
Abstract
Background
Documented risk factors and prodromal features of dementia in primary care practices may support dementia prevention and early detection in routine care.
Objective
To identify documented prodromal features and risk factors of dementia before the incident dementia diagnosis in German primary care practices.
Methods
This case-control study used documented diagnoses (risk factors, prodromal features) and prescriptions of primary care practices for 73,717 patients with dementia disease and 73,717 matched controls (ratio 1:1). Logistic regression models were used to assess the associations between these documentations and the development of dementia diseases within 12 (1 year), 12–60 (1–5 years), and 60–120 months (5–10 years) before the incident dementia diagnosis.
Results
Mild cognitive impairment, depression, symptoms involving the emotional state, dizziness, and age-related physical debility were documented prodromal features associated with developing dementia diagnosis across all periods. Difficulties in gait and mobility and conduct disorders occurred significantly more often five years before the diagnosis. In terms of documented risk factors, hearing loss, visual disturbances, diabetes mellitus, and cerebrovascular diseases were associated with dementia across all periods. Mental and behavioral disorders due to the use of alcohol, intracranial injury, Parkinson's disease, chronic fatigue, intellectual disabilities, pneumonia, and epilepsy were also more often documented 60 months before the diagnosis.
Conclusions
Next to mild cognitive deficits, several factors, such as disorders of conduct and emotions, gait, mobility, and mental health, can be identified and monitored in primary care practices, helping physicians focus on potential consequences for cognitive decline and subsequent dementia.
Introduction
The worldwide number of people living with dementia (PlwD) will continue to increase to 78 million by 2030 as mortality at younger ages declines, posing a tremendous societal and economic challenge.1,2 Therefore, the World Alzheimer Report in 2023 started the campaign ‘Never too early, never too late’, underscoring the pivotal role of identifying prodromal symptoms and risk factors and proactive adopting risk reduction initiatives to delay and potentially even prevent the onset of dementia diseases. 3
There is evidence that the underlying diseases start many years before the first symptoms of dementia. 4 Such prodromal features refer to early signs and symptoms that precede the full manifestation of the dementia disease. In addition, several risk factors exist, defined as conditions or characteristics that increase the likelihood of developing dementia diseases. 4 The age-specific incidence has fallen in many countries, probably due to healthier lifestyles and improved education, nutrition, and health care. 5 However, the global demographic changes will increase the number of PlwD. Therefore, it is vital to understand, identify and respond to these prodromal features and risk factors.
Based on a growing body of evidence, the Lancet Commission on dementia prevention, intervention, and care published nine potentially modifiable risk factors for dementia in 2017: less education, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, and low social contact. 6 In 2020, the Commission added excessive alcohol consumption, traumatic brain injury, and air pollution, yielding 12 risk factors that account for around 40% of worldwide dementias that are theoretically preventable; 7 60% of risk factors are non-modifiable, like genetic risk, or unknown. A large body of evidence confirms the factors of the Lancet Commission8–14 and further prodromal features and factors carrying a relevant risk for developing dementia disorders.4,15,16
Most of these risk factors and prodromal features have been identified from epidemiological data and specialized cohort studies. In contrast, risk factors and prodromal features based on primary care data documented by physicians have found less attention so far. Studies identified agitation, anxiety, hallucinations, aberrant motor behavior, intracranial injury, diabetes, lipid metabolism, stroke, Parkinson's disease, intracranial injury, coronary heart disease, mild cognitive impairment (MCI), mental and behavioral disorders due to alcohol use, neuropsychiatric symptoms, seizures, hypertension, dyslipidemia obesity, and sleep disorder as documented risk factors that are associated with a documented dementia diseases later on in primary care.17–19 Therefore, primary care is essential for identifying possible dementia risk factors and prodromal features documentation in senior people who present to primary care physicians with any health concern, which would be essential to reduce the diagnostic delay by guiding general practitioners in early detection and referrals to specialists.
Also of particular interest is the timing of documented risk factors, some of which do not always carry the same risk. For example, midlife obesity is a risk factor for dementia. However, obesity later in life may rather be protective.10,20–22 Therefore, consecutive cascades of risk factors or prodromal features documentation and combinations of risk factors and prodromal features documentation over different periods can facilitate and support the early identification of risk factors and prevention of dementia diseases in primary care practices.
As a prerequisite, it is crucial to determine if established prodromal symptoms and risk factors are documented in routine care practice over time, allowing primary care physicians to oversee time-specific patient pathways that may lead to dementia later on. However, evidence about the interaction of documented risk factors and prodromal features with a documented dementia diagnosis over different time windows is limited, especially in primary care data.
Here, we studied the prevalence of documented risk factors and prodromal symptoms derived from secondary data from primary care practices at specific time windows before the index date of a dementia diagnosis, following a timing approach previously applied to Parkinson's disease. 23 We evaluated a wide range of known comorbidities and medications as documented risk factors or prodromal features, looking at ten, five, and one year before dementia diagnosis. This evidence will generate but not confirm hypotheses on associated factors, as they are based on secondary data from primary care practices. However, healthcare providers and decision-makers can be informed about different time windows for documented prodromal features and risk factors of patients developing dementia diseases in primary care, contributing to individualized and time-specific therapies and prevention strategies.
Methods
Study design
This case-control study used the Disease Analyzer database (IQVIA) in Germany, containing demographic, diagnosis, and prescription data from more than 6 million patients between 2015 and 2022 obtained in anonymized format from general practices in Germany. The Disease Analyzer database has been described in detail elsewhere. 24 Diagnoses were coded using the German adaptation of the International Classification of Diseases, tenth revision (ICD-10), and prescriptionms using the Anatomical Classification of Pharmaceutical Products of the European Pharmaceutical Marketing Research Association (EphMRA).
