
Abstract
Background
Hearing loss is a potentially modifiable risk factor implicated in dementia, with recent research suggesting an association between age-related hearing degradation and dementia.
Objective
This study aims to elucidate the relationship between hearing decline and dementia risk.
Methods
We analyzed data from 511,953 subjects from the Korean National Health Insurance Service-Senior Cohort (2002–2008). After excluding those diagnosed with dementia in 2002, 511,935 subjects were included. Subjects with hearing loss between 2002 and 2008 were selected and matched with a control group without hearing impairment based on age and gender. Statistical analyses, including Pearson's chi-squared test and the Cox proportional hazards model, were conducted, controlling for confounding variables such as household income and residential area. Subgroup analysis was also performed for Alzheimer's disease and vascular dementia.
Results
Subjects with hearing loss had a 1.245 times higher risk of all-cause dementia compared to those without hearing loss (adjusted hazard ratio over 3 years, 95% CI = 1.201–1.290), adjusting for gender, age, residence, and income. The adjusted hazard ratios for Alzheimer's disease over 3, 5, 7, and 10 years from the index date were 1.259 (95% CI = 1.211–1.308), 1.258 (95% CI = 1.208–1.310), 1.269 (95% CI = 1.215–1.325), and 1.235 (95% CI = 1.170–1.304), respectively. No significant association was found for vascular dementia, except for 3 years.
Conclusions
Hearing loss consistently increased the risk of all-cause dementia and Alzheimer's disease across timespans, suggesting a complex link between hearing loss and neurodegenerative diseases. These findings highlight the importance of early intervention and cognitive monitoring for individuals with hearing loss.
Introduction
As people grow older, they often face challenges that can impede their personal well-being, social connections, self-reliance, and efficiency and cognitive and sensory degenerations are common companions of aging. About 10% of the general population struggles with hearing loss significant enough to hinder effective communication that clinically significant hearing impediments, capable of affecting regular conversations, are prevalent in approximately two-thirds of individuals aged 70 and above. 1 Alongside hearing decline, cognitive decline is also a natural part of the aging process. 2 These cognitive changes manifest diversely across individuals and can span from standard aging repercussions to conditions like mild cognitive impairment (MCI), Alzheimer's disease (AD), and other associated dementias. 3
Among the spectrum of cognitive decline, dementia stands as a widespread neurodegenerative disease, inflicting significant social and economic impacts that about 1% of those between 60–70 years and 6–8% of individuals aged 85 and above globally receive a dementia diagnosis annually. 4 Given its progressive nature, signs of dementia often manifest over 20 years before an official diagnosis and the most efficient preventive measures against dementia involve addressing its modifiable risk factors. 5 Moreover, recent insights point at hearing loss as a potentially amendable risk factor 6 as existing literature indicates a correlation between more severe hearing deficits and cognitive decline, poorer outcomes in auditory and non-auditory assessments, accelerated cognitive degradation, and emerging dementia cases.7–9 Past research has indicated a potential link between age-induced hearing degradation and dementia. Hearing loss has been identified as a significant risk factor for dementia in several large-scale population studies.10,11 These studies indicate that individuals with hearing impairment are more likely to develop dementia compared to those with normal hearing. Interventions targeting hearing impairment, such as hearing aid use and auditory rehabilitation programs, may help reduce cognitive decline, suggesting a potential avenue for mitigating dementia risk. 12 Additionally, associations between hearing loss and cognitive impairment have been observed across various populations and study designs,13,14 highlighting the need for further research in this area.
In this study, we analyzed a large-scale national elderly cohort of over 500,000 participants, monitored for up to 17 years (2002–2019), to determine if hearing loss consistently elevates dementia risk across different timespans following the diagnosis. Compared to previous studies, which often had limited follow-up periods or smaller sample sizes, our research leverages comprehensive national health insurance claims data, offering several key advantages: (1) a nationally representative elderly sample covering a wide demographic range, (2) audiometric and cognitive assessments that were consistently applied during the diagnostic process to ensure the reliability and accuracy of identifying both hearing loss and dementia, (3) detailed longitudinal medical history, and (4) an approach to evaluate the dementia risk after a variety of timespans of 3, 5, 7, and 10 years post-index date. This approach enables us to evaluate the reliability of the association between hearing loss and dementia.
Methods
Data acquisition
The study data set was obtained from the Korean National Health Insurance Service (NHIS), which was founded in 2000 as a single-insurer system. The formation of this system involved integrating more than 366 medical insurance organizations that were present in South Korea, and storing and converting the medical records of individuals into a national database called the National Health Information Database. This database contains personal information, demographics, and medical treatment data for South Korean citizens who were categorized as insured employees, insured self-employed individuals, or medical aid beneficiaries.
