
Abstract
Background
The risk of unprovoked seizures in patients with Alzheimer's disease (AD) is three-fold higher than the general population. However, no studies to date have reported on amyloid-β (Aβ) deposition in patients with Alzheimer's disease with epilepsy (ADEP).
Objective
The aim of this study was to collect clinical and positron emission tomography (PET)/magnetic resonance imaging (MRI) data from ADEP patients to compare and present the clinical characteristics and Aβ deposition patterns in this patient population.
Methods
Fifteen patients with ADEP, thirty-five patients with AD, twenty-three with late-onset epilepsy (LOEP), and twelve healthy controls were recruited. PET/MRI detected intracranial Aβ deposition, and differences in the brain regions distribution were compared between groups at the region of interest and voxel levels. Demographic data and medical history were further collected, while clinical and cognitive assessments were performed.
Results
In ADEP patients, the first seizure occurred in the early stages of AD, with focal-onset motor seizures accompanied by impaired consciousness being the predominant seizure type. Diagnosis and initiation of antiseizure medication (ASMs) were significantly delayed compared to LOEP patients. Additionally, the ADEP group showed less Aβ deposition in the middle cingulate gyrus than the AD group and had higher Mini-Mental State Exam and Montreal Cognitive Assessment scores.
Conclusions
This study reveals the clinical features and brain imaging differences between AD patients with and without EP, preliminarily confirming that the spatial deposition pattern of Aβ may be related to epilepsy and ASMs.
Introduction
Alzheimer's disease (AD) is the most common type of dementia, clinically characterized by a progressive decline in near-memory and cognitive abilities in older adults, which imposes a heavy disease burden on both caregivers and society. 1 The risk of unprovoked seizures in patients with AD is approximately 3.4-fold higher than that in the general population, with an incidence of 400 per 100,000 person-years. 2 In addition, up to 42.4%-50% of patients with AD also experiencing frequent spontaneous subclinical epileptic discharges (SEA).3,4 AD with comorbid epilepsy or SEA has previously been reported to be associated with accelerated progressive deterioration. However, the diagnosis of AD combined with epilepsy (ADEP) and SEA are delayed. There are several reasons for this. Firstly, the diagnosis and staging of AD relies on the amyloid-tau-neurodegeneration (A/T/N) system, which is defined by imaging and humoral examinations, while electrophysiologic examinations are not routinely used to screen for combined abnormal discharges. Further, ADEP is more difficult to diagnose than late-onset epilepsy (LOEP) without cognitive decline. Focal-onset nonconvulsive motor seizure with impaired consciousness is a common seizure type in ADEP; however, the semiology is insidious and easily confused with the complex neuropsychiatric symptoms of AD, making it more difficult for clinicians to recognize early symptoms.5,6 Diagnoses using electrophysiological methods also suffer from the dilemma of deep discharges that are difficult to capture. The number of discharges captured by combined long-duration electroencephalogram (EEG) and magnetoencephalography in AD patients is only approximately 1/10 of that captured by patent foramen ovale electrodes, 7 while the discharge waveforms are morphologically diverse, requiring specialized epileptologists to interpret their significance. 8 Therefore, enhanced knowledge of the clinical characteristics of ADEP patients can help in the early identification of such patients for subsequent stratification and management, saving limited resources for electrophysiologic examinations.
Amyloid-β (Aβ) deposition is a hallmark pathological marker in patients with AD and is further considered to be the earliest pathophysiologic change to occur in the AD disease spectrum continuum. This factor has further been shown to play an important role in AD-combined seizures and SEA.8,9 Large population-based cohort studies have shown significantly lower cerebrospinal fluid Aβ42 levels in patients with ADEP compared to those without epilepsy, 10 whereas a reduced plasma Aβ42/Aβ40 ratio in middle-aged and older adults has been associated with a subsequent increased risk of epileptogenesis. 11 Further, spontaneous seizures and SEA have been identified in a variety of AD model mice with abnormal Aβ deposition and have a discharge pattern very similar to that of human temporal lobe epilepsy patients.12,13 However, there have been no reports of brain Aβ burden in patients with ADEP.
In this study, we compared the clinical characteristics of AD patients with or without epilepsy and matched patients with late-onset epilepsy, and further quantified the spatial pattern of Aβ loading in the three patient groups using Aβ positron emission tomography (PET). We hypothesised that patients with ADEP may have unique clinical and Aβ depositional features that could aid in early recognition.