Several variables (e.g., age of physician, specialty, community size category, and German federal state) were used to select the panel of practices for this analysis. The Disease Analyzer database includes approximately 3% (1284 general practitioner practices) of German general practices 24 and was previously used for several epidemiological studies on dementia diseases. 25
Retrospective anonymized data of routine care practice usage for scientific research in Germany is regulated by the Code of Social Law (Sozialgesetzbuch, SGB V). Ethical approval and informed consent from PlwD are not required for these routinely collected pseudonymized data. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. 26
Study population
We identified all patients aged 60 years or older who received a first dementia diagnosis between January 1, 2015, and December 31, 2022 (index date). Incident dementia diagnosis was defined as the presence of the ICD-10 codes F01, F03, and G30 without a previous dementia diagnosis in the preceding ten years. Patients had to be registered for at least 12 months before the index date to be included to avoid including patients with existing dementia diagnoses. Individuals without dementia (“non-demented controls”) were matched (1:1) to those with dementia by sex, age and pre-observation time (at least one, at least five and at least ten years). In patients without dementia, the index date corresponded to a randomly selected visit date between January 2015 and December 2022. The participant flow and study selection process is demonstrated in Figure 1.
Prodromal features, risk factors, comorbidities, and medications
Prodromal features, comorbidities, risk factors and medications coded or prescribed by general practitioners with a potential association with subsequent diagnosis of dementia were identified based on a narrative review of the literature (PubMed, Google Scholar). Extracted findings were finally discussed with experts in dementia research and care, resulting in a list of all prodromal features, risk factors, and medications shown in Supplemental Table 1.
We recorded the occurrence of listed diagnoses, medications and symptoms previously reported to be associated with later diagnosis of dementia disease before the index date in patients with and without dementia. Associations of prodromal features, risk factors and medications were presented separately for the following three periods: (i) less than 12 months before the index date, (ii) more than 12 but less than 60 months (5 years) before the index date, and (iii) more than 60 months (5 years) but less than 120 months (10 years) before the index date. For each analysis, only patients with an appropriate pre-observation time were included, i.e., at least one year, five years and ten years pre-observation time.
Statistical analysis
The prevalence of prodromal features, risk factors and medication intake are presented descriptively using percentage values.
Odds ratios (ORs) were calculated for prodromal features, risk factors and medications, demonstrating the association with developing dementia diseases separately (one model for each period with all factors) for (i) one year before the index date (period 1) and (ii) pooled for the periods 12 months to 5 years (period 2) and (iii) five to ten years (period 3) before the index data. The 95% confidence intervals (CIs) were calculated using the method by Altmann (46) with conservative Bonferroni adjustment for multiple comparisons. Therefore, based on the inclusion of 59 prodromal features, risk factors or medications, a p-value of less than 0.001 (≤0.001; 0.05/59≈0.001) was considered statistically significant to reduce the risk of error due to multiple comparisons. Therefore, even though the 95% CI of the OR did not overlap with the null value (e.g., OR = 1.0), this was considered non-significant when the p-value was higher than 0.001. Due to the multicollinearity between specific diseases and medications, like hypertension and antihypertensive drugs, sensitivity analyses without drug therapies were conducted within a sensitivity analysis.
Also, we used the lift value (percentage lift) to compare these prevalences between patients with and without dementia, expressing the relative difference between the two percentage prevalences. A lift value of 2.0 demonstrates that a factor is two times more prevalent in PlwD (for example, 20% versus 10%).
Statistical analyses were performed using SAS, version 9.4 (SAS Institute).
Results
Study population
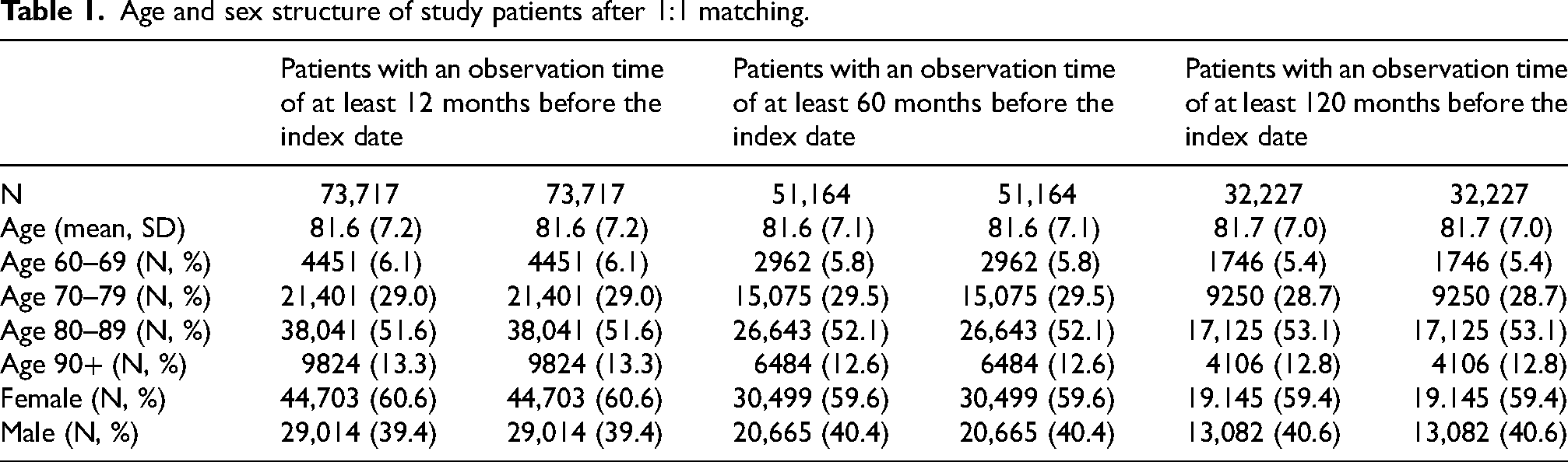
A total of 73,717 patients with incident dementia (mean [SD] age, 81.6 [7.2] years; 44,704 female [60.6%]; 29,014 male [39.4%]) and 73,717 matched controls with the same age and sex characteristics and distribution were included. The longer the observation, the lower the number of patients included (n = 73,717 for 0–12 months, 51,164 for 12–60 months, and 32,227 for 60–120 months before the incident dementia diagnosis). Study populations are described in Table 1.