The NHIS Senior Cohort (NHIS-SC) is a research database for the elderly constructed in a cohort format for investigating the risk factors and prognosis of geriatric diseases. The NHIS-SC used a simple randomization method to extract data from 511,953 persons, representing 8% of the 6.4 million population aged between 60 and 80 years in 2008 who had maintained their health insurance and medical-care status for the entire year of 2008, followed from 2002 to the end of December 2019. The members of the NHIS-SC comprise 18-year cohort (2002–2019) whose socioeconomic variables (residence area, year and month of death, cause of death, and income level) and medical treatments (health examinations, medical-care history, and medical-care institutions) are tracked. These data enable long-term observations and can be used to investigate association between hearing loss and the risk of dementia. The cessation of follow-up for individual subjects in the NHIS-SC data set was determined by their death. The elderly subjects sampled in 2008 for the NHIS-SC continue to drop out as they die, and there has been an influx of 8% of 60-year-old elderly subjects every year since 2009.
Diseases are registered in the NHIS-SC based on the sixth edition of the Korean Classification of Disease, which is modified from the 10th revision of the International Classification of Disease (ICD-10) for use in the NHIS and medical-care institutions in South Korea. This study was conducted using NHIS-SC (NHIS-2023-2-260) and approved by the Institutional Review Board of Kangwon National University Hospital (approval no. KNUH-2023-08-014).
Subjects
This study analyzed a population-based matched cohort constructed using the NHIS-SC. Hearing loss was defined based on the ICD-10 classification codes (H90) combined with pure tone audiometry (PTA) (F6341-F6347) or speech audiometry (F6300-F6301) for the first diagnosis for medical expense claims between January 1, 2002 up to December 31, 2008. The index date for these subjects was defined as the date when hearing loss was first diagnosed between 2002 and 2008. All-cause dementia was defined based on the ICD-10 classification codes (F00, F01, F02, F03, or G30) used with anti-dementia drugs (donepezil, galantamine, rivastigmine, or memantine) for the first or second diagnosis and dementia test such as Mini-Mental State Examination (F6216) or Global Deterioration Scale (F6221) or MMSE and Clinical Dementia Rating (F6222) for medical-expense claims through an outpatient clinic. Alzheimer's dementia (F00, G30) and vascular dementia (F01) were also defined in the same way.
Among 511,953 subjects registered in 2008, we excluded subscribers with dementia diagnosis in 2002 (n = 18). For each subject in the case group with hearing loss between 2002 and 2008, five subjects without hearing loss were randomly selected and matched for age and gender at the index date as controls. After excluding subjects without information of income and region (n = 750), the resulting hearing loss patients (n = 34,397) became the case group. Considering the characteristics of dementia, dementia diagnosed after k (k = 3,5,7,10) years from the index date was observed as the event of interest (Figure 1).

Scheme of hearing loss subject selection. We defined hearing loss and all-cause dementia based on the ICD-10 classification codes. After selecting the case and the matched control group, we applied timespans of k = 3, 5, 7, and 10 years from the diagnosis of hearing loss between 2002 and 2008.
In addition to diagnoses, other variables such as gender, age, household income, and residence area were extracted on the day closest to the index date. Household income was defined as yearly household income and classified into 4 categories (0–2 for low, 3–5 for middle low, 6–8 for middle high, 9 and more for high). The residence areas were classified into the following two regions according to their geographical location: (1) Seoul metropolitan area (Seoul, Incheon, and Gyeonggi-do) and (2) other areas (Busan, Daegu, Ulsan, Gangwon-do, Gyeongsangbuk-do, Gyeongsangnam-do, Gwangju, Daejeon, Chungcheongbuk-do, Chungcheongnam-do, Jeollabuk-do, Jeollanam-do, and Jeju).
Statistical analysis
We used Pearson's chi-squared test to compare differences in the proportions of dementia between groups according to gender, age, residence area, and household income. The Cox proportional hazards model was used to calculate the adjusted hazard ratio (HR) and 95% confidence interval (CI) to determine whether hearing loss was a significant risk factor for dementia after adjusting for gender, age, residence area, and household income. Survival time was defined as the duration from the index date up to a diagnosis of dementia or up to the censoring due to death, lost to follow-up, or the end of the study on December 31, 2019, whichever occurred first, after a certain timespan. Those who were dead, lost to follow-up, or were never diagnosed with a dementia by the end of the study after the index date were treated as censored. Subjects who diagnosed with dementia before k years from the index date were treated as censored. Also, the subscribers with dementia before the index date and those who were diagnosed with hearing loss after index date in the control group were treated as censored. Kaplan-Meier survival curves were estimated, and the log-rank test was performed to compare differences in the curves between two groups. Subgroup analysis was performed for the risk of Alzheimer's dementia (AD) (F00, G30) and vascular dementia (VaD) (F01) respectively. In this case, AD and VaD were treated as competing risks in such a way that the other was treated as censored for the survival analysis of one dementia. The statistical analyses were performed using the SAS for Windows statistical package (version 7.1, SAS Institute, Cary, NC, USA).
