
Abstract
Background
Exercise, as an adjunctive therapy for Alzheimer's disease (AD) patients, is meaningful and common. However, it remains unclear whether the modality of exercise has a positive impact on elderly AD patients.
Objective
The exploration of how multicomponent exercise can have positive effects on older adults with AD.
Methods
A detailed search was conducted across six databases, followed by independent screening to identify the final studies included in the analysis. The study was conducted following the guidelines of the Cochrane Handbook.
Results
Seventeen studies were included in the final analysis. The results showed that ME effectively improved activities of daily living (ADL) [SMD = 0.46, 95% CI (0.13, 0.79)], depression [SMD = −0.32, 95% CI (−0.63, −0.01)], and balance [SMD = 0.73, 95% CI (0.32, 1.14)]. In terms of ADL, an intervention period of 12 weeks, with 3–5 sessions per week and each session lasting 30–60 min, may be more effective.
Conclusions
Multicomponent exercise demonstrates statistically significant effects in improving ADL, depression, and balance in AD patients aged 60 and above. Future studies with larger sample sizes are needed to provide higher-level evidence.
Introduction
Alzheimer's disease (AD), as the leading form of dementia, 1 is one of the major public health concerns worldwide. With the global aging trend, the number of AD patients continues to rise. In the United States alone, approximately 6.07 million people were affected in 2020, and it is estimated that this number will increase to 13.85 million by 2060. 2 In China, a highly populated country, the overall prevalence rate is 3.48%, 3 while in Europe, the prevalence is even higher, around 5.05%. 4 Meanwhile, AD brings increasingly adverse impacts to patients, their families, and society. As the severity of AD progresses, patients may experience declines in cognitive ability, language expression, emotional stability, and other aspects.5–7 Most patients are cared for by family members, and the time, effort, and additional financial costs involved increase the health and economic burdens on caregivers.8–10 Furthermore, with the growing number of AD patients, governments around the world will face rising healthcare and social care expenditures,11,12 which may eventually have an impact on the socio-economic structure.
However, there is currently no cure for AD. Most pharmacological treatments involve acetylcholinesterase inhibitors. 13 However, these medications often cause gastrointestinal discomfort14–16 and other side effects, which may further burden patients. Moreover, it is important to note that these drugs do not reverse or halt the progression of the disease but only improve cognitive function. Given these limitations, non-pharmacological approaches have emerged as viable adjunctive therapies. Among them, exercise has been widely utilized in the prevention and management of AD due to its advantages, including fewer side effects, low cost, and ease of implementation. Previous studies have used exercise as an intervention and systematically compared its effects with non-intervention approaches, such as standard care.17,18 Several review studies have shown that various forms of exercise can effectively improve cognitive function in AD patients19–22 and enhance quality of life. 23 Overall, exercise can serve as an adjunctive therapy to improve certain symptoms in patients with AD.
As one of the most recommended exercise modalities for the elderly, 24 multicomponent exercise (ME) is a comprehensive form of exercise that includes endurance training, strength exercises, balance training, and flexibility exercises. 25 A meta-analysis indicated that ME can play an effective role in preventing the decline of activities of daily living (ADL) in elderly individuals with dementia. 26 It has also been shown to improve muscle strength, balance, 27 gait, 28 and more. Importantly, the effectiveness of ME in improving cognitive impairment in the elderly has been supported by evidence.24,29–31
A previous meta-analysis used a network meta-analysis approach to examine the effectiveness of various exercise modalities, including ME, on visuospatial memory in patients with AD. 32 Additionally, several meta-analyses, systematic reviews, and retrospective studies involving patients with dementia have explored whether ME can improve dementia-related symptoms.33–35 However, the effects of ME on outcomes such as depression and balance ability in older adults with AD have been rarely addressed in existing meta-analyses. Therefore, the specific effects of ME on older adults with AD remain underexplored in meta-analyses.
This study aims to investigate the specific effects of ME on older adults with AD concerning their quality of daily life, depression, and global cognition using a meta-analytic approach. The findings will provide clinical adjunctive treatment options and offer systematic evidence for caregivers, clinicians, and healthcare providers.
Methods
Search strategy
A detailed search was conducted up to December 1, 2024, in the following databases: PubMed, Embase, Web of Science, Cochrane Central Register of Controlled Trials, CINAHL, and PsycInfo. No restrictions were placed on the publication date or language of the literature. The detailed search process can be found in Supplemental Material 1. The registration number is CRD42025629965.
Eligibility criteria
Participants. The age limit for inclusion in the final analysis was set at over 60 years old. Additionally, participants must have been professionally diagnosed with AD based on established clinical criteria. Diagnosis was determined by a combination of clinical symptoms and biomarker assessments when available. To clarify the effects of ME on patients with AD, studies in which participants had other neurological or psychiatric disorders as primary diagnoses (e.g., Parkinson's disease, stroke) were excluded from the final analysis.
Interventions. The intervention in the experimental group must be ME, involving at least two types of training. To assess the specific effects of ME, the control group should not engage in organized physical exercise or other forms of exercise. Instead, they typically underwent standard medical care, participated in health education programs, or were placed on a waitlist control.
Outcome measures. The study should report at least one of the following outcome variables: ADL, including Basic Activities of Daily Living (BADL) and Instrumental Activities of Daily Living (IADL), global cognition, depression, balance, functional endurance, or functional mobility. The 6-min walk test (6MWT) may be used to assess functional endurance, while the Timed Up and Go (TUG) test may be used to assess functional mobility.
Study selection
The literature retrieved from the databases will be screened using EndNote software. The screening process will be conducted independently by two researchers. Any discrepancies or differences will be checked by a third researcher, and the final decision will be made through group discussion. During the screening process, conference papers, animal studies, and observational studies were explicitly excluded. To enhance the quality of the research, only randomized controlled trials (RCTs) were selected.
Data extraction
The required data for the study, including the mean values, standard deviations, and sample sizes of the experimental and control groups before and after the intervention, will be independently extracted by two researchers. In cases of discrepancies, a third researcher will assess the data, and the final decision will be made through group discussion. For studies where data are reported in the form of images, the researchers will extract the data using Engauge Digitizer software. If the data are not directly reported in the form of mean ± standard deviation (MD ± SD), the researchers will first attempt to contact the authors via email for clarification. In cases where the authors cannot be contacted due to the age of the publication, data will be calculated using formulas. Specifically, the data required are those reported as standard error (SE) and 95% confidence intervals (CI). These will be calculated using Equation 1
36
and Equation 2.
