
Abstract
Background
Cerebrospinal fluid (CSF) core biomarkers play a pivotal role in the biological diagnosis of Alzheimer's disease (AD). While various commercial assays and kits are available for quantifying these biomarkers, their performance across diverse clinical settings remains insufficiently evaluated.
Objective
This study aimed to compare the diagnostic accuracy of AD core biomarkers using four measurement methods in a Chinese population and to establish method-specific cutoff values tailored to different clinical scenarios.
Methods
A total of 309 participants were enrolled from the PUMCH dementia cohort, comprising 176 AD, 114 non-AD dementia cases, and 19 cognitively normal controls (CN). For biomarker quantification, we employed one manual immunoassay (INNOTEST, conducted in two independent laboratories) and two fully automated immunoassay platforms (Lumipulse G and Roche Elecsys). These methods were used to measure CSF Aβ1–40, Aβ1–42, t-tau, and p-tau181, and to calculate three biomarker ratios (Aβ1–42/Aβ1–40, t-tau/Aβ1–42, and p-tau181/Aβ1–42).
Results
Our findings provide method-specific and clinical context-optimized cutoff values for each application scenario including clinically diagnosed AD versus non-AD dementia, amyloid PET-positive versus PET-negative dementia, and AD versus CN. The accuracy of differential diagnosis was higher using biomarker ratios (Aβ1–42/Aβ1–40, t-tau/Aβ1–42, p-tau181/Aβ1–42) than absolute values. Most of the high accuracy was achieved using automated assays especially Lumipulse G rather than manual assays.
Conclusions
In this first comparative study of three immunoassays in a Chinese cohort, automated assays demonstrated superior performance compared to manual assays. We established assay-specific cutoff values tailored to different clinical contexts in a Chinese population.
Introduction
Alzheimer's disease (AD) represents a significant public health challenge in China, underscoring the urgent need for early and precise diagnostic strategies. Cerebrospinal fluid (CSF) core biomarkers, including amyloid-β (Aβ)1–40, Aβ1–42, t-tau, and p-tau181, play a pivotal role in the biological diagnosis of AD and constitute essential components of the AD biomarker framework.1,2 These biomarkers are extensively utilized in research settings to facilitate early and accurate diagnosis of AD, enable prediction of disease progression trajectories, and optimize the design of disease-modifying clinical trials.3–5 Numerous cohort studies, including those with postmortem-confirmed AD cases, have demonstrated the clinical utility of CSF biomarkers, particularly biomarker ratios (Aβ1–42/Aβ1–40, t-tau/Aβ1–42, and p-tau181/Aβ1–42), in facilitating accurate diagnosis, differential diagnosis, and prediction of disease progression in AD.6,7
To date, immunoassay-based platforms have emerged as the predominant methodology for quantifying Aβ1–40, Aβ1–42, t-tau, and p-tau181 biomarkers in both research and clinical settings. 8 The INNOTEST platform employs a manual enzyme-linked immunosorbent assay (ELISA) methodology, requiring labor-intensive manual handling of reagent addition and removal processes using multi-well plates. In contrast, the Fujirebio Lumipulse G system and Roche Elecsys platforms represent automated immunoassay technologies, offering enhanced analytical performance with superior repeatability and intermediate precision. 9 Previous comparative studies have demonstrated that the Lumipulse G and Elecsys CSF AD biomarker assays exhibit superior analytical performance and enhanced clinical utility when compared to non-standardized manual methodologies, such as the INNOTEST ELISA platform. 10 Consequently, automated immunoassay platforms have become the preferred methodology for CSF AD biomarker quantification, significantly reducing both inter- and intra-laboratory variability while enhancing measurement reproducibility.
Despite the widespread availability of commercial assays and kits for biomarker analysis, their broader implementation in clinical practice faces several significant challenges. Foremost among these is the lack of universal standardization and quality control protocols for CSF collection and analysis. Although the Alzheimer's Association has developed a simplified and standardized pre-analytical protocol for CSF collection and processing to facilitate routine clinical implementation, comprehensive adoption remains limited. 11 Secondly, the interpretation of results faces significant challenges due to methodological variability, particularly when comparing automated and manual assay platforms. Thirdly, even within the same assay system, the establishment of appropriate cutoff values requires careful consideration of racial/ethnic differences and specific clinical contexts, such as distinguishing AD from non-AD dementia or predicting the conversion from mild cognitive impairment (MCI) to AD.
