
Abstract
Background
Gantenerumab is a fully human anti-amyloid-β (Aβ) immunoglobulin G1 monoclonal antibody for subcutaneous (SC) administration. The efficacy and safety of low-dose (105 mg or 225 mg) gantenerumab were investigated in SCarlet RoAD (SR; NCT01224106), a Phase III, double-blind (DB), placebo-controlled study in participants with prodromal Alzheimer's disease. Following a pre-planned futility analysis, SR was converted into an open-label extension (OLE) study.
Objective
To assess the long-term safety and tolerability of SC gantenerumab at doses of up to 1200 mg every 4 weeks (Q4W) in OLE participants who previously received placebo or gantenerumab in the DB part of SR.
Methods
Participants of the DB part of SR, who met the eligibility criteria for the OLE, were offered the opportunity to receive gantenerumab up-titrated to 1200 mg Q4W according to prespecified titration regimens. Safety and tolerability were assessed using magnetic resonance imaging (MRI), physical and neurologic examinations, and adverse event monitoring.
Results
Overall, 154 participants were rolled over from the DB part of SR and received at least one dose of gantenerumab in the SR OLE. The median duration of treatment was 2.9 years (152.9 weeks). Forty-seven (30.5%) participants had an amyloid-related imaging abnormalities – edema (ARIA-E) MRI finding, and 51 (33.1%) had an ARIA – hemorrhage MRI finding. Most ARIA-E findings were asymptomatic and manageable by MRI monitoring and dose intervention. There were no unexpected safety findings.
Conclusions
SC gantenerumab at doses of up to 1200 mg Q4W was well tolerated with no unexpected safety findings in participants with prodromal Alzheimer's disease.
Introduction
Alzheimer's disease (AD) is the most common cause of dementia and may contribute to 60–70% of all cases. 1 In 2020, it was estimated that there are around 55 million people worldwide living with dementia. As the proportion of older people in the population is increasing, this number is expected to rise to 78 million in 2030 and 139 million in 2050. 2
Recent studies have shown that monoclonal antibodies that target amyloid-β (Aβ) species can slow the rate of disease progression in AD.3–5 To date, three molecules have received approval based on evidence of amyloid-lowering activity. Aducanumab was the first anti-amyloid antibody to receive accelerated approval by the US Food and Drug Administration (FDA) in June 2021 and lecanemab was the second, receiving an accelerated approval in January 2023, followed by traditional FDA approval in July 2023.6,7 Most recently, donanemab received a traditional FDA approval in July 2024. 8
Gantenerumab is an investigational, fully human anti-Aβ immunoglobulin G1 monoclonal antibody for subcutaneous (SC) administration, with highest affinity for aggregated Aβ, including oligomers, fibrils, and plaques.9–11 It is thought to remove Aβ via microglia-mediated phagocytosis, to promote amyloid plaque clearance,9,11 and it has shown downstream effects on biomarkers of AD pathology and neurodegeneration in clinical trials.9,12–14
The effects of SC low-dose (105 mg or 225 mg every 4 weeks [Q4W]) gantenerumab on cognition and function were investigated in two multicenter, randomized, double-blind, placebo-controlled studies in participants with prodromal AD (SCarlet RoAD [SR]; NCT0122410612,15) and mild AD dementia (Marguerite RoAD [MR]; NCT02051608 16 ). Dosing in the double-blind part of the SR study was halted on December 19, 2014 following a preplanned futility analysis, and the primary data from the double-blind part of the study were subsequently published. 12 Data from these analyses, together with results from the PRIME Phase Ib study (NCT01677572) of aducanumab, suggested that the gantenerumab doses under study were subtherapeutic. 17 Subgroup analyses indicated that higher exposure to gantenerumab may have clinically relevant effects on cognition and function in participants predicted to show faster progression as defined by a mathematical model developed by Delor et al. (2013).12,18
The SR and MR studies were converted into open-label extension studies (OLEs) to enable comprehensive and rigorous assessment of the safety and tolerability of SC gantenerumab titrated to doses of up to 1200 mg Q4W, in participants who received placebo or gantenerumab in the double-blind parts of the respective studies.
Several titration regimens were modeled to achieve a significant reduction in the amyloid positron emission tomography (PET) signal after 1 year of treatment while ensuring an acceptable amyloid-related imaging abnormalities – edema (ARIA-E) event rate over 2 years for both apolipoprotein E ε4 allele (APOE ε4) carriers and non-carriers. The models used to inform dose selection and titration regimens for the SR OLE have been described previously. 17 Briefly, a population pharmacokinetic (PK)/pharmacodynamic model estimated that a gantenerumab dose of 1200 mg administered SC Q4W would lead to 20% plaque removal after 1 year. This model was supported by the PRIME study, in which treatment with aducanumab reduced brain Aβ plaques measured by florbetapir PET imaging in a dose-dependent manner. An aducanumab dose level of 10 mg/kg was associated with 20% less amyloid on PET standardized uptake value ratio at 54 weeks. Simultaneously, in those receiving 10 mg/kg aducanumab, statistically significant slowing of clinical decline measured by the Clinical Dementia Rating – Sum of Boxes (CDR-SB) at Week 54 was observed. 19 Safety outcomes, with respect to ARIA-E, at doses higher than the 225 mg dose (the highest gantenerumab dose tested in the SR double-blind treatment period) were projected from the results of the double-blind part of SR and the PRIME study, using a bapineuzumab-based empirical time-to-event model for ARIA-E,19,20 taking into consideration known risk factors for ARIA-E: drug concentrations, time since the first dose, and APOE ε4 allele status. The fixed dose of 1200 mg SC Q4W, required to achieve the targeted plaque removal, was associated with a high predicted ARIA-E rate of approximately 60% in APOE ε4 carriers.
With the implementation of a dosing regimen with gradual up-titration, it was predicted that participants should be able to reach the target dose of 1200 mg within 10 months (for APOE ε4 carriers on placebo or 105 mg gantenerumab during double-blind treatment) and within 6 months (for APOE ε4 carriers who previously received 225 mg and non-carriers). With such a schedule, the incidence of ARIA-E was expected to be approximately 25%, lower than the incidence of approximately 60% predicted for APOE ε4 carriers without using a gradual up-titration regimen.
