
Abstract
Background
While the preventive effects of green tea and coffee on cognitive decline have been demonstrated, their long-term effects on cognition remain unclear.
Objective
This study aims to investigate the effect of green tea and coffee consumption in middle age on the prevention of dementia.
Methods
This population-based cohort study included 1155 participants (aged 44–66 in 1995). Participants’ consumption of green tea and coffee was assessed using questionnaires in 1995 and 2000. Their cognitive levels were neuropsychologically evaluated in 2025–2015. Logistic regression analyses were conducted with significant cognitive decline (defined as multi-domain cognitive decline and more severe conditions) as the dependent variable. Stratified analyses were also conducted by sex and age.
Results
Individuals who consumed 2–3 cups of green tea daily had a significantly reduced risk of cognitive decline (OR = 0.56, 95%CI: 0.35–0.91) after adjusting potential confounders. However, this effect was not significant with consumption of 4 or more cups. This protective effect was particularly observed in males (OR = 0.38, 95%CI: 0.19–0.76). A significant risk reduction was also observed in individuals consuming one or more cups of coffee daily (OR = 0.54, 95%CI: 0.34–0.84) in the older subjects (median age [53 years old] and older in 1995) in the same fully adjusted model, but not in the entire sample.
Conclusions
Our findings suggest that moderate green tea consumption in midlife may have a beneficial effect on preventing dementia, particularly in males. The effects of coffee consumption may be more advantageous for older individuals.
Introduction
Dementia prevention is critically important in our increasingly ageing society. 1 The number of people with dementia worldwide is escalating rapidly; over 55 million people were affected in 2019, and projections suggest that this number will rise to 139 million by 2050. The financial impact of dementia is also staggering, with costs expected to reach 2.8 trillion dollars by 2030. 2 Several preventive approaches have been identified, including the management of modifiable risk factors for dementia (e.g. hypertension and smoking) and early detection/intervention strategies to slow the progression of dementia. Neuroimaging evidence has revealed that the accumulation of amyloid begins even in middle age, 20–30 years before the onset of Alzheimer's disease (AD). 3 Additionally, metabolic syndrome in middle age significantly increases the risk of dementia, including AD, with vascular ageing believed to affect amyloid-β (Aβ) processing and clearance. 4 Given these findings, identifying modifiable factors associated with the development of dementia is crucial, regardless of the type of dementia. In this context, lifestyle in middle age, including dietary and drinking habits, has increasingly attracted attention.
The effect of tea and coffee on dementia prevention, especially their long-term effects, remains a subject of ongoing debate. In contrast, the Mediterranean diet has shown robust preventive benefits and our previous study also demonstrated a protective effect of fish consumption.5,6 A recent meta-analysis of coffee indicated that one cup of coffee daily may reduce the risk of dementia, especially in individuals aged over 60 years. 7 Regarding tea, various kinds of tea are consumed worldwide, including black tea and green tea, and the protective effects of both on dementia have been documented repeatedly.8–15 Recent large-sampled cohort studies using the UK biobank data demonstrated a U-shaped relationship between dementia risk reduction and the consumption of both teas (including black and green tea),8,9 although a previous meta-analysis showed a linear relationship between decline in dementia risk and green tea consumption. 7
While the mechanisms of the preventive effect of green tea and coffee on cognitive decline have been broadly proposed, these mechanisms are not fully understood. The effects of green tea consumption include antioxidation, anti-inflammation, vasoprotection, and protection of Aβ accumulation. One of the major green tea polyphenols, epigallocatechin gallate, appears to provide these preventive effects as its main actions.9,16 Other components of green tea, such as theanine and arginine—specific amino acids extracted from tea leaves—could also have neuroprotective effects, primarily involving relaxation effects. 17 The preventive effect of coffee on cognitive decline may also have broad mechanisms, including cognitive stimulation, antioxidation, anti-inflammation, and protection against Aβ accumulation.18,19
Although current cohort studies have revealed medium-term effects (5–9 years) of green tea and coffee habits on dementia prevention, their longer-term effects remain unknown. Given the desirability of preventing early amyloid accumulation and the acceleration of vascular ageing, investigating the effects of green tea and coffee habits in middle age on the development of dementia is pressing. Here, we examined the data of a 20-year follow-up cohort study to investigate the long-term effects of green tea and coffee habits.