37


Risk of bias of individual studies
Two researchers will independently assess the risk of bias for each study based on the Cochrane Handbook for Systematic Reviews of Interventions,
37
ROB1 tool was used for risk of bias assessment.
Random sequence generation: Assesses whether participants were allocated using a truly random method to avoid selection bias. Allocation concealment: Evaluates whether researchers were unable to predict group assignments before allocation to prevent selection bias. Blinding of participants and personnel: Determines whether participants and study personnel were blinded to the intervention to reduce performance bias. Blinding of outcome assessment: Assesses whether outcome assessors were blinded to group allocation to minimize detection bias. Incomplete outcome data: Evaluates whether follow-up data were complete and whether missing data could impact study conclusions. Selective reporting: Determines whether all predefined outcomes were reported to prevent reporting bias. Other bias: Assesses whether the study had additional sources of bias, such as baseline imbalances or conflicts of interest.
Each RCT will be classified into one of three risk levels: “low risk of bias,” “unclear risk of bias,” or “high risk of bias”.37,38
Data analysis
The analysis results will be expressed using standardized mean differences (SMD) and 95% confidence intervals (CI) based on the characteristics of the intervention.39,40 The effect sizes based on SMD will be classified as small (≤0.2), medium (≤0.5), large (≤0.8), and very large (>0.8). 41 Heterogeneity between studies will be assessed using the Cochrane Q test and I² statistic. The degree of heterogeneity will be classified as low heterogeneity (I² ≤ 25%), moderate heterogeneity (25% < I² ≤ 50%), substantial heterogeneity (50% < I² ≤ 75%), and significant heterogeneity (I² > 75%). 42 Based on the level of heterogeneity, the appropriate effect model will be selected. When heterogeneity is high (p < 0.1 or I² > 50%), a random-effects model will be used, 43 which is suitable for cases with significant heterogeneity and accurately reflects differences between studies. In cases of low heterogeneity (p ≥ 0.1 and I² ≤ 50%), a fixed-effects model will be applied.
The sources of heterogeneity between studies will be explored through subgroup analyses. Subgroup analyses will be conducted based on categorical variables, including intervention type, total duration of the intervention, frequency of intervention per week, and duration of each intervention session. Funnel plots will be used to examine the potential for significant publication bias, and Egger's test will be used to determine statistical significance based on the p-value. Sensitivity analysis will be performed by sequentially excluding individual studies to assess the impact of each study on the overall results. Statistical significance will be considered at p < 0.05.
Results
Study selection process
A total of 12,373 studies were initially retrieved from the databases based on the research topic. Following the established screening criteria, duplicate studies were excluded, and studies were assessed based on their titles and abstracts to determine eligibility. Full-text reviews were conducted for studies that met the inclusion criteria. Ultimately, 17 studies were included in the quantitative synthesis. The detailed process of exclusion and inclusion is shown in Figure 1.
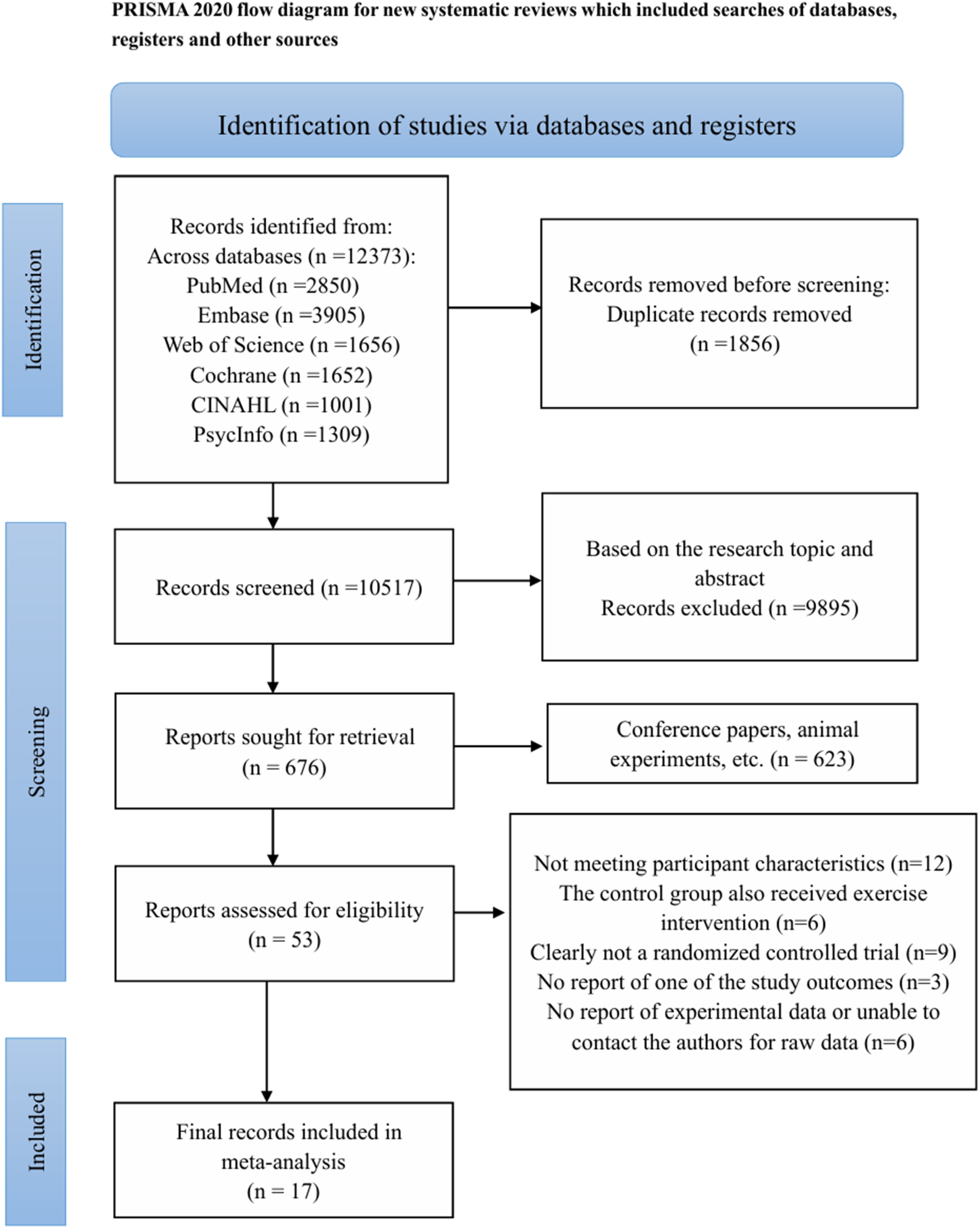
Detailed search process.