Here, we present safety and efficacy data, along with data from the pharmacodynamic analysis from the SR OLE that were used, in conjunction with data from the MR OLE (Neve A, et al. unpublished data), to inform the dose and titration scheme of the GRADUATE I and II Phase III studies (NCT03444870; NCT03443973). 21
Methods
Study design and participants
SR was a Phase III, multicenter, randomized, double-blind, placebo-controlled, parallel-group study of gantenerumab for participants with prodromal AD, which was followed by an OLE. The methods for the double-blind part of the study have been reported previously. 12
Briefly, the double-blind part of SR consisted of Parts 1 and 2 (Figure 1). In Part 1, 799 participants were enrolled and consisted of individuals aged 50–85 years who met the International Working Group criteria for prodromal AD, with evidence of amyloid pathology via cerebrospinal fluid Aβ42 assessment and largely preserved functional abilities such that a diagnosis of dementia could not be made. These participants were randomized to receive gantenerumab (105 mg or 225 mg) or placebo SC Q4W for 104 weeks. Participants who had completed Part 1 of the study through the Week 104 visit were then given the option to enter a (blinded) extension of the study (Part 2), in which they continued to receive the study drug for up to 2 additional years. All participants who were enrolled into SR, met the eligibility criteria, and had at least one follow-up/drop-out visit after double-blind treatment, were offered participation in the OLE (Part 3).

Study schema. aDosing in Parts 1 and 2 of the study was terminated on December 19, 2014 as a result of the preplanned futility analysis, and participants continued with the DB follow-up as per protocol. bThis period was not prespecified in the protocol – its length was dependent on approval of Protocol WN25203G by health authorities and IRBs/ECs. cAfter the initial 156 weeks of OLE, participants had the option to continue treatment until July 2020 under Protocol WN25203H (with the exception of Canada and Russia, these local protocols were not extended beyond the initial 156 weeks as participants would not complete the Week 156 visit until close to the July 2020 last dose date). All participants who consented to these additional years (beyond Week 156) completed the study in July 2020 regardless of the visit week. The last dosing visit week was dependent on when participants enrolled in the OLE; therefore, participants could reach up to OLE Week 236. DB: double-blind; EC: ethics committee; IRB: institutional review board; OLE: open-label extension.
Participants were not eligible for the trial if they met treatment discontinuation criteria for cumulative ARIA – hemorrhage (ARIA-H), had received another investigational medicine after the end of the double-blind part, or had discontinued from the double-blind part for safety reasons (see the Supplemental Material for further details).
Participants continuing from the double-blind part of SR into the OLE had an off-study period lasting between 12 and 18 months after completion of the double-blind follow-up period. This period of 12–18 months was not prespecified in the protocol, and its length was dependent on the approval of the OLE protocol by health authorities and institutional review boards/ethics committees. Only participants at countries/sites where this OLE protocol had been approved had the option to participate in the OLE; this limited the number of participants who were eligible to enroll into the OLE.
This study was conducted in accordance with the Declaration of Helsinki and the study protocol was approved by the relevant local institutional review boards/ethics committees.
Titration regimen and dose administration
Two titration regimens were tested in the SR OLE (Figure 2), taking into consideration the number of participants in the OLE, the anticipated risk in the population, and the length of the time that participants were “off treatment” between the end of the SR double-blind part and the start of the SR OLE. 17 The two regimens differed in starting dose, number of up-titration steps, and time to reach the target dose, and were dependent on the last dose that the participants received in the double-blind part of the study, as well as their APOE ε4 carrier status.

Up-titration regimen for the SCarlet RoAD OLE. MRI performed prior to each dose increase and then at regular intervals. Implementation of dosing algorithms in case of ARIA findings. APOE ε4: apolipoprotein E ε4 allele; ARIA: amyloid-related imaging abnormalities; MRI: magnetic resonance imaging; OLE: open-label extension. Adapted from Bateman RJ et al. Alzheimers Res Ther 14, 178 (2022) under the terms of the Creative Commons CC BY license https://creativecommons.org/licenses/by/4.0/.
As APOE ε4 carrier status is a known risk factor for ARIA, the initial dose in the SR OLE was 105 mg for APOE ε4 carriers receiving placebo and 105 mg gantenerumab during double-blind treatment, and 225 mg for APOE ε4 carriers previously receiving 225 mg gantenerumab and participants who were non-carriers.
Doses of 105 and 225 mg were administered SC by a pre-filled syringe or from a vial. 22 The 450 mg and 900 mg doses could be administered SC by pre-filled syringe or from vials using an infusion pump. The 1200 mg gantenerumab dose was administered SC from vials using an infusion pump.
Outcome measures
The primary objective of the OLE was to assess the safety and tolerability of gantenerumab given at doses up to 1200 mg SC Q4W. Safety and tolerability were assessed by magnetic resonance imaging (MRI), physical and neurologic examinations, vital signs, blood safety tests, electrocardiograms, Columbia Suicide Severity Rating Scale, and adverse event (AE) reporting. AEs were coded using the Medical Dictionary for Regulatory Activities (MedDRA) version 23.1.
Secondary outcomes included: the effect of 1200 mg gantenerumab SC Q4W over time on brain amyloid load by PET imaging; the effect of 1200 mg gantenerumab SC Q4W over time on clinical outcomes (cognition and function) compared with the start of the OLE; and to explore PK and the incidence of anti-drug antibodies with higher gantenerumab doses in the target participant population. A full schedule of assessments is provided in Supplemental Table 1.
MRI monitoring and management of MRI findings
MRI scans in the OLE were performed prior to each increase in gantenerumab dose and at regular intervals (∼6 months) thereafter. All MRI scans were read by a central reader, and information about potential central nervous system (CNS) symptoms was collected prospectively (i.e., the investigator contacted the participant up to 1 week prior to each MRI).
Prespecified dose intervention rules were included in the SR OLE for both ARIA-E and ARIA-H findings (Table 1). Briefly, in the case of asymptomatic ARIA-E with a Barkhof Grand Total Scale score 23 of <4, dosing could continue at the same dose level, but no up-titration could occur. If the ARIA-E was symptomatic or with a Barkhof Grand Total Scale score of ≥4, dosing was temporarily interrupted; reintroduction of dosing/titration occurred once ARIA-E was considered resolved. For ARIA-H findings, if the cumulative number of ARIA-H reached more than eight at dose levels below 450 mg, study treatment was discontinued; at dose levels of 450 mg or higher, further up-titration was suspended. If the cumulative number of ARIA-H reached more than ten, study treatment was discontinued.