Methods
Study population
We recruited participants treated at the tertiary epilepsy centre and memory clinic at the West China Hospital of Sichuan University between February 2023 and October 2023. Ethical approval for this study was obtained from the Biomedical Research Ethics Committee of the West China Hospital of Sichuan University, and the trial process followed the Declaration of Helsinki. This study was registered with the China Clinical Trial Registry under registration number ChiCTR2300069032. Inclusion criteria for the ADEP group, the AD group and the late-onset epilepsy group (LOEP) were as follows: (1) age 60–75 years; (2) a diagnosis of AD, and a Clinical Dementia Rating (CDR) score of ≤1 with or without epilepsy; and (3) a diagnosis of LOEP (age at first seizure ≥55 years), with an as yet unspecified etiology (excluding stroke, tumors, encephalitis, etc.) 14 ; (4) Participants agreed to participate in the study and voluntarily signed an informed consent form. AD diagnosis met the National Institute on Aging-Alzheimer's Disease Association (2018 edition) criteria for likely AD diagnosis. Epilepsy diagnosis met the diagnostic criteria in line with the International League Against Epilepsy (ILAE) Diagnostic Criteria for Epilepsy (2014 edition), with both diagnoses confirmed by two neurologists. The exclusion criteria included: (1) epilepsy secondary to cerebrovascular disease, traumatic brain injury, infection, etc., or with a definite epileptic focus such as cortical dysplasia or tuberous sclerosis; (2) diagnosis of a specific subtype of AD, such as posterior cortical atrophy, etc.; (3) patients with a family history of early onset AD or known early onset AD mutation; and (4) a concomitant history of other major neurologic or psychiatric disorders, such as Parkinson's disease, stroke, schizophrenia, alcohol- or substance abuse-induced dementia, multiple sclerosis or other demyelinating diseases, encephalitis or meningitis, untreated vitamin B12 deficiency, severe periventricular white matter disease or white matter lesions greater than grade 4; (5) other major systemic diseases, severe organ dysfunction, and malignant tumors; (6) contraindications to magnetic resonance imaging (MRI) or PET scanning, including claustrophobia (e.g., history of claustrophobia, metal implants or severe alcohol allergy, etc.).
Healthy controls (HC) were recruited concurrently during the study, for whom the inclusion criteria were as follows: (1) a score of ≥28 on the Brief Mental State Examination (MMSE), a CDR score of 0, and no cognitive problems reported by the person or his/her family members; and (2) normal magnetic resonance imaging (MRI) results of the brain, or age-appropriate atrophy, with no neurological disorders that might affect cognition. Written informed consent was obtained from all participants.
Clinical information collection and apolipoprotein genotyping
Basic demographic information regarding the subjects’ age, handedness, height, weight, years of education, blood pressure, history of hypertension, history of hyperlipidemia, and history of diabetes mellitus was collected. Patients were also questioned in detail regarding their dementia and epilepsy-related medical history (including age of onset, seizure type and frequency, current neuropsychiatric medications, history of previous trauma, family history, etc.), as well as general information including occupation, place of residence (rural or urban area), history of smoking, history of alcohol consumption, and whether they had any exercise habit (defined as an average of at least 1 time per week of >30 min of moderate-intensity aerobic exercise, including walking, running, cycling, etc.), in addition to other sociological information. In addition, all participants underwent outpatient EEG recordings. The seizure onset date was further obtained by asking patients and caregivers when they noticed the first seizure. Additionally, we reviewed medical records to verify and ensure the accuracy of the reported timing and details of the first seizure.
Blood samples were collected from the median elbow vein in the morning in the fasting state and sent to the Clinical Laboratory of West China Hospital of Sichuan University. The defined APOE single nucleotide variants APOE ε2, ε3, and ε4 (rs429358 C/T and rs7412C/T) were genotyped by real-time fluorescence quantitative polymerase chain reaction using nucleic acid detection reagents.
Neuropsychological assessment
All participants underwent standardized neuropsychological assessments in a quiet room. The MMSE, Montreal Cognitive Assessment (MoCA), and CDR were used for cognitive assessments. We further applied the Neuropsychiatric Inventory (NPI) to assess patients’ neuropsychiatric symptoms and the Alzheimer's Disease Cooperative Study-Ability for Daily Living Scale (ADCS-ADL) to assess instrumental and daily living abilities. In addition, we reported patients’ anxiety and depressive symptoms (generalized anxiety scale [GAD-7], Patient Health Questionnaire-9 [PHQ-9]) and sleep quality (Pittsburgh Sleep Quality Index [PSQI]).
PET-MRI imaging, preprocessing, and analysis
18F-Florbetapir was produced and processed at a certified PET manufacturing site in accordance with Good Manufacturing Practices, and subsequently shipped to our institution's PET Imaging Centre for use in the visualization of the subjects’ brain Aβ load. PET scans were acquired using A PET/MR scanner (SIGNA PET/MR, GE Healthcare, Boston, MA). Images were all acquired 45–50 min after intravenous injection.
The Slicer (Version 5.2.2) was applied for and visual inspection. The format conversion, image co-registration of PET and MRI data, image segmentation and normalization of MRI were then completed using software SPM12 in MATLAB (Version 2022 B), and all PET images were smoothed using an 8 mm FWHM Gaussian filter. The SUV values of 116 cortical regions as regions of interest (ROIs) were extracted using the MarsBar (Version 0.44) plug-in based on the anatomical autolabeling (AAL) partitioning of the Montreal Neurological Institute (MNI), and the normalized uptake value ratio (SUVR) was calculated using the cerebellum as a baseline. Statistical maps were saved as NifTI files and visualized using ggseg with R Studio (Version 4.2.2), and BrainNet Viewer toolbox(Version 1.61).15,16 More details can be found in the Supplemental Material.
Statistical analysis of demographic and clinical information
Demographic and clinical characteristics, as well as brain region SUVR values, of patients in the ADEP, AD, and LOEP groups were statistically analyzed using R (version 4.2.0). All comparisons were between-group analyses. Specifically, continuous variables (e.g., age, MoCA score, regional SUVRs) were compared between groups using the Mann–Whitney U test due to non-normal distribution. Categorical variables (e.g., sex, APOE ε4 carrier status) were assessed using the chi-square test. To examine relationships between SUVR values, MoCA score and clinical variables, we performed within-group spearman correlation analyses. The significance threshold for general statistical tests was set at p < 0.05.