Age and sex structure of study patients after 1:1 matching.
Prodromal features
Odds ratios for prodromal features were highest at 12 months and lowest 60 to 120 months before the index date. There were significant positive associations for all three observation periods (0–12 months; 12–60 months; 60–120 months) with a subsequent dementia diagnosis for mild cognitive impairment (OR 4.46, 95% CI [4.10–4.86]; 3.41 [3.14–3.7]; 3.07 [2.6–3.62]), depression (1.54 [1.47–1.61], 1.48 [1.42–1.55]; 1.32 [1.25–1.4]), symptoms and signs involving emotional state (1.89 [1.74–2.04]; 1.41 [1.31–1.52]); 1.29 [1.17–1.42]), dizziness (1.29 [1.23–1.36]; 1.24 [1.19–1.29]; 1.15 [1.09–1.22]), and age-related physical debility (1.46 [1.38–1.55]; 1.23 [1.17–1.29]; 1.27 [1.16–1.39]).
Also, the following significant positive associations occurred within 12 months and 12 to 60 months before diagnosis, but not within 60 to 120 months before the index date: anxiety (0–12 months: 1.3 [1.21–1.41]; 12–60 months: 1.26 [1.17–1.35]; 60–120 months: 1.11 [1.02–1.22]), delirium (4.57 [3.46–6.02]; 2.42 [1.7–3.44]; 2.05 [0.72–5.83]), personality and behavioral disorders (3.92 [2.49–6.16)]; 1.97 [1.34–2.91]; 1.18 [0.75–1.87]), abnormalities of gait and mobility (1.5 [1.43–1.58]; 1.29 [1.23–1.35]; 1.38 [1.25–1.52]), injuries to arm, hand, feet, hip and foot (1.29 [1.24–1.35]; 1.18 [1.14–1.23]; 1.08 [1.02–1.13]), other symptoms and signs involving general sensations and perceptions (2.99 [2.32–3.86]; 1.55 [1.14–2.09]; 1.35 [0.70–2.63]), unspecified pain (1.13 [1.09–1.18]; 1.17 [1.12–1.22]; 1.05 [0.99–1.11]), constipation (1.17 [1.11–1.24]; 1.28 [1.22–1.36]; 1.11 [1.03–1.21]), and neuromuscular dysfunction of bladder (1.62 [1.29–2.03]; 1.52 [1.26–1.84]; 1.22 [0.93–1.61]).
Conduct disorders were found to be significantly associated with dementia diagnoses only within the 12 months before the index date (0–12 months: 5.31 [3.61–7.81]; 12–60 months: 1.4 [0.99–1.99]; 60–120 months: 1.06 [0.6–1.88]). We found no association for sexual dysfunction (0–12 months: not prevalent; 12–60 months: 2.18 [0.41–11.62]; 60–120 months: 1.25 [0.17–9.06]) and tremor (1.13 [0.97–1.32]; 1.15 [1.01–1.30]; 1.18 [0.99–1.41]). Associations between prodromal features and the development of dementia and the prevalence of these features are shown in Table 2.
Associated prodromal features over time.
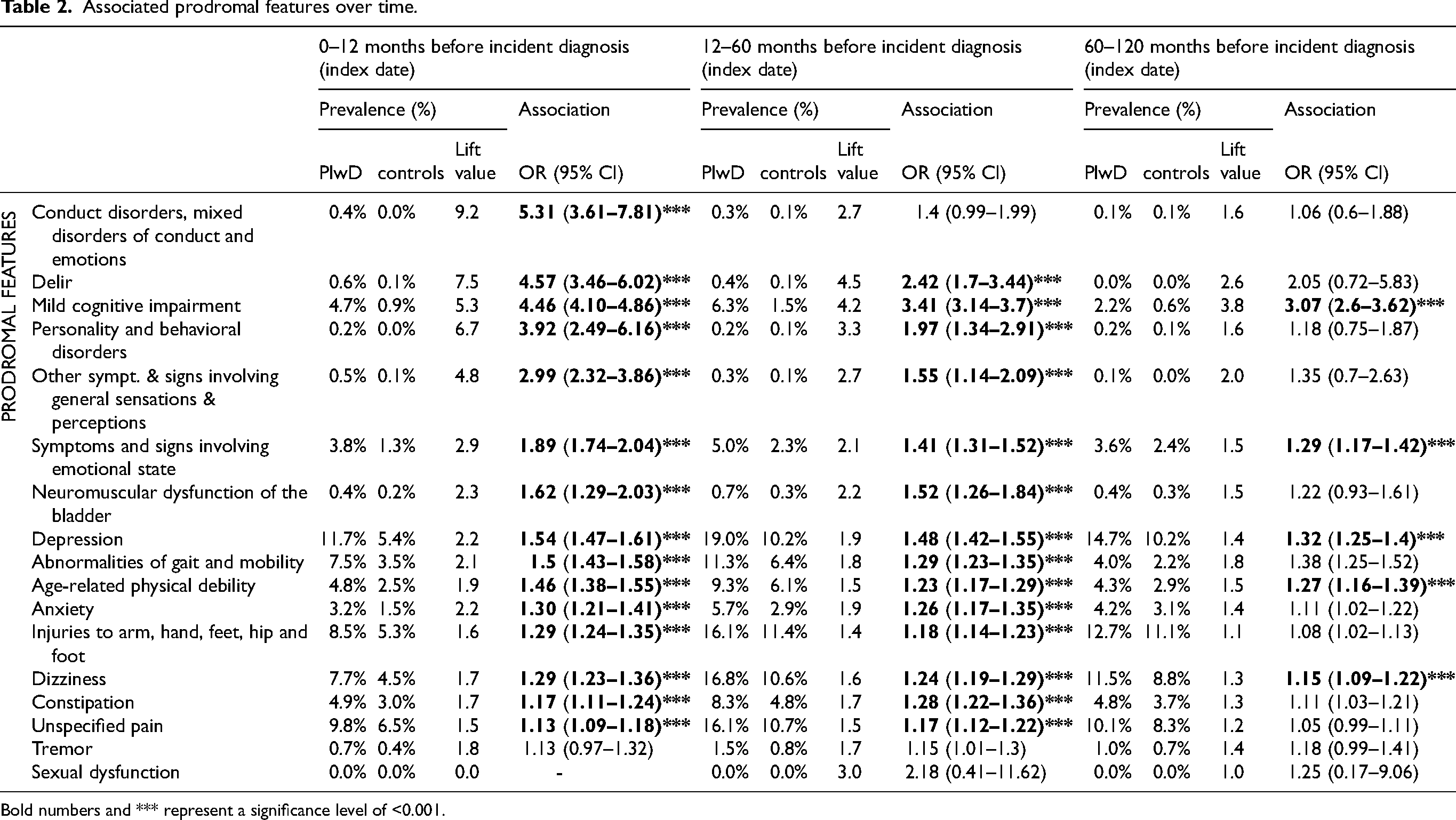
Bold numbers and *** represent a significance level of <0.001.
The highest prevalences for PlwD were found for depression (19.0%), dizziness (16.8%), injuries to arm, hand, feet, hip and foot (16.1%), unspecific pain (16.1%), and abnormalities of gait and mobility (11.3%) for the period of 12 to 60 months before the index date. However, prodromal features with relatively high prevalences had a relatively low lift value of less than two, indicating that such features were less than two times more often seen in PlwD than healthy controls. Contrary to this, the highest lift values were found for prodromal features with the lowest prevalence. The highest lift values were seen within 12 months before the index found for conduct disorders (prevalence 0.4% versus 0.0%, lift value 9.2), delir (prevalence 0.6% vs 0.1%, lift value 7.5), mild cognitive impairment (prevalence 4.7% versus 0.9%, lift value 5.3), and symptoms and signs involving general sensations and perceptions (prevalence 0.5% versus 0.1%, lift value 4.8).
