
Abstract
Despite growing awareness that disclosing biomarker results to research participants is aligned with ethical principles of researcher-participant partnership, there are currently no widely adopted guidelines for this disclosure in Alzheimer's disease research. We developed a process and tools to deliver biomarker and genetic results to 65 participants of The Memory and Aging Study of the Duke-UNC Alzheimer's Disease Research Center (ADRC). Survey responses of 46 participants were analyzed. We show high participant satisfaction and lower anxiety levels after receiving the results. The developed process and materials provide a template for standardized Alzheimer's disease biomarker result delivery in the research setting.
Keywords
Introduction
Recent advances in Alzheimer's disease research provide access to biomarker and genetic testing 1 and may lead to the development of earlier diagnosis and novel treatments. Individuals with a positive biomarker profile are now a target population for clinical trials even when cognition is unimpaired.2,3
There is now a growing awareness in the Alzheimer's disease research field that disclosure of biomarker and genetic results to research participants is integral to participant rights and study integrity. 4 Emphasis on disclosure coincides with 2024 published recommendations from the National Academies calling for research studies to develop and update policies that increase public access to results of publicly funded research. 5
However, many Alzheimer's disease studies do not disclose biomarker and genetic results to participants. 6 One 2021 publication reported that 43% of Alzheimer's Disease Research Centers (ADRC) disclosed amyloid positron emission tomography (PET), 10% disclosed tau PET and only 7% disclosed APOE status to participants. 7 Among ADRCs, return of results is now becoming a priority. The most recent Request for Applications for National Institute on Aging-funded ADRC's calls for centers to “assure appropriate disclosure of biomarker and other results” 8 and the National Alzheimer's Coordinating Center (NACC) has provided ADRCs with best practice guidance on biomarker disclosure. 9
Previous lack of disclosure may be explained by barriers to returning results including concerns of psychological harm to participants, stigma for the participant within their community, or negative impacts on study participation. 10 There may also be lack of infrastructure or resources to return results. While some evidence exists that disclosing biomarker results in the context of a diagnosis of mild cognitive impairment (MCI) may cause emotional distress, it did not deter people from trial participation. 11 A meta-analysis of 35 studies on biomarker disclosure examined the “expected and experienced” consequences of sharing results concluding that research participants had strong interest in learning biomarker results with no short-term psychological harm. 12 Another study found that result disclosure is a strong driver of participation in research studies, especially for African Americans. 13 Sharing biomarker results also supports diagnostic confidence, and personalized health and lifestyle change. 14 Another important factor in disclosing biomarker results is that it supports participant empowerment in management of healthcare decisions.11,15 This includes managing decisions for the present and for the future, as they prepare for what may come on an emotional and financial level.
There are currently no widely adopted guidelines for disclosure of biomarker results in research studies. 16 Many prior studies on best practices for results delivery were performed in fictitious settings or with proxy patients as test trials.17,18 Resources for training personnel to deliver results are also lacking, perhaps because they have not formalized a standard practice. 19
Several studies explore ethical guidelines for delivering biomarker results to patients with MCI and dementia in clinical settings, mostly in Europe. The European Alzheimer's Disease Consortium recommends result delivery based on the ethical principles of “the right to know” versus “the wish not to know.” In addition, they recommend post-biomarker counseling with education about brain health and treatment. 20 A recent publication outlined a five-step disclosure process based on the authors’ own experience delivering biomarker results. The steps include providing pre-test education, consent to receive the information and providing adequate follow up after disclosure. 21
In this paper we share early experience and evidence from the biomarker delivery process developed for participants in the Duke University and University of North Carolina at Chapel Hill Alzheimer's Disease Research Center (Duke-UNC ADRC) Memory and Aging study, which was launched in 2021. We examine results of our post biomarker disclosure survey to better inform the field on practical biomarker disclosure practices.
Methods
The ADRC study is approved by the Duke University and University of North Carolina at Chapel Hill institutional review boards in accordance with ethical principles and applicable regulatory requirements (Duke University IRB Protocol Number: Pro00103958). The Duke/UNC ADRC emphasized age-related factors across the lifespan that contribute to AD and dementia, and many participants are relatively young and cognitively unimpaired. Written informed consent is obtained from all participants ages 25 to 80 years.