For voxel-wise analysis of 18F-Florbetapir PET data, we adopted a standard approach using the two-sample t-test in SPM12 in MATLAB (Version 2022 B), with group comparisons performed between ADEP, AD, and LOEP. 17 As these were exploratory analyses, we prioritized sensitivity in terms of thresholds, initially applying a loose threshold of p < 0.001 (uncorrected), which was subsequently set to p < 0.05 (FDR-corrected, cluster-level). The thresholds are labelled in the figure legends.
Results
Participants
The demographic and basic clinical characteristics of patients with ADEP, AD, and LOEP are summarized in Table 1. The mean age of ADEP patients included in this study was 66.8 years. 64.3% were female and 35.7% were male.71.4% lived in urban areas. The average number of years of education is 7.5 years. Patients with AD and LOEP showed no significant differences from patients with ADEP in terms of age, sex, comorbidities, smoking, and drinking habits. A greater proportion of patients with ADEP performed daily exercise (p < 0.05). All participants included in this study were of Han ethnicity. No significant differences were found between the AD and ADEP groups(p = 0.12) or between the ADEP and LOEP groups (p = 0.41) in terms of years of education.
Participant demographics and clinical characteristics.
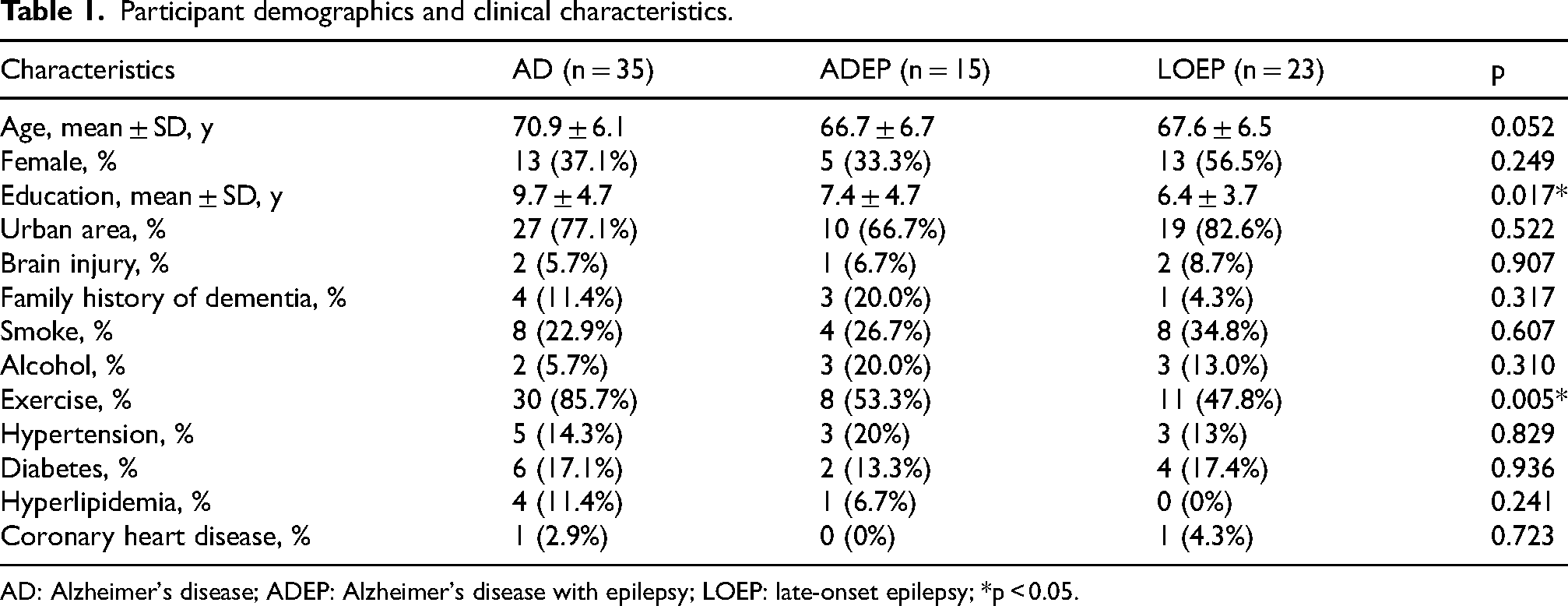
AD: Alzheimer's disease; ADEP: Alzheimer's disease with epilepsy; LOEP: late-onset epilepsy; *p < 0.05.
Demographic information on the healthy control group can be found in the Supplementary Material.
Clinical characteristics
The age at the first seizure in ADEP patients was 64.6 years. As shown in Table 2, ADEP patients had a matched course of dementia and epilepsy with AD patients and LOEP patients, respectively. Further, 80% of the ADEP patients had already started at least single ASMs therapy, with initiation on average 2.3 years after the first seizure, which was significantly later than for LOEP patients (mean, 1.1 years). The ASMs of patients with ADEP included levetiracetam, valproic acid, oxcarbazepine, and topiramate, with levetiracetam being the most prevalent (n = 8), at dosages ranging from 500 to 1500 mg/day; 20% of patients with ADEP achieved complete seizure remission. Half of the patients with ADEP were using cognitive enhancers, including cholinesterase inhibitors and memantine, at the time of enrolment. Cognitive enhancers were started before the first seizure. One patient with ADEP was taking anxiolytic and depressant medications, which were initiated following the first seizure.
Onset, duration of disease and medication.