Risk factors and comorbidities
The following positive and significant associations between risk factors and comorbidities and the development of dementia diseases were found constantly for all three periods (0–12 months, 12–60 months, 60–120 months before index): hearing loss (1.24 [1.15–1.35]; 1.24 [1.17–1.32]; 1.29 [1.2–1.39]), visual disturbances (1.2 [1.09–1.32]; 1.45 [1.35–1.55]; 1.48 [1.38–1.59]), diabetes mellitus (1.15 [1.12–1.19]; 1.19 [1.15–1.24]; 1.31 [1.25–1.37]), and cerebrovascular diseases (1.45 [1.39–1.51]; 1.26 [1.21–1.32]; 1.27 [1.2–1.34]). Contrary to this, hypertension (adjusted for hypertensive drugs) (0.84 [0.82–0.87]; 0.87 [0.85–0.9]; 0.88 [0.84–0.92]) and reflux disease (0.83 [0.8–0.88]; 0.81 [0.77–0.85]; 0.86 [0.82–0.91]) represented protective factors in all three periods.
The following associations occurred within 12 and 12 to 60 months before the diagnosis, but not more than 60 months before the index date: mental and behavioral disorders due to use of alcohol (2.36 [1.98–2.81]; 1.7 [1.46–1.97]; 1.34 [1.10–1.63]), intracranial injury (1.67 [1.39–2.01]; 1.5 [1.28–1.77]; 1.45 [1.13–1.85]), Parkinson's disease (1.5 [1.37–1.65]; 1.38 [1.26–1.52]; 1.09 [0.94–1.27]), and epilepsy (1.43 [1.25–1.64]; 1.43 [1.25–1.63]; 1.19 [0.98–1.44]) as factors increasing the risk of developing dementia diseases, and lipid metabolism disorders (1.29 [1.24–1.35]; 1.18 [1.14–1.23]; 0.97 [0.92–1.01]) as protective factor. Chronic fatigue (1.83 [1.23–2.73]), intellectual disabilities (4.77 [2.1–10.84]), and pneumonia (1.29 [1.18–1.41]; 1.05 [0.97–1.12]; 0.98 [0.88–1.08]) demonstrated significant risk factors within 12 months before index only, whereas osteoporosis (0.91 [0.87–0.96]; 0.96 [0.02–1.00]; 0.97 [0.91–1.03]) was a protective factor 12 months before index only.
Up to twelve months before the index, OR was highest for alcohol abuse (OR 2.36), followed by schizophrenia (OR 2.02), Parkinson's disease (OR1.5), cerebrovascular diseases (OR 1.45), epilepsy (OR 1.43), and sepsis (OR 1.35). In the 60 to 120-month prior index period, OR were highest for schizophrenia (OR 2.19), followed by intracranial injuries (OR 1.45), diabetes mellitus (OR 1.31) and cerebrovascular diseases (OR 1.27). There were further significant associations for hypotension, schizophrenia and rheumatoid arthritis as risk factors and upper respiratory and urinary tract infection and gastritis as protective factors for specific periods. We found no association for anosmia, sleep disorders, mental and behavioral disorders due to the use of tobacco, obesity, ischemic heart diseases, atrial fibrillation, migraine, sepsis, ulcus, noninfective enteritis and colitis, osteoarthritis, and bipolar disorder.