Methods
Population
This cohort study was conducted in a subgroup of the Japan Public Health Center-based Prospective Study (JPHC Study), initiated in 1990–1993. 20 The original study consisted of questionnaires at baseline, as well as at 5- and 10-year follow-up (response rate: 74–81%). The present study was conducted on residents in the Saku Public Health Center catchment area (Nagano Prefecture) and involved 12,219 participants at study initiation in 1990. An invitation letter for mental health screening was sent to this population (8827 participants), excluding people who had moved out of the study area, died, or did not respond to the later questionnaires in 2014–2015. Responses were received from 1297 participants. Among these, 1204 had comprehensive dietary assessment data from both the 5- and 10-year follow-up surveys. One participant was excluded from the present analysis due to insufficient data for classifying cognitive decline. Another participant who reported an unusual average total amount of non-alcoholic drinking was excluded because these responses were considered inaccurate. Participants with a self-reported history of stroke (N = 7), a potential mediator for dementia, were also excluded. Finally, data from 1155 participants (475 men and 680 women) were analyzed. Participants provided written informed consent for participation in the mental health screening survey conducted in 2014–2015. The study design is illustrated in Figure 1. The study was approved by the Institutional Review Board of the National Cancer Center Japan and Keio University School of Medicine. The study was carried out in accordance with the ethical guidelines set forth by the Declaration of Helsinki.
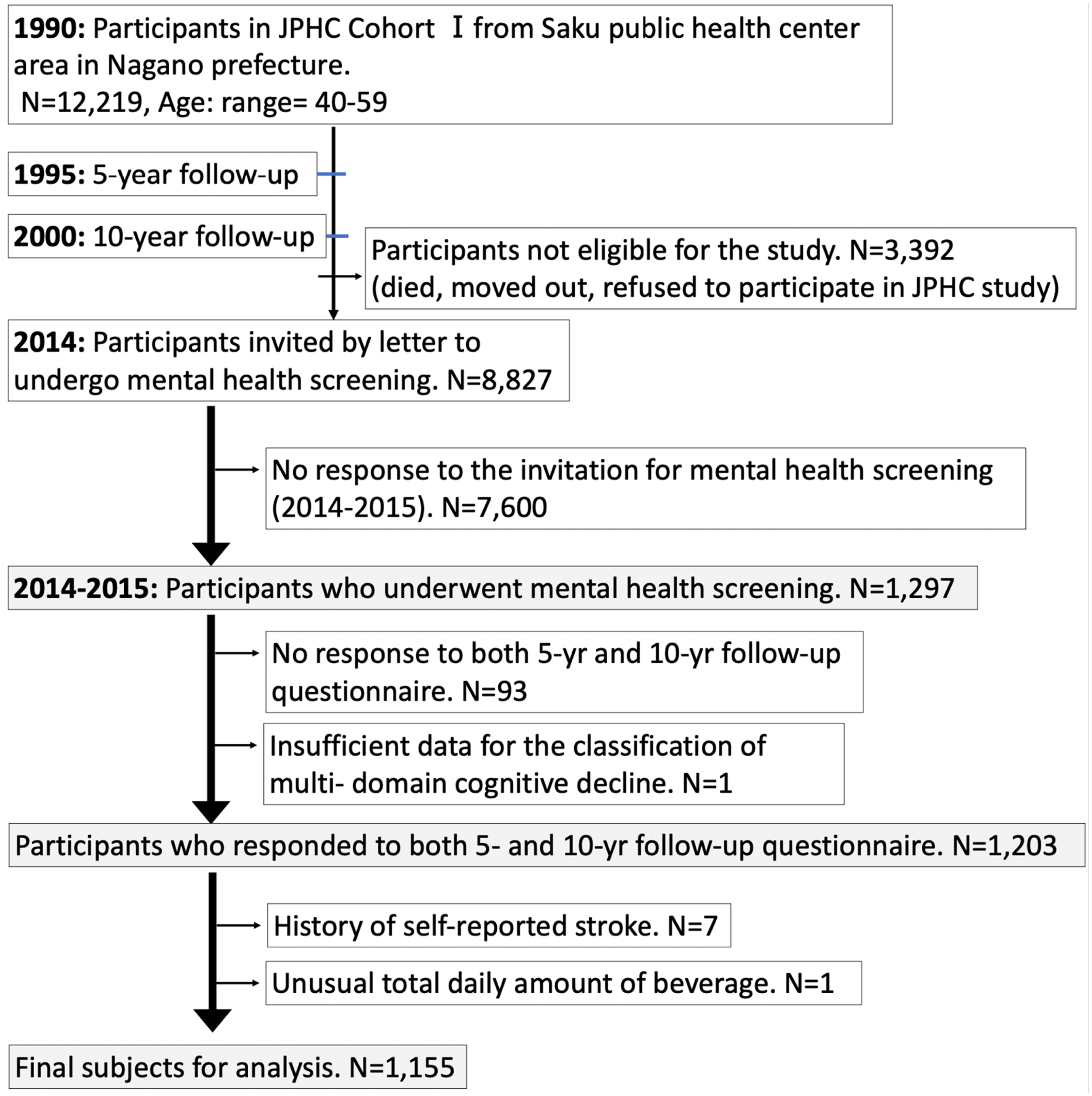
Study population and flowchart.