Results
All-cause dementia
Both prevalence and incidence rates of hearing loss in this cohort were calculated in Table 1. This presents the prevalence and incidence of hearing loss in our study cohort from 2003 to 2019. Prevalence is calculated as the total number of hearing loss cases per 100,000 population for each year. Incidence is calculated as the number of new (de novo) hearing loss cases per 100,000 person-years for each year. Both crude and age-standardized rates are provided. The prevalence of hearing loss showed an increasing trend over time, rising from 834.9 per 100,000 in 2003 to 3597.2 per 100,000 in 2019 (crude rates). The age-standardized prevalence similarly increased from 887.4 to 3488.4 per 100,000 over the same period. Incidence rates also demonstrated an upward trend. The crude incidence rate increased from 791.4 per 100,000 person-years in 2003 to 2210.4 per 100,000 person-years in 2019. Age-standardized incidence rates showed a similar pattern, rising from 839.4 to 2157.0 per 100,000 person-years. ‘De novo’ in this context refers to newly diagnosed cases of hearing loss each year.
Prevalence and incidence of researched subjects with hearing loss in used cohort.

Population in 2008 is used as a standard population. Prevalence and incidence rate per 100,000 person-years and trend indicates the results of Cochran-Armitage trend analysis. The mean of * is that P value for the total trend is less than 0.0001. The abbreviation of N indicates the frequency.
The basic characteristics of the case and control subjects before applying the timespan from the index date are summarized in Table 2. The data showed that subjects with hearing loss have higher household income than those in control group. Note that the proportions of men and women with hearing loss were similar at 0.1671 and 0.1672, respectively.
Baseline characteristics in population matched cohort.

p value acquired from Pearson's chi-squared test.
*The household income of 0 in lowest groups receive medical aid in their life.
The data with the timespan of 3 years from the diagnosis of hearing loss showed that 3823 subjects among those with hearing loss (11.11%) and 13,769 subjects among those without hearing loss (8.04%) were diagnosed with all-cause dementia (Tables 3 and 4). Females were more likely to have all-cause dementia than males and older subjects were more likely diagnosed with all-cause dementia than younger ones. Subjects who live in non-metropolitan are more likely diagnosed with all-cause dementia. Cox regression analysis showed that subjects with hearing loss showed a 1.245 times higher risk of all-cause dementia than those without hearing loss (adjusted HR, 95% CI = 1.201–1.290) after adjusting for gender, age, residence area, and household income. The risk of all-cause dementia in females was 1.411 times higher than that in males (adjusted HR, 95% CI = 1.367–1.457). The risk of all-cause dementia increased as age increased, but as household income decreased. Subjects living in non-metropolitan area showed a 1.310 times higher risk of all-cause dementia than those in metropolitan area (adjusted HR, 95% CI = 1.269–1.351) (Table 3). Note that each data with different timespans showed the qualitatively similar results as the data with the timespan of 3 years (Table 3, Supplemental Table 1). The Kaplan-Meier survival curves for the risk of all-cause dementia differed significantly between the two groups, and the risk of all-cause dementia was significantly higher in the case group than the control group (log-rank p < 0.0001) (Figure 2). The adjusted HRs for all-cause dementia with the timespan of 5 years, 7 years, and 10 years from the index date were 1.239 (95% CI = 1.193–1.287), 1.250 (95% CI = 1.200–1.302), and 1.222 (95% CI = 1.161–1.286), respectively (Table 4). The adjusted HRs for all-cause dementia showed the highest value with the timespan of 7 years. They were significant in data with all timespans after adjusting for gender, age, residence area, and household income.