The highest prevalence of risk or protective factors and comorbidities was found for hypertension (36.8%–50.6%), diabetes mellitus (18.5%–27.9%), lipid metabolism disorders (15.7%–29.0%), and cerebrovascular diseases (9.7%–15.3%). Instead, intellectual disabilities (2.5–6.1), mental and behavioral disorders due to the use of alcohol (1.6–3.2), schizophrenia (2.1–3.0), intracranial injury (1.8–2.6), and epilepsy (1.6–2.6) represented the highest lift values Table 3.
Associated risk factors over time.
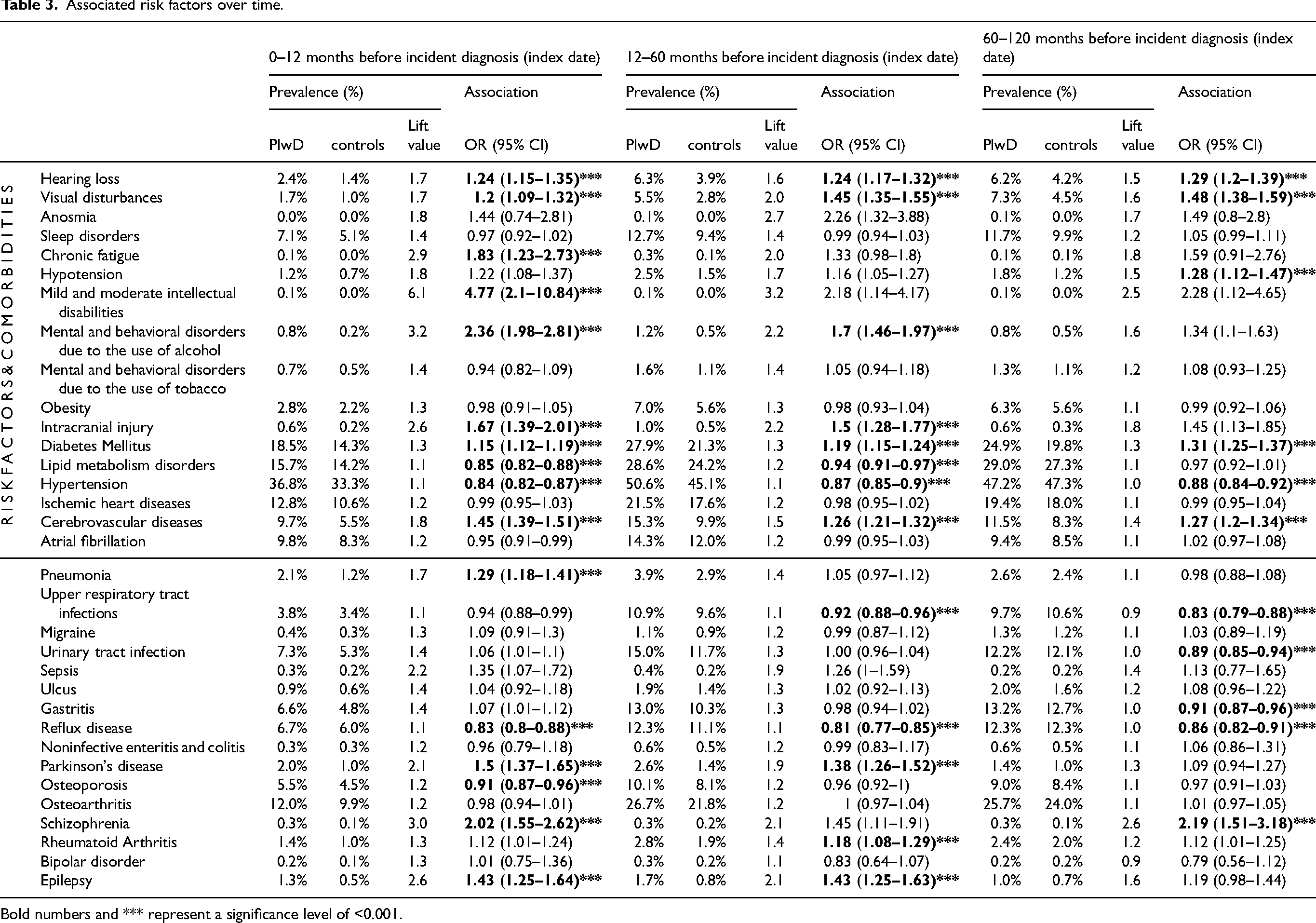
Bold numbers and *** represent a significance level of <0.001.
Medication
Proton pump inhibitors were the only medication showing consistently significant associations over all three periods (1.08 [1.05–1.11]; 1.04 [1.01–1.08]; 1.11 [1.05–1.16]). Antihypertensives (1.22 [1.19–1.25]; 1.15 [1.11–1.19]), statins (1.09 [1.06–1.12]; 1.11 [1.08–1.15]), metformin (1.08 [1.04–1.12]; 1.08 [1.03–1.13]), and antidepressants (1.43 [1.38–1.49]; 1.17 [1.12–1.22]) were significantly associated with the development of dementia within 12 and between 12 and 60 months. Anti-seizure medication (1.38 [1.26–1.51]) demonstrated significant risk factors within 12 months before the index only, while corticosteroids (0.89 [0.85–0.94]) were a protective factor 12 months before the index date. There was a further sporadic association for non-steroidal anti-inflammatory drugs (see Table 4).
Associated medication therapies over time.