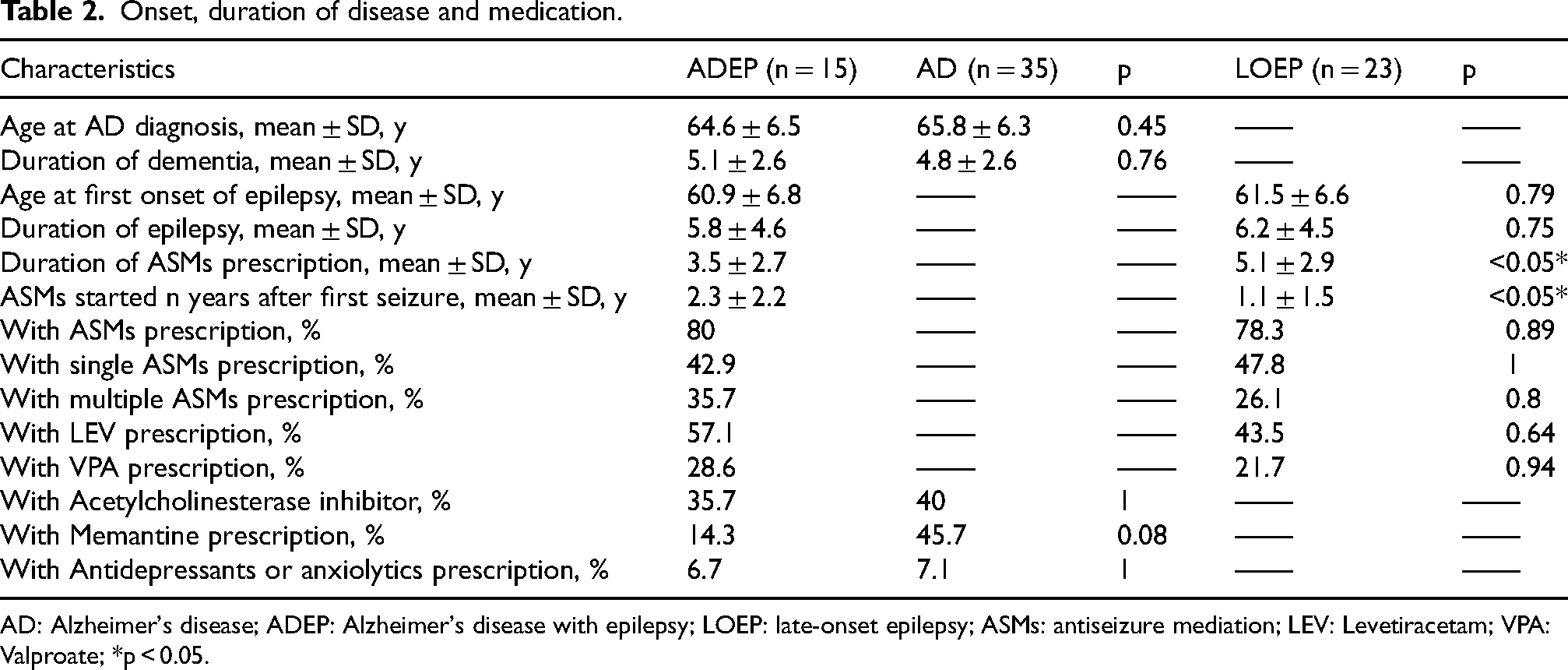
AD: Alzheimer's disease; ADEP: Alzheimer's disease with epilepsy; LOEP: late-onset epilepsy; ASMs: antiseizure mediation; LEV: Levetiracetam; VPA: Valproate; *p < 0.05.
Information on epilepsy types and semiology in patients with ADEP and LOEP is provided in Supplemental Tables 1 and 2. The most common classification was focal onset with impaired consciousness and motor seizures, which was identified in 10/15 of patients. The most common form of semiology was oropharyngeal automatisms. Focal progression to bilateral tonic-clonic seizures occurred in five patients.
Neuropsychological performance
The participants’ neuropsychological test scores are presented in Table 3. Patients with ADEP had higher MMSE (p < 0.01) and MoCA scores (p < 0.01) than those with AD without epilepsy. ADEP patients had higher CDR scores than LOEP patients (p < 0.01), as well as a higher ability to perform activities of daily living (p < 0.01). The psychiatric symptoms, depression-anxiety scores, and sleep scores of ADEP patients were not significantly different from those of epilepsy and LOEP patients without AD. Further, the proportions of APOE4 carriers and white matter high-signal grades were not significantly different between the groups.
Neuropsychological assessment, APOE4 genotype and white matter hyperintensities.