Habitual tea and coffee consumption
The questionnaire asked participants about their frequency of consumption over the past year of the following items: green tea (sen-cha), green tea (ban-cha/genmai-cha), and coffee and canned coffee. There were 9 categories for each item (<1 time/week, 1–2 times/week, 3–4 times/week, 5–6 times/week, 1 cup/day, 2–3 cups/day, 4–6 cups/day, 7–9 cups/day, and ≥10 cups/day). We asked about the frequency of tea and coffee consumption in the same manner in both the 5- and 10-year follow-up surveys. To evaluate habitual tea and coffee consumption over these extended periods, we calculated the average consumption over 5 years by using both questionnaires. Tea consumption was calculated based on 120 ml/cup per single time, while the two green tea items were summed between the two questionnaires. Coffee consumption was also calculated as 120 ml/cup per single time and the two coffee items were summed between the two questionnaires. Although oolong tea and black tea were also included in our questionnaire, they were excluded from our analysis due to the insufficient number of participants (85 and 25 participants, respectively) who consumed these teas daily or more frequently. These categorical data on tea and coffee consumption were recalculated and incorporated into our statistical models (see Statistics section).
Evaluation of cognitive decline and current depressive symptoms
In the present investigation in 2014–2015, cognitive function was assessed by experienced neuropsychologists using the Mini-Mental State Examination (MMSE), 21 Wechsler Memory Scale Revised (WMS-R) logical memory, 22 clock drawing test, 23 and Clinical Dementia Rating (CDR) scale. 24 Dementia was initially defined with an MMSE cut-off point (23/24). 21 Mild cognitive impairment (MCI) was categorized as amnestic MCI, which was originally presented by Petersen et al. 25 Alongside these neuropsychological assessments, depressive symptoms were evaluated using the Center for Epidemiologic Studies Depression Scale (CES-D) and the Patient Health Questionnaire-9 (PHQ-9).25,26 Final diagnoses were made by trained psychiatrists who were blinded to the questionnaire results through clinical interviews incorporating both neuropsychological and psychiatric assessments in accordance with the Diagnostic and Statistical Manual of Mental Disorder, 4th Edition, Text Revision. 27 As no brain imaging was conducted, types of dementia were not classified. Given the high risk of conversion in MCI, 28 participants labeled with MCI were further categorized into two groups: single-domain MCI, indicated solely by memory impairment manifested by the logical memory subset test; and multi-domain MCI, indicated by either a decline in the clock drawing test or CDR ≥ 0.5 in at least one of the categories (orientation, judgment and problem-solving, community affairs, home and hobbies, and personal care, in addition to memory impairment). 25 This classification method follows that of our previous study. 29 Participants who had clinically significant depressive symptoms in the clinical interview with the above questionnaires were diagnosed as having a current depressive episode.
Identification of physical illness and lifestyle
Past medical history, including head injury, depression, diabetes, cancer, and ischemic heart disease, along with educational level were assessed at the time of mental health screening (2014–2015). Educational level was also collected as categorical data (junior high school, high school, junior college, and college or higher level). Body mass index (BMI: <18.5, 18.5–22.9, ≥23), smoking status (never, former, and current), fish consumption (estimated based on food frequency in the questionnaire), 6 and frequency of alcohol (6 categories from no or little to every day) and sports (5 categories from one or less/month to almost every day) were extracted from the data of the 5-year follow-up survey.