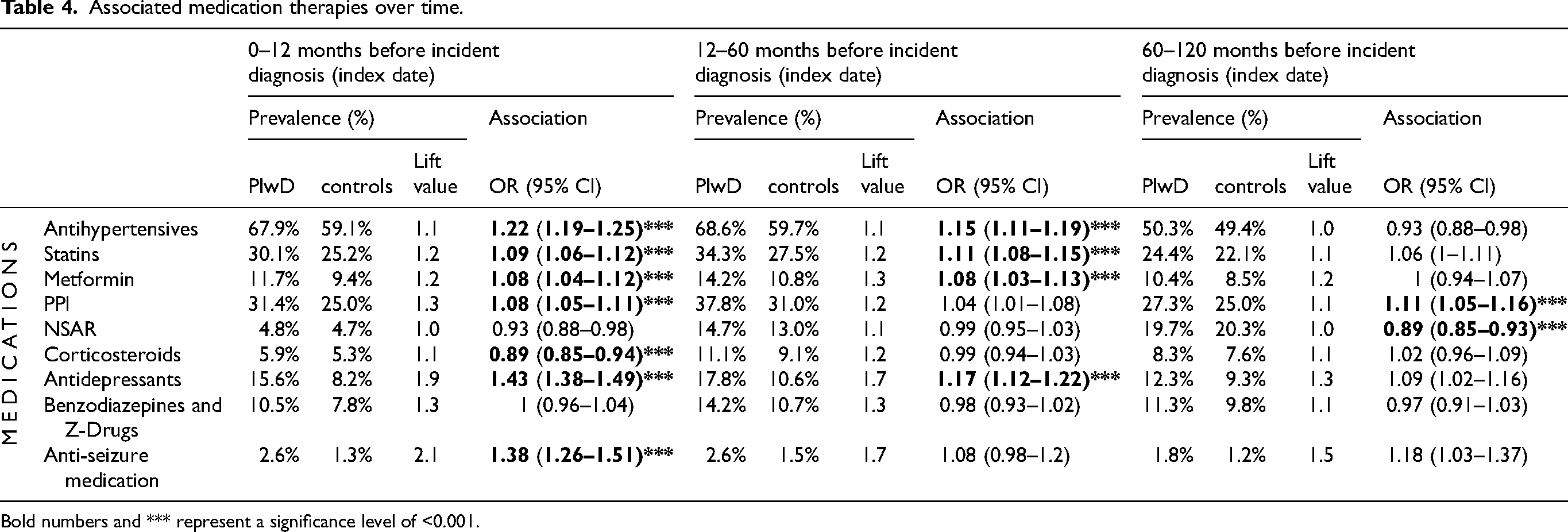
Bold numbers and *** represent a significance level of <0.001.
The prevalences of antihypertensives (50.3–67.9%), statins (24.4%–34.3%), metformin (10.4%–14.2%), and proton pump inhibitors (27.3%–31.4%) were relatively high, but lift values were low, between 1.1 and 1.3. The highest lift value (1.9) and a high prescription prevalence (12.3%–17.8%) were seen for anti-depressive medications. Anti-seizure medication had a relatively high lift value (2.1) but a low prescription prevalence (2.6%).
Discussion
Summary of findings
The study widened the spectrum of the prodromal features and risk factors documented in primary care practices over different periods before the incident dementia diagnosis. Mild cognitive impairment, depression, symptoms involving the emotional state, dizziness, and age-related physical debility were documented prodromal features associated with developing dementia diagnosis across all periods and already five to ten years before the dementia diagnosis. Consistent with the Lancet Commission on dementia prevention, risk factors, such as hearing loss, visual disturbances, diabetes mellitus, and cerebrovascular diseases, were also associated with dementia across all periods. Identifying and more intensively monitoring these factors may help primary care physicians focus on potential consequences for cognitive decline and subsequent dementia.
Prodromal features
There is extensive literature about the prodromal features of dementia.4,15,16 This study demonstrated that primary care physicians documented these features five to ten years before the incident dementia diagnosis. Especially mild cognitive impairment, depression, signs involving the emotional state, dizziness, and age-related physical debility were documented prodromal features already five to ten years before the incident dementia diagnosis, underlining that several prodromal features are visible years before the diagnosis. However, several studies reported that dementia diagnoses are underdiagnosed and delayed in primary care, 27 hindering early detection and post-diagnostic treatment and care to delay the progression of dementia. It is, therefore, possible that a manifest dementia disease already exists in most of these cases even though dementia has not yet been diagnosed.
The diverse array of prodromal symptoms underlined the multifaceted nature of early signs preceding dementia and the challenge of recognizing these in primary care. The difference in the prevalence of prodromal features between PlwD and cognitively healthy controls was low. Therefore, there is a need for enhanced screening strategies, validated assessment tools, guidance and quality indicators, and best practice models for the detection and prevention of these prodromal features in primary care. 28 The highest prevalence was found for mild cognitive impairment, depression, diabetes, signs involving the emotional state and abnormalities of gait and mobility. Additionally, behavioral symptoms, such as conduct disorders, signs involving the emotional state, personality and behavioral disorders, anxiety, and signs involving general sensation and perceptions demonstrated odds comparable with mild cognitive impairment, underlining the importance of considering patients’ behavioral changes as most likely noticeable symptoms that are documented in routine care practice in addition to the cognitive decline. Monitoring these behavioral changes in combination with cognitive function could help general practitioners earlier identify dementia cases and initiate post-diagnostic treatment and care. Translational research strategies are urgently needed to inform primary care physicians about the array of documented prodromal features, enabling an increased sensitivity for these identifiable prodromal features. Also, future research should investigate differences in prodromal features between earlier identified cases of, for example, younger patients and older patients with a high likelihood of a delayed documented diagnosis.