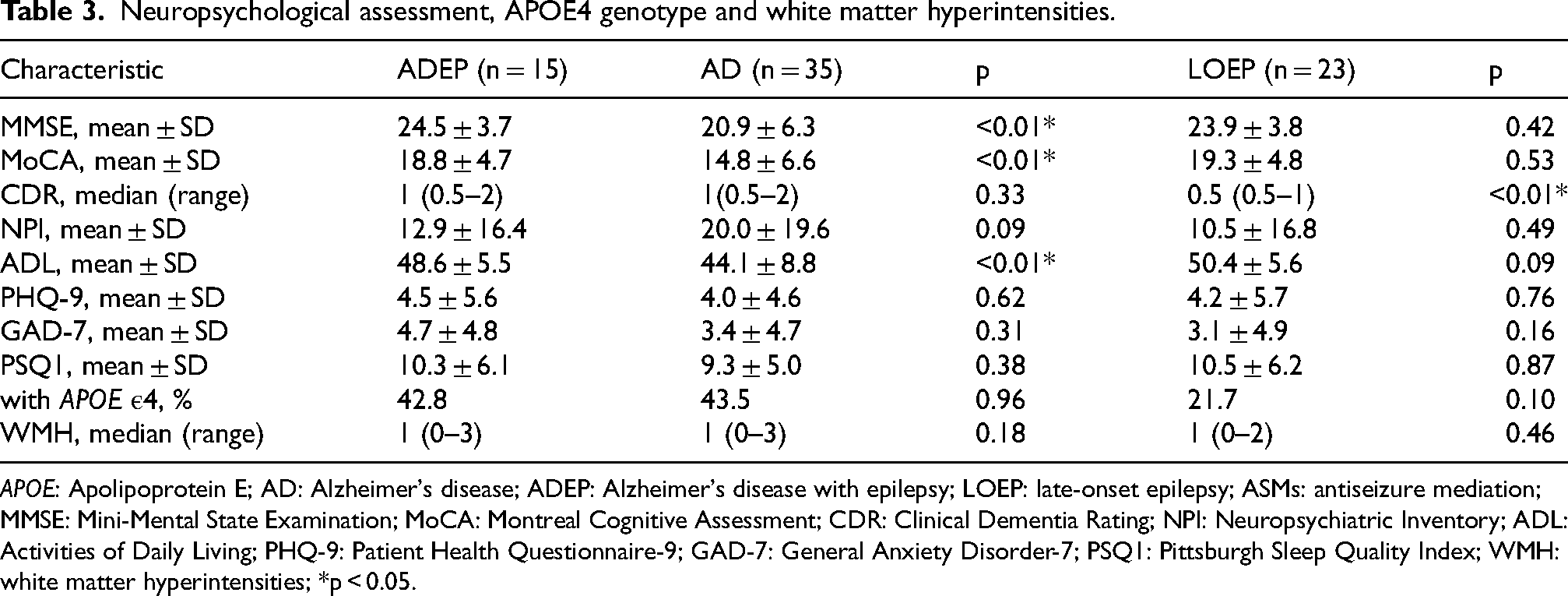
APOE: Apolipoprotein E; AD: Alzheimer's disease; ADEP: Alzheimer's disease with epilepsy; LOEP: late-onset epilepsy; ASMs: antiseizure mediation; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; CDR: Clinical Dementia Rating; NPI: Neuropsychiatric Inventory; ADL: Activities of Daily Living; PHQ-9: Patient Health Questionnaire-9; GAD-7: General Anxiety Disorder-7; PSQ1: Pittsburgh Sleep Quality Index; WMH: white matter hyperintensities; *p < 0.05.
Comparisons of deposition of Aβ
Significant intergroup differences were observed in whole-brain Aβ SUVR levels between the AD and LOEP groups (p < 0.01), the AD and HC groups (p < 0.01), the ADEP and LOEP groups (p < 0.01), and the ADEP and HC groups (p < 0.01).
In voxel-based analyses, patients with ADEP showed lower accumulation in the middle cingulate cortex than patients with AD (p < 0.05, FDR-corrected). After further relaxing the thresholds to enhance sensitivity, we identified regions of relatively low accumulation in the precuneus and extreme prefrontal cortex (p < 0.001, uncorrected, Figure 1(b)). Similarly, in the ROI-based analyses, we found that patients with ADEP had less deposition in the middle cingulate gyrus, superior orbitofrontal gyrus, middle orbitofrontal gyrus, fusiform gyrus, and insular gyrus than patients with AD (p < 0.001, uncorrected). To explore the factors influencing cognition and Aβ burden in ADEP patients, we performed spearman correlation analyses to assess the duration of epilepsy, seizure frequency, and years of ASMs use with MoCA scores, as well as the SUVR of the ROI in the middle cingulate gyrus of the 18F-Florbetapir PET.12 patients with ADEP with PET and MRI data were included in the analysis. No significant correlation was found (Figure 2). However, the duration of epilepsy and the ASM prescription duration showed a positive trend with MoCA scores, and a negative trend with Aβ deposition in the middle cingulate cortex. The sensitivity analysis regarding cognitive enhancers can be found in the Supplementary Material.