All participants enroll in the Duke/UNC ADRC study and indicate at the time of consent if they wish to receive results of their APOE genetic and biomarker status, including amyloid and tau. There are two age cohorts in the study, a young cohort comprised of participants ages 25–44 and a longitudinal cohort comprised of individuals ages 45–80. Further information about composition of cohorts, inclusion and exclusion criteria and genetic and cerebrospinal fluid (CSF) biomarker testing procedures can be found in the ADRC memory and aging study protocol provided in the Supplemental Material.
Consensus process
Faculty members from neuropsychology, neurology and geriatric psychiatry and study coordinators meet monthly as a formal consensus panel to confer a clinical diagnosis based on review of Uniform Data Set 3.0 (UDS) data. 22 UDS data includes standardized medical history, family history, assessment of cognition and functioning, assessment of mood and behavior, full neurologic exam, as well as a formal neuropsychological battery. Quarterly, after magnetic resonance imaging (MRI) T2 flair, diffusion and susceptibility weighed imaging sequences and CSF biomarker data are available including amyloid (Aβ42/40) and total tau and phosphorylated tau, the consensus panel reviews biomarker results with the clinical diagnosis and confers a clinical-pathological diagnosis based on the standardized UDS format in a formal biomarker consensus meeting.
Data collection
After participants are given their results, a 5-question survey is sent through REDCap to the participant to assess satisfaction and anxiety levels from the delivery process. Answer choices are based on a 1–5 Likert scale with the following values: 1–2 low, 3 medium, 4–5 high. The five questions included: 1) Do you feel the information you received today was helpful? 2) What was your level of anxiety before receiving the results? 3) What was your level of anxiety after receiving the results? 4) Are you pleased with your decision to receive the results? 5) Would you like a follow up call from our study concierge coordinator to discuss your results or any additional concerns? Survey requests are sent twice at 7-day intervals with one opportunity to complete the survey.
Statistical analysis
Descriptive statistics were used to describe participant characteristics. Wilcoxon rank sum test was performed to compare the anxiety levels before and after treatment. These were derived from the 5-question survey sent through REDCap. All the statistical analyses were done using the R Software with publicly available R packages.
Results
Duke/UNC ADRC results disclosure process
A clinician in our study scheduled participants to receive results through a video telehealth platform. Using a slide presentation, the clinician presented content to educate participants about risk factors for cognitive decline, the possible clinical diagnoses and the significance of APOE and CSF biomarkers including amyloid and tau. The clinician reviewed potential anticipated and unanticipated consequences for the participant and their loved ones of learning results including emotional considerations. The clinician then confirmed that participant's desire to learn their APOE and CSF biomarker results as indicated on their consent form. Participants were advised that results are obtained in a research setting where labs are not monitored or certified in the same way as clinical labs and results should be confirmed prior to any treatment decisions. After the participant re-confirmed the desire to receive results, the clinician presented results of APOE and CSF testing on a slide, including whether there was evidence of abnormal brain amyloid or tau based upon CSF amyloid and tau values with the wording “amyloid normal or low” and “tau normal or high” (Supplemental Figure 1). The clinical diagnosis given by the consensus panel is also included with the results. All questions are answered and the disclosure process duration varied from 30 to 40 min. At the conclusion of the session the clinician sent the participant the survey. If participants had abnormal CSF biomarkers in the setting of normal cognition, a clinical trial coordinator followed up with a telephone call about clinical trial options if desired. If participants had abnormal CSF biomarkers in the setting of abnormal cognition, participants were advised to follow up with a clinical provider. If desired, participants were referred to the Duke or UNC Memory Clinics. A study concierge, a position staffed by a person with research and social work background, was available to help participants navigate the process and various challenges. Participants are given a free copy of their MRI images. Any clinically meaningful incidental findings are disclosed immediately. Detailed reports on imaging and neuropsychological assessments are beyond the scope of this disclosure process.
Thus far, 241 participants have consented for the study, of which 178 (73.9%) indicated they wanted to be notified of research results, 3 (1.3%) indicated they did not want to be notified of research results, and 60 (24.9%) indicated they wanted to be asked at the time of notification whether to receive the research results. Here, we present data from the first 65 participants to receive their genetic and biomarker results.
Characteristics of participants who have received results are outlined in Table 1.
Characteristics of study participants by CSF amyloid levels.