Statistics
To conduct binary logistic analysis, participants were divided into two groups: those with significant cognitive decline and those without. This categorization served as an independent variable. The significant cognitive decline group included participants with dementia and multi-domain MCI as defined above. Regarding green tea consumption, due to the distribution of data, green tea consumption (total amount of both sen-cha and ban-cha/genmai-cha) was reclassified into 5 categories based on average consumption over the 5- and 10-year follow-up as follows: ≤1 cup, 2–3 cups, 4–6 cups and ≥7 cups, with one cup defined as 120 ml. Coffee was categorized into 2 categories based on average consumption in a similar manner, namely <1 cup, and 1 or more cups. These recategorizations were conducted based on the applicability of data to our daily lives and data distribution. Age, sex, and education were also included in the minimal model of multivariable analysis. The fully adjusted model also considered body mass index, smoking status, frequency of alcohol consumption, frequency of sports participation, fish consumption, and history of depression, diabetes mellitus, cancer, and ischemic heart disease. History of depression included both past and current depressive episodes. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated using the lowest categories of tea/coffee consumption as references. Furthermore, stratified analyses by age (using a median split: ≥75 years or younger) and sex were conducted to examine potential modifications of the effect of tea and coffee consumption. All p-values were two-sided, with statistical significance set at a p-value < 0.05. All statistical analyses were performed using R (4.3.2), with the ‘multcomp’ package.30,31
Results
Of the 1155 participants, 58.9% (n = 680) were female. Mean age in 1995 (at first assessment) was 53.3 years, with a standard deviation (SD) of 5.6 years, and ranging from 44 to 66 years. At the time of the cognitive assessment in 2014–2015, 22.4% (n = 259) showed significant cognitive decline, as indexed by multiple-domain MCI or dementia (17.5% [n = 202], and 4.9% [n = 57], respectively). Table 1 detail the participants’ characteristics according to their tea or coffee consumption (Table 1).
Participant characteristics by total green tea or coffee consumption.
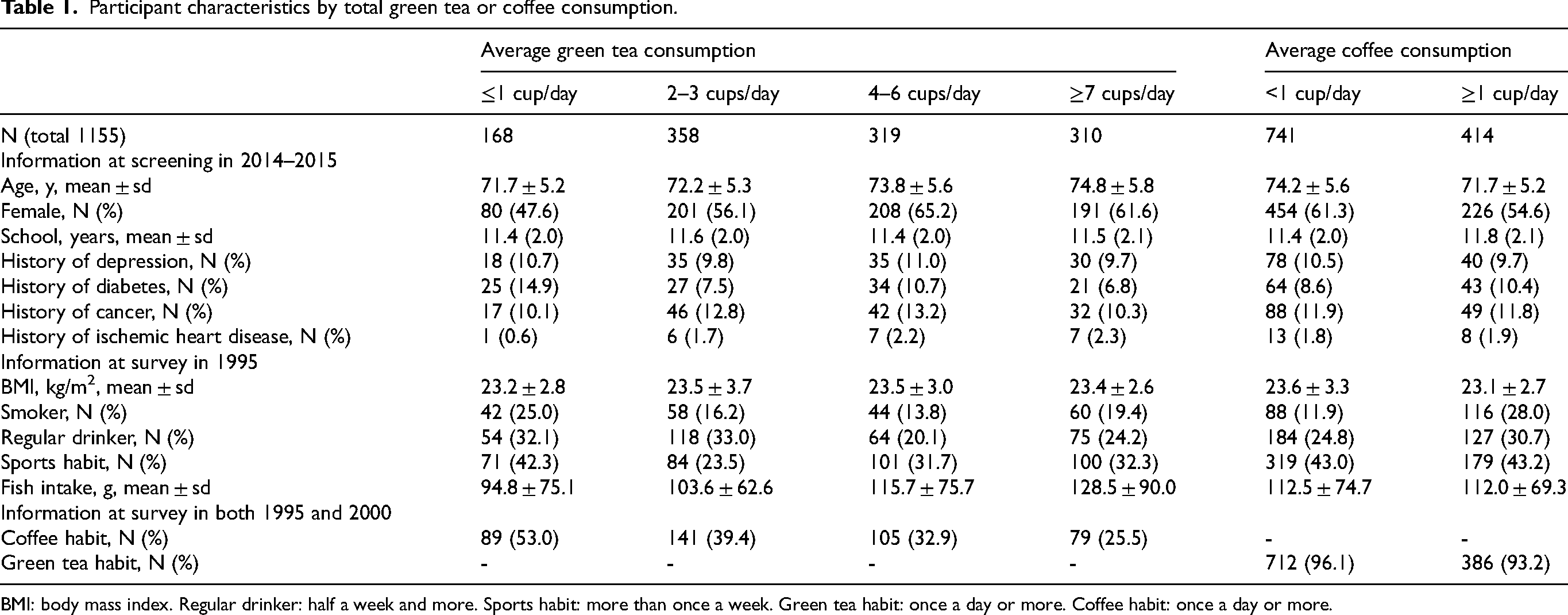
BMI: body mass index. Regular drinker: half a week and more. Sports habit: more than once a week. Green tea habit: once a day or more. Coffee habit: once a day or more.
Tea consumption
Regarding tea consumption (Table 2), our full model confirmed that participants consuming 2–3 cups of tea had a significantly reduced risk of cognitive decline (OR = 0.56, CI: 0.35–0.91). In contrast, higher consumption categories did not show this significant protective effect, indicating a U-shaped relationship between tea consumption and cognitive decline risk.