Study characteristics
Among the 17 studies, data from 1061 participants were included in the final analysis. All participants were diagnosed with, with ages ranging from 60 to 94 years. The specific components of the ME intervention include aerobic exercise, balance training, resistance exercise, stretching exercise, strength and endurance training, functional training, flexibility training, and coordination training. Each of the experimental group interventions includes 2 to 4 of the aforementioned components. The interventions in all experimental groups included at least two types of exercise training, with a maximum of four types. Detailed characteristics of each study are summarized in Supplemental Material 2.
Risk of bias of individual studies
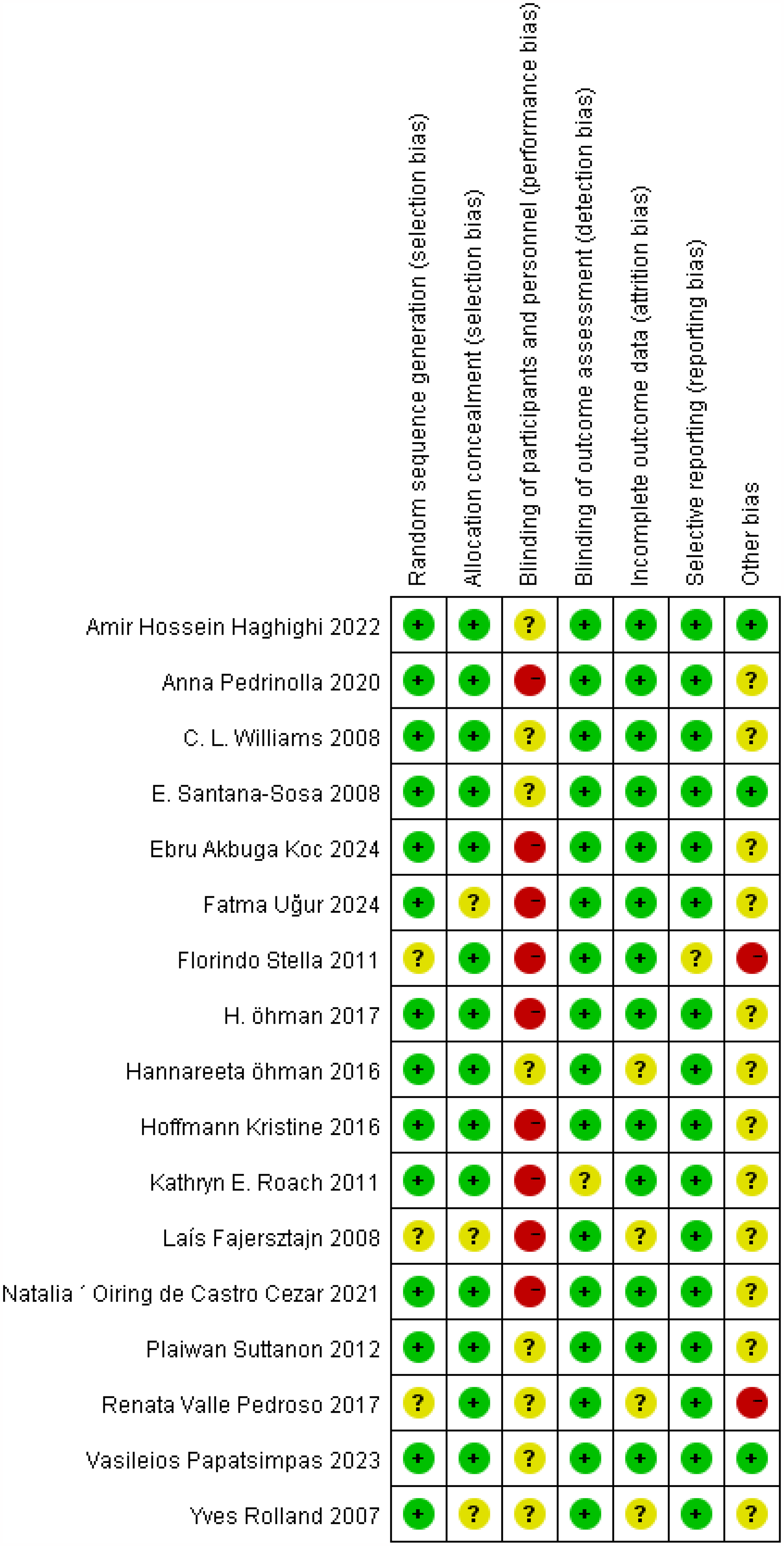
The assessment of each included study is presented in Figure 2, while the overall risk of bias for all included studies is provided in Supplemental Material 3. In the blinding of participants and personnel domain, since exercise is used as an intervention, certain biases are unavoidable. 44 Therefore, in this risk assessment, studies that explicitly stated the impossibility of blinding were considered to have a high risk of bias, while studies that did not report the use of blinding were classified as having an unclear risk of bias. Regarding other bias, a substantial number of studies may have systematic biases such as baseline characteristic imbalances, but their actual impact on the results remains unclear; thus, they were assessed as having an unclear risk of bias. Similarly, in the assessment of other domains, if certain aspects cannot be clearly determined, they are also classified as having an unclear risk of bias. If no influencing factors are identified, the study is rated as having a low risk of bias according to the assessment criteria. However, if issues affecting the outcome determination are present, the study is considered to have a high risk of bias.
Publication bias.
