
Abstract
We evaluated whether apolipoprotein E (APOE) genotype-guided slow titration of monoclonal antibodies reduced amyloid-related imaging abnormalities (ARIA) in Alzheimer's disease. We retrospectively analyzed ARIA incidence in 25 patients on aducanumab and 19 patients on lecanemab on a genotype-informed protocol in a private practice setting. ARIA-E and ARIA-H each occurred in 4% of the aducanumab group and 5% of the lecanemab group. Plaque clearance was achieved in 50% of evaluable aducanumab patients and 26.3% of lecanemab patients. Compared to clinical trial ARIA rates, our results suggest that individualized, genotype-informed titration improves safety although plaque clearance rates were less robust.
Keywords
Introduction
Monoclonal antibodies (mAb) targeting amyloid-β (Aβ) plaques, including aducanumab and lecanemab, have shifted the treatment landscape for Alzheimer's disease (AD). However, amyloid-related imaging abnormalities (ARIA) with edema (ARIA-E) and hemorrhage (ARIA-H), remain significant safety concerns, particularly in apolipoprotein E (APOE) ɛ4 carriers, with the highest risk in ɛ4 homozygotes.1–4
While pivotal trials employed fixed titration schedules, emerging real-world evidence suggests that slow, individualized titration may mitigate ARIA risk. For example, modified dose escalation with donanemab significantly reduced ARIA incidence. 5 Here, we present outcomes from a real-world cohort treated with aducanumab and lecanemab using an APOE genotype-informed slow titration strategy, evaluating ARIA incidence and plaque clearance. These findings may inform clinical application of currently approved monoclonal antibodies (mAbs).
Methods
Study design and patients
We conducted a retrospective chart review at a single private practice, including patients with mild cognitive impairment with AD pathology or early symptomatic AD initiated on aducanumab (n = 25) or lecanemab (n = 19) between January 2021 and December 2023. Institutional Review Board approval was obtained prior to study initiation. Due to the retrospective nature of the study, informed consent was not required.
Inclusion criteria
Clinical diagnosis of mild cognitive impairment (MCI) or mild dementia due to AD.
Confirmed amyloid positivity by PET imaging or cerebrospinal fluid biomarkers.
Availability of APOE genotype.
Minimum of six months of treatment.
Titration protocols
Aducanumab was initiated at 1 mg/kg monthly for 3 months, then up-titrated by 1 mg/kg every 2 months (APOE ɛ4/ɛ4 and APOE ɛ4/-) or monthly (APOE -/-), with 10 mg/kg reached at about 21 and 12 months respectively.
Lecanemab was initiated at 5 mg/kg for four biweekly infusions, then up-titrated by 1 mg/kg every 8 weeks (APOE ɛ4/ɛ4), 6 weeks (APOE ɛ4/-), or 4 weeks (APOE -/-), with 10 mg/kg reached at about 12, 10, and 7 months, respectively.
All patients underwent standardized clinical examinations (monthly for aducanumab, bi-weekly for lecanemab) and MRI monitoring with additional imaging after each dose escalation. Titration was paused or delayed upon detection of moderate ARIA.
Outcome measures
Incidence of ARIA-E and ARIA-H.
Amyloid plaque clearance defined as amyloid-PET conversion to plaque-negative status.
Results
Patient characteristics are shown in Table 1. ARIA outcomes and plaque clearance are summarized in Table 2. One patient with a PSEN1 mutation and diffuse amyloid deposition began aducanumab at age 31, three years after a positive amyloid scan. Two patients with low Mini-Mental State Examination scores due to expressive aphasia also initiated aducanumab.
Patient characteristics.
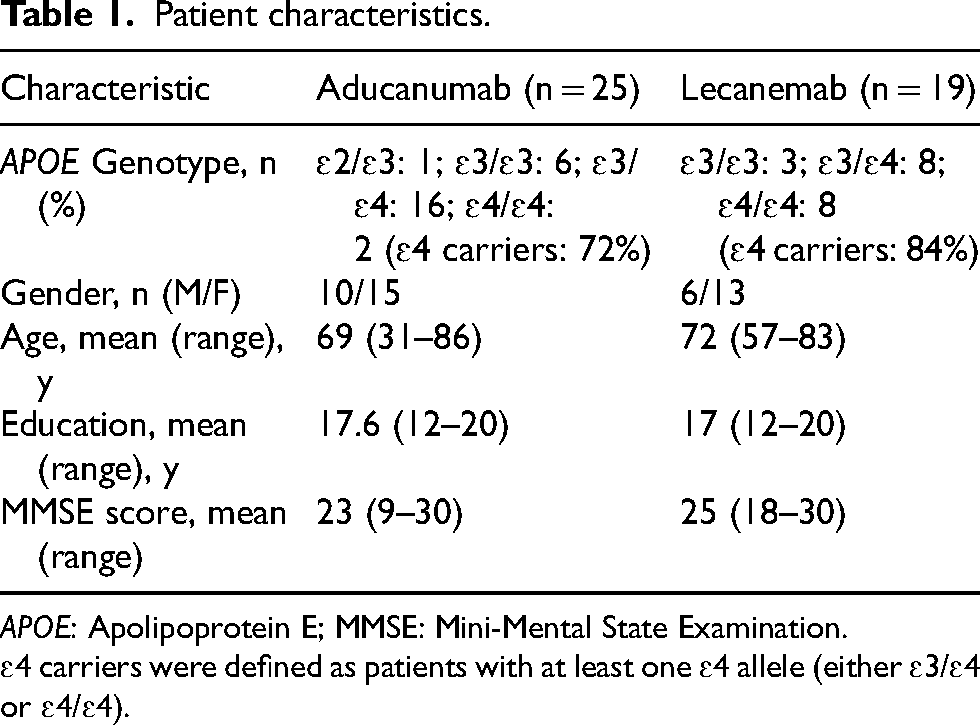
APOE: Apolipoprotein E; MMSE: Mini-Mental State Examination.