Despite the availability of commercial kits, assays, and platforms in China, there remains a critical gap in systematic comparative evaluations of these methodologies within the Chinese population. Furthermore, population-specific cutoff values for AD core biomarkers across different assay platforms have not been established for Chinese individuals. This study aims to comprehensively evaluate the diagnostic performance of AD core biomarkers using multiple analytical platforms in the Chinese population. Additionally, we seek to establish and compare method-specific cutoff values tailored to distinct clinical scenarios, including: (1) differentiation between clinically diagnosed AD and non-AD dementia, (2) discrimination of amyloid PET-positive and PET-negative cases, and (3) distinction between AD patients and cognitively normal controls.
Methods
Participants
Study participants were systematically recruited from the dementia registry maintained by the Department of Neurology at Peking Union Medical College Hospital (PUMCH Dementia Cohort). The research protocol was conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki (1975) and its subsequent amendments. The Institutional Review Board (IRB) of Peking Union Medical College Hospital granted ethical approval for this study (Approval No. JS2810).
A total of 290 patients were enrolled in the study, of whom 176 met the clinical diagnostic criteria for probable Alzheimer's disease as defined by the 2011 National Institute on Aging-Alzheimer's Association (NIA-AA) guidelines 12 and agreement with lumbar puncture. 114 patients were diagnosed with non-AD dementia, including frontotemporal dementia (n = 43) that were diagnosed according to the established criteria by McKhann et al., 13 vascular dementia (n = 25) diagnosed according to the International Society of Vascular Behavioral and Cognitive Disorders (VASCOG) criteria, 14 dementia with Lewy body/Parkinson syndrome (n = 20) diagnosed using McKeith et al. and Emre et al. criteria,15,16 normal pressure hydrocephalus (n = 11), neuronal intranuclear inclusion body disease (n = 3), Creutzfeldt- Jacob disease (n = 2), amyotrophic lateral sclerosis (n = 1), Huntington's disease (n = 1), adult onset leukoencephalopathy with spheroid axons and pigmented glia (n = 1) and unclassified dementia (n = 7). Comprehensive clinical information was obtained through structured interviews with reliable family members or caregivers. All participants underwent a systematic physical examination, extensive laboratory investigations (including hepatic and renal function panels, homocysteine levels, thyroid function tests, folic acid and vitamin B12 measurements, blood ammonia analysis, and rapid plasma reagin testing), and brain magnetic resonance imaging to support accurate diagnosis and differential diagnosis. A detailed neuropsychological assessment protocol was implemented, comprising initial screening tests followed by domain-specific cognitive batteries. Additionally, 19 cognitively normal (CN) control participants were recruited from healthy volunteers and from individuals undergoing CSF analysis for clinical indications (e.g., peripheral neuropathy) who demonstrated no evidence of cognitive impairment upon comprehensive evaluation.
CSF collection
CSF samples were collected via gravity drip method into Eppendorf Protein LoBind® polypropylene tubes (Eppendorf AG, Hamburg, Germany) to minimize protein adsorption. Immediately after collection, the samples were aliquoted into 0.5 mL Eppendorf Protein LoBind® polypropylene tubes and subsequently stored at −80°C in a temperature-monitored ultra-low temperature freezer to ensure sample integrity. All samples were maintained under these conditions until batch analysis to ensure consistency in the analytical process. Based on the Alzheimer's Association international guidelines, 11 to ensure sample quality, CSF samples were processed without centrifugation when no visible blood contamination was observed. In cases where visible blood contamination was present, the samples were centrifuged at 2000 × g for 10 min at room temperature (20–25°C) to remove cellular components before aliquoting and storage. The samples were stored and performed at clinical biobank (ISO20387), Peking Union Medical College Hospital, Chinese Academy of Medical Sciences.