In the domain of random sequence generation and allocation concealment, 3 studies were rated as having an unclear risk of bias, while 14 studies were judged to have a low risk of bias. For blinding of participants and personnel, 8 studies had an unclear risk of bias, and 1 study was assessed as having a high risk of bias. In the domains of blinding of outcome assessment and selective reporting, 1 study each was assessed as having an unclear risk of bias, whereas 17 studies had a low risk of bias. Regarding incomplete outcome data, 4 studies were judged to have an unclear risk of bias, and 13 studies had a low risk of bias. In the domain of other bias, 2 studies were rated as having a high risk of bias, 12 studies had an unclear risk, and 3 studies were considered to have a low risk of bias. The detailed results are presented in Figure 2.
Meta-analysis of outcome measures
Impact of ME on ADL. Ten studies reported on the ADL measure. The results (Figure 3) showed that, compared to the control group, ME had a moderate effect on improving ADL in patients [SMD = 0.46, 95% CI (0.13, 0.79), p = 0.006, I²=70.6%]. However, there was considerable heterogeneity between the studies.
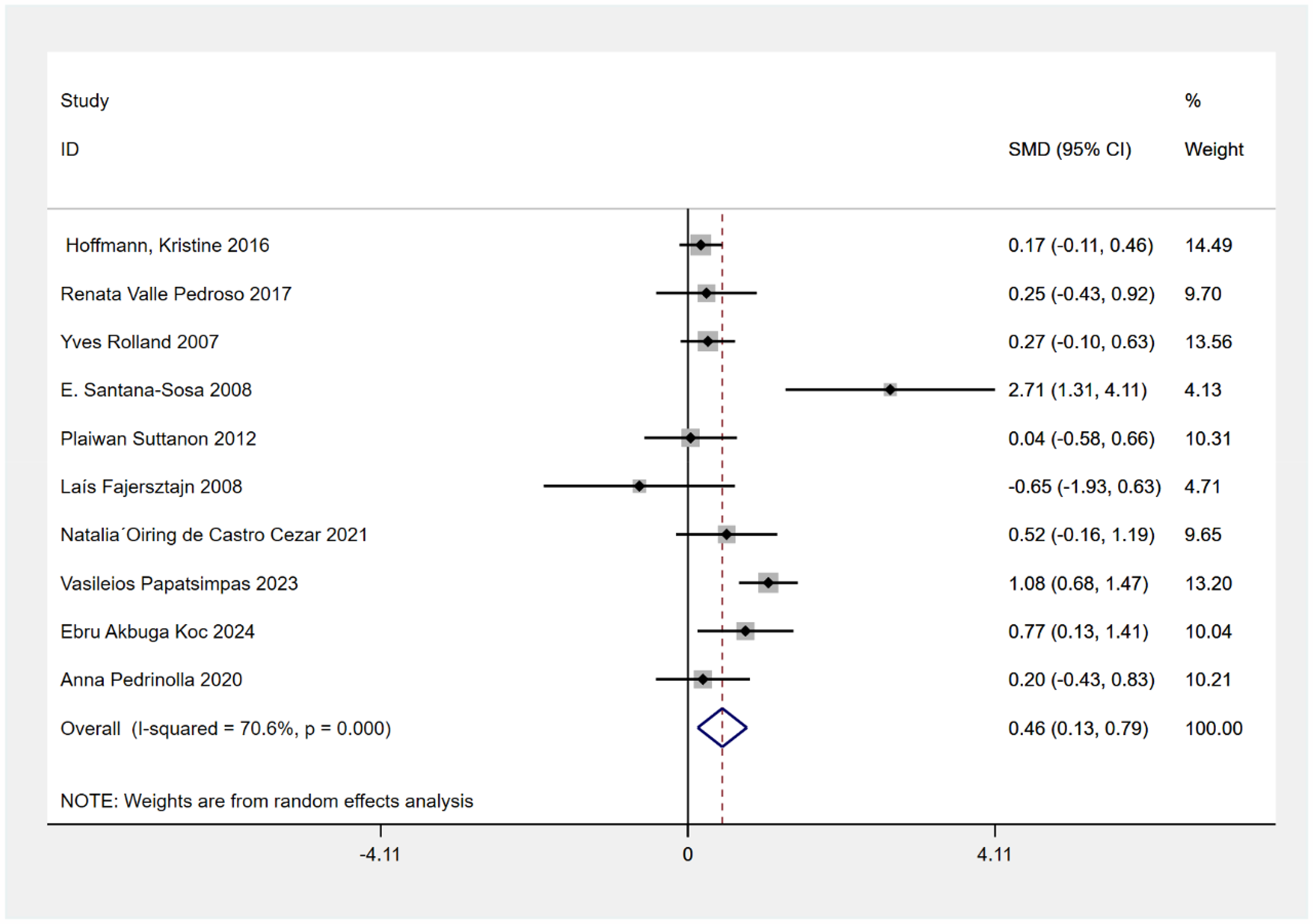
The impact of exercise on activities of daily living.