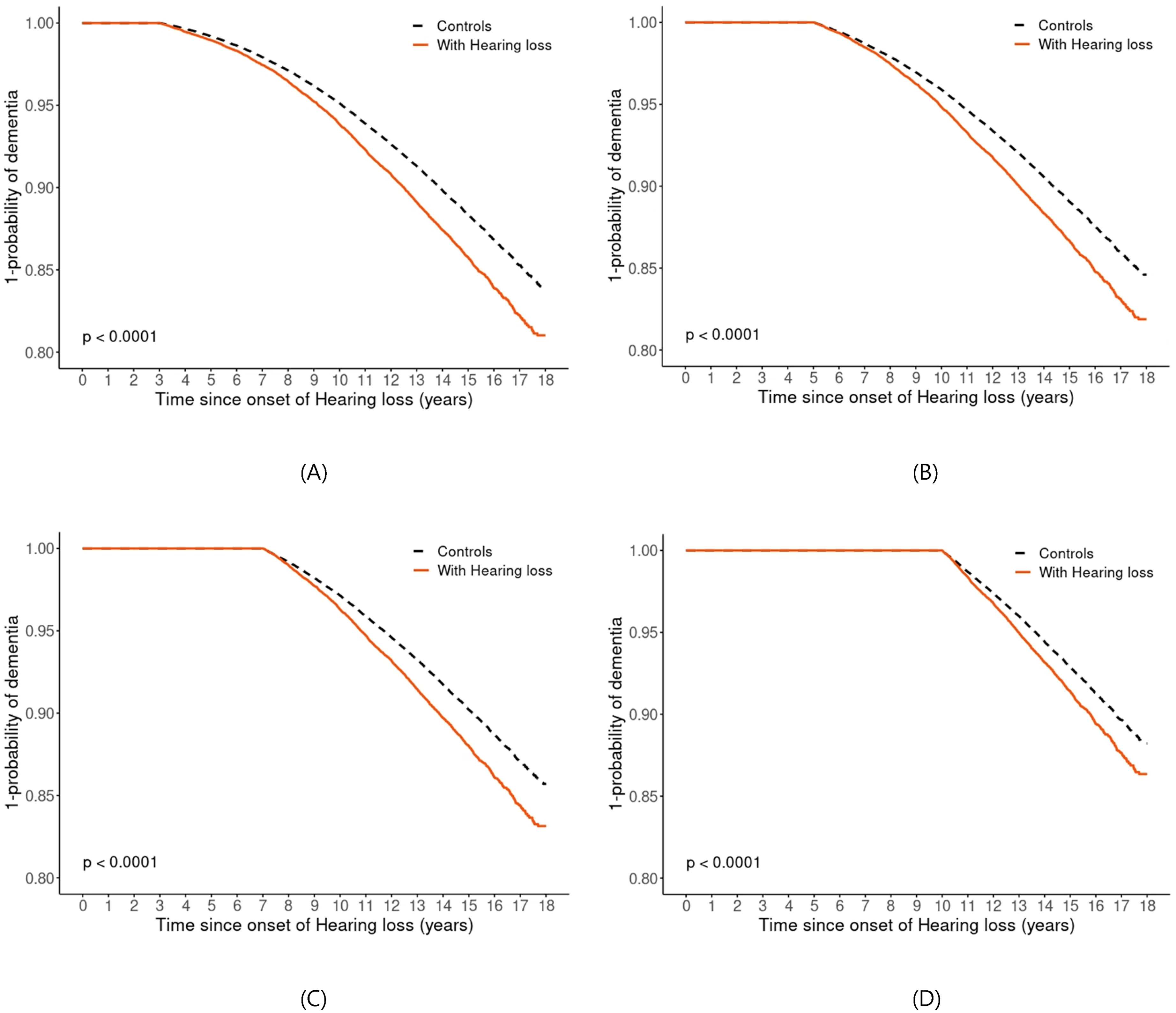
Kaplan-Meier survival curves by different timespans. The results of Kaplan-Meier survival analysis curves for all-cause dementia subjects with hearing loss and control groups in used cohort with different timespan of 3 years (A), 5 years (B), 7 years (C), and 10 years (D), respectively. p is p-value from the log-rank test.
The Cox proportional-hazards results for all-cause dementia with the timespan of 3 years after the first diagnosis of hearing impairment.