Risk of significant cognitive decline and green tea consumption.
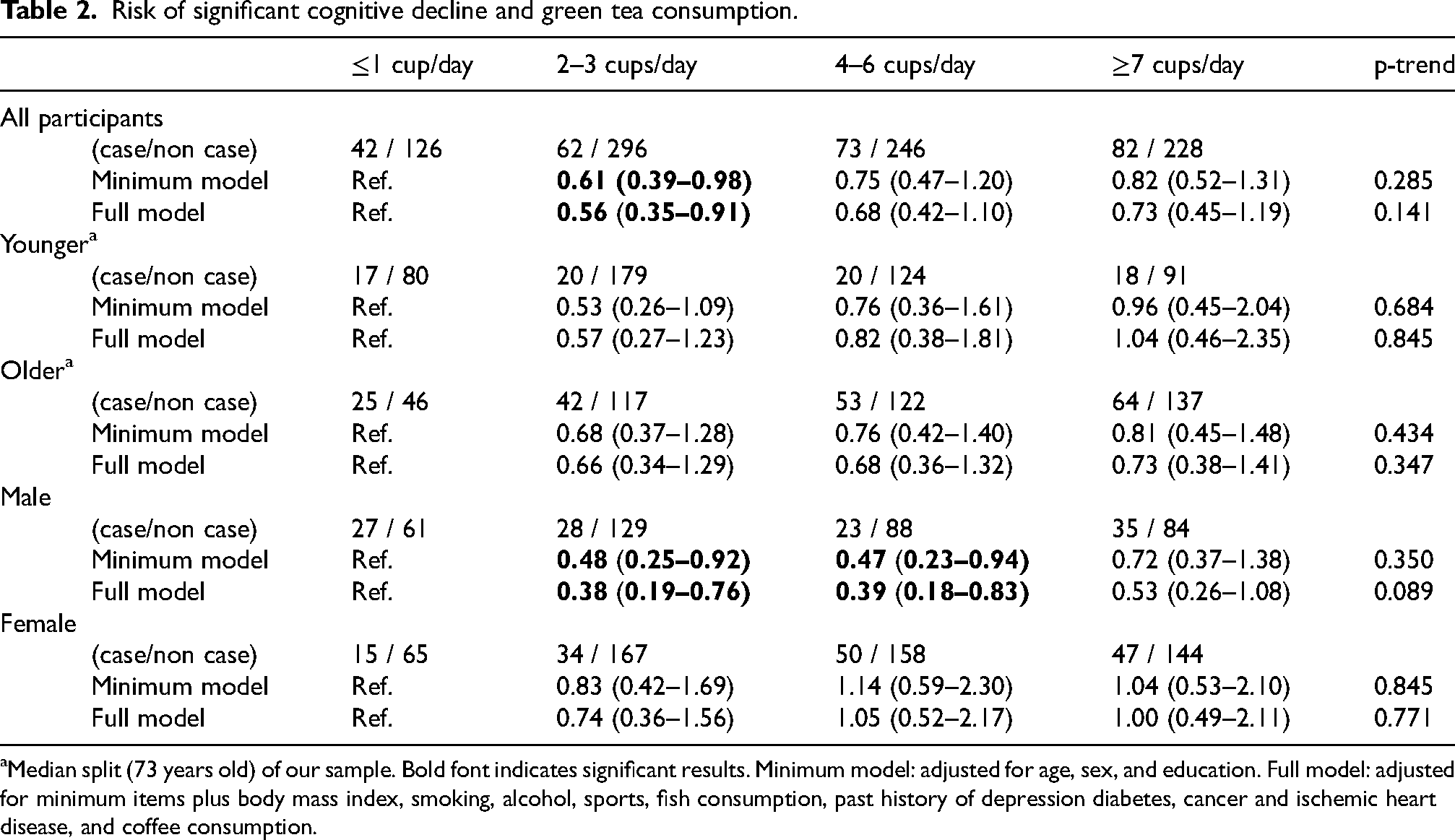
Median split (73 years old) of our sample. Bold font indicates significant results. Minimum model: adjusted for age, sex, and education. Full model: adjusted for minimum items plus body mass index, smoking, alcohol, sports, fish consumption, past history of depression diabetes, cancer and ischemic heart disease, and coffee consumption.