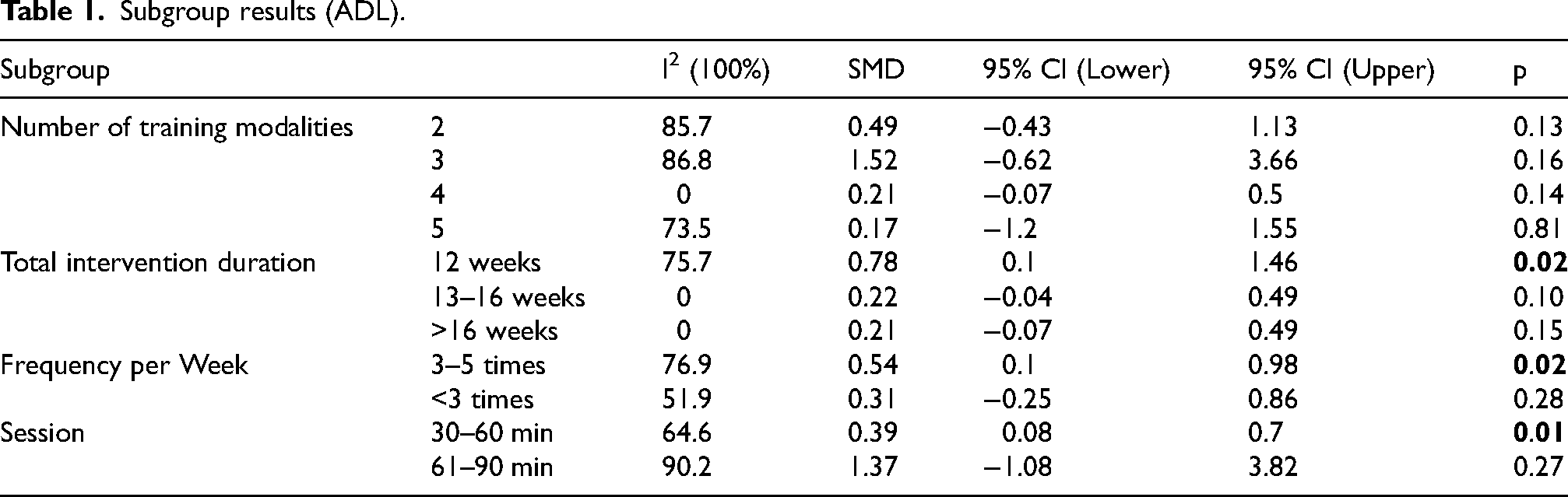
Subgroup analysis. To explore the potential sources of heterogeneity, a subgroup analysis was performed, and the results are shown in Table 1. The number of training components in ME did not have a significant positive effect on ADL. However, a total intervention period of 12 weeks [SMD = 0.78, 95% CI (0.1, 1.46), p = 0.02], intervention 3–5 times per week [SMD = 0.54, 95% CI (0.1, 0.98), p = 0.02], and each session lasting 30–60 min [SMD = 0.39, 95% CI (0.08, 0.7), p = 0.01] demonstrated a moderating effect on the intervention outcomes. Specifically, a single intervention duration of 30–60 min showed a moderate effect size, while the intervention frequency of 3–5 times per week and a total intervention period of 12 weeks showed a large effect size. Overall, ME was found to be effective in improving patients’ ADL.
Subgroup results (ADL).
Sensitivity analysis
We conducted a sensitivity analysis by sequentially excluding individual studies, and the results are presented in Figure 4. The analysis showed that after excluding the study by E. Santana-Sosa, the heterogeneity between studies decreased (I2 = 60.3%), but the overall heterogeneity remained high, indicating that the high heterogeneity of the results was largely unchanged.

Sensitivity analysis of ADL outcomes.
Impact of ME on depression. Seven studies included the intervention effects on depression, with the results shown in Figure 5. ME was found to alleviate depressive symptoms in patients [SMD = −0.32, 95% CI (−0.63, −0.01), p = 0.04]. However, there was considerable heterogeneity between the studies (I² = 62.4%, p = 0.01).
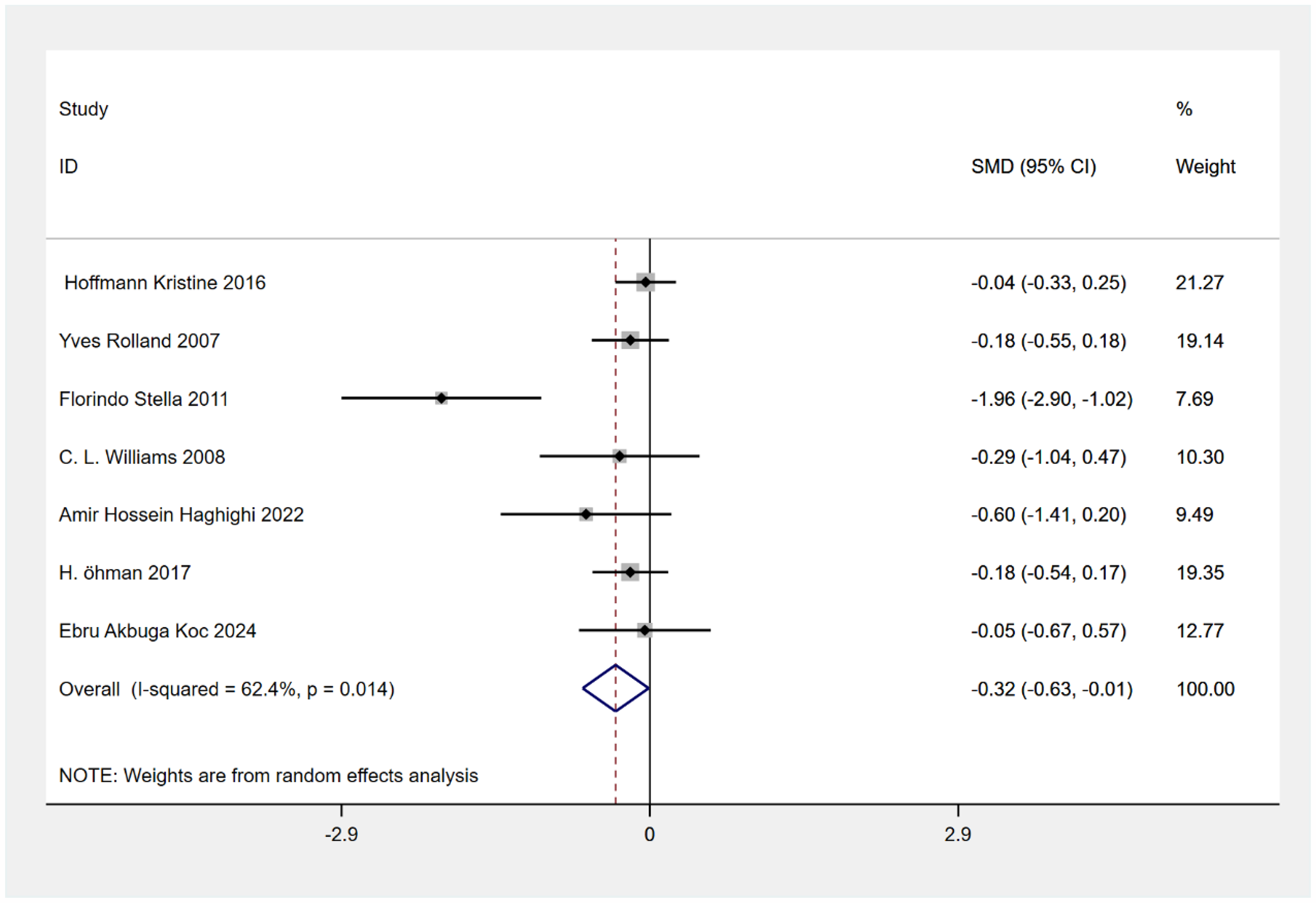
The impact of exercise on depression.
