
Abstract
Background
Gait speed slows prior to cognitive decline in clinical Alzheimer's disease (AD), and is associated with cognitive performance and biomarkers of amyloid-β (Aβ) pathology in cognitively unimpaired (CU) older adults. However, the influence of subjective cognitive decline (SCD) severity on the association between Aβ and gait speed is not known.
Objective
We examined the relationship among gait speed, SCD severity and Aβ deposition in CU older adults.
Methods
Gait speed was measured over 15-feet. Aβ deposition was quantified using Pittsburgh-B (PiB) PET, expressed in Centiloid units (CL). Severity of SCD was quantified on the Memory Functioning Questionnaire (MFQ) on measures of seriousness and frequency of forgetting, mnemonic usage and retrospective functioning. We fitted a series of linear models with gait speed as the dependent variable; and each dichotomized sub-scale of the MFQ and Aβ as independent variables, adjusting for depression, white matter hyperintensity volume and executive function.
Results
In 58 CU individuals (mean age 85, 35% female), mean gait speed was 0.91 m/s and Aβ deposition was 36 CL. The relationship between slower gait and greater Aβ deposition showed a stronger association in those with more frequent mnemonic use (r = −0.36, p = 0.05) and with greater seriousness of forgetting (r = −0.33, p = 0.08) compared to those with lesser severity of subjective cognitive concerns (r = 0.02, p = 0.9 and r = −0.08, p = 0.7 respectively).
Conclusions
The findings indicate that in those with greater severity of SCD, association between slower gait and greater Aβ deposition is stronger, warranting longitudinal assessments of SCD severity and gait changes in preclinical AD.
Introduction
The preclinical phase of Alzheimer's disease (AD), characterized by accumulation of AD pathology (brain amyloid-β or Aβ plaque, hyperphosphorylated tau tangles), 1 is associated with self-perceived changes in cognition and subtle motor changes. 2 Subjective cognitive decline (SCD) refers to one's experience of cognitive functional change without objective evidence of cognitive impairment. 3 Subjective measures of cognitive abilities assist in better delineating variability in self-perceptions about memory and could reveal information on daily cognitive function not captured on objective tests. 4 Cognitively unimpaired (CU) older adults with SCD are more likely to progress to rapid cognitive decline in the presence of Aβ pathology, but AD pathology is seen in approximately 50% of those with SCD. 5 The presence of cognitive complaints and slow gait increases dementia risk 6 ; however, the relationship between severity of cognitive complaints, gait speed and Aβ deposition in CU older adults is not well understood.
Gait slowing precedes onset of cognitive decline in the evolution of dementia by 6–15 years. 7 We found that Aβ pathology is associated with slower gait in dementia-free older adults. 8 Furthermore, in CU older adults, Aβ deposition on positron emission tomography (PET) was associated with magnitude of gait slowing while performing cognitive-motor dual-tasks. 9 This line of work suggests that Aβ deposition int he brain influences both gait and cognition in CU older adults. Therefore, we sought to examine the relationships among severity of self-perceived cognitive concerns, gait speed and Aβ in CU oldest-old. As SCD is a plausible and early global marker of cognitive change in AD and related to Aβ, we hypothesized that Aβ would be related to gait speed, particularly in those with greater compared to lesser severity of cognitive complaints.
Methods
Population
We performed a secondary analysis of data of CU older adults enrolled in the imaging extension of the Gingko Evaluation of Memory Study (GEM) study. The GEM study was a randomized double-blind, placebo-controlled trial of Ginkgo biloba targeted to prevent dementia, particularly AD, that recruited CU older adults and older adults with mild cognitive impairment (MCI). 10 Participants were 75 years or older recruited from the community. Those with self-report of dementia or Parkinson's disease, Clinical Dementia Rating (CDR) scale score of 0.5 or, dementia range performance on cognitive testing (see below), use of cholinesterase inhibitors, severe depression, abnormal thyroid function tests or vitamin B12 levels, anemia, and treatment with medications that potentially affect gait and cognition (tricyclic antidepressants, antipsychotics, anticholinergics, and dopaminergic medications) were excluded from the GEM study. Participants completed annual cognitive assessments for the duration of the study, and approximately 10 ± 3 months following the closeout visit, 194 participants enrolled at the University of Pittsburgh study-site underwent amyloid PET and brain MRI as part of the GEM imaging study. 11 We included data from 58 CU participants from this sample who had completed brain MRI, Aβ PET, physical performance measures and self-perceived cognitive functioning questionnaires within one-year of brain imaging.
