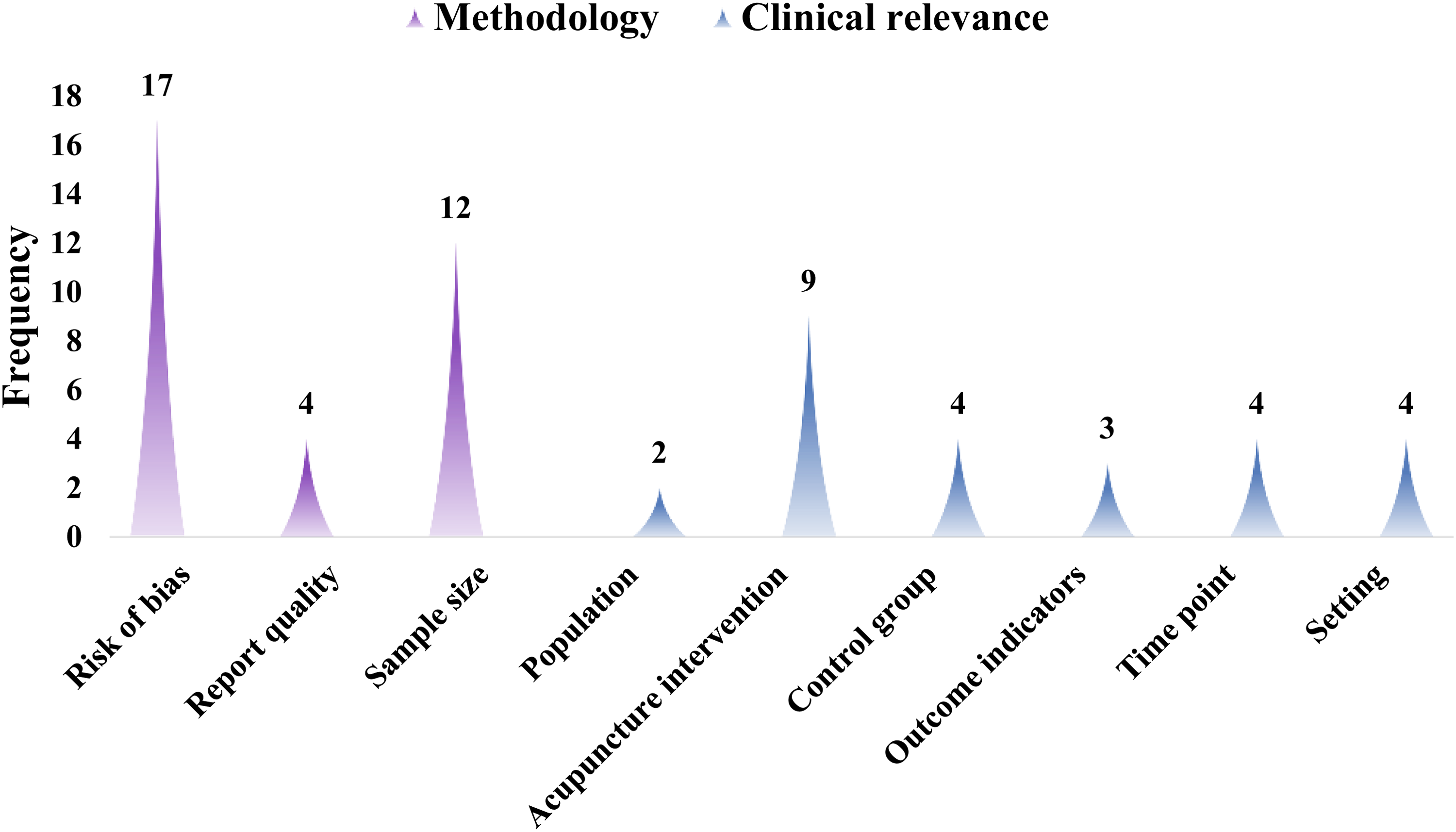
Research problems and research gaps suggested by SRs and MAs.
The ordinate of Figure 9 represents articles and the abscissa represents the 16 items of AMSTAR 2. 1-0.5-0 represented three evaluation options: yes, no, and partial yes.
Acupuncture for improvement in BPSD
Based on the above outcomes of RCTs and SRs/MAs, we found that there is a current lack of focus on acupuncture's impact on behavioral and psychological symptoms of dementia (BPSD). Based on this gap, we concentrated on acupuncture for improvement in BPSD. The severity of BPSD symptoms, reported as Behavioral Pathology in the BEHAVE-AD, NPI, and Brief Psychiatric Rating Scale (BPRS) were considered the primary outcomes. Finally, nine relevant articles were selected (Table 5).