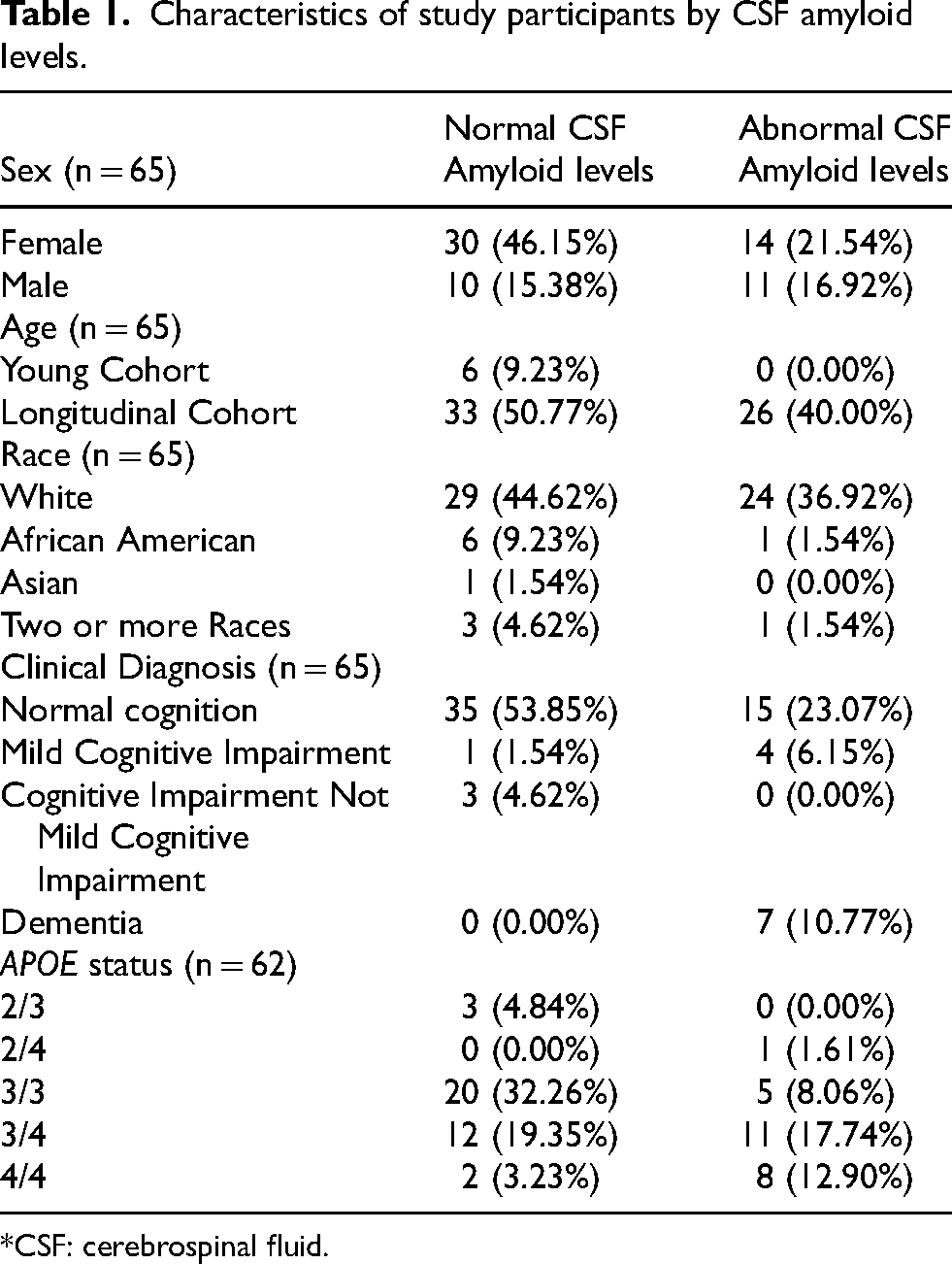
*CSF: cerebrospinal fluid.
The post results survey completion rate was 71% with 46 of 65 participants completing the survey. Approximately 96% (44/46) of respondents were pleased with the decision to receive the results and reported the information helpful (Figure 1).