PET scan
Amyloid PET scan was performed in part of the participants. Acquisitions were conducted in accordance with the guidelines of the Alzheimer's Association Amyloid Imaging Task Force and the Society of Nuclear Medicine and Molecular Imaging (SNMMI). 17 Brain images were collected with a specialized PET/CT scanner (PoleStar m660; SinoUnion Healthcare Inc., Beijing, China). A low-dose CT scan of the brain (120 kV, 260 mAs, 2.5 mm layer thickness, 512 × 512 matrix) and a PET scan (512 × 512 matrix) were performed 45 min following the intravenous administration of 307–470 MBq (8.3–12.7 mCi) of 18F-flobetapir. Reconstruction of PET images employed the ordered-subsets expectation maximization (OSEM: 10 subsets, 4 iterations, FWHM of 2.5 mm) with the time-of-flight (TOF) technique. The diagnosis of PET-positive or negative was made by consensus of a diagnosing group including two professional neurologists and two radiologists.
CSF analysis
One manual immunoassay (INNOTEST, Fujirebio, Belgium) and two fully automated immunoassays (Lumipulse G, Fujirebio, Belgium and Roche Elecsys, Roche Diagnostics, Switzerland), were selected and used for the measurement of CSF core biomarkers. On the day of analysis, CSF samples were thawed at room temperature, and the storage tubes were thoroughly vortexed. The ELISA kits were employed following the manufacturer's instructions. INNOTEST ELISA measurements were conducted parallelly in two qualified laboratories with different batches, and one of these laboratories also performed the two fully automated immunoassays as part of this work. Only measurements where quality control (QC) results were within the allowable range set by the manufacturer were considered valid and results of clinical samples were used for further analysis. According to the manufacturer's instructions, the Lumipulse G1200 fully automated immunoassay system, coupled with Lumipulse® G Aβ1–40, Aβ1–42, t-tau, and p-tau181 kits, employing a two-step sandwich chemiluminescent enzyme-immunoassay, was utilized for measurements of another aliquot. 18 Additionally, the Roche Cobas e801 chemiluminescence analyzer, utilizing second-generation Elecsys Aβ1–42, t-tau, and p-tau181 kits, based on an electrochemiluminescence immunoassay, was used. 19 Since 0.5 mL Eppendorf Protein LoBind® polypropylene tubes were unsuitable for direct measurements with the fully automated immunoassay system, CSF samples were transferred into Hatichi sample cups as recommended by the Lumipulse G manufacturer. The study utilized the same batch of reagents for each biomarker. However, measurements for these samples were conducted on different days. The methods used and biomarkers analyzed were summarized in Table 1.
Methods and biomarkers analyzed.
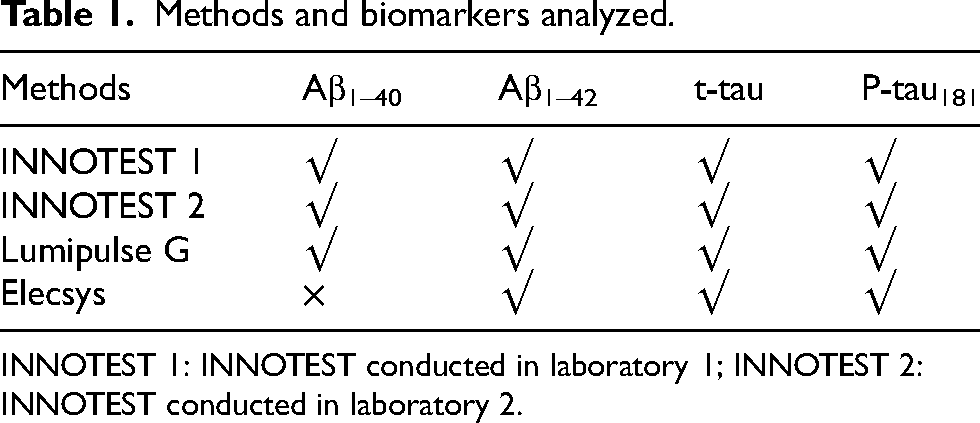
INNOTEST 1: INNOTEST conducted in laboratory 1; INNOTEST 2: INNOTEST conducted in laboratory 2.