Subgroup analysis. We explored the effects of the total intervention period and the weekly intervention frequency, with the results presented in Table 2. Both grouping methods reduced some of the I² values, suggesting they could be potential sources of heterogeneity, although this is unlikely. Therefore, it is highly probable that other factors or a combination of factors may have influenced the results. Nevertheless, overall, ME was found to be effective in alleviating depression.
Subgroup results (depression).

Impact of ME on balance ability. The analysis of balance ability was conducted based on data from four studies, with the results shown in Figure 6. Compared to the control group, ME was found to enhance patients’ balance ability [SMD = 0.73, 95% CI (0.32, 1.14), p = 0.00]. Moreover, there was no significant heterogeneity between the studies (I² = 0%, p = 0.45). Overall, ME had a large effect on improving the balance ability of AD patients.
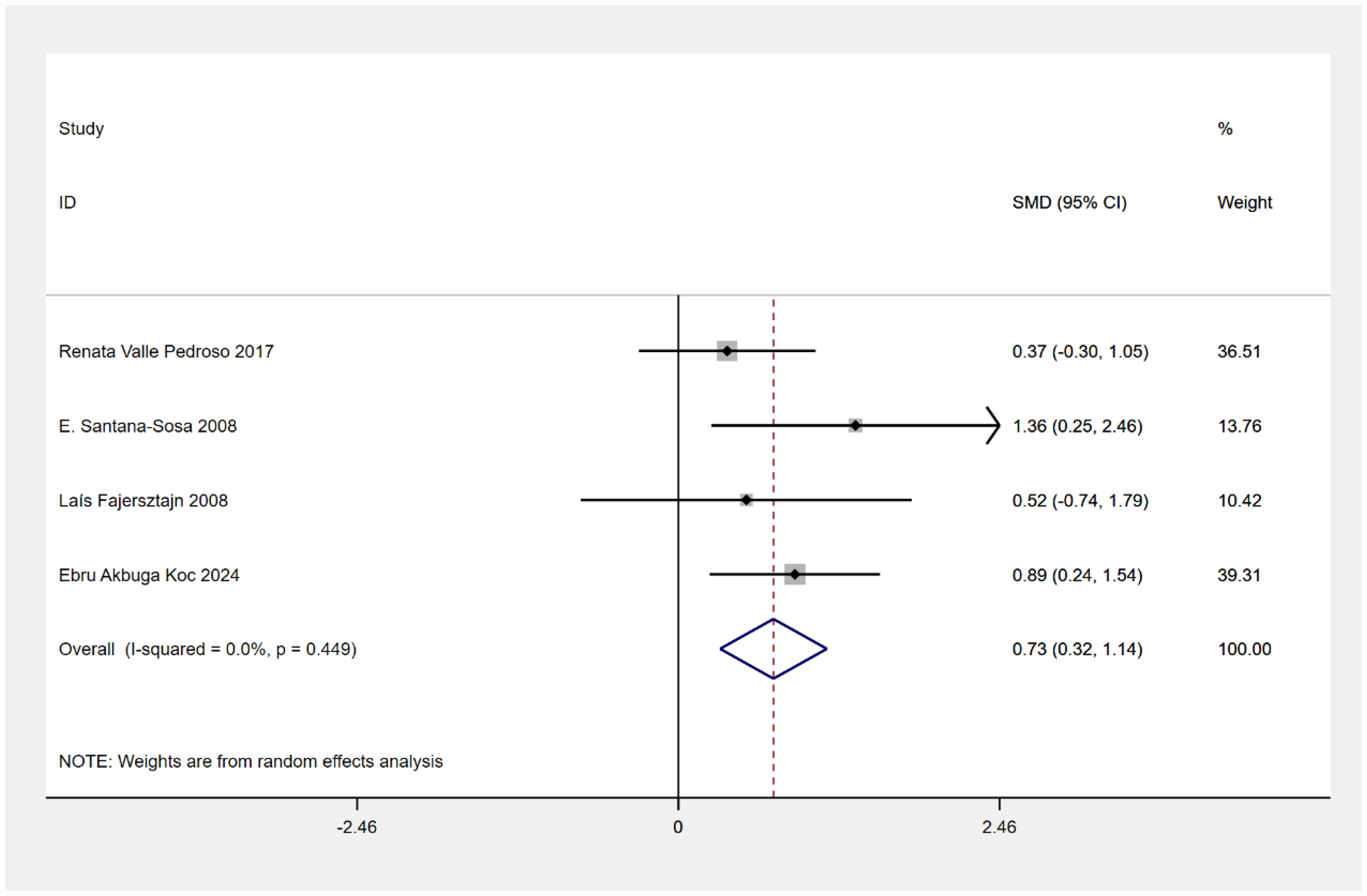
The impact of exercise on balance.
Impact of ME on MMSE, TUG, and 6-Minute Walk test. The results indicated that, compared to the control group, ME as an intervention had no significant impact on the patients’ MMSE [SMD = 0.52, 95% CI (−0.26, 1.30), p = 0.19], TUG [SMD = −0.28, 95% CI (−0.58, 0.00), p = 0.05], or 6MWT [SMD = 0.32, 95% CI (−0.04, 0.67), p = 0.08], results are in Supplemental Material 5.
Publication bias
By observing the funnel plot (Figure 7), a noticeable asymmetry was found, suggesting the possibility of publication bias. Further analysis using Egger's test showed that the p-values for ADL, depression, and balance ability were all greater than 0.05, indicating no statistically significant publication bias. Additionally, sensitivity testing, where individual studies were excluded one by one (Supplemental Material 4), did not reveal any studies that significantly impacted the results. In conclusion, these findings suggest that the results are robust.