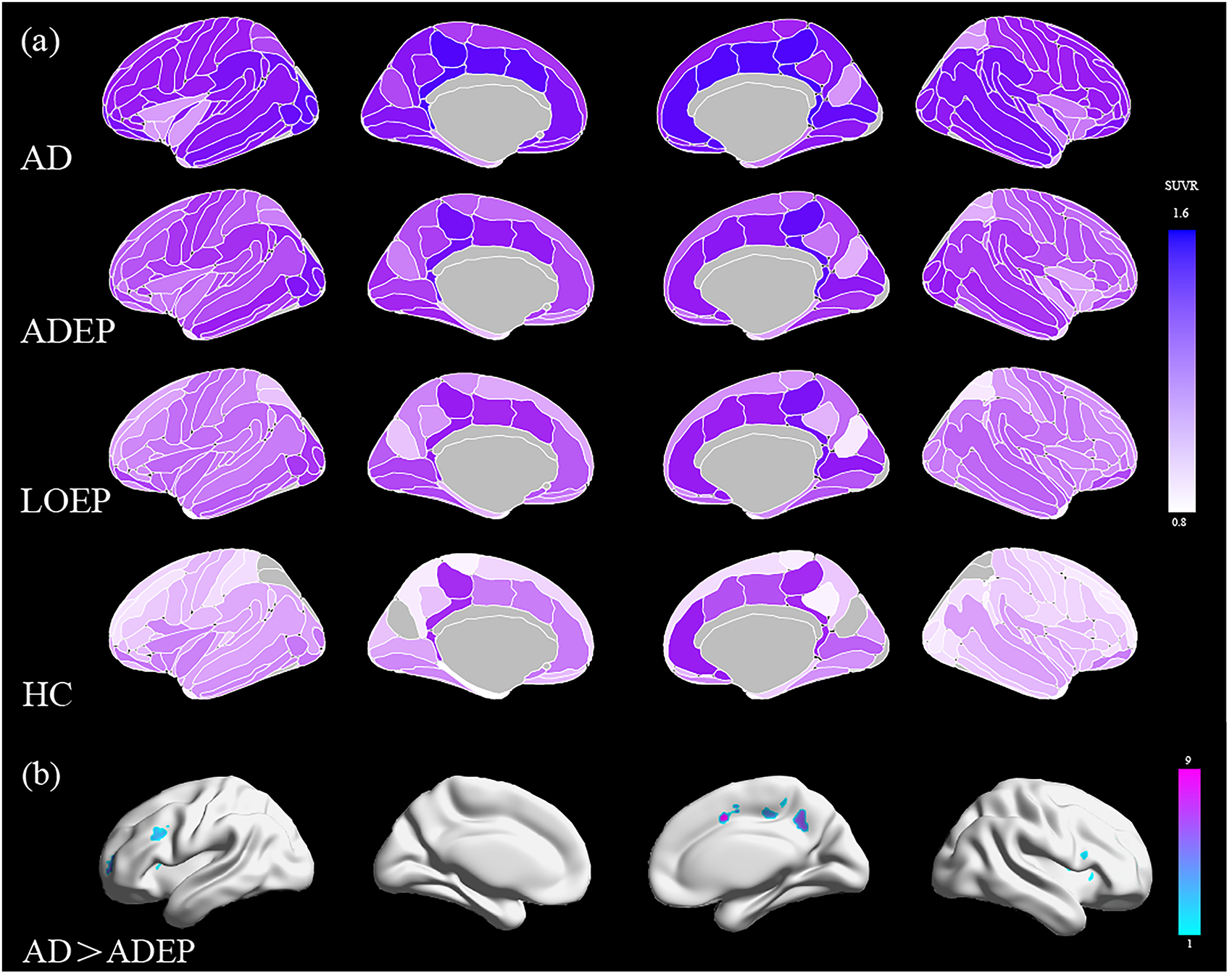
Spatial characterization of Aβ accumulation ADEP, AD, and LOEP patients. (a) Spatial patterns of amyloid deposition in AD, ADEP, LOEP, and HC based on ROI analysis; (b) Comparison of AD and ADEP amyloid deposition based on voxel analysis (p < 0.001, unadjusted).
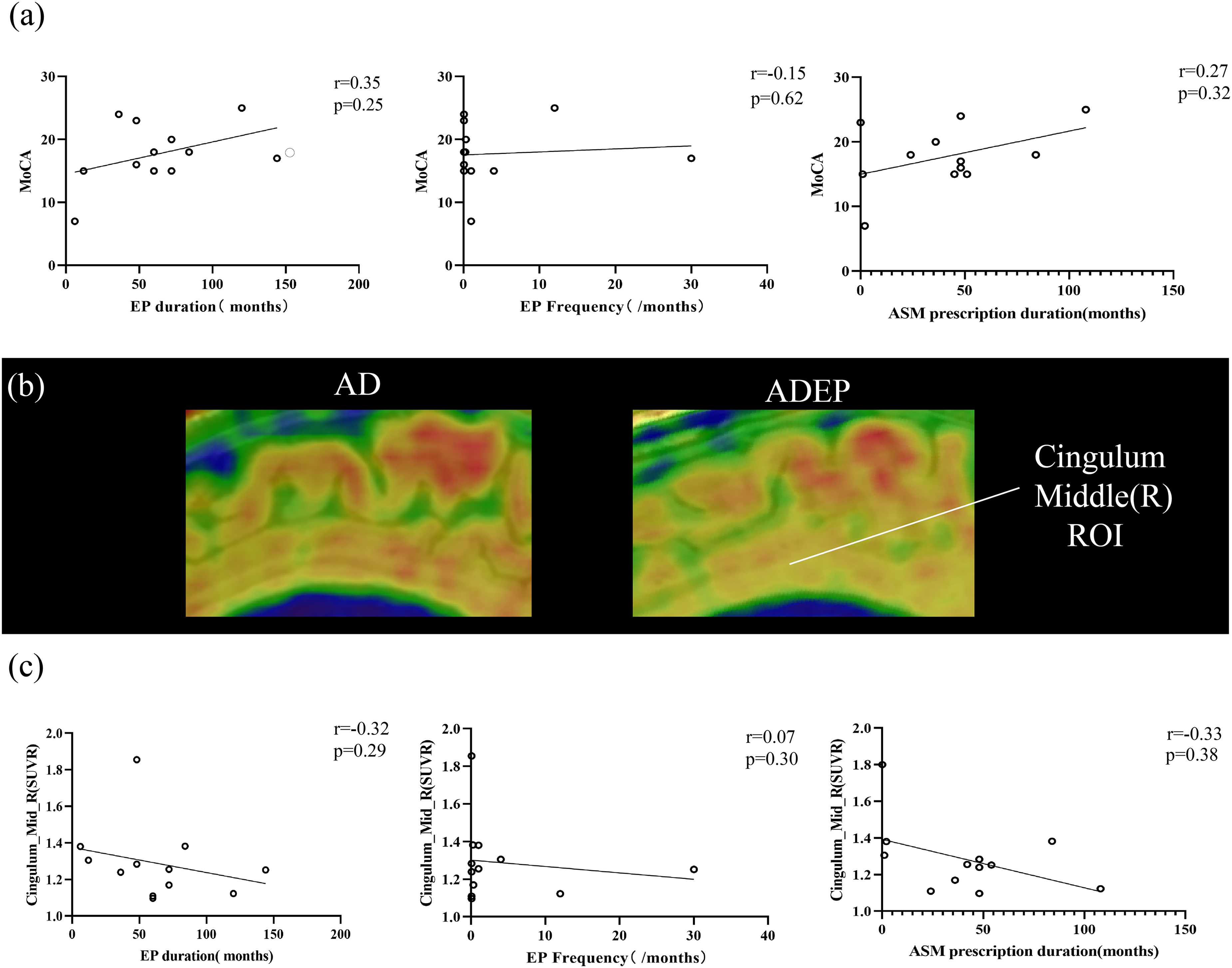
Characteristics of epilepsy and correlation with MoCA score and cingulum accumulation in ADEP patient. (a) Correlation of epilepsy duration, seizure frequency, and duration of antiepileptic drug administration with MoCA scores in ADEP patients; (b) AD patients have more cingulate gyrus deposits than ADEP patients; (c) Correlation of epilepsy duration, seizure frequency, and duration of antiepileptic drug use with cingulate gyrus deposition in ADEP patients.
Discussion
Alzheimer's disease and epilepsy have a strong bidirectional link. 18 However, it is difficult to recognize early, due in part to a lack of sufficient clinical experience and objective evidence to facilitate early screening and treatment of comorbidities. In the present study, we showed that seizures in patients with ADEP occur in the early stages following the onset of cognitive decline. Focal-onset motor seizures with impaired consciousness are the predominant type of seizures. Patients with ADEP scored significantly higher on cognitive tests than patients with AD without epilepsy when matched for course. PET/MRI analysis further showed that Aβ deposition in the middle cingulate gyrus was significantly lower in ADEP patients than in AD patients without epilepsy.
Consistent with previous studies, we observed that the first epilepsy seizures generally appeared in the early stages of cognitive decline, and were characterized by focal-onset nonconvulsive motor seizures, which could not be easily observed or recognized as the primary seizure manifestation.19,20 In terms of seizure symptoms, oropharyngeal automatism manifesting as chewing, pouting, smacking, and