Statistical analysis
Prior to comparative analyses, the normality of biomarker distributions was assessed using the Kolmogorov-Smirnov test. Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables (e.g., sex, APOE ε4 carrier status) were presented as proportions. Group comparisons were performed using Student's t-tests for normally distributed continuous variables and Pearson's chi-square tests for categorical variables.
Diagnostic performance was evaluated using receiver operating characteristic (ROC) curve analysis, with the optimal cutoff determined by maximizing the area under the curve (AUC). Accuracy was calculated as:
A two-tailed p-value < 0.05 was considered statistically significant. All analyses were conducted using R statistical software (version 4.2.1; R Foundation for Statistical Computing).
Results
Characteristics of study population
The study cohort comprised 309 participants, including 176 patients with clinically diagnosed AD, 114 non-AD individuals, and 19 cognitively CN. Within this population, amyloid-PET/CT imaging revealed 50 amyloid-positive (PET+) and 21 amyloid-negative (PET−) cases.
As detailed in Table 2, demographic characteristics were comparable between groups in terms of age and sex distribution. However, APOE ε4 carrier status showed significant between-group differences, with a higher prevalence observed in the AD group compared to non-AD participants (p < 0.05).
Characteristics of study population and subgroups.
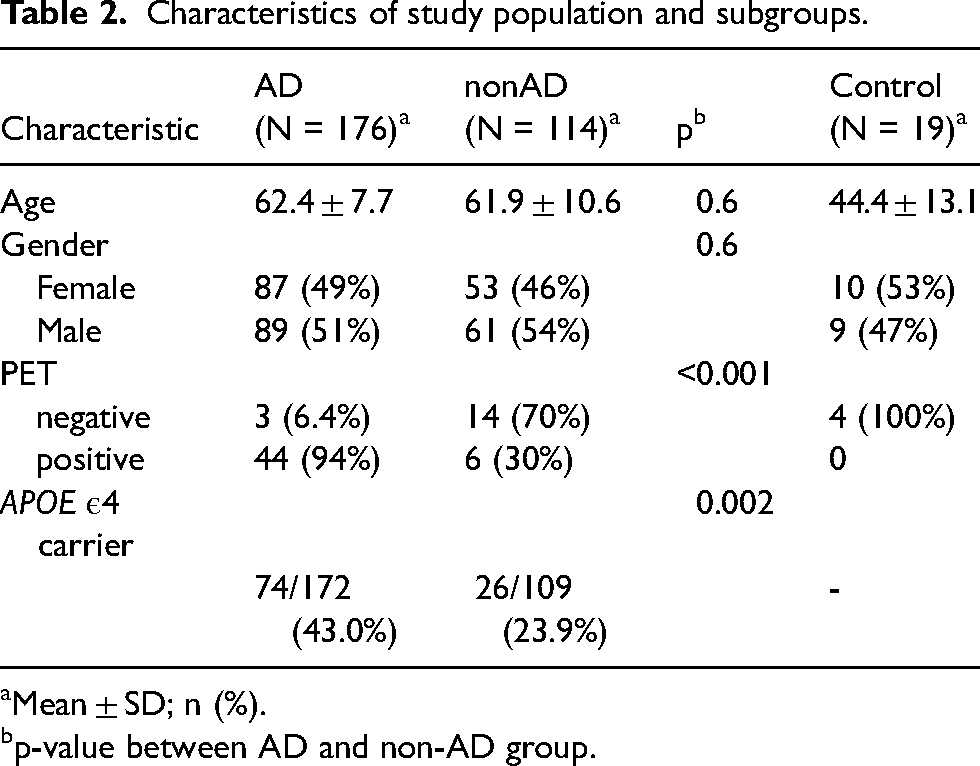
Mean ± SD; n (%).
p-value between AD and non-AD group.
Cutoffs of CSF biomarkers between clinically diagnosed AD and non-AD
We evaluated and compared the diagnostic accuracy of four CSF assay platforms (INNOTEST®1 and 2, Lumipulse® G, and Elecsys®) for discriminating between clinically