Basic characteristics and quality of the literature in acupuncture with BPSD of AD.
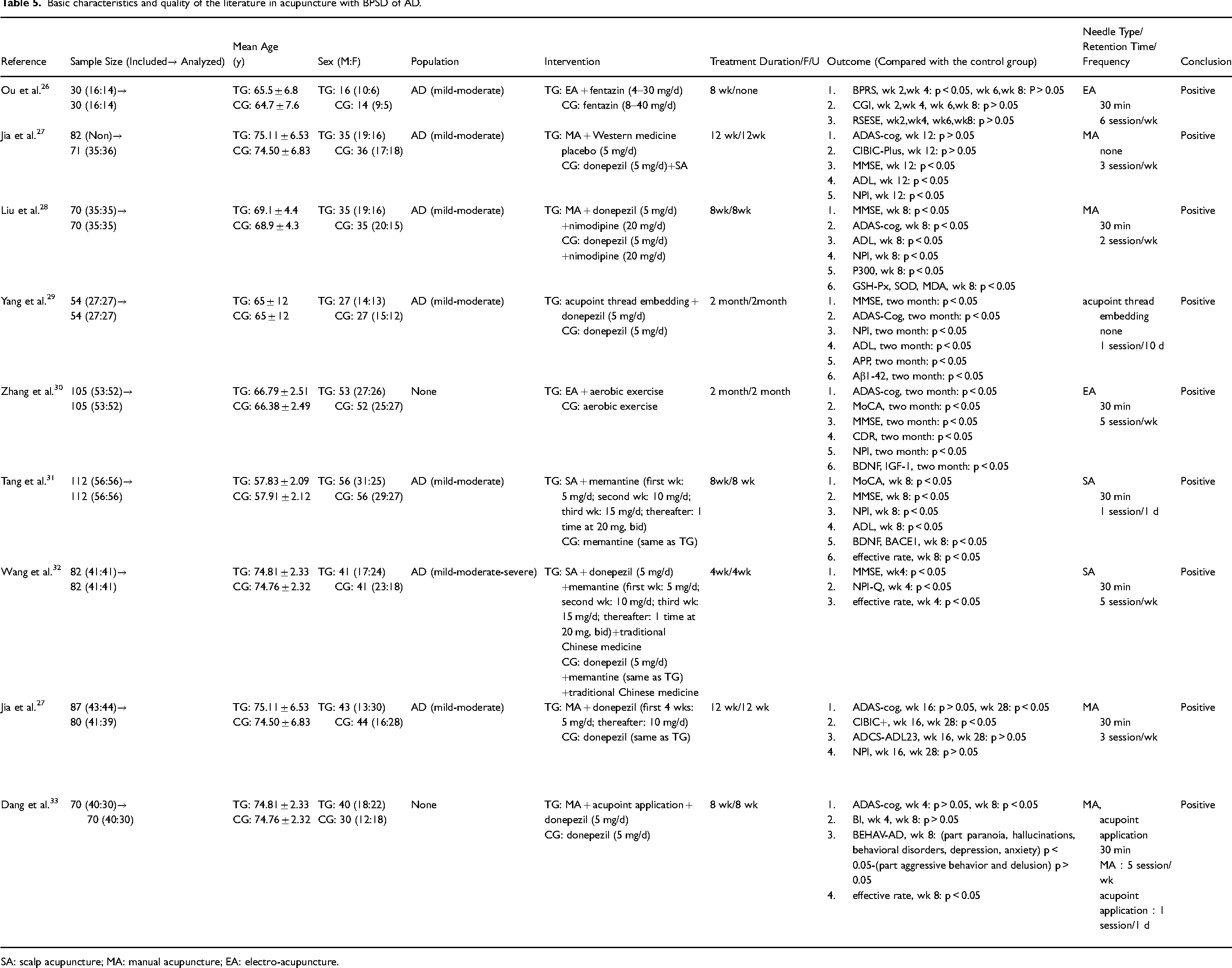
SA: scalp acupuncture; MA: manual acupuncture; EA: electro-acupuncture.