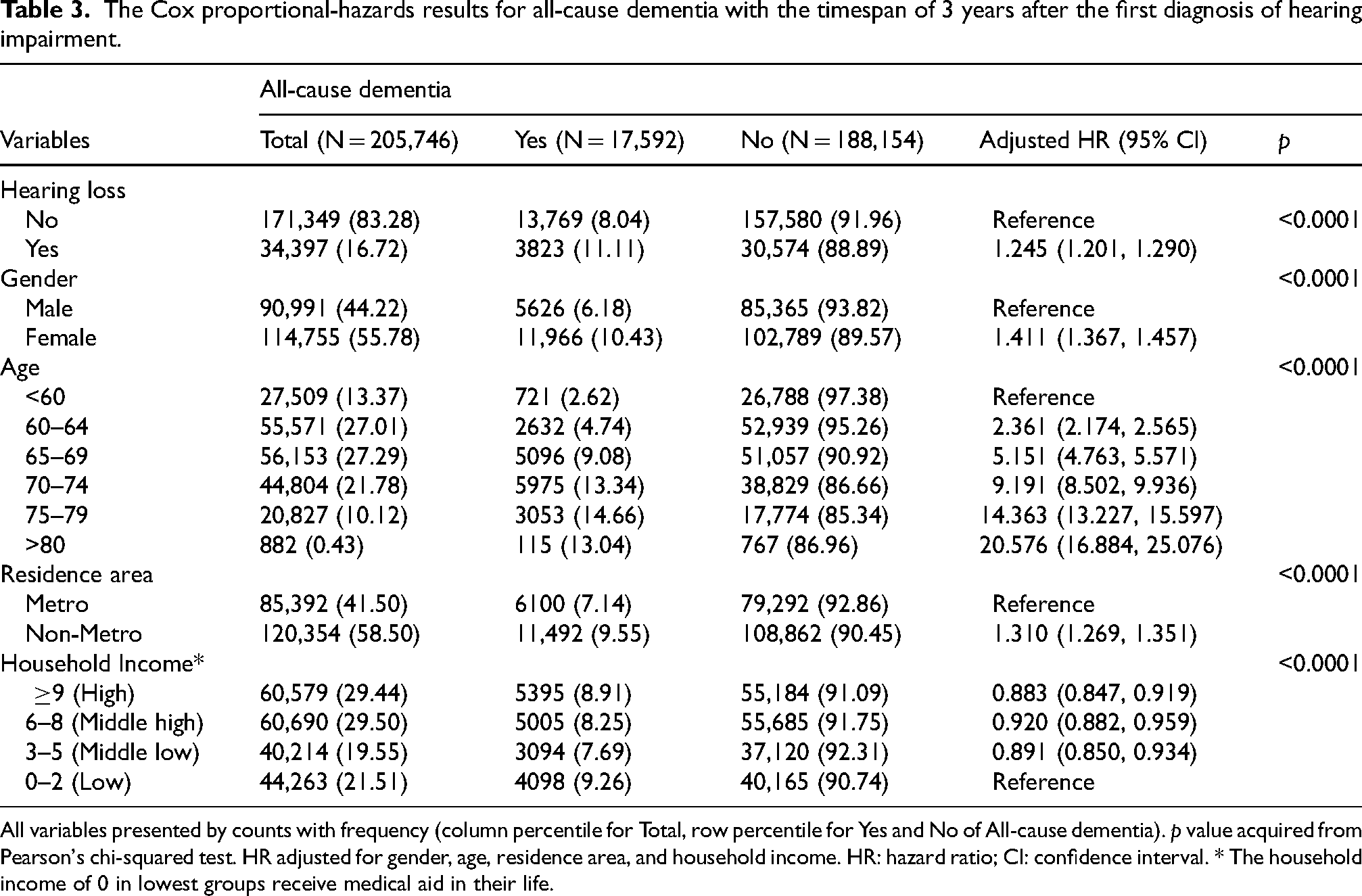
All variables presented by counts with frequency (column percentile for Total, row percentile for Yes and No of All-cause dementia). p value acquired from Pearson's chi-squared test. HR adjusted for gender, age, residence area, and household income. HR: hazard ratio; CI: confidence interval. * The household income of 0 in lowest groups receive medical aid in their life.
Results from the Cox proportional-hazards model for all-cause dementia for the data with the timespan of k years (k = 3,5,7,10) after the first diagnosis of hearing loss.
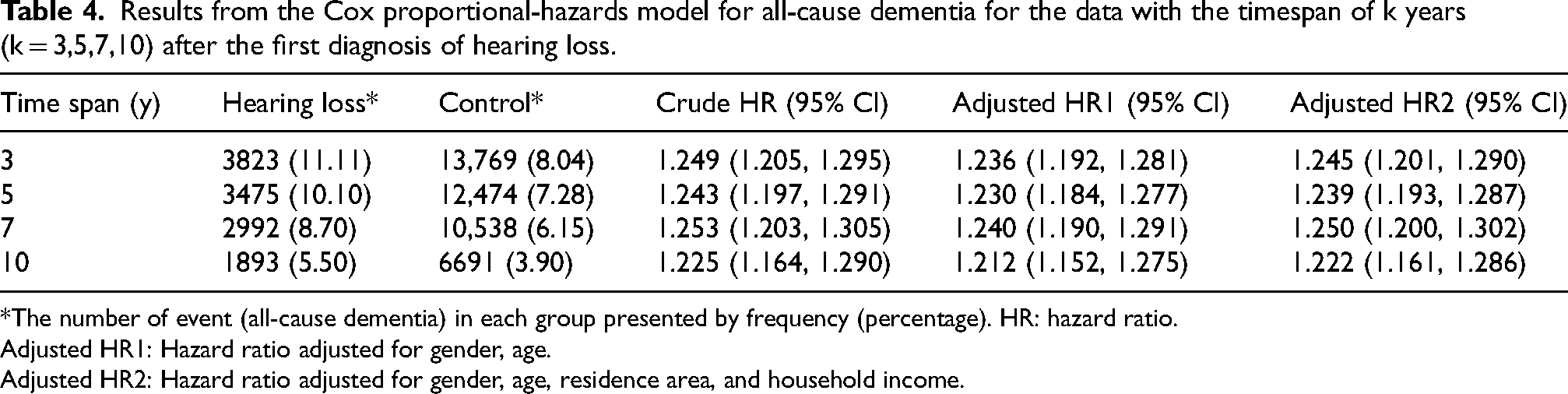
*The number of event (all-cause dementia) in each group presented by frequency (percentage). HR: hazard ratio.