Risk factors and comorbidities
Consistent with the Lancet Commission on dementia prevention, intervention, and care,6,7 hearing loss, traumatic brain injury, alcohol consumption, depression, and diabetes mellitus were identified as risk factors for dementia that primary care physicians documented before the dementia diagnosis, supporting the existing body of evidence.6,7 However, we found no significant association for other reported risk factors, e.g., sleep disorders, arterial fibrillation, inflammation, migraine, gastrointestinal diseases, nicotine abuse and obesity.
For smoking, there is uncertain evidence that non-smokers have a lower risk of developing dementia diseases.29,30 However, in primary care, “Mental and behavioral disorders due to use of tobacco” can only be used as an indicator instead of “smoking” itself, limiting the differentiation between smokers and non-smokers and between heavy, infrequent and non-smokers. Also, our analysis included patients who survived over ten years before the incident documented dementia diagnosis. Since smoking is a predictor of premature death, 31 a bias in our data is possible, underlining the challenges of using secondary data.
Looking at obesity, meta-analyses6,7,32 that included people aged 35 to 65 years demonstrated that a body mass index higher than 30 (RR 1.3,95% CI 1.1–1.6) in mid-life (40 to 60 years of age) was associated with increased risk of developing dementia diseases. Contrary to this, studies conducted with patients in their late life stages revealed inconsistent results. 33 Therefore, the presented results of our late-life cohort with an average age range from 63 to 73 align with this evidence. Also, there were counterintuitive results for hypertension, representing a consistent protective factor for developing dementia in our data, which the same age-specific pattern could explain. Several studies revealed that persistent midlife hypertension but not late-life hypertension is associated with an increased dementia risk, 7 mainly if hypertension persists into later life.9,21 A cohort study from the UK demonstrated that hypertension was a significant risk factor for persons aged 50 years but not for persons aged 60 to 70 years, for which a reduced risk was found. 34 Our study aligns with these findings. Blood pressure generally falls with the onset of dementia, 35 which could then lead to a lower prevalence of elevated blood pressure in the early dementia phase. Therefore, it is possible that the incident-documented dementia diagnoses were delayed so that the ten-year period still falls within the early dementia phase. Our models were adjusted for hypertensive drugs, which could additionally affect the presented results. However, sensitivity analyses that excluded the medications confirmed hypertension as a protective factor. This means that some of the well-known risk factors for dementia, such as obesity and hypertension, were non-significant or protective factors in the late-life period. This underlines the challenge of primary care physicians’ recognition of risk factors, shifting to focus on late-life risk factors only, which is currently not well-known and established. Therefore, age-specific preventive screening and intervention strategies are needed to improve the efficiency of preventive measures in routine care practice.
Implication and conclusion
The results have significant implications for healthcare providers, especially primary care physicians, who are crucial in identifying prodromal symptoms and risk factors to initiate interventions to prevent cognitive decline and detect dementia diseases as early as possible. The diverse nature of prodromal features and risk factors and minor differences in the prevalence of these factors between PlwD and those without dementia underscore the challenge of detecting dementia diseases in primary care. It also emphasizes the importance of a holistic approach to patient care that not only focuses on patients’ cognition as prodromal features. Primary care physicians have to take a broader view, especially on changes in social behavior, mental health, mood, and limitations in functional abilities. These features have the potential to be recognized and linked to dementia years before the incident diagnosis is made. Additionally, most factors are also relevant for preventing non-communicable diseases or are non-communicable diseases themselves, which is tremendously relevant for primary care physicians who take a more holistic approach toward health beyond just dementia prevention.
Risk factors must be identified and monitored in relation to the patient's age, especially in mid- and late life. Well-known risk factors may present a risk in midlife but are protective in late life, increasing the challenge of handling risk factors and preventive strategies in primary care. This also underscores the extended time window for preventive strategies, starting at the beginning of mid-life at 40. Thus, prevention strategies in routine care urgently need guidance to consider all risk factors, comorbidities and medications simultaneously at the respective age. This represents a tremendous challenge, especially regarding demographic changes, with an increasing number of patients per physician practice. Innovative approaches, such as machine learning and artificial intelligence, are needed and could assist and support dementia risk prediction in routine care practice, using documented diagnoses in real time to foster early identification of common prodromal features and risk factor patterns associated with dementia diseases. Whereas a first study indicated acceptable accuracy for early dementia screening, 36 further research is needed to evaluate such approaches under routine care conditions.
Limitations
Certain limitations should be acknowledged. The study's retrospective nature and reliance on routine care data may introduce bias. The data can only be used to generate hypotheses, not to confirm known prodromal features and risk factors based on secondary primary care physician documentation data. Another major limitation is the exclusion of patients who passed away during the observation period of 10 years. The mortality rate of older adults at the age of 80 is approximately five to ten percent. The exclusion of these patients is biased and limits the presented results’ generalizability. Also, we could not evaluate physical inactivity, social integration, air pollution and smoking due to the non-existence of routinely collected data in primary care practices.
In addition, there could be sex-specific differences between the presented findings. Several studies examined sex and gender differences in the development of dementia as a biological variable in dementia research to advance the understanding of the pathophysiology of these condition,37,38 revealing, for example, that estrogen production plays tissue-specific roles 39 and elucidating sex differences in disease phenotypes will be instrumental for individual, multimodal, biomarker-driven and sex-sensitive strategies for disease prevention and detection. 40 Therefore, future research should explore the interplay between genetic predispositions and environmental factors as well as sex-specific differences, providing a more nuanced understanding of dementia risk.
There is also the possibility of reverse causation in risk factors that could not be elaborated, limiting the generalizability of the presented results. This would mean that early symptoms might be caused by underlying, undiagnosed dementia, rather than being risk factors for its development. Some studies demonstrated that, for example, depressive episodes41,42 or weight loss 43 can be an early symptom of dementia rather than a risk factor. Investigating potential interactions between identified risk factors may contribute to a more comprehensive risk assessment model and should be focus of future studies.