Stratified analysis by age (≥73 years or younger at cognitive assessment, equal to ≥53 years or younger at first assessment in this study) yielded no significant results, likely due to the small number of participants in each category when compared to the total sample analysis. Nevertheless, the trend indicating that 2–3 cups of tea represented the lowest risk category persisted, with the OR being lower in the younger segment of the sample than in the older segment.
Stratified analysis by sex revealed that the significant preventive effect of moderate tea consumption was particularly evident among males (OR = 0.38, CI: 0.19–0.76 for 2–3 cups, and OR = 0.39, CI: 0.18–0.83 for 4–6 cups in the full model). While a similar trend suggested that 2–3 cups represented the lowest risk category in females also, this did not reach statistical significance.
Coffee consumption
Regarding coffee consumption (Table 3), our model indicated that participants consuming more than one cup of coffee were at reduced risk of cognitive decline (OR = 0.72, CI: 0.51–1.01 in the full model), albeit that this did not reach statistical significance.
Risk for significant cognitive decline and coffee consumption.
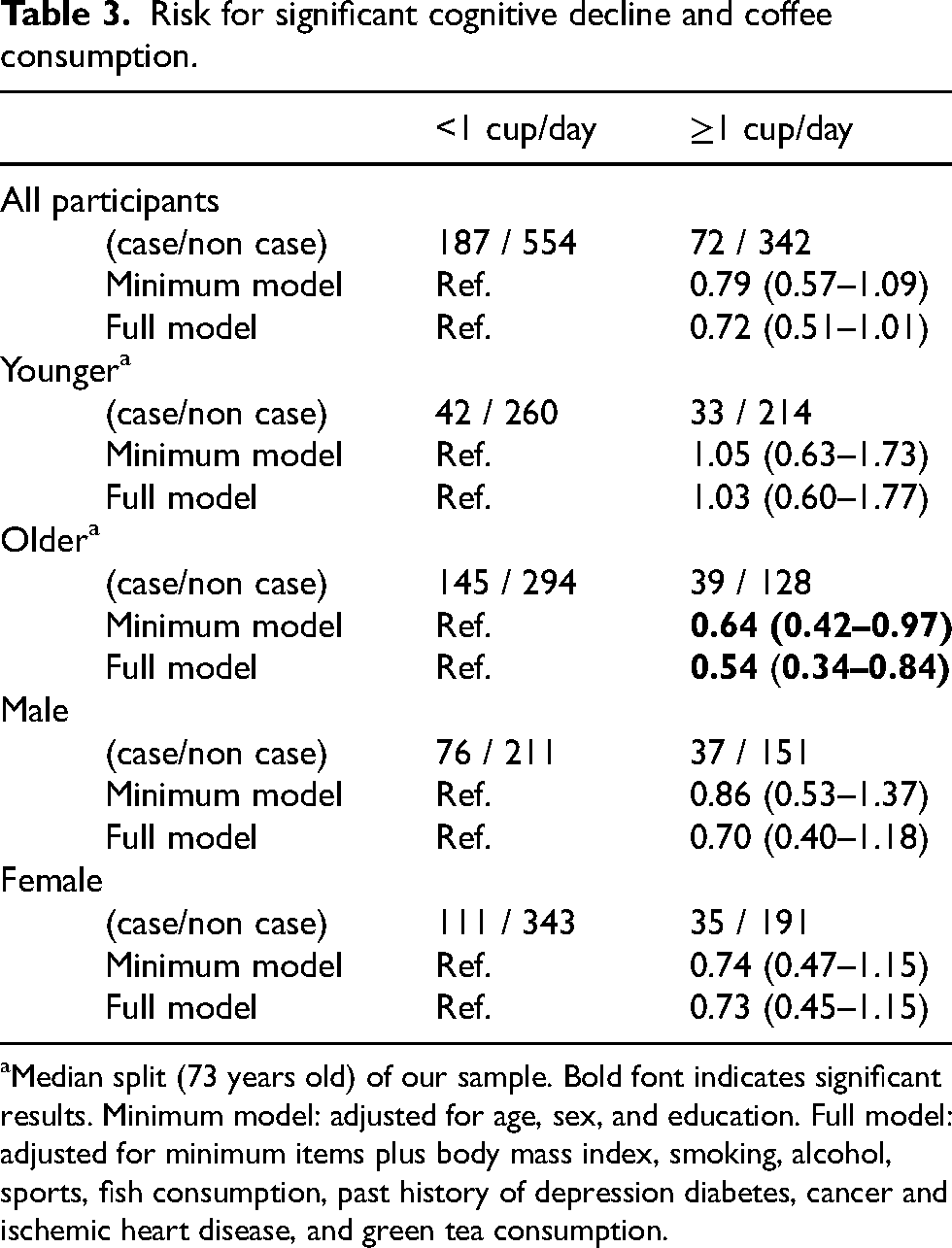
Median split (73 years old) of our sample. Bold font indicates significant results. Minimum model: adjusted for age, sex, and education. Full model: adjusted for minimum items plus body mass index, smoking, alcohol, sports, fish consumption, past history of depression diabetes, cancer and ischemic heart disease, and green tea consumption.