Adjusted HR1: Hazard ratio adjusted for gender, age.
Adjusted HR2: Hazard ratio adjusted for gender, age, residence area, and household income.
Alzheimer's dementia and vascular dementia
Table 5 showed that the adjusted HRs for AD (F00, G30) in data with the timespan of 3 years, 5 years, 7 years, and 10 years from the index date were 1.259 (95% CI = 1.211–1.308), 1.258 (95% CI = 1.208–1.310), 1.269 (95% CI = 1.215–1.325), and 1.235 (95% CI 1.170–1.304), respectively, which shows the highest with the timespan of 7 years. The adjusted HRs for VaD (F01) in data with the timespan of 3 years, 5 years, 7 years, and 10 years from the index date were 1.167 (95% CI = 1.040–1.309), 1.114 (95% CI = 0.985–1.260), 1.129 (95% CI = 0.987–1.292), and 1.084 (95% CI = 0.911–1.290), respectively, The adjusted HRs for AD were significant in data with all timespans after adjusting for gender, age, residence area, and household income, showing the same results as all-cause dementia. However, the adjusted HRs for VaD were found significant only for the data with timespan of 3 years (Table 5, Supplemental Tables 2 and 3).
Results from the cox proportional-hazards model for Alzheimer's dementia and vascular dementia in data with the timespan of k years
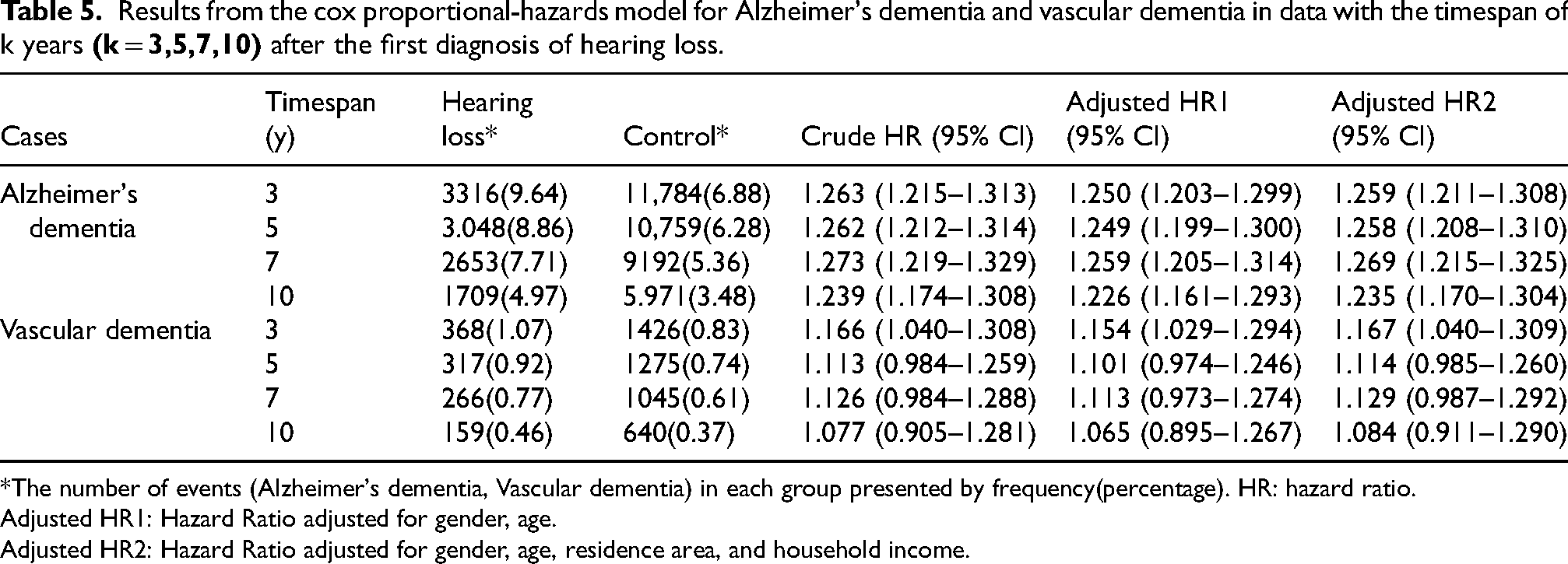
*The number of events (Alzheimer's dementia, Vascular dementia) in each group presented by frequency(percentage). HR: hazard ratio.