Cognitive assessment and screening for depression
Participants were deemed cognitively unimpaired based on their performance on cognitive assessments that included tests of memory, visuospatial function, language, psychomotor speed, attention, executive function and global cognitive functioning. 12 Diagnostic adjudication of cognitive status (CU, MCI or dementia) was performed based on clinical information, cognitive assessments and functional status annually in the GEM study and at entry to the GEM imaging study. Depression was screened using the Center for Epidemiological Studies Depression Scale (CES-D), 13 a self-reported or interview-based screening tool for depression in older adults.
Gait speed
Time to walk 15-feet was measured as described previously. 14 Briefly, a 15-foot-long traverse was demarcated with tape and participants were instructed to begin walking from standing position at the start line and continue walking past the end line. Time was measured using a stop-watch, which was started after the prompt when one foot started to move across the start line and was stopped when the first foot crossed the 15-foot end mark. Two consecutive 15-foot walks were obtained – the first, a usual self-paced walk, and the second, a fast-paced walk. We used the usual self-paced timed walk measure and derived gait speed by converting it to meters per second.
Amyloid PET
Aβ PET was performed using Pittsburgh Compound-B (PiB). PiB-PET imaging methods were reported previously. 11 Briefly, 15 mCi of [C11] PiB ligand was injected over 20 s and a 10-min transmission scan was acquired for attenuation correction followed by a 20-min PiB-PET scan (4 × 5 min frames) acquired 50 to 70 min post injection. Images were reconstructed using filtered back projection and emission data were corrected for attenuation, scatter and radioactive decay. PiB retention in the brain was assessed using the CapAIBL image analysis software (Commonwealth Scientific, and Industrial Research Organization, Canberra, Australia), and expressed in Centiloid (CL) units, independent of MRI co-registration otherwise necessary for Aβ quatification. 15
Severity of cognitive complaints
Cognitive complaint severity was quantified on the Memory Functioning Questionnaire (MFQ). 16 The MFQ is 64-item scale, with each item denoting a cognitive concern scored on a 1 (worse) to 7 (better) scale range. Participant's concerns regarding their cognitive symptoms was assessed on the following question stems for each sub-scale of the MFQ: Mnemonic usage (8-items; “How often do you use these techniques to remind yourself?”), Seriousness of forgetting (18-items; “When you actually forget, how serious of a problem do you consider memory failure to be?”, lists specific situations), Frequency of forgetting (18-items; “How often do these present a problem for you?”, lists names, faces, numbers, recalling reading, events, etc.), and Retrospective function (6-items; “How is your memory compared to way it was?”, lists several time periods from 1 year ago 20 years ago, and at age 18). Composite scores were created for each sub-scale of the MFQ, and each sub-scale was dichotomized for severity of cognitive concerns based on a median-split. The sum of scores on each sub-scale provided a total score on the MFQ.
Statistical analysis
We used appropriate descriptive statistics (means, standard deviations, frequencies, percentages) to summarize participant characteristics. We fitted a series of linear models with gait speed as the dependent variable; and each dichotomized sub-scale of the MFQ, Aβ and their interaction as independent variables. As ours was a secondary analysis with a limited sample size focused on preliminary evidence, all statistical significance levels were interpreted as indicators of strength of evidence rather than those confirmatory based on a strict ≤0.05 criterion. Interaction term significance level was interpreted as an indicator of the strength of evidence supporting a differential gait speed-Aβ association between those with greater and lesser levels of SCD, based on median-split for each composite sub-scale score of the MFQ. We used Pearson correlation coefficients (r) to summarize the gait speed-Aβ associations separately in those with greater and lesser severity of SCD. We repeated the analyses after adjusting for feeling depressed at least some of the time during the prior 7 days, CES-D score, time to complete the Trails B test and white matter hyperintensity volume (WMH) normalized to intracranial volume on brain MRI. SAS® version 9.4 (SAS Institute, Inc., Cary, North Carolina) was used for all statistical analyses and graphical summarizations.