Sample sizes varied from 30 to 112 patients. The study was mainly performed on mild-moderate AD cases. In the nine RCTs, six compared acupuncture combined with anti-dementia drugs to anti-dementia drugs alone. One RCT compared acupuncture combined with aerobic exercise to aerobic exercise alone, another compared acupuncture combined with an anti-dementia placebo to sham acupuncture combined with anti-dementia drugs, and one compared acupuncture combined with anti-dementia drugs plus TCM to anti-dementia drugs plus TCM. Only one RCT included a follow-up assessment after completion. The treatment duration varied from 4 to 12 weeks, with 8 weeks being the most frequently observed period among the RCTs. The conclusions were mostly positive.
Discussion
An increasing research and development trend
The number of scholarly articles can reflect the current state of research in a specific field and offer insights into future trends. Recent studies have demonstrated a notable increase in research output over the last decade, peaking in 2019. Subsequently, there was a decrease in research output, potentially attributable to the COVID-19 outbreak, followed by a gradual resurgence in 2023. AD is a neurological condition characterized by a progressive cognitive decline as its primary clinical feature. It contributes significantly to the prevalence of dementia and imposes a substantial burden on affected individuals and society. It is increasingly acknowledged that a protracted pathophysiological progression commences years prior to the onset of symptoms and persists for years after that. 34 Currently approved pharmacological treatments for AD, such as acetylcholinesterase inhibitors and N-methyl-D-aspartate receptor (NMDAR) antagonists, aim to ameliorate clinical symptoms and functional impairment. 35 Consequently, there is a growing demand for effective interventions. Acupuncture is receiving increasing attention as an alternative therapeutic strategy. However, all the RCTs were conducted in China. Except for China, only Korea released its MAs and SRs. This indicates that international attention paid to acupuncture for AD is insufficient.
The methodological quality of the included studies needs to be further improved
We used the Cochrane risk-of-bias tool for the quality assessment of 117 RCTs and the AMSTAR 2 tool to assess the methodological quality of the included SRs and MAs. We summarized the study questions and gaps in current studies.
All existing RCTs showed relatively low methodological quality, mainly manifested as: (1) Risk of bias: Random sequence generation and allocation concealment is poorly described; specific blinding methods are not mentioned, and there are many barriers to implementing blinding, potential publication bias. (2) Sample size: The sample size of the RCTs was small, and most studies did not specify an estimation method for the sample size. (3) Report quality: Most studies did not describe patient loss, loss to follow-up, or how to handle them; some reports had incomplete information. Therefore, reporting is recommended strictly per the Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) guidelines. 36
Our research also indicates that the methodological quality of the studies included in the SRs and MAs was subpar. This can be attributed to the non-standardized implementation and reporting of SRs and MAs. Additionally, the methodological quality of the original RCTs was not high, contributing to the overall low level of evidence in SRs and MAs. Future studies should focus on improving the quality of RCTs to enhance the quality of acupuncture RCT reports for AD.
Gaps in clinically relevant evidence require urgent attention
Included populations. The existing evidence suggests that the different disease degrees, different Western medicine diagnostic criteria among patients with AD, and poor integration of Chinese and Western medicine diagnostic reference criteria varied between studies; these are issues that need attention.
According to literature mentioning the degree of disease, the majority of patients with AD exhibited mild to moderate disease severity. Thus, ongoing clinical RCTs on acupuncture intervention in AD primarily focus on the evaluation of patients with mild to moderate symptoms. 37 Researchers utilized the CDR to assess and monitor the severity of dementia while excluding cases of vascular dementia through the Hachinski Ischemic Score. These findings serve as a foundation for future research on selecting the diagnostic criteria for AD.
Of the 14 Western medicine diagnostic criteria mentioned, the 1984 American Society of Neurology, Language Disorder, and Stroke-The Alzheimer's Disease and Related Diseases Working Group criteria (NINCDS-ADRDA), Diagnostic and Statistical Manual of Mental Disorders IV and IV-R criteria (DSM-IV and DSM-IV-R), and the 2011 National Institute on Aging and Alzheimer's Association criteria (NIA-AA) for AD were identified as the primary diagnostic tools in this literature review, aligning with findings from previous studies. 1 Guidelines also support the use of diagnostic criteria from the 1984 NINCDS-ADRDA or the 2011 NIA-AA for the clinical diagnosis of AD. 38 The NINCDS-ADRDA criteria were the first internationally recognized standards for diagnosing AD. In contrast, the NIA-AA guidelines divide the course of AD into three stages: the preclinical stage of AD, AD-derived MCI, and AD dementia.