Rules for ARIA management in the SR OLE.
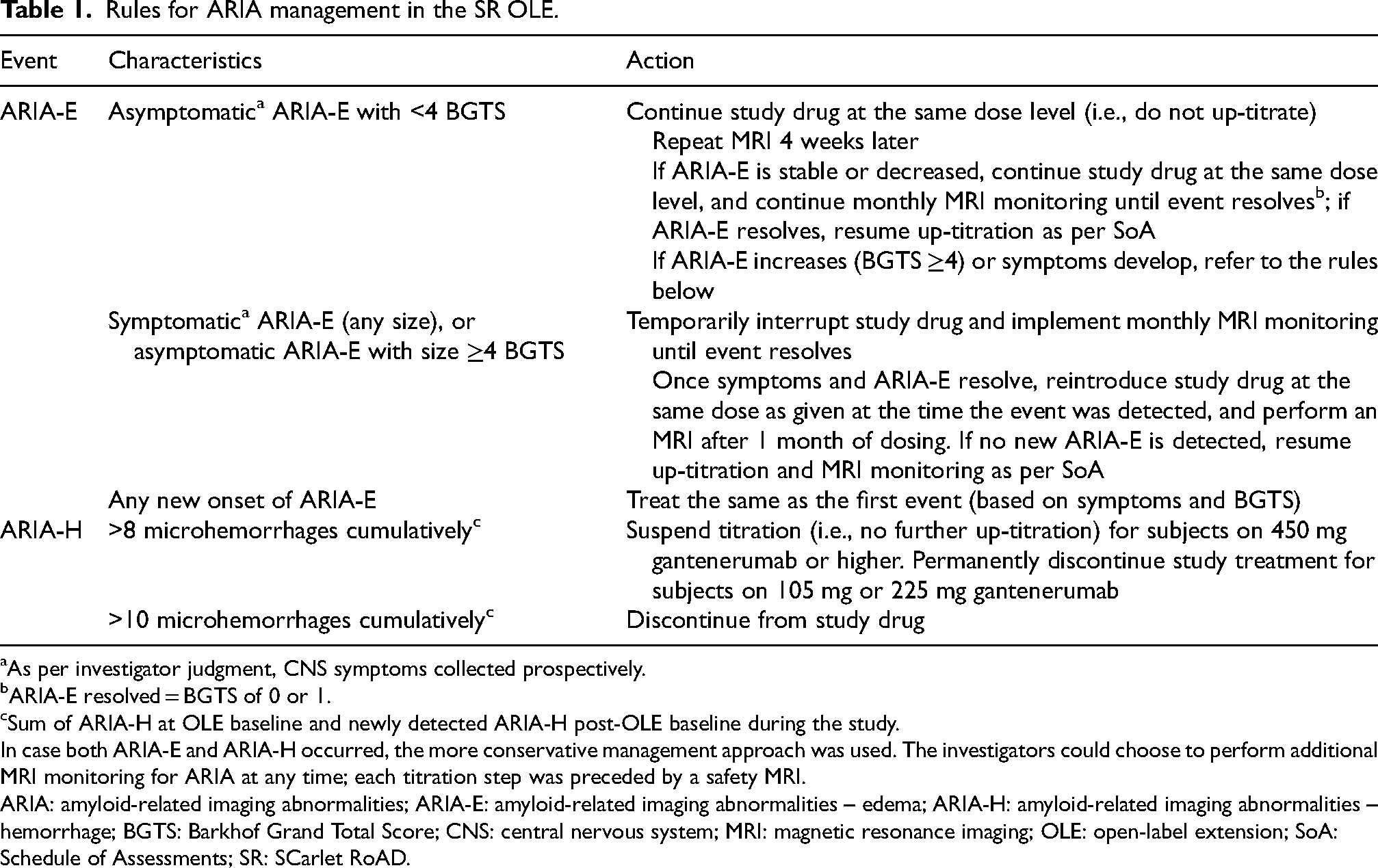
aAs per investigator judgment, CNS symptoms collected prospectively.
bARIA-E resolved = BGTS of 0 or 1.
cSum of ARIA-H at OLE baseline and newly detected ARIA-H post-OLE baseline during the study.
In case both ARIA-E and ARIA-H occurred, the more conservative management approach was used. The investigators could choose to perform additional MRI monitoring for ARIA at any time; each titration step was preceded by a safety MRI.
ARIA: amyloid-related imaging abnormalities; ARIA-E: amyloid-related imaging abnormalities – edema; ARIA-H: amyloid-related imaging abnormalities – hemorrhage; BGTS: Barkhof Grand Total Score; CNS: central nervous system; MRI: magnetic resonance imaging; OLE: open-label extension; SoA: Schedule of Assessments; SR: SCarlet RoAD.
Not all ARIA-E, ARIA-H, or other MRI findings were reportable AEs. These were only reportable as AEs if they met one or more of the following criteria: were accompanied by clinical symptoms; led to a change in study treatment (e.g., dose interruption or permanent discontinuation); required a change in concomitant therapy; resulted in a medical intervention; or were otherwise clinically significant in the investigator's judgment.
For ARIA-E analysis, using MedDRA standards, ARIA-E events reported as AEs were mapped to the following terms: “amyloid-related imaging abnormality-edema/effusion” or “vasogenic cerebral edema”. For ARIA-H analysis, ARIA-H events were mapped to the following: “amyloid-related imaging abnormality-microhemorrhages and hemosiderin deposits”, “cerebellar microhemorrhage”, “cerebral microhemorrhage”, or “cerebral hemosiderin deposition”.
Imaging assessments
Changes in brain amyloid load over time were assessed using Florbetapir 18F (AV-45; Amyvid™), and compared with screening (if available) and the OLE baseline PET (defined as either the last PET scan performed during the double-blind part of the study within 12 months prior to the first dose in the OLE, or if not available, an OLE baseline scan performed within 8 weeks prior to the first dose in the OLE). This objective was evaluated annually during the initial 3 years of the OLE in a subset of consenting participants in the longitudinal PET sub-study.
MRI was used to evaluate the effect of gantenerumab over time on hippocampal volume, whole brain volume, ventricular enlargement, and other volumetric measures of the brain compared with the double-blind phase baseline screening. This objective was assessed during the initial 3 years of the OLE.