swallowing, and manual automatism manifesting as groping were most commonly observed. These seizure manifestations most commonly originated in temporal lobe epilepsy,21,22 which is consistent with the localization findings of previous electrophysiological studies of epilepsy in AD.7,8,23 At the same time, we observed a significant delay between diagnosis and the time of first medication in ADEP compared to LOEP, suggesting a deficit in the early diagnosis of ADEP. This may be due to the similarity of certain epilepsy symptoms and AD symptoms. Similar to automatisms, early AD may present with repetitive abnormal motor symptoms, such as pacing back and forth, fumbling with buttons, winding a rope, or repeatedly performing other movements, etc., which are also defined as mild behavioral disorders. Moreover, for general caregivers, it is also difficult to differentiate between transient disorders of consciousness caused by epilepsy, and the daily symptoms of apathy in patients with AD, which hampers early detection of epileptic symptoms in patients with AD.24,25
In terms of seizure control, only a small proportion of patients have achieved complete seizure freedom, which is inconsistent with the results of previous small-sample studies.6,20 In previous studies, 89.5% of patients were well controlled by a single ASM, and 63.1% achieved seizure freedom. We further observed a trend toward smaller doses of ASMs, such as levetiracetam and lamotrigine, in patients with ADEP in the present study compared to previous studies, while seizure frequency was more frequent, possibly explaining the difference in results. Moreover, large case-control studies have found that epilepsy accompanied by AD is associated with a high risk of recurrence and is more frequent. 26 However, further clinical trials with long-term longitudinal follow-ups and subgroup analyses comparing the selection and efficacy of ASMs in patients with ADEP are required to validate these findings.