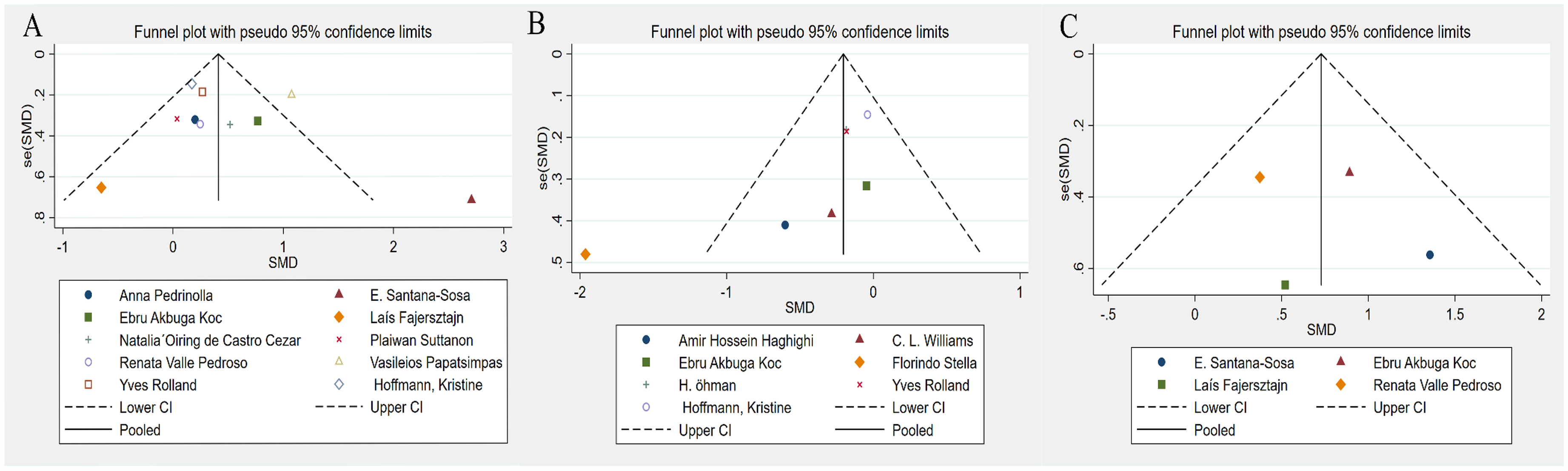
Funnel chart: A(ADL); B(Depression); C(Balance).
Discussion
This study analyzed 17 RCTs to assess the impact of ME on ADL, depression, balance ability, global cognition, functional endurance, and the functional mobility in AD patients. The results indicated that ME significantly improved patients’ ADL, with the most effective intervention being a 12-week program, with 3–5 sessions per week, each lasting 30–60 min. ME also alleviated depressive symptoms and enhanced balance ability. However, no positive effects were found on global cognition, functional endurance, or the functional mobility.
The results indicate that ME has a significant positive effect on improving ADL. A previous meta-analysis also concluded that ME has beneficial effects. However, the participants in this study were AD patients, whereas the meta-analysis included dementia patients. Although the majority of participants in that study had AD-type dementia, not all dementia patients were classified as having AD-type dementia. 45 Therefore, there is a difference in participant composition between the two studies. Additionally, ME did not yield a significant positive result in the TUG test, which contrasts with a previous study that concluded ME could improve the functional mobility of dementia patients. 33 This discrepancy is primarily due to differences in participant composition and the number of included studies. Similarly, ME did not produce a significant positive result in the MMSE scale, suggesting that ME may be ineffective in improving cognitive function. Two previous review studies also indicated that there is no evidence supporting the effectiveness of ME in enhancing cognitive function in AD patients.46,47 Furthermore, another network meta-analysis found that ME did not improve visuospatial memory in AD patients, and visuospatial abilities are a subcategory of cognitive function.
In the studies examining the effects of ME on ADL and depression, there exists considerable heterogeneity. Despite conducting subgroup analyses, the sources of this high heterogeneity remain undetermined. Therefore, by tracing back to the original studies, we hypothesize that the heterogeneity may arise from several factors. First, since ME is used as the intervention, it is impossible to achieve complete blinding of both the intervention providers and participants, which may lead to variations in the intervention effects across studies. Second, as ME encompasses a variety of specific exercise components, the training contents in each study are not entirely consistent, which could also contribute to the heterogeneity. Regarding the high heterogeneity associated with the study by E. Santana-Sosa, this may be attributed not only to the aforementioned reasons but also to the diversity of outcome measurement tools used, which reduced the comparability of results with those of other studies, further increasing the heterogeneity. Additionally, differences in training environments, supervision methods, and cultural backgrounds are likely to be sources of the high heterogeneity observed.
ME demonstrated a significant advantage in improving ADL in AD patients, which may be related to the multidimensional nature of the intervention itself. ADL is influenced by various factors such as physical fitness and bodily functions.48,49 ME incorporates multiple types of exercise interventions,50,51 which can act on various levels simultaneously, achieving overall rehabilitation effects. Mechanistically, the positive impact of ME on ADL may stem from several combined effects. Firstly, ME has been shown to improve executive function in older adults. 52 Improvements in executive function effectively enhance organizational and problem-solving abilities, 53 which are crucial for AD patients in handling complex daily activities such as shopping and meal preparation. Secondly, the strength training component of ME may enhance muscle strength and coordination,54,55 increasing motor control ability 56 and improving the efficiency of daily task performance. In other words, ME may promote multisensory motor adaptation and coordination between different muscle fiber bundles,57,58 leading to significant improvements.