This study was in compliance with the ethical rules for human experimentation as stated in the Declaration of Helsinki, and followed approval by the University of Pittsburgh's Institutional Review Board.
Results
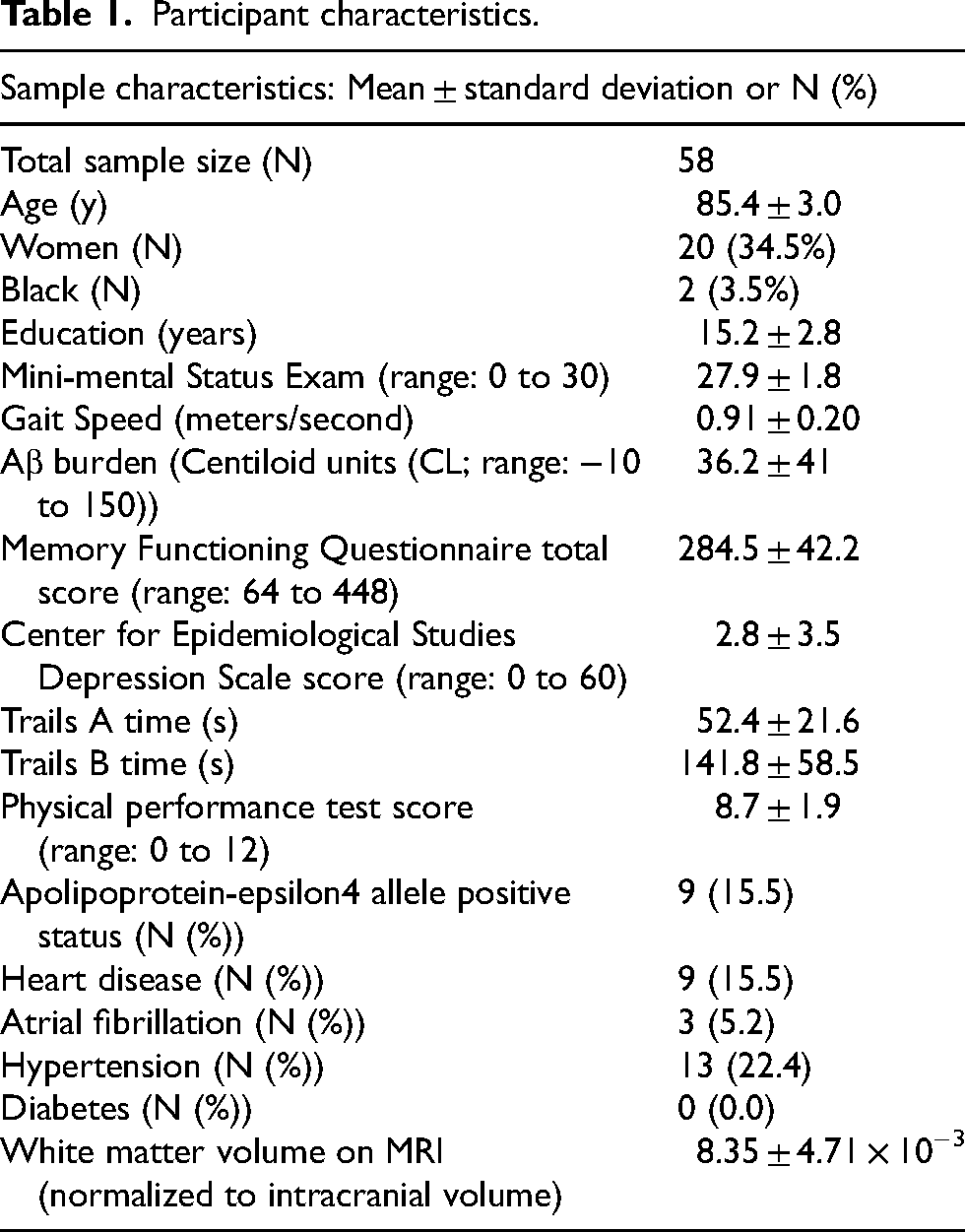
Participants were 85.4 ± 3.0 years old with 15.2 years of education on average (Table 1). Mini-mental Status Examination (MMSE) score was 27.9 ± 1.8. Gait speed was 0.91 ± 0.20 meters/second (m/s) and MFQ total score was 284.5 ± 42.2. Time to complete Trails B was 141.8 ± 58.5 s. Vast majority (52/58 or 90%) reported feeling depressed rarely or none of the time during the prior week, and CES-D score was 2.8 ± 3.5 (range 0 to 60).