Acupuncture, as a component of TCM, requires the inclusion of the TCM diagnostic criteria in clinical studies. Only 31 articles incorporated these criteria, with the Guiding Principles of Clinical Research on New Drugs of Chinese Medicines (GPCRNDCM) and the Assessment Criteria for the Diagnosis, Dialectic, and Curative Effects of Dementia (ACDDCED) being the most prevalent. Future research should prioritize incorporating TCM diagnostic criteria and the documentation of TCM diagnosis and treatment details to enhance the TCM characteristics of our studies.
Acupuncture intervention and control. The predominant forms of acupuncture therapy include manual acupuncture and EA. The treatment course, duration, and techniques employed in the acupuncture practice exhibited subjectivity and flexibility. Consequently, it is imperative to maintain strict control of the intervention process.
Regarding the control group, we found a lack of sham or placebo acupuncture settings. This would increase the placebo effect in the intervention group, especially since the Chinese usually have high expectations for acupuncture, which may exaggerate the treatment outcome of combination therapy. Most Western medicines used in the control group were donepezil, nimodipine, and memantine hydrochloride tablets. There is no unified standard, thus showing selection bias and certain differences in the course of treatment.
Association rules of acupuncture point prescription
According to the results of the literature mining, the most frequently targeted acupoints included GV20, EX-HN1, ST36, KI3, HT7, and GV24. The primary meridians used were the GV, ST, and EX. The most strongly supported associations between the acupoints were GV20, EX-HN1, GV20, GV24, GV20, EX-HN1, and ST36. Similarly, the most strongly supported associations between meridians are GV
Selection of the outcome indicators
Outcome indicators play crucial roles in assessing the efficacy of clinical research interventions. The rationality, objectivity, and standardization of these indicators directly affect the evaluation of intervention measures, ultimately influencing treatment decisions in clinical practice. This study observed a predominant focus on cognitive function improvement, health status, overall quality of life, and response rate in current clinical studies on acupuncture in AD. These were observed in the RCTs, MAs, and SRs. Acupuncture has a comprehensive regulatory effect on both physical and mental health. Therefore, researchers prefer to consider the outcome indicators of the overall quality of life; thus, the advantages of acupuncture treatment can be displayed in a multi-angle, all-round manner. Clinical response rate as a primary outcome measure in studies is discouraged because of potential inconsistencies in defining the criteria across different research studies.
Second, acupuncture pays insufficient attention to TCM syndromes, and only seven RCTs have reported such indicators, which have not yet reflected the TCM characteristics of acupuncture for AD. This aspect should receive more attention in future studies. Learning TCM treatments can be more justified by focusing on changes and improvements in TCM syndrome. Moreover, identifying specific targets for enhancing TCM treatment can establish a TCM foundation for developing relevant diagnostic and treatment guidelines, ultimately facilitating a more cohesive integration with modern medicine.
Acupuncture is an invasive procedure, so a thorough evaluation of its safety for clinical use is necessary. Some studies did not describe the adverse effects, and their safety could not be evaluated. However, only 23 RCTs focused on the acupuncture treatment of AD reported adverse events. Researchers have overlooked these concerns owing to the low incidence of adverse events. Hence, further research is required to enhance the understanding of adverse events associated with acupuncture. Only one RCT examined patient expectations and satisfaction, whereas no RCT assessed health-economic indicators, indicating a lack of attention to these important factors.
As an outcome indicator, scales can be too subjective, less accurate, and sensitive, making the data difficult to save and not accurately reflect the true effect of acupuncture treatment. Therefore, objective indicators have gradually emerged, with laboratory tests introduced in 2006, imaging tests in 2008, electrophysiological tests in 2014, and ultrasound tests in 2018. It is important to note that advanced techniques are gradually being widely used to evaluate and study the mechanisms of acupuncture treatment for AD. In particular, fMRI, EEG or ERP, and TCD represent imaging modalities that offer novel avenues for investigating the mechanisms underlying acupuncture treatment for AD in a dynamic, visual, and objective manner. 42 These approaches hold promise for inspiring researchers to evaluate the clinical efficacy of acupuncture through sophisticated technical methodologies and engage in unremitting explorations.
Time points of measurement and follow-up
Regarding measurement time, most studies did not describe follow-up or evaluate long-term efficacy. In terms of research sites, there was a lack of multi-center RCT trials, and most studies were completed in China.