ɛ4 carriers were defined as patients with at least one ɛ4 allele (either ɛ3/ɛ4 or ɛ4/ɛ4).
Summary of outcomes (ARIA incidence and plaque clearance).

ARIA-E: amyloid-related imaging abnormalities–edema; ARIA-H: amyloid-related imaging abnormalities–hemorrhage.
Among patients receiving aducanumab, an APOE ɛ4/ɛ4 individual developed moderate, asymptomatic ARIA-E detected on routine imaging 468 days after starting treatment, shortly after a dose increase to 8 mg/kg. An APOE ɛ3/ɛ4 patient developed mild, asymptomatic ARIA-H on MRI 147 days after initiation, also following a dose increase.
Two patients who remained plaque-positive on aducanumab were switched to lecanemab once it became available and are included in the lecanemab analysis. One of these patients (APOE ɛ3/ɛ4), developed mild ARIA-E 71 days after switching. Another patient, not previously on aducanumab (APOE ɛ4/ɛ4), developed asymptomatic mild ARIA-H 401 days after starting lecanemab.
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Discussion
Our findings demonstrate that APOE genotype-guided slow titration strategies significantly reduce ARIA incidence although plaque clearance was not as robust and may take longer to achieve. Compared with pivotal trial data—where ARIA incidence in APOE ɛ4 carriers reached 35–40%—our observed rates were substantially lower (4–5%).1,3,4,6 In our cohort, 72% of aducanumab-treated patients and 84% of lecanemab-treated patients were APOE ɛ4 carriers.
Recent work with donanemab also supports this approach: modified slower dose titration reduced ARIA-E from 24% to 14%, and from 57% to 19% in ɛ4 homozygotes, without compromising plaque clearance. 5
In our cohort, aducanumab plaque clearance rates (50%) were consistent with EMERGE and ENGAGE trial benchmarks (∼30–40% amyloid reduction at 18 months). 4 Lecanemab plaque clearance (26%) was lower than the 68% plaque-negativity rate reported in the CLARITY trial. 3 However, we did not measure percentage reductions in amyloid burden, and our patients may have started with higher baseline levels, limiting plaque negativity despite possible signal reduction.
Notably, some patients cleared plaque at doses as low as 6 mg/kg on aducanumab, consistent with trial data. 7 ARIA onset was delayed (median ∼300 days) supporting the safety of slow escalation.
The biological rationale for slow titration is grounded in Aβ clearance mechanisms. Solubilized Aβ is cleared via several pathways: transport across the blood-brain barrier (BBB) into vascular smooth muscle cells, along perivascular routes to the glymphatic system or through neuronal, glial or enzymatic degradation. 8
Rapid solubilization may overwhelm these systems, promoting vascular amyloid deposition, inflammation and BBB disruption, ultimately leading to ARIA-E and ARIA-H.
APOE proteins facilitate Aβ clearance, but the ɛ4 isoform is less effective, making ɛ4 carriers particularly vulnerable to ARIA with mAb therapy. 8
A slower titration likely reduces the sudden load of solubilized Aβ, giving clearance pathways time to adapt and possibly allowing the BBB to repair itself. In a prior study of 20 AD patients (19/20 ɛ4 carriers), none developed ARIA during slow-titrated, low-dose aducanumab over 8 months, the period of highest ARIA risk. 9
Our observations also align with studies like ICEBERG (2024), which suggest that vascular amyloid (cerebral amyloid angiopathy, or CAA) and microvascular fragility—not simply parenchymal plaques—may drive ARIA risk. 10 CAA affects ∼80% of AD patients and weakens vascular integrity, leading to hemorrhagic and ischemic lesions8.
Thus, mitigating ARIA may require accommodating the vascular amyloid burden alongside plaque clearance goals.
Our study limitations include retrospective design, limited sample size, and potential imaging variability. Notably, amyloid clearance rates were modest (26–50%) compared to nearly 70–80% clearance rates reported in pivotal trials, possibly reflecting shorter follow-up durations and patient heterogeneity. Additionally, because this was a clinical study, quantitative measures of amyloid burden, such as centiloid values, were unavailable. Nevertheless, these real-world observations support further prospective validation.
Conclusions
As monoclonal antibody use becomes more widespread, strategies to mitigate ARIA will be critical. APOE genotype-guided slow dose titration appears effective at reducing ARIA risk although plaque clearance was reduced and may require a longer treatment course.
Especially in APOE ɛ4 carriers, slow titration may better accommodate concurrent CAA and allow BBB stabilization, decreasing both ARIA-E and ARIA-H incidence.
Future research should focus on algorithm-driven titration schedules personalized to genetic risk, co-morbidities such as CAA, baseline amyloid burden, and emerging plasma biomarkers (e.g., p-tau217) to further enhance safety and efficacy.
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
Consent to participate
The requirement for informed consent to participate has been waived by the Institutional Review Board.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported by NIH grant P30AG066512 (to TW); All of Us Research Program.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.