Cognitive and functional assessments
Cognition was assessed using the Alzheimer Disease Assessment Scale – Cognitive Subscales 11 and 13 and the Free and Cued Selective Reminding Test – Immediate Recall during the initial 3 years of the OLE, and by Mini Mental State Exam for the entire duration of the OLE. During the initial 3 years of the OLE, secondary endpoints also included the Functional Activities Questionnaire compared with the OLE baseline, and the CDR-SB and CDR – Global Score compared with the OLE baseline.
Dementia assessment was performed to assess a diagnosis of dementia. In most cases, to meet the criteria for dementia, worsening from baseline should be seen on one or more domains of the CDR, the Functional Activities Questionnaire, and in cognition. Time to dementia was defined as the time interval between the first treatment date and the date that the participant is assessed as having Alzheimer-type dementia by investigators. This objective was evaluated only during the initial 3 years of the OLE.
PK assessments
PK were quantified using plasma concentrations of gantenerumab. The development of anti-drug antibodies was assessed, and the impact of these on PK and safety was explored.
Statistical analysis
The analysis population for this study was the safety-evaluable population, which comprised participants who received at least one dose of gantenerumab during the OLE. There was no formal hypothesis testing in the OLE portion of the study. The analyses of ARIA events were summarized by the up-titration scheme assigned in the OLE or APOE ε4 status to inform the incidence of ARIA findings and provide further supporting evidence to the ARIA management guidance. Non-ARIA analyses were summarized by cohort. These reflected the treatment assignment that participants received during the double-blind part of the study, as neither the up-titration scheme nor APOE ε4 status was considered to bear a significant impact on the non-ARIA analyses, which focused on change in outcomes over time.
Results
Study population
All 154 participants enrolled in the OLE had received at least one dose of gantenerumab and were thus included in the safety-evaluable analysis population. All participants also had at least one post-OLE baseline MRI. Eighty-one (53%) participants were assigned to up-titration scheme 1 (35 participants had received placebo and 46 received gantenerumab during the double-blind part of the study), and 73 (47%) were assigned to up-titration scheme 2 (14 participants had received placebo and 59 had received gantenerumab during the double-blind part of the study). Fifty-nine participants completed up-titration scheme 1 and reached the target dose of 1200 mg, and 64 participants completed up-titration scheme 2 and reached the target dose of 1200 mg (Figure 3).
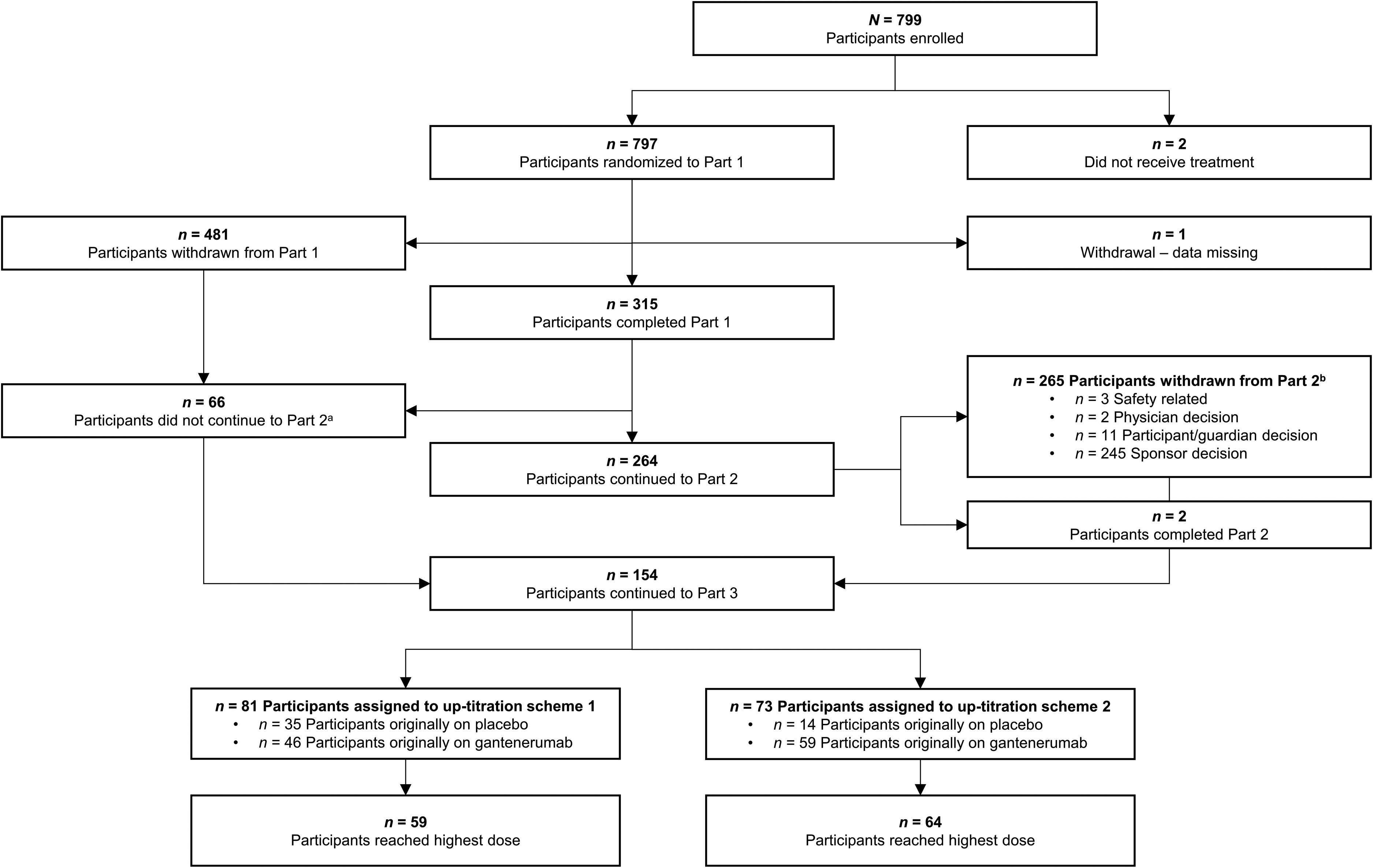
Disposition of participants in the Scarlet RoAD OLE. aParticipants who did not complete Part 1 but had at least one follow-up/drop-out visit, and thus were given the option to participate in Part 3. bParticipants who did not complete Part 2 but had at least one follow-up/drop-out visit, and thus were given the option to participate in Part 3. OLE: open-label extension.