Participant characteristics.
Gait speed was significantly correlated with MMSE score (r = 0.46, p < 0.001) but was not correlated with age, Aβ burden on PET, and white matter hyperintensities or hippocampal volumes on MRI. Aβ burden was not significantly correlated with total MFQ score or individual item scores (mnemonic usage, seriousness of forgetting, frequency of forgetting and retrospective functioning).
We observed some evidence of an Aβ burden × mnemonic usage interaction effect controlling for Trails B time (p = 0.09). In more frequent mnemonic users, higher Aβ burden was associated with slower gait speed (r = −0.36, p = 0.05) but the same relationship was not observed in less frequent mnemonic users (r = 0.02, p = 0.9; Figure 1). Findings qualitatively persisted after adjusting for covariates with correlations of −0.27 to −0.37 among more frequent mnemonic users and 0.02 to 0.05 among less frequent mnemonic users. Similarly, higher Aβ burden had a correlation of greater magnitude with gait (r = −0.33, p = 0.08) in those with greater seriousness of forgetting than in those with lesser severity of forgetting (r = −0.08, p = 0.7; Figure 2). After adjusting for depressive symptoms in the prior week, total CES-D score, and executive function performance as measured on Trails B, and WMH volume on brain MRI, findings qualitatively persisted with correlations of −0.33 to −0.40 and −0.04 to 0.07 in those with greater and lesser seriousness of forgetting, respectively. There was no indication of an interaction between subjective cognitive concerns that tap into frequency of forgetting or retrospective functioning with Aβ from tests of interaction or correlation coefficients of substantially different magnitude.

Association between global cortical Aβ deposition on Pittsburgh compound-B (PiB) (PiB)-PET expressed in Centiloid units (CL) and gait speed stratified by self-perceived use of mnemonics to recall items in cognitively unimpaired older adults.