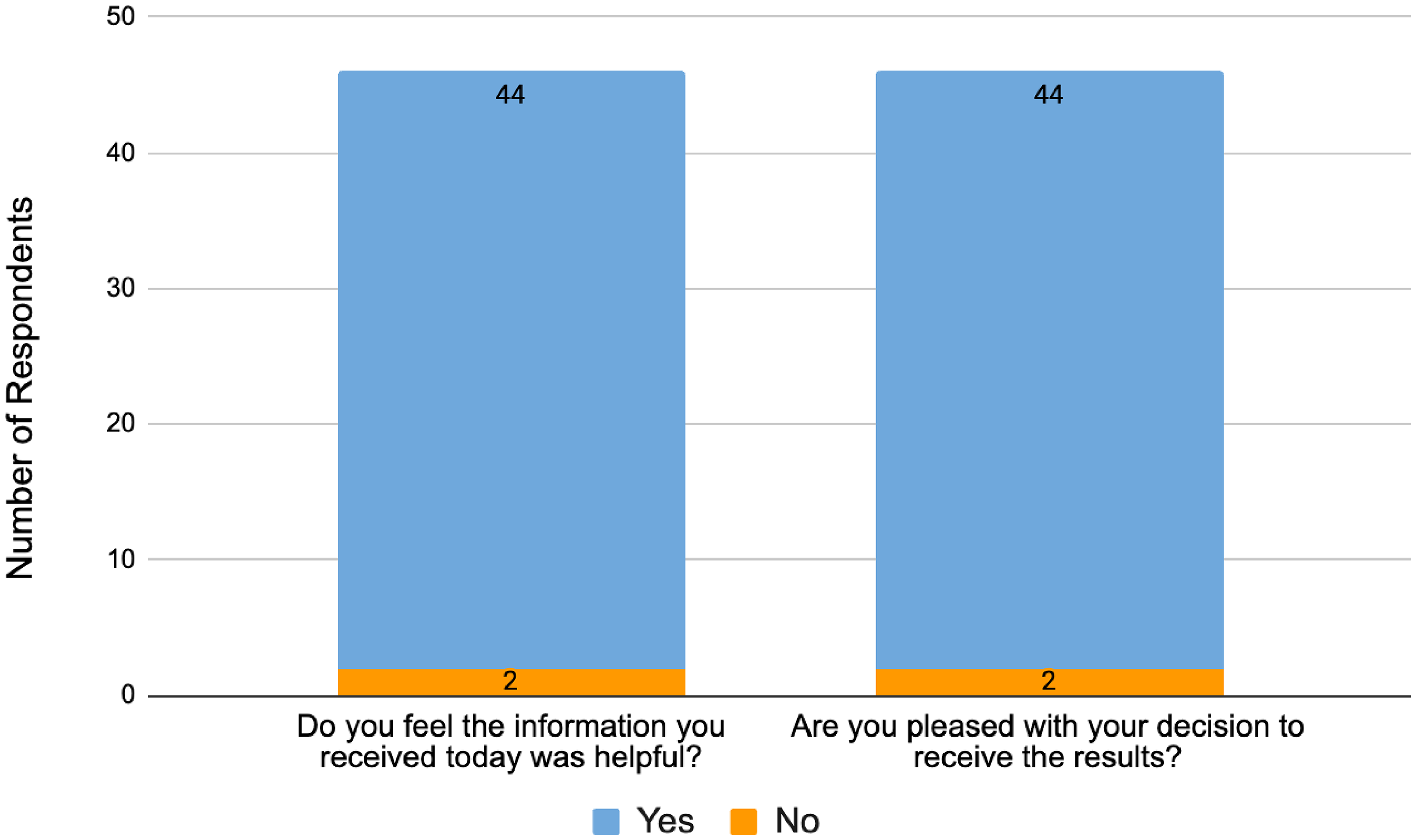
Participants satisfaction with biomarker results disclosure.
Anxiety levels were assessed based upon the following survey values: 1–2 low, 3 medium, 4–5 high (based upon the 1–5 Likert scale answer choices). Anxiety levels decreased after receiving results. 57% (26/46) of participants reported low anxiety before results and 85% (39/46) of participants reported low anxiety after receiving results. While 43% (20/46) of participants reported medium/high level of anxiety before receiving results, only 15% (7/46) reported medium/high level of anxiety after receiving results. 6.5% (3/46) of participants reported an overall increase in anxiety, after receiving results. The mean anxiety level before receiving results was 2.48 and after receiving results was 1.67. The Wilcoxon signed rank test gave a p-value of 0.00018, which indicates significant difference between before and after treatment (Figure 2).