Baseline characteristics
Of the 154 participants, 32% had received placebo and 68% had received gantenerumab (105 mg: 30%; and 225 mg: 38%) in the double-blind part of the study (Table 2). Participants had a median age of 75 years at OLE baseline; the majority were female (59.1%) and White (92.9%). The APOE 1ε4 genotype was the most common (57.8%), followed by 0ε4 (29.2%) and 2ε4 (13.0%). These participants differed in terms of baseline demographic and disease characteristics from participants originally enrolled in the SR double-blind study in that they were older, with the majority >70 years old. The mean CDR-SB (standard deviation) of the originally enrolled participants was 2.11 (0.97), whereas by the start of Part 3, the mean CDR-SB (standard deviation) worsened to 5.24 (3.12). Other baseline characteristics were indicative of disease progression, which was expected due to the elapsed time. 12 Assigned up-titration schemes in Part 3 were not matched as they were allocated based on prior treatment history, which was determined, in part, by APOE ε4 status.
Demographic characteristics by previous randomization at OLE baseline.

ADAS-Cog11/13: Alzheimer's Disease Assessment Scale – Cognitive Subscale 11/13; APOE: apolipoprotein E allele; ARIA-E: amyloid-related imaging abnormalities – edema; ARIA-H: amyloid-related imaging abnormalities – hemorrhage; CDR-GS: Clinical Dementia Rating – Global Score; CDR-SB: Clinical Dementia Rating – Sum of Boxes; DB: double blind; FAQ: Functional Activities Questionnaire; FCSRT-IR: Free and Cued Selective Reminding Test – Immediate Recall; MMSE: Mini-Mental State Examination; OLE: open-label extension; SD: standard deviation; SR: SCarlet RoAD.
Most participants (93.5%) had not experienced an ARIA-E during the double-blind part, and 72.1% did not have ARIA-H at OLE baseline. Based on the CDR – Global Score at OLE baseline, 64 participants (41.6%) had mild dementia, 18 (11.7%) had moderate dementia, and one (0.6%) had severe dementia.
The use of any approved symptomatic treatments for AD was permitted during the OLE. Please see the Supplemental Material for further details on the symptomatic treatments initiated during the OLE.
Summary of AEs
The median duration of exposure to treatment was 2.93 years (152.86 weeks), and the median number of treatment administrations was 38. Of the 154 participants who received gantenerumab in the OLE, 146 participants (94.8%) reported at least one AE.
The most frequently reported treatment-related AEs were injection site reactions (54 [35.1%] participants); ARIA-E (41 [26.6%] participants), and ARIA-H (25 [16.2%] participants).
Fifty-seven (37%) participants experienced AEs leading to dose intervention, with ARIA-E and ARIA-H being the most frequent (31 [20.1%] and 15 [9.8%] participants, respectively). Twenty-nine (18.8%) participants were withdrawn from treatment following an AE, with the most frequent events being ARIA-H (11 [7.1%] participants) and ARIA-E (6 [3.9%] participants) (Table 3).
Overview of AEs by previous randomization (safety-evaluable population).

All values are n (%) unless otherwise stated.
Administration-related reaction (referred to as “injection site reaction”) is defined as terms that contained “injection site”, “infusion site”, or “injection-related”.
AE: adverse event; ARIA-E: amyloid-related imaging abnormalities – edema; ARIA-H: amyloid-related imaging abnormalities – hemorrhage.
Forty-six participants experienced serious AEs (SAEs; 29.9%), of whom six had SAEs that were assessed by the principal investigator as related to study treatment (one participant experienced ARIA-E and epilepsy; one participant experienced a confusional state as a symptom of ARIA-E; and single occurrences of cerebral hemorrhage, cerebral hematoma, generalized tonic–clonic seizure, and epilepsy were reported in four participants). There were four deaths (2.6%) (due to arrhythmia, myocardial infarction, sepsis, and a sudden death); all were considered unrelated to study treatment by the principal investigator. There were no AEs of special interest (drug-induced liver injury, suspected transmission of infectious agent), and no clinically relevant changes from OLE baseline were observed for any of the laboratory parameters and electrocardiograms (data on file). For the most frequently reported AEs (≥5% of participants), please refer to Supplemental Table 2.
Incidence of ARIA MRI findings
All 154 participants who received gantenerumab had at least one post-baseline MRI scan in the OLE. Not all ARIA-E or ARIA-H cases were reportable as AEs (see Methods); hence, data in this section are based on ARIA-E and ARIA-H MRI findings. Overall, 47 (30.5%) participants had a new ARIA-E MRI finding post baseline in the OLE and 51 (33.1%) participants had a new ARIA-H MRI finding post-OLE baseline. Thirty-one (20.1%) participants had both new ARIA-E and new ARIA-H MRI findings post baseline in the OLE, not necessarily concurrently (Table 4). 24
ARIA findings by up-titration regimen (safety-evaluable population with post-baseline MRI in OLE)a.