Adjusted HR1: Hazard Ratio adjusted for gender, age.
Adjusted HR2: Hazard Ratio adjusted for gender, age, residence area, and household income.
Discussion
Our study suggested that hearing loss may increase the risk of all-cause dementia in elderly subjects over diverse timespan post-diagnosis as hearing loss. Notably, this increased tendency was evident in AD but not in VaD, suggesting a specific vulnerability associated with AD.15,16 The clinically novel implication of this study is that it is worthwhile to focus on the cognitive decline from the nascent stages of hearing loss, as this interval is characterized by elevated risk of progression to dementia.17,18 To the best of our knowledge, this study is the first investigation to demonstrate how the risk of dementia maintained with time since hearing loss onset according to a variety of timespan, providing vital insights into stability and reliability of the association between hearing loss and the risk of developing dementia. Our study aligns with previous research indicating that hearing loss substantially increases the risk of dementia and AD. A meta-analysis involving 726,900 participants across fourteen cohort studies has shown that hearing loss significantly elevates the risk of dementia by 59% when compared to individuals without hearing loss. 6 This finding is further substantiated by recent large-scale population-based cohort studies (n = 942,567 and n = 573,088) with extended follow-up periods, which consistently demonstrated increased dementia risk among those with hearing impairment.10,11 The relationship between hearing loss and cognitive decline has been observed across different study designs, from cross-sectional analyses of middle-aged adults (n = 62,072) showing immediate associations with cognitive impairment, 13 to longitudinal studies revealing impacts on both cognitive function and overall functional status. 14 Furthermore, the analysis indicates that hearing loss more than doubles the risk of AD, which is in line with our study. Notably, emerging interventional evidence from a recent randomized controlled trial (n = 977) suggests the potential of hearing rehabilitation in mitigating cognitive decline. 12 However, the Marinelli et al. study revises this perceived association, showing no direct link between objective measures of hearing loss and dementia onset, 19 though it highlights that subjective hearing complaints are significantly related to dementia development.20,21 This distinction points to the importance of considering central auditory processing and its impact on cognitive health, suggesting that the relationship between hearing abilities and dementia might be more complex than previously understood. The 2024 Lancet Commission meta-analysis and recent large-scale cohort studies have strengthened the evidence base linking hearing loss to increased dementia risk. The Commission's findings, which report a hazard ratio (HR) of 1.37 for dementia risk among individuals with hearing loss, align with the direction and magnitude of our findings. 22 By examining a large, nationally representative cohort over multiple timespans, our study extends these findings and reinforces the clinical relevance of early hearing intervention as a preventive strategy against cognitive decline. The association between hearing loss and dementia can be explained through several interconnected hypotheses. First, hearing loss may lead to reduced cognitive stimulation, as individuals with hearing impairments might engage less in conversations and other brain-stimulating activities, potentially accelerating cognitive decline.23,24 Second, the increased listening effort required to understand speech with hearing loss can cause cognitive overload, reducing the brain's resources for other cognitive processes and increasing dementia risk. 25 Third, information degradation due to poor-quality auditory input might lead to incorrect or incomplete information processing by the brain, negatively impacting cognitive functions over time. 26 Additionally, hearing loss can cause social isolation, a known risk factor for cognitive decline and dementia, as individuals withdraw from social interactions due to communication difficulties.27,28 Common underlying pathologies, such as neurodegenerative diseases, might simultaneously affect both the auditory system and cognitive brain regions. 29 Hearing loss is also associated with depression and reduced self-efficacy and less physical activities those linked to higher dementia risk. 30
A recent cross-sectional study investigates the association between hearing loss, hearing aid use, and dementia prevalence among older adults in the US, utilizing data from the National Health and Aging Trends Study found that moderate to severe hearing loss was linked to a higher prevalence of dementia compared to normal hearing. 7 However, hearing aid use among those with moderate to severe hearing loss was associated with a lower prevalence of dementia.20,31,32 A recent systematic review and meta-analysis of 31 studies comprising 137,484 participants found that the use of hearing restorative devices was associated with a 19% reduction in hazards of cognitive decline, including incident dementia, over follow-up periods ranging from 2 to 25 years. 33 Additionally, hearing aid use was linked to a 3% improvement in short-term cognitive test scores assessing general cognition. These benefits were observed across various cognitive domains and were consistent in subgroup analyses by geographic region and study quality. The cognitive benefits of hearing aids may be attributed to reduced cognitive load, improved social engagement, and mitigation of cortical atrophy associated with auditory deprivation. 