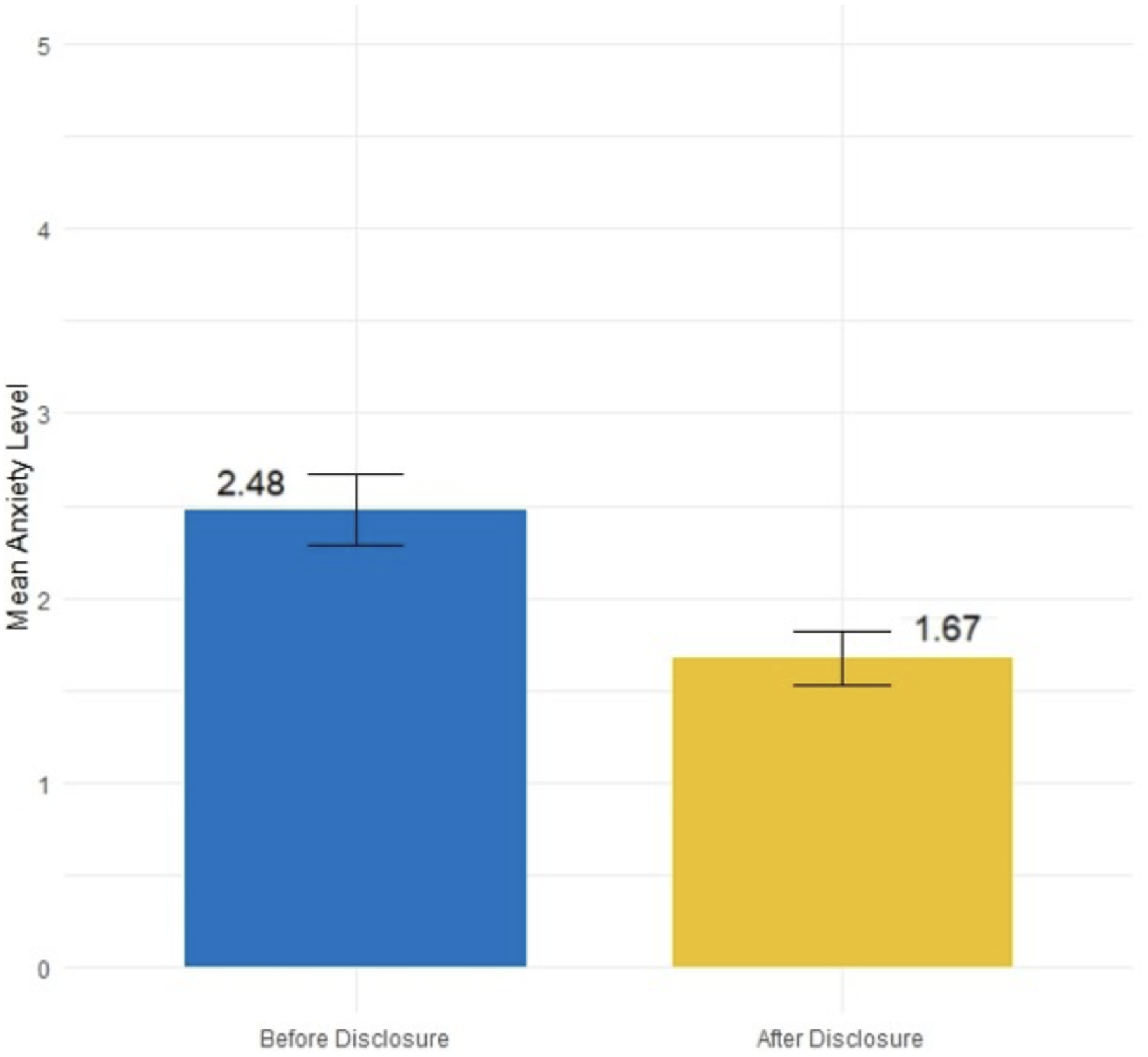
Mean anxiety levels before and after receiving biomarker results reported by participants.
Discussion
Our result delivery process follows recommendations from a recent publication listing transparency, participant choice, adequate training of personnel, innovation of delivery methods, harmonization, and evaluation of the experience as important principles of disclosure. 23 We believe our process and participant experience, specifically delivering and receiving genetic and CSF biomarker results through a telehealth educational presentation, with a 5-question post result session survey adds dimension to the discussion about effective biomarker result delivery in a real-world practical setting. Previous research on disclosure of amyloid PET results indicates that studies can safely share biomarker results to cognitively unimpaired individuals and calls for more research on best disclosure practices and better understanding of psychosocial impacts. 24 In addition, past studies in research settings have used several detailed validated tools to measure depression, anxiety and suicidality and provided intervention as part of a trial. One study concluded that delivery of amyloid positive results in a cognitively unimpaired research population does not cause an increase in psychological stress or adverse effects. 25 We used a brief survey to capture this information in a real-world practical setting. Our participant feedback indicates low anxiety levels after receiving results and high satisfaction with decisions to receive results and the helpfulness of the information. The majority of participants during the consent process elect to learn their results when they become available. The overall decrease in anxiety levels after receiving results even in participants who were given a clinical diagnosis of MCI/dementia, presence of the APOE4 allele, or evidence of amyloid positivity may reflect satisfaction with knowing the information. We postulate that our educational process delivering results and the support we provide after receiving results with a study concierge and referral to clinical care if needed may contribute to the low levels of anxiety after receiving results, but these ideas need further study.