In addition, studies on ME in AD have provided a deeper understanding of the neurobiological mechanisms. ME typically combines different forms of exercise, such as aerobic exercise, strength training, and coordination training. These exercise modalities may effectively increase levels of brain-derived neurotrophic factor (BDNF) through various pathways, promoting neurogenesis and enhancing plasticity. Aerobic exercise in ME improves cardiovascular function, activates the cortical brain areas, and stimulates BDNF secretion. 59 Resistance or strength training, by enhancing the muscle strength of AD patients, may facilitate the adaptability of the nervous system and, through improving neuro-muscular plasticity, increase BDNF concentrations.60,61 Additionally, aerobic exercise within ME is believed to regulate the activity of brain proteases, particularly by reducing the activity of BACE1, thereby decreasing amyloid-β (Aβ) production.62,63 Reducing Aβ accumulation or promoting its clearance helps alleviate the neuroinflammation and oxidative stress induced by Aβ, 64 mitigating neurotoxicity and thus delaying the decline in cognitive function. Furthermore, the beneficial effects of aerobic exercise on AD may be mediated through the improvement of blood supply and neuronal activity regulation in regions of the brain that are particularly vulnerable to AD, such as the hippocampus and prefrontal cortex. Through aerobic exercise, areas of the brain that are typically under perfused in AD may receive increased blood flow, thereby enhancing cerebral perfusion. 65
Building on the above, the subgroup analysis in this study further highlights the critical role of intervention duration, frequency, and session length in improving ADL in AD patients. The intervention lasting 12 weeks, with 3 to 5 sessions per week and 30 to 60 min per session, demonstrated significant benefits. The potential reasons for the positive effects of this intervention duration, frequency, and session length may include the following. This result suggests that an optimal intervention duration and training frequency provide patients with sufficient time and stimulation to enhance physical function. The 12-week duration may provide adequate time for the nervous system to adapt and repair, while the 3 to 5 sessions per week may help maintain a continuous exercise load, maintaining neural system activity and muscle function improvement. 66 Each session lasting 30 to 60 min is suggested to strike strikes a balance, preventing excessive fatigue while effectively improving cardiovascular health, strength, and coordination, 67 thereby possibly contributing directly contributing to the enhancement of ADL. In conclusion, a well-structured intervention cycle, frequency, and session duration may be key factors in the effectiveness of ME interventions for improving AD patients’ daily living abilities.
Balance ability is a key factor for the independence of daily living activities in AD patients and one of the predictive factors for adherence to daily living activities. 68 Many studies on ME interventions include exercises targeting balance ability. This specific training has been shown to enhance balance in older adults.69,70 Within the balance training content, the interventions may stimulate the vestibular system, 71 sensory systems,72,73 and cerebellar functions related to balance, 74 with these three systems working synergistically to improve postural control. Additionally, specialized balance exercises may also enhance the self-confidence of older adults with AD, reduce fear of falling, and alleviate psychological distress,75–77 further promoting balance performance in daily life. The combined effects of these potential psychological factors contribute to the improvement of balance in elderly AD patients. This, in turn, provides further support for the improvement of ADL.
The role of exercise in improving depression has been supported by many studies.78–80 As a comprehensive form of exercise, ME offers multiple potential explanations for its effects on depression in AD patients. Most of the included studies incorporated aerobic exercise, resistance training, or strength training. Aerobic exercise can alleviate depressive symptoms by regulating neurotransmitters such as monoamines (serotonin, dopamine, norepinephrine, etc.), increasing cortisol and adrenocorticotropic hormone levels, 81 and boosting β-endorphins. 82 Similarly, research has confirmed the effectiveness of resistance training in alleviating depression in older adults. 83 In addition to the physiological and psychological mechanisms mentioned above, social mechanisms may also explain this outcome. ME is typically conducted in group or team formats, increasing opportunities for social interaction, reducing feelings of social isolation, 84 and fostering a positive mental state, which further helps alleviate depression. Overall, the different components of ME complement each other, collectively contributing to its effectiveness in improving depression.
The lack of significant improvements in global cognition, functional endurance, and the functional mobility following ME intervention may be attributed to both the design of the intervention and the evaluation methods employed. First, the absence of cognitive enhancement may be due to the relatively short duration of the intervention, which likely failed to capture the long-term effects of neuroplasticity. Neuroplasticity typically requires an extended period to manifest, and short-term interventions may not allow enough time to observe meaningful cognitive improvements.85,86 Furthermore, the intervention may have lacked sufficient cognitive challenges, such as dual-task training or executive function challenges, which are essential to fully engage the brain's neuroplasticity. 87 Regarding the TUG test, if the intervention did not emphasize balance and coordination training specifically, it could explain the lack of significant improvements in dynamic balance. 88 The TUG test primarily assesses balance and mobility, 89 and if the intervention focused more on strength or cardiovascular fitness, it may not have sufficiently improved balance control, resulting in no significant change in TUG performance. For the 6MWT, while multi-component exercise can improve overall fitness, the intervention might have lacked sufficient endurance training or a focus on aerobic exercise, which is crucial for enhancing walking endurance. As a result, improvements in walking capacity during the 6-min walk test were not observed. In summary, the lack of significant improvement in these outcomes may stem from the intervention's content and intensity not being optimized to meet the specific demands of these tests.
Strengths and limitations of the study
First, our study only included RCTs, which enhances the reliability and reproducibility of the results and improves the evidence level of the study. Second, through subgroup analysis, we identified the optimal intervention period, frequency, and duration of each session for the ADL outcomes.
However, there are certain limitations in the study. Firstly, although 17 studies were included in this analysis, variations in study design quality, sample size, and other factors may impact the reliability of the results. Studies of lower quality may introduce biases, which in turn could affect the accuracy of the overall conclusions. Secondly, the components of ME are not completely standardized, with variations in the selection of specific intervention elements such as aerobic exercise, resistance training, balance training, and coordination exercises, which may influence the interpretation of the results. Thirdly, due to differences in the severity of AD, participant gender distribution, baseline physical activity level, and regional or cultural factors across studies, it is not possible to assess the extent to which these potential disparities might influence the outcomes. Finally, although bias analysis was conducted, the evident asymmetry of the funnel plot still suggests the potential presence of publication bias. Moreover, it is important to emphasize that the effect of ME may have been overestimated.
In conclusion, future research should include more high-quality RCTs to further validate the effects of ME on AD patients and provide higher-level evidence.
Conclusion
ME demonstrates statistically significant effects in improving ADL, depression, and balance ability in AD patients aged 60 and above. However, as the physical condition of patients may vary, the choice of ME interventions should be tailored to the individual patient's needs.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251346989 - Supplemental material for Multicomponent exercise interventions for older adults with Alzheimer's disease: A systematic review and meta-analytical perspective
Supplemental material, sj-docx-1-alz-10.1177_13872877251346989 for Multicomponent exercise interventions for older adults with Alzheimer's disease: A systematic review and meta-analytical perspective by Duo Yang, Na Hou and Mingyuan Jia in Journal of Alzheimer's Disease
Footnotes
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available within the article and/or its supplemental material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.