34 This suggests that improving access to hearing care and hearing aids could be a significant public health measure to reduce dementia prevalence. Regarding association with hearing loss and cause-specific dementia, the differential outcomes observed between AD and VaD represent a noteworthy aspect of this study's findings. AD is neurodegenerative disease as major cause of dementia21,35 and notably affects the ability to analyze complex auditory environments, which is a distinct feature of its pathology.36–38 This issue, which goes beyond basic sound perception or cognitive deficits, may indicate AD early on and is associated with difficulties in recognizing auditory objects.39,40 This auditory dysfunction is tied to neurodegeneration in key brain networks, underlining a significant disruption in auditory processing as part of AD's impact.41,42 The complex interplay between ‘peripheral’ and ‘central’ hearing influenced by both cochlear sensitivity and brain processing. 43 PTA is traditionally seen as measuring ‘peripheral’ hearing but is also impacted by cognitive functions and non-cochlear brain pathologies44–46 that reflects the significant interplay between central and peripheral processes on hearing. 47 The interaction between ‘central’ hearing abilities and peripheral auditory health suggests that neurodegenerative diseases and aging affect hearing across a spectrum, from cochlea to cortex.48–50 This complex interaction may lead to significant hearing loss under certain conditions, especially when compensatory mechanisms fail, highlighting the dual impairment of neurodegeneration and peripheral hearing loss.43,51,52
Limitations of our study
This study acknowledges certain limitations. Primarily, the challenge in ensuring data reliability arises from the variability in hearing loss diagnosis standards among experts, compounded by occasional code exaggerations driven by the fee-for-service reimbursement system. 53 To mitigate this, we established inclusion criteria for subjects with hearing loss based on rational benchmarks, such as PTA or speech audiometry results, in conjunction with ICD-10 codes. While this approach enhanced diagnostic reliability, it may have led to underestimation of mild hearing impairment cases where formal testing is not routinely performed in clinical practice. Secondly, the NHIS-SC database does not provide detailed information on the MCI that we could not confirm the risk of conversion to MCI from cognitively normal subjects. Thirdly, it is important to note that changes in the severity of hearing loss over time were not considered in our analysis. This limitation should be taken into account when interpreting the results, as it may impact the observed associations. Despite these constraints, the NHIS-SC database offers a comprehensive sample of 558,147 subjects over an extensive follow-up period from 2002 to 2015, thereby ensuring a representative of the elderly population. Future research should continue exploring these relationships, focusing on longitudinal studies and interventions to confirm these findings and develop effective strategies for dementia prevention in individuals with hearing loss.
Conclusions
In this study, hearing loss significantly correlates with an increased risk of dementia, particularly AD, while not showing a direct link with VaD. This suggests neurodegenerative disease such as AD's unique vulnerability to auditory processing impairments that highlights the complex interplay between peripheral and central hearing processes affected by neurodegeneration, suggesting a multifaceted approach to understand and address the cognitive decline associated with hearing loss.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251316805 - Supplemental material for Hearing loss and the risk of dementia: A longitudinal analysis of the Korean National Health Insurance Service Senior Cohort
Supplemental material, sj-docx-1-alz-10.1177_13872877251316805 for Hearing loss and the risk of dementia: A longitudinal analysis of the Korean National Health Insurance Service Senior Cohort by Jae-Won Jang, Seung-Hwan Lee, Taesu Kim, Eunju Lee, Sang Won Park, Na Young Yeo and Young-Ju Kim in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
This study used National Health Insurance Service-Senior Cohort data (NHIS-2023-2-260), made by National Health Insurance Service. Authors thanks to Gaeul Jang and Seyeon Yeon for data management. ChatGPT, version 4o, a language model developed by OpenAI (![]() ), was used for language refinement of this manuscript.
), was used for language refinement of this manuscript.
Author contributions
Jae-won Jang (Conceptualization; Writing – original draft; Writing – review & editing); Seung-Hwan Lee (Writing – review & editing); Taesu Kim (Writing – review & editing); Eunju Lee (Data curation; Formal analysis); Sang Won Park (Investigation; Visualization); Na Young Yeo (Investigation; Visualization); Young-Ju Kim (Conceptualization; Supervision; Writing – original draft; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS-2023-00242528) and funded by “Regional Innovation Strategy (RIS)” through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (MOE) (2022RIS-005).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data used in this study is not available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.