We also postulate that naturally occurring emotions when given unfavorable news may result in the experience of higher anxiety in participants who are APOE4 or amyloid positive than in participants who are APOE4 or amyloid negative. However, we observed overall low levels of post-results anxiety in all participants regardless of genetic or biomarker status, with most participants indicating the information is helpful and useful in understanding their health status. These results align with previous literature on participants’ desire to learn their health status regardless of the outcome.11,14,15,20 As previous research studies indicate, we postulate that disclosure of genetic and biomarker results may provide motivation for our participants to participate in the study although we did not specifically assess this in our study. We continue to improve our process, based on subjective participant feedback. Future efforts will expand our results return to include results of neuropsychological assessments and incorporate additional education about prevention and brain protection strategies. In addition, we want to incorporate a “teach back technique” to ensure participants understand and retain the results information. 17 Our study enrolls many individuals with a family history of dementia but who are unimpaired or have an MCI diagnosis at the time of enrollment. As our cohort ages and we identify new cases of biologically defined Alzheimer's disease, our experience with results disclosure may change. We will continue to use telehealth platforms. This study did not directly assess how the video telehealth method of delivering results was perceived by participants; however, previous studies on disclosure of amyloid PET results supports the use of telehealth as an effective and safe means of delivering results. 26 We may also consider sending our survey at several points in time after the result delivery session to further evaluate delayed anxiety and satisfaction and further assess patient interest in follow up and/or additional support.
Limitations of our study include small sample size of participants that received results; however, there is value in sharing early experience with a new program prior to iterative changes. Although the response rate to the post results survey was rather high at 71%, our results may be subject to a reporting bias. Of note, two respondents did not find the results return to be helpful. Although it was outside the scope of the present study, future work should identify participant- or process-related factors associated with a negative experience with results return. In addition, it is possible that the study is self-selecting participants that are more likely to accept results without excess anxiety. Our participants may sign up for the study to learn more about their genetic or biomarker status and due to family history or symptoms may be prepared for their results at the time of disclosure.
The importance of disclosure of biomarker results to research participants is now widely accepted within the research community, though widespread integration into studies related to cognition is needed and the development and distribution of protocols for biomarker disclosure has been slow. With the rapid advancement in biomarker testing in recent times, guidelines for the disclosure process are due. The process, materials, and survey data presented here provide an example of result delivery in a real-world practical setting.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251315957 - Supplemental material for Genetic and biomarker disclosure process in a memory and aging study
Supplemental material, sj-docx-1-alz-10.1177_13872877251315957 for Genetic and biomarker disclosure process in a memory and aging study by Inbal Mayan, Heidi Roth, Dhrubajyoti Ghosh, Heather E Whitson and Kim G Johnson in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors would like to express gratitude to Leila Hannon for her work on analysis of the results.
Author contributions
Inbal Mayan (Conceptualization; Data curation; Formal analysis; Writing – original draft; Writing – review & editing); Heidi Roth (Formal analysis; Writing – original draft; Writing – review & editing); Dhrubajyoti Ghosh (Formal analysis; Methodology; Software; Validation); Heather Whitson (Conceptualization; Formal analysis; Methodology; Writing – review & editing); Kim Johnson (Conceptualization; Formal analysis; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing).
Funding
This study did not receive any direct funding. Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number P30AG072958. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
Kim G. Johnson reports the following disclosures: Contributor to C2N Diagnostics QUIP II study on Precivity AD2 test; PI of the AHEAD A3-45 clinical trial Combination anti-amyloid therapy for preclinical Alzheimer's disease; PI of clinical trial sponsored by LEXEO Pharmaceuticals - A 52-Week, Multicenter, Phase 1 Open-label Study to Evaluate the Safety of LX1001 in Participants with APOE4 Homozygote Alzheimer's Disease; Consultant, University of Southern California; Speaker, Eisai Anti-Amyloid Education Event; Co-Investigator, Automated High-purity Exosome isolation-based AD diagnostics system (AHEADx); Research participant, Cleveland Clinic Center for Bioethics Research Results study.
The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.