A stratified analysis by age demonstrated a significant preventive impact of coffee consumption, particularly among older participants (OR = 0.54, CI: 0.34–0.84 in ≥1 cup in the full model). Stratified analysis by sex showed no significant results but indicated a trend in which consumption of more than one cup of coffee was associated with reduced risk of cognitive decline in both sexes.
Discussion
To our knowledge, this is the longest cohort study to investigate the protective effect of green tea and coffee against significant cognitive decline. This study, carried out in Japan, a country known for its relatively high green tea consumption, offers a comprehensive analysis of how different levels of tea consumption in middle age are associated with cognitive decline twenty years later. Considering the desirability of preventing early amyloid accumulation and acceleration of vascular ageing, and the limitations of existing medium-term cohort studies, our findings emphasize the importance of modifiable habits in middle age. We demonstrated that consumption of a few cups of green tea/day was associated with reduced risk of cognitive decline. The U-shaped relationship in green tea consumption was consistent with recent cohort studies using the UK biobank data, which also reported a U-shaped relationship between dementia risk reduction and consumption of tea (including black and green tea).8,9 Furthermore, our findings also showed a pronounced effect in males, which is also consistent with previous studies.9,15,32 We also observed a preventive effect of coffee consumption, particularly in older individuals. This finding was consistent with findings from a recent meta-analysis. 7
First, with regard to green tea consumption, the U-shaped relationship in green tea consumption suggests the presence of an optimal quantity for its protective effect. Our finding, notably that the strongest protective effect was afforded with green tea consumption of 2–3 cups, aligns with UK studies showing peak protective effects at 3–4 cups of tea (green and black).8,9 These U-shaped relationships suggest a delicate balance between protective and harmful effects. The protective effects may come from antioxidation, anti-inflammation, vasoprotection, and protection against Aβ accumulation as mentioned in the Introduction.9,16,17 In contrast, the potential detrimental effects of excessive green tea consumption might be attributable to various factors. The caffeine content of green tea is one-third that of coffee. 33 Similar U-shaped relationships have been reported in studies on coffee consumption.7,34 Caffeine in coffee, while beneficial in moderation, can cause sleep problems—a known dementia risk factor—and in high amounts may lead to a reduction in hippocampal volume and increase vascular risks, such as hypertension and hyperlipidemia.35–38 However, Matsushita et al. reported a dose-dependent risk reduction in dementia with caffeine intake, possibly attributable to age differences within the target population. As discussed later, the consumption of coffee, which contains more caffeine than tea, proved to be advantageous for older individuals, suggesting that the benefits and drawbacks of caffeine intake may vary depending on age. Overconsumption can also impair iron absorption, 39 which is related to anemia, a cognitive decline risk. 40 Toxicological effects of green tea have also been reported, especially while consumed on an empty stomach. 41 This might affect frequent tea drinkers. Beyond the contents of green tea, anxiety could serve as a potential confounding factor that could not be controlled in the present study. Anxiety-driven drinking habits can develop as a way to manage thirst, and as coping strategies. 42 These habits and their mutual interaction with the stimulating effects of tea consumption might have affected our findings. It is noteworthy that increased tea consumption was not associated with heightened risk of cognitive decline in the current study, suggesting that the drawbacks of green tea may not outweigh its benefit.
Our stratified analyses by sex showed that the protective effect of green tea was particularly evident in males. This finding is compatible with some epidemiological studies,9,15,32 showing more pronounced associations in males. Moreover, a biological investigation demonstrated a significant association between frequent green tea consumption and low level of t-tau/Aβ in cerebrospinal fluid in males, but not females. 43 This sex difference might be attributable to sex-specific structural and functional brain ageing processes.9,32 In addition, it has been reported that males experience a higher degree of neurodegeneration-related oxidative stress, 44 potentially leading to a greater protective effect from green tea in males. Various female-specific factors associated with AD, such as sex hormones, immune response, and genetic background, may also reduce sensitivity in detecting this association in females. 45 Furthermore, a sex difference was evident in the relationship between all-cause dementia and cardiovascular risk, where a U-sharped relationship was observed in males but not in females. 46
Our stratified analyses by age showed a more pronounced effect in younger participants, albeit that this did not reach significance, possibly due to the small number of participants in each category when compared to the total sample analysis. The protective effect of green tea consumption is more evident in younger than in older study participant groups.15,32 While differences among studies make it challenging to determine the precise optimal timing for dementia prevention in the context of green tea consumption, our findings suggest that the protective effects of green tea might be maximized in mid-life. The age of onset of amyloid accumulation and metabolic syndrome as mid-life risk factors for dementia may represent an ideal time to maximize green tea's protective effects.3,4,47 This may be attributed to the general principle that early intervention yields a better outcome.