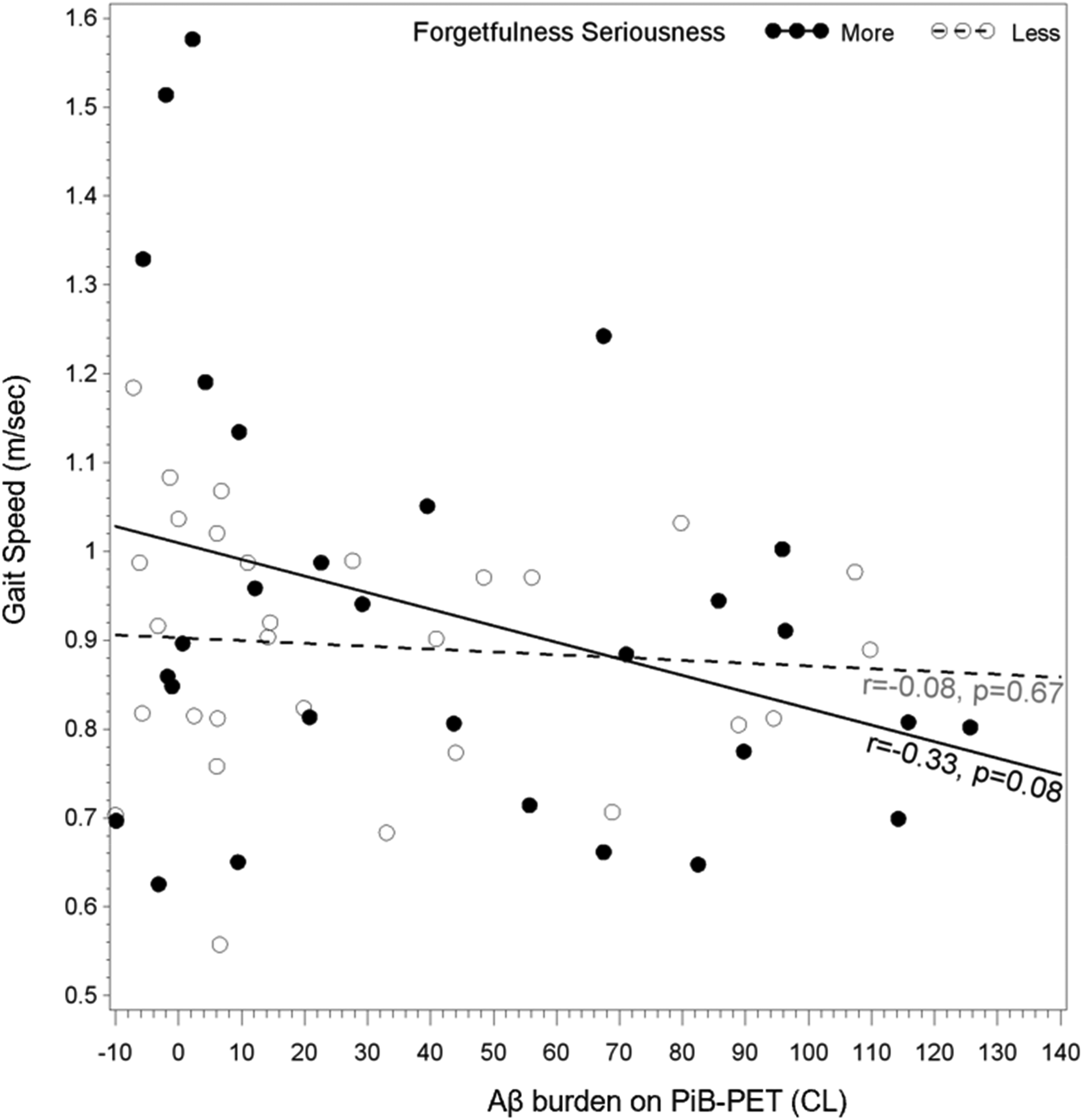
Association between global cortical Aβ deposition on Pittsburgh compound-B (PiB) (PiB)-PET expressed in Centiloid units (CL) and gait speed stratified by self-perceived seriousness of forgetting in cognitively unimpaired older adults.
Discussion
We and others previously found that slower gait is associated with higher Aβ deposition in the brain of older adults free of dementia.8,17 The results of the current study build on these prior findings suggesting that slower gait is associated with Aβ in CU individuals who have greater severity of self-perceived memory concerns.