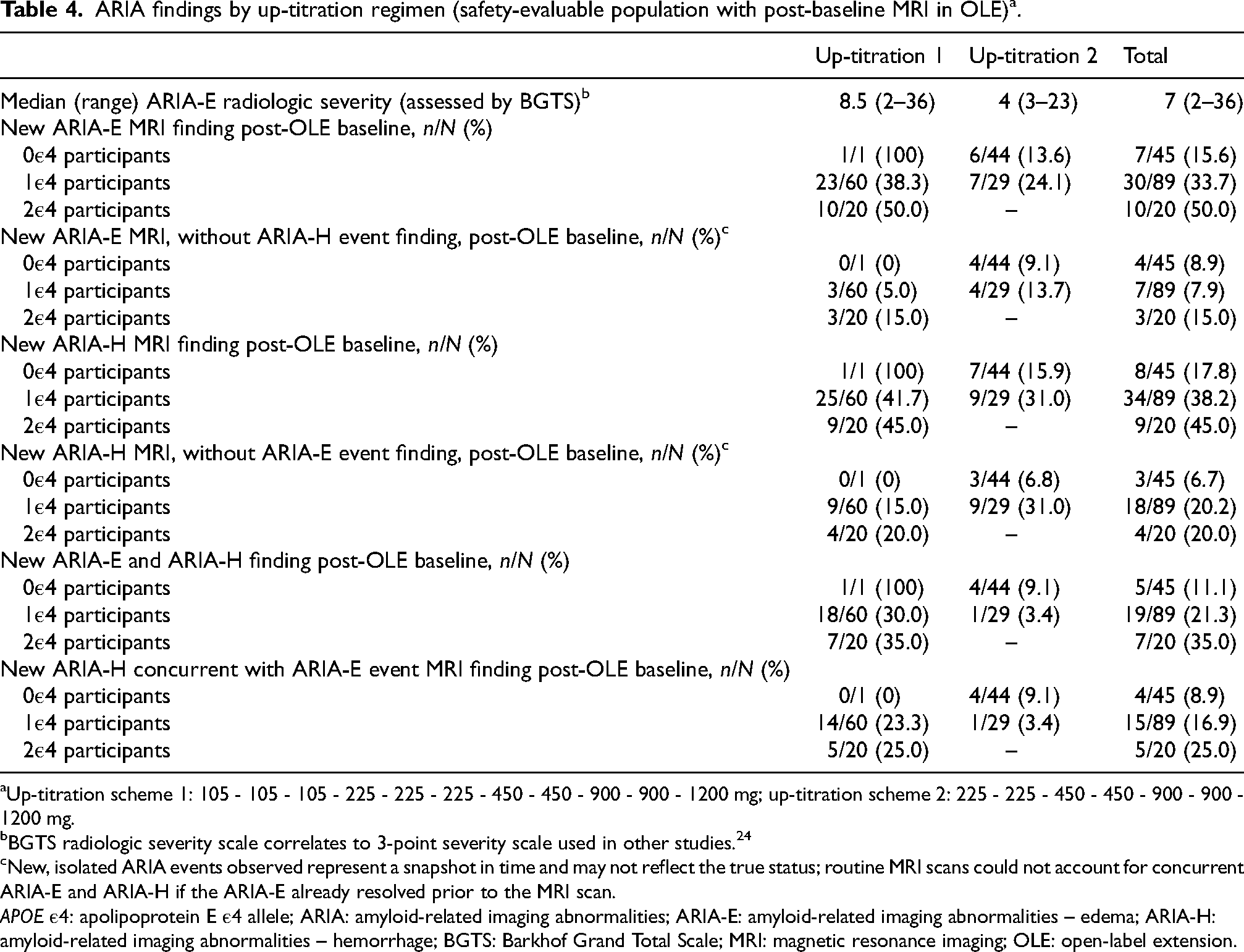
aUp-titration scheme 1: 105 - 105 - 105 - 225 - 225 - 225 - 450 - 450 - 900 - 900 - 1200 mg; up-titration scheme 2: 225 - 225 - 450 - 450 - 900 - 900 - 1200 mg.
bBGTS radiologic severity scale correlates to 3-point severity scale used in other studies. 24
cNew, isolated ARIA events observed represent a snapshot in time and may not reflect the true status; routine MRI scans could not account for concurrent ARIA-E and ARIA-H if the ARIA-E already resolved prior to the MRI scan.
APOE ε4: apolipoprotein E ε4 allele; ARIA: amyloid-related imaging abnormalities; ARIA-E: amyloid-related imaging abnormalities – edema; ARIA-H: amyloid-related imaging abnormalities – hemorrhage; BGTS: Barkhof Grand Total Scale; MRI: magnetic resonance imaging; OLE: open-label extension.
Most ARIA-E findings were seen at higher doses and in APOE ε4 carriers (Table 4 and Supplemental Table 3). Of the 20 APOE ε4 homozygous carriers, ten (50.0%; all in up-titration scheme 1 because no APOE ε4 homozygous carriers were included in up-titration scheme 2) had ARIA-E MRI findings in the OLE. Of the 89 APOE ε4 heterozygous carriers, 30 (33.7%; 23 in up-titration scheme 1 and seven in up-titration scheme 2) had ARIA-E MRI findings in the OLE. Of the 45 APOE ε4 non-carriers, seven (15.6%; one participant in up-titration scheme 1; six participants in up-titration scheme 2) had ARIA-E MRI findings in the OLE.
The median time to first ARIA-E MRI finding was 38 weeks, and ≥75% of the first ARIA-E MRI findings occurred in the first 52 weeks of the OLE. Overall, 65 of the 71 (91.5%) ARIA-E MRI findings in the OLE resolved during the observation time of this study, of which 53% of the ARIA-E MRI findings resolved within 12 weeks, and 87% within 24 weeks. The time to first ARIA-E event and time to ARIA resolution by APOE ε4 carrier status are shown in Figure 4.

Time to first ARIA-E event (a) and time to ARIA-E resolution (b) by APOE ε4 carrier status. Treated participants have received at least one dose of study drug. Time to first ARIA-E event (weeks) - Censoring: Event (1 = censored, 0 = event). Time to first ARIA-E event in OLE for the participants with/without ARIA-E is calculated as ARIA-E onset date in OLE - first study drug intake in OLE + 1 day, otherwise ARIA-E onset date is the latest MRI scan date in OLE after first study drug intake in OLE. APOE ε4: apolipoprotein E ε4 allele; ARIA-E: amyloid-related imaging abnormalities – edema; MRI: magnetic resonance imaging; NE: no event; OLE: open-label extension.
CNS symptoms that were associated with ARIA-E MRI findings
Two approaches to identify symptoms associated with ARIA-E were used. The first was a protocol-defined approach, whereby participants were contacted by the investigator within 1 week prior to each MRI, to determine, by non-directive, unbiased questioning, if they experienced any CNS AEs. Such AEs were to be specifically designated in the electronic case report form. Those AEs that were reported accordingly and were associated with a prospective ARIA-E MRI finding were used for this analysis. Based on this approach, eight participants reported at least one AE that was considered a symptom associated with an ARIA-E. In total, nine AEs were reported (Table 5). The majority of reported AEs were non-serious, and mild or moderate in intensity. None of the events in these participants led to permanent discontinuation of study treatment.
AEs reported as symptoms of ARIA-E MRI findings per study protocol approach (safety-evaluable population with one post-baseline MRI in OLE).