Second, regarding coffee consumption, due to the small amount of coffee consumption in our sample, we observed a preventive effect with only one or more cups of coffee and could not identify a U-shaped relationship as reported in other studies.7–9 Our stratified analyses by age clarified that the preventive effect of coffee on cognitive decline was only observed in older participants. A recent meta-analysis reported that the lowest risk associated with coffee consumption was seen exclusively in individuals aged over 60 years, and that there were no significant effects in those under 60 years. 7 This age-specific effect of coffee suggests that its benefits on cognition may be less lasting compared to that of green tea, possibly suggesting that its dominant mechanism is its cognitive stimulation effect. It is noteworthy that our findings persisted after controlling for green tea or coffee consumption, suggesting independent mechanisms that may vary with the participant age.
The strength of our study lies in its long follow-up (20 years), which is consistent with the younger onset and long progressive nature of the pathology of dementia. Furthermore, detailed cognitive assessments, including the distinction of multi-domain MCI, enhanced sensitivity in detecting the beneficial effects of tea and coffee consumption. On the other hand, several limitations also warrant mention. First, cognitive assessment was conducted only once, without determining the onset of cognitive decline. Second, green tea and coffee consumption was not assessed between the 10-year follow-up and our cognitive assessment, leaving a 15-year gap. Third, having a limited number of participants at the time of cognitive assessment within this overall cohort study may have introduced a risk of selection bias. Fourth, APOE, a significant genetic risk factor for dementia, was not evaluated. Further research is necessary to address these limitations.
Conclusion
Our long cohort study suggests that moderate green tea consumption in midlife may have a beneficial effect on preventing dementia, especially in males. The effects of coffee consumption may be advantageous only for older individuals. In light of the pathophysiological progression of dementia from middle age and its wide-reaching societal impact, we believe that our findings provide invaluable insights into the modification of daily life to prevent dementia, beginning in mid-life.
Footnotes
Acknowledgments
We appreciate all the personnel involved in this cohort study. In the initial preparation of this manuscript, ChatGPT-4 was used solely for grammar checks and to enhance the readability of the paper.
Author contributions
Akihiro Koreki (Conceptualization; Data curation; Formal analysis; Investigation; Software; Visualization; Writing – original draft; Writing – review & editing); Shoko Nozaki (Conceptualization; Data curation; Investigation; Methodology; Project administration; Resources; Supervision; Validation; Writing – original draft; Writing – review & editing); Ryo Shikimoto (Conceptualization; Data curation; Investigation; Methodology; Project administration; Resources; Supervision; Validation; Writing – review & editing); Shoichiro Tsugane (Conceptualization; Data curation; Investigation; Methodology; Project administration; Resources; Supervision; Validation; Writing – review & editing); Masaru Mimura (Conceptualization; Data curation; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Validation; Writing – review & editing); Norie Sawada (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Validation; Writing – original draft; Writing – review & editing).
Funding
The Cohort study was originally supported by National Cancer Center Research and Development Fund. The funding agency had no role in the design and conduct of the study; data collection; data management; analysis; interpretation of the data; review or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of conflicting interests
AK has received research support from Eisai outside the submitted work. RS has received speaker's honoraria from Eisai, and Kowa Company, and grants from Univers Foundation, and Sasakawa Health Foundation. MM has received speaker's honoraria from Biogen Japan, Byer Pharmaceutical, Daiichi Sankyo, Dainippon-Sumitomo Pharma, Demant Japan, Eisai, Eli Lilly, Fuji Film RI Pharma, Hisamitsu Pharmaceutical, H.U. Frontier, Janssen Pharmaceutical, Mochida Pharmaceutical, MSD, Mylan EPD, Nippon Chemiphar, Novartis Pharma, Ono Yakuhin, Otsuka Pharmaceutical, Pfizer, Shionogi, Takeda Yakuhin, Teijin Pharma, and Viatris within the past two years. Also, he has received grants from Daiichi Sankyo, Eisai, Fronteo, Shionogi, Takeda, Tanabe Mitsubishi and Tsumura within the past three years outside the submitted work.