During our measurements of Aβ in patients with LOEP of unknown etiology, we identified one case with amyloid deposition. The patient was a 64-year-old male with an APOE e3/e3 genotype who had experienced focal seizures since the age of 60. His primary seizure semiology included ictal gaze and phantom smells. The MoCA scores were 28, and the CDR was 0. His MRI findings were negative. Over the course of a one-year prospective follow-up, no significant cognitive decline was observed. Although we did not observe any significant differences in Aβ deposition between the LOEP group and the HC group, it is worth noting that the prevalence of Aβ positivity increases with age in cognitively normal older adults. 27 Longitudinal follow-up of cohorts of LOEP patients with Aβ abnormalities is essential to accurately stratify their risk of developing dementia. 12
To the best of our knowledge, this is the first report investigating the spatial characterization of Aβ deposition in ADEP patients. Aβ deposition in the patients in the present study was predominantly concentrated in the cingulate cortex, which is consistent with previous reports, and in line with the pathway of early Aβ deposition observed in patients with classical AD.26,28,29 In voxel-based and SUVR analyses based on ROIs, we observed significantly less Aβ deposition in the anterior middle cingulate gyrus cortex primarily in ADEP patients than in AD patients, with a similar trend toward less deposition in the orbitofrontal gyrus and fusiform gyrus, and precuneus. In addition, in the neurocognitive assessment of patients with ADEP, we found that both the MMSE and MoCA scores were higher than those of the control AD group, which is not entirely consistent with the findings of previous studies concerning AD with SEA or epilepsy.13,30 Several previous studies have suggested that SEA and seizures in patients with AD may be associated with faster cognitive decline31,32 . It has also been shown that there is no significant difference in the rate of progression of MMSE scores or dementia conversion between ASM-treated preexisting AD patients with epilepsy and preexisting AD patients without epilepsy. The reason for the discrepant results is uncertain. We speculate that the difference is due to the following aspects. First, early-onset epilepsy may draw increased attention from physicians and caregivers, leading to better care such as medication reminders and extra cognitive training, which could potentially help delay cognitive decline. Secondly, fewer depositions and higher cognitive scores revealed a trend in the correlation analyses related to epilepsy duration and duration of ASMs use, suggesting a potential influence of ASMs and seizures on the course of AD. The middle cingulate cortex is predominantly connected to areas involved in motor control and decision making, response selection, attentional processing, conflict monitoring, and errors.33–35 Levetiracetam, valproic acid, and topiramate have been reported to improve learning memory deficits in transgenic mice by increasing Aβ clearance through the upregulation of Aβ transport across the blood-brain barrier and autophagic digestion. 36 Levetiracetam has further been reported to increase MMSE scores and improve spatial memory and executive function in patients37,38; however, its effects are dose-dependent, and require early and prolonged administration.39,40 Additionally, the impact of epilepsy on brain network connectivity in AD patients could be a potential reason for the discrepancy with the findings of SEA studies. 41 Functional imaging studies of the pathophysiological continuum of AD have found that compensatory mechanisms appear in the form of increased functional connectivity in the early stages of AD, whereas compensatory mechanisms break down due to increased localized and global neurodegenerative pathology in more advanced stages.42,43 Brain network studies on AD seizures have suggested that highly epileptogenic nodes are present in the cingulate, orbitofrontal, and pontine cortices, 44 which occur as compensatory connectivity nodes for the decoupling of autobiographical memory networks in the early stages of dementia according to the hypothesis of functional imaging. 45 The generation of epileptic seizures in the early stages of AD may be a compensatory mechanism to restore neural oscillatory connectivity.45,46
Our study has several limitations. Firstly, the study's conclusions are based on a relatively small sample size (15 ADEP patients), which may limit the statistical power and generalizability of the findings and further observations are needed. Second, we only observed patients cross-sectionally in a single center, without performing long-term follow-up to understand the prognosis of the patients, and the longitudinal changes in the rate of cognitive decline and Aβ accumulation over time. Also, the chance of co-epilepsy will probably exist in the future in the current AD group of patients. Further, we were unable to exclude the role of cognitive enhancers in the development of epilepsy. In addition, we did not record long-duration EEG or magnetoencephalography in the included patients with AD to stratify them into subclinical epileptiform discharges or further measure the correlation between discharge characteristics and depositional features. Finally, the types of seizures in our included patients with ADEP did not include myoclonic seizures, which have further been reported as common in patients with ADEP.
Despite these limitations, our study is the first to report the cognitive features and differential amyloid spatial deposition patterns in patients with ADEP, adding the most recent objective imaging data and clinical evidence to the study of Alzheimer's disease-associated epilepsy to further reduce comorbidity diagnostic uncertainty in the future. Our study reported better cognitive function and milder Aβ deposition in the middle cingulate gyrus in ADEP patients compared with AD patients without epilepsy, indicating that abnormal neuroelectric activity of seizures and use of ASMs may be associated with slower Aβ deposition in the brain of ADEP patients. Future studies are required to prospectively observe the complex interactions of AD development, Aβ deposition, tau pathology, epileptiform discharges, and ASMs, as well as to develop and validate new therapeutic approaches and technologies in this regard.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251360425 - Supplemental material for Cognitive and spatial patterns of amyloid-β burden in Alzheimer's disease with epilepsy
Supplemental material, sj-docx-1-alz-10.1177_13872877251360425 for Cognitive and spatial patterns of amyloid-β burden in Alzheimer's disease with epilepsy by Yilin Xia, Leihao Sha, Muchan Tao, Anjiao Peng, Hua Li, Yusha Tang, Wanlin Lai, Zhu Liu, Ximeng Yang, Sijia Basang, DeBo Li and Lei Chen in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors gratefully acknowledge Huawei Cai and Fanglan Li from Department of Nuclear Medicine of West China Hospital for their insightful suggestions on the research design. The authors also thank Kai Xu from Lung Cancer Center of West China Hospital for his valuable assistance with the results visualization.
Ethical considerations
The Biomedical Research Ethics Committee of the West China Hospital at SichuanUniversity approved our interviews (approval: 2023(242)) on Month 01, 2023.
Consent to participate
Respondents gave written consent for review and signature before starting interviews.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by Sichuan Science and Technology Program (2023ZYD0075).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.