In conclusion, this study contributes valuable information to the growing knowledge of dementia risk factors and prodromal symptoms. The consistent and novel findings underscore the importance of continued research to inform preventive strategies and enhance the early detection of individuals at risk for dementia.
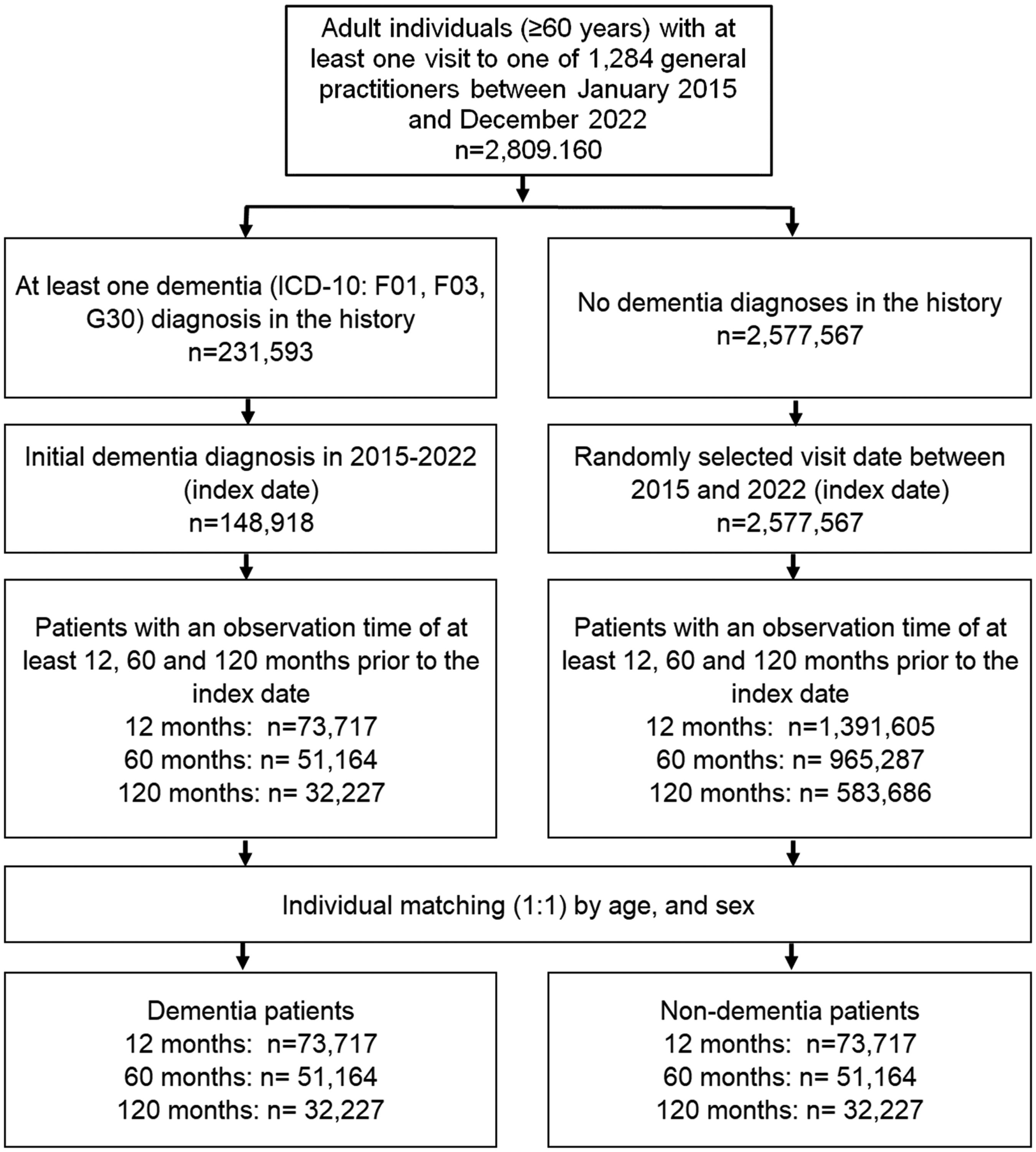
Participant Flow. Selection of study patients.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241295407 - Supplemental material for Documentation of prodromal features and risk factors of dementia disease in primary care practice
Supplemental material, sj-docx-1-alz-10.1177_13872877241295407 for Documentation of prodromal features and risk factors of dementia disease in primary care practice by Bernhard Michalowsky, Stefan Teipel, Steffi Riedel-Heller, Karel Kostev and Jens Bohlken in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Bernhard Michalowsky (Conceptualization; Data curation; Investigation; Methodology; Supervision; Visualization; Writing – original draft); Stefan Teipel (Conceptualization; Supervision; Validation; Writing – review & editing); Steffi Riedel-Heller (Conceptualization; Methodology; Supervision; Validation; Writing – review & editing); Karel Kostev (Data curation; Formal analysis; Methodology; Writing – review & editing); Jens Bohlken (Conceptualization; Formal analysis; Supervision; Validation; Writing – review & editing).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BM, KK, and ST are Editorial Board Members of this journal but were not involved in the peer-review process of this article nor had access to any information regarding its peer-review. BM received consulting fees from Lilly and Biogen and is a paid lecturer of the University Greifswald for the lecture “Health Economic Evaluation.” JB received consulting fees from Lilly, Biogen, and Schwabe. ST received payment for a lecture/symposium with Eli Lilly in November 2023 and is a Member of the Data Safety and Monitoring Board of Envision (Biogen) and a member of Advisory Boards for Eisai, Lilly, and Biogen. SRH and KK have no conflicts of interest.
Data availability
Data used belongs to IQVIA and can only be obtained in aggregated form upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.