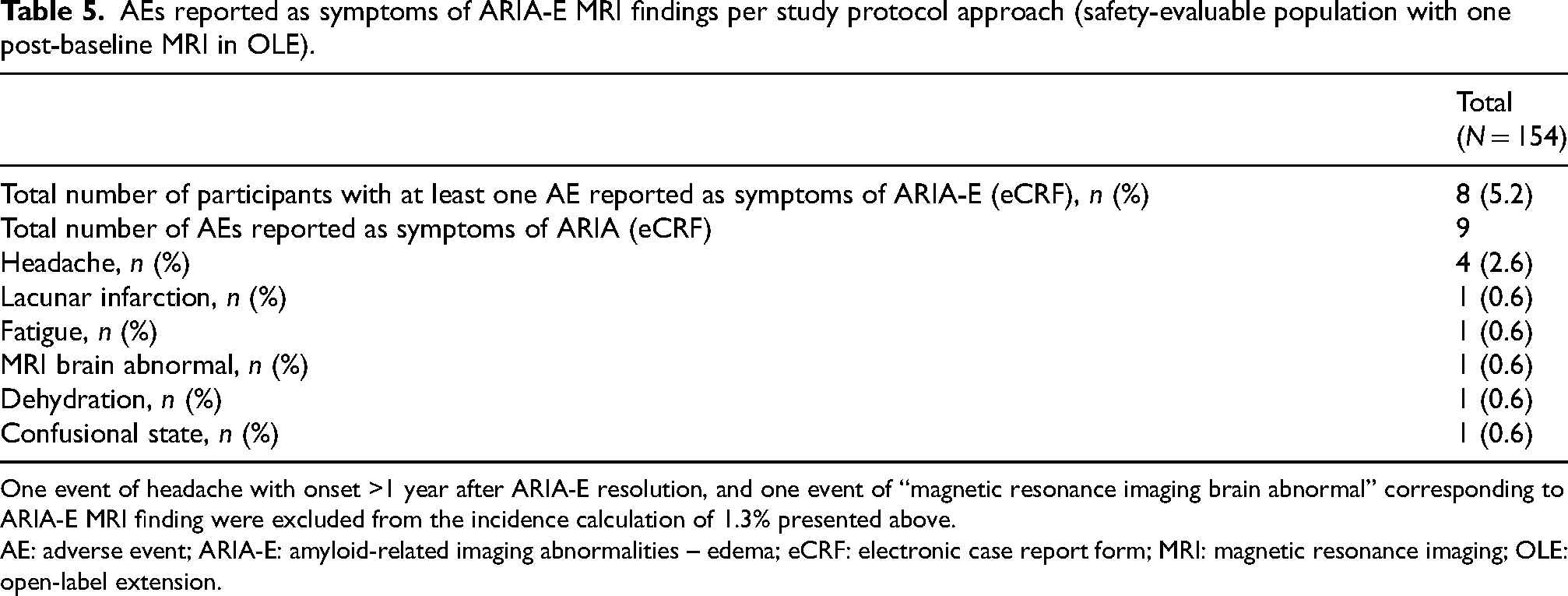
One event of headache with onset >1 year after ARIA-E resolution, and one event of “magnetic resonance imaging brain abnormal” corresponding to ARIA-E MRI finding were excluded from the incidence calculation of 1.3% presented above.
AE: adverse event; ARIA-E: amyloid-related imaging abnormalities – edema; eCRF: electronic case report form; MRI: magnetic resonance imaging; OLE: open-label extension.
In a second, post hoc analysis (see the Supplemental Material for methodology), of the 19 participants with ARIA-E MRI findings and with an associated CNS AE (Supplemental Table 4), 4 events were reported as serious, all led to hospitalization. Two participants reported an event of seizure and one participant reported an event of cerebral hematoma, all of which were severe in intensity. One participant reported a serious event of confusional state that was moderate in intensity. Out of the four SAEs, three (seizure, cerebral hematoma, confusional state) were assessed as related to study treatment by the investigator. Please refer to the Supplemental Material for further details.
Injection site reactions
Of the 154 participants, injection site reactions were reported in 56 (36.4%) participants, who included 53 (34.4%) participants with an event of injection site reaction, and three (1.9%) participants with events of injection site erythema. In total, 635 events of injection site reaction were reported (Table 6). All events of injection site reaction were non-serious and mild in intensity, except one that was of moderate intensity. All events except one resolved, and only 5.4% of participants (3 out of the 56) who experienced an injection site reaction received treatment, which included topical steroids and antihistamines. No participants withdrew from study treatment due to an injection site reaction.
Signs and symptoms associated with injection site reactions by previous randomization (safety-evaluable population).

All values are n (%) unless otherwise stated.
aAdministration-related reaction (referred to as “injection site reaction”) is defined as terms that contained “injection site”, “infusion site”, or “injection-related”.
Assessment of changes in amyloid load over time
Amyloid PET burden decreased substantially for all participants with available PET data in the OLE. The group mean centiloid value after 104 weeks of treatment in the OLE was below the positivity threshold of 24 centiloids, which is considered to be the threshold differentiating no-to-sparse plaques from moderate-to-frequent plaques in histopathology-verified PET studies. 25 Data from the amyloid PET sub-study for change in Aβ plaque burden from OLE baseline to Week 52, Week 104, and Week 156 assessed using Florbetapir 18F PET have been previously published.9,26
Discussion
The SR OLE study investigated the long-term safety and tolerability of 1200 mg SC Q4W gantenerumab, which was achieved through two up-titration regimens. Overall, gantenerumab doses of up to 1200 mg SC Q4W had an acceptable safety and tolerability profile in participants with AD. Amyloid burden decreased substantially over time, demonstrating a strong pharmacodynamic effect of gantenerumab 1200 mg SC Q4W. ARIA-E incidence in each of the up-titration regimens was acceptable and below that expected without up-titration. The majority of participants did not experience ARIA-E during the study period. When ARIA-E findings did occur, these were mostly asymptomatic. If symptoms were associated with ARIA-E findings, they were mostly non-serious and mild. Overall, ARIA findings were clinically manageable with the protocol-defined MRI monitoring and dose intervention rules. As reported by others,5,27–29 there was an association between APOE ε4 carrier status and incidence of ARIA-E and ARIA-H seen in 50% of participants with the APOE 2ε4 genotype; a doubling of the incidence observed in participants with the APOE 1ε4 genotype. It has been hypothesized that the higher incidence of both ARIA-E and ARIA-H in APOE ε4 homozygous carriers is likely due to a higher presence of cerebral amyloid angiopathy. 30 Injection site reactions were non-serious, and generally mild in intensity. These findings support and provide evidence for a favorable safety profile of gantenerumab at doses of 1200 mg administered SC Q4W.