This study has some limitations. Firstly, all included RCTs were conducted in China, with only one meta-analysis and systematic review from Korea, indicating limited international representation and applicability. While the majority of studies included in the analysis reported positive outcomes, the methodological quality of the RCTs was generally low, with issues such as poorly described random sequence generation, allocation concealment, and blinding, as well as potential publication bias. The sample sizes were often small, and many studies did not specify the estimation method for sample sizes or adequately report patient loss or follow-up details, or describe how such data was handled. Additionally, there was a lack of sham or placebo acupuncture settings in control groups, which could lead to an exaggerated placebo effect due to high expectations from acupuncture. The outcome measures also had limitations, including insufficient attention to TCM syndromes, adverse events, patient expectations, and health-economic indicators. The scales used were often subjective and less sensitive. Meanwhile, we found that the clinical focus on psychobehavioral symptoms in patients with AD is still insufficient. More RCTs, SRs, and MAs should focus on analyzing psychobehavioral symptoms in the future. Furthermore, many studies did not describe follow-up periods or evaluate long-term efficacy. There was also a lack of multicenter trials, with most studies being completed in China. Finally, the study noted the gradual introduction of advanced techniques like imaging, electrophysiology, and ultrasound, but these methods are not yet widely adopted or standardized in evaluating acupuncture for AD. Consequently, additional research is necessary to strengthen the validity of the findings of this study.
Despite these limitations, current evidence suggests that acupuncture may be a useful alternative therapy for AD-type dementia, especially in improving the cognitive and functional abilities of patients with AD. This is the first evidence map exploring acupuncture treatment for AD. This study addresses critical gaps in the existing literature on acupuncture as a treatment for AD and proposes methodological improvements for future research. This study enhances the scientific understanding and clinical application of acupuncture in managing AD, thereby contributing valuable insights to scholars in the field.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241295400 - Supplemental material for Acupuncture for patients with Alzheimer's disease: An evidence map of randomized controlled trials, systematic reviews, and meta-analysis
Supplemental material, sj-docx-1-alz-10.1177_13872877241295400 for Acupuncture for patients with Alzheimer's disease: An evidence map of randomized controlled trials, systematic reviews, and meta-analysis by Chao Ke, Shengtao Shan, Juli Yu, Xin Wei, Jiang Pan and Wei Zhang in Journal of Alzheimer's Disease
Supplemental Material
sj-docx-2-alz-10.1177_13872877241295400 - Supplemental material for Acupuncture for patients with Alzheimer's disease: An evidence map of randomized controlled trials, systematic reviews, and meta-analysis
Supplemental material, sj-docx-2-alz-10.1177_13872877241295400 for Acupuncture for patients with Alzheimer's disease: An evidence map of randomized controlled trials, systematic reviews, and meta-analysis by Chao Ke, Shengtao Shan, Juli Yu, Xin Wei, Jiang Pan and Wei Zhang in Journal of Alzheimer's Disease
Supplemental Material
sj-docx-3-alz-10.1177_13872877241295400 - Supplemental material for Acupuncture for patients with Alzheimer's disease: An evidence map of randomized controlled trials, systematic reviews, and meta-analysis
Supplemental material, sj-docx-3-alz-10.1177_13872877241295400 for Acupuncture for patients with Alzheimer's disease: An evidence map of randomized controlled trials, systematic reviews, and meta-analysis by Chao Ke, Shengtao Shan, Juli Yu, Xin Wei, Jiang Pan and Wei Zhang in Journal of Alzheimer's Disease
Supplemental Material
sj-docx-4-alz-10.1177_13872877241295400 - Supplemental material for Acupuncture for patients with Alzheimer's disease: An evidence map of randomized controlled trials, systematic reviews, and meta-analysis
Supplemental material, sj-docx-4-alz-10.1177_13872877241295400 for Acupuncture for patients with Alzheimer's disease: An evidence map of randomized controlled trials, systematic reviews, and meta-analysis by Chao Ke, Shengtao Shan, Juli Yu, Xin Wei, Jiang Pan and Wei Zhang in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
Author contributions
Chao Ke (Conceptualization; Data curation; Funding acquisition; Writing – original draft; Writing – review & editing); Shengtao Shan (Conceptualization; Data curation; Writing – original draft; Writing – review & editing); Juli Yu (Conceptualization; Validation); Xin Wei (Conceptualization; Validation); Jiang Pan (Writing – review & editing); Wei Zhang (Conceptualization; Funding acquisition; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Program of National Natural Science Foundation of China (81973956), Youth Project of National Natural Science Foundation of China (82405580), Natural Science Foundation of Changsha (kq2403097), the General Project of the Hunan Provincial Health Commission (W20243005), and the Key Project of the School and Hospital with Hunan University of Traditional Chinese Medicine Scientific Research Fund (czkt-2024004).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data generated or analyzed during this study are included in this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.