These findings are in line with prior findings that link both memory complaints and slow gait to preclinical AD pathology. Gait declines prior to cognitive decline in early AD, 18 and dual-declines (gait and cognition) further increases dementia risk. 19 Our findings support previous studies that found that the phenotype of memory complaints and slow gait is predictive of progression to dementia. 6 Moreover, frequency of forgetting and retrospective cognitive functioning showed no interaction with Aβ with respect to gait speed in our study. This could be likely because questions that tap into a respondent's behavior of interest in relation to a prior reference period may be confounded by effects of aging on self-interpretation of cognitive concerns for temporarily accessible information. 20
The relationship between Aβ pathology and gait in those with greater SCD also suggests that preclinical AD pathology may present with subtle declines in objective motor measures and with more overt subjective measures of cognitive changes. These findings may explain discordant findings on the relationship between Aβ and gait speed in older adults.8,21 Our findings suggest that studies that examine relationships between AD pathology and motor function in CU samples also consider the severity of subjective cognitive concerns in the study samples. Ascertaining single memory items on subjective cognitive complaints may be unreliable or may be insufficient to understand cognitive-motor interactions in older adult samples. 22 Certain features associated with severity of cognitive complaints in SCD such as worries associated with complaints or, a feeling of worse performance than others of the same age group, may predict faster progression to MCI. 23 As slow gait has a stronger association with Aβ in those with greater severity of SCD, gait slowing may be another feature in the severity of SCD as likely to be associated with faster conversion to MCI and only be addressed by a longitudinal analysis of the sample examining MCI outcomes in relation to gait and cognitive symptoms. In those with greater severity of memory concerns, the finding of slow gait may suggest that preclinical AD pathology may be present. Additional studies examining preclinical AD pathology and longitudinal evaluations are warranted in order to better ascertain the relationships with future clinical AD in populations with greater severity of SCD and slow gait.
The mechanisms underlying our findings are not fully understood. Self-perception of cognitive changes is highly dependent on executive functioning, 24 as is with maintenance of gait speed in older adults. The association of Aβ and gait may be mediated in part through executive functioning and working memory. Greater severity of SCD is also linked to structural and physiological changes in the brain that are linked to slower gait. Higher Aβ in the frontal and parietal cortices is seen in SCD, 25 and Aβ in these brain regions is also associated with gait slowing in young 26 and older CU individuals. 8 Gait slowing is observed in MCI, and frontal cortical atrophy is associated with the severity of amnestic symptoms in MCI and slow gait. 27 Regional atrophy in frontal cortical regions is also related to slow gait in older adults, overlapping with regional changes observed with subjective memory changes. 28 Further research examining regional Aβ deposition and regional grey matter volumes may provide pathophysiological basis for the link between cognitive symptom severity and slower walking in preclinical AD.
The limitations of our study are important to contextualize. We had a small sample and thus the statistical power is limited especially to detect significance of interaction effects. Our sample size precludes adjusting the results for a comprehensive set of covariates. While the possibility of residual confounding cannot be entirely ruled out, the persistence of findings after adjusting for important covariates such as measures of depression and executive function is reassuring. We did not examine the regional changes due to limited sample size to draw conclusions on regional atrophy and Aβ deposition. Also, the sample is older, predominantly White and well-educated, which limits generalizability. Moreover, coexistent age-related neuropathological changes that tend to occur in people over age 80 such as synucleiopathies and limbic-predominant age-related TDP-43 encephalopathy (LATE), which can affect cognitive and motor functions,29,30 and peripheral changes such as severity of osteoarthritis and sensory neuropathies, which can affect gait, were not accounted for in the data and analysis. Finally, ours was a cross-sectional analysis, which precludes predictions on progression to prodromal AD in those with high Aβ.
In summary, we found that the severity of subjective cognitive concerns that tap into memory, influences the relationship between gait speed and Aβ such that those with greater burden of cognitive complaints show stronger association between slower gait and greater Aβ burden. Larger samples followed longitudinally, expanded AD biomarker profiles and examining regional AD pathology differences is warranted to draw more definitive conclusions. The findings of this analysis also suggest that severity of cognitive concerns rather than only the presence of memory complaints may be important to consider. These preliminary findings also support the need to incorporate into routine assessments, the evaluation of severity of self-reported concerns and motor changes such as slowing down while walking, in older adults without cognitive impairment.
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by grants K23 AG049945, P50 AG05133, P30 AG024827, R37 AG025516, and P01 AG025204 from the National Institute on Aging, and U01 AT000162 from the National Center for Complementary and Alternative Medicine
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.