The results of the SR OLE study should be interpreted in the context of the following limitations. Firstly, there was no placebo arm in the SR OLE, as it was designed to evaluate two different up-titration schemes for safety and biomarker outcomes and therefore no conclusions regarding the clinical efficacy of gantenerumab can be drawn. However, an exploratory analysis comparing the SR OLE (and MR OLE) data with an Alzheimer's Disease Neuroimaging Initiative external control showed a slowing of cognitive decline compared with these external controls, as seen on the CDR-SB and other measures, following continued gantenerumab treatment over 3 years. 31 Secondly, the titration regimens were confounded with baseline risk factors, including APOE ε4 status and prior dosing history, and speed of up-titration, due to which comparisons between the two different titration regimens cannot be made.
In summary, data from the SR OLE study provide evidence of a favorable benefit/risk profile of SC gantenerumab at this higher target dose. With this overall profile, participants who completed the OLEs of SR and MR were given the option to continue open-label gantenerumab in the Open RoAD study (NCT04339413), a multicenter, rollover study to evaluate the safety and tolerability of long-term administration of gantenerumab. 32 Following the negative pre-planned analysis of pivotal Phase III studies GRADUATE I and GRADUATE II (see below), Open RoAD was terminated by the Sponsor as the benefit-risk assessment in participants with Alzheimer's disease was no longer considered favorable.
SR OLE data were used to inform the design of the pivotal Phase III GRADUATE I and II studies, which included a single 9-month titration regimen that aimed to maximize exposure to SC gantenerumab for all participants, regardless of APOE ε4 status. 21 The outcomes from the GRADUATE studies indicated a lower overall effect on pharmacodynamic measures, with notably lower amyloid plaque removal than observed in the SR and MR OLE studies,9,26 and statistically significant clinical efficacy was not demonstrated. 21 The reasons for these outcomes are currently being explored.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241303644 - Supplemental material for Long-term safety of gantenerumab in participants with Alzheimer's disease: A phase III, open-label extension study (SCarlet RoAD)
Supplemental material, sj-docx-1-alz-10.1177_13872877241303644 for Long-term safety of gantenerumab in participants with Alzheimer's disease: A phase III, open-label extension study (SCarlet RoAD) by Mercè Boada, Anuja Neve, Bibha Das, Jakub Wojtowicz, Zhiyue Huang, Szofia Bullain, Michelle Watkin, Dominik Lott, Tobias Bittner, Paul Delmar, Gregory Klein, Carsten Hofmann, Geoffrey A Kerchner, Janice Smith, Monika Baudler, Paulo Fontoura and Rachelle S Doody in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
We would like to thank all participants, study partners, investigators, and site staff for their engagement with the gantenerumab program.
Author contributions
Mercè Boada (Formal analysis; Writing – review & editing); Anuja Neve (Data curation; Formal analysis; Supervision; Writing – original draft; Writing – review & editing); Bibha Das (Data curation; Formal analysis; Writing – review & editing); Jakub Wojtowicz (Data curation; Formal analysis; Writing – review & editing); Zhiyue Huang (Data curation; Formal analysis; Writing – review & editing); Szofia Bullain (Formal analysis; Writing – review & editing); Michelle Watkin (Formal analysis; Writing – review & editing); Dominik Lott (Formal analysis; Writing – review & editing); Tobias Bittner (Formal analysis; Writing – review & editing); Paul Delmar (Formal analysis; Writing – review & editing); Gregory Klein (Formal analysis; Writing – review & editing); Carsten Hofmann (Conceptualization; Formal analysis; Methodology; Writing – review & editing); Geoffrey A Kerchner (Formal analysis; Writing – review & editing); Janice Smith (Formal analysis; Writing – review & editing); Monika Baudler (Formal analysis; Writing – review & editing); Paulo Fontoura (Conceptualization; Formal analysis; Supervision; Writing – review & editing); Rachelle S Doody (Formal analysis; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by F. Hoffmann-La Roche Ltd, Basel, Switzerland. Medical writing support for the development of this manuscript was provided by Joshua Quartey, BSc, and Matt Gooding, PhD, of Nucleus Global, funded by F. Hoffmann-La Roche Ltd, Basel, Switzerland.
Declaration of conflicting interests
Mercè Boada reports receiving consulting fees from Grifols, Araclon Biotech, F. Hoffmann-La Roche Ltd, Biogen, Lilly, Merck, Zambon, and Novo-Nordisk; holding advisory board memberships with Grifols, F. Hoffmann-La Roche Ltd, Lilly, Araclon Biotech, Merck, Zambon, Biogen, Novo-Nordisk, Bioiberica, Eisai, Servier, and Schwabe Pharma; and receiving lecture fees from F. Hoffmann-La Roche Ltd, Biogen, Grifols, Nutricia, Araclon Biotech, Servier, and Novo-Nordisk.
Anuja Neve is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Bibha Das is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Jakub Wojtowicz is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Zhiyue Huang is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Szofia Bullain was an employee of and owned stock or stock options in F. Hoffmann-La Roche Ltd at the time of the study. Szofia Bullain is currently an employee of and owns stock in Biogen Inc.
Michelle Watkin is an employee of Roche Products Ltd, and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Dominik Lott is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Tobias Bittner is an employee of F. Hoffmann-La Roche Ltd and Genentech Inc., part of F. Hoffmann-La Roche Ltd, and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Paul Delmar is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Gregory Klein is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Carsten Hofmann is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Geoffrey A. Kerchner is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Janice Smith is an employee of Roche Products Ltd, and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Monika Baudler is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Paulo Fontoura is an employee of and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Rachelle S. Doody is an employee of F. Hoffmann-La Roche Ltd and Genentech Inc., part of F. Hoffmann-La Roche Ltd, and owns stock or stock options in F. Hoffmann-La Roche Ltd.
Data availability
For eligible studies, qualified researchers may request access to individual participant-level clinical data through a data request platform. At the time of writing, this request platform is Vivli (https://vivli.org/ourmember/roche/). For up-to-date details on Roche's Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here: ![]() . Anonymized records for individual participants across more than one data source external to Roche cannot, and should not, be linked due to a potential increase in risk of patient re-identification.
. Anonymized records for individual participants across more than one data source external to Roche cannot, and should not, be linked due to a potential increase in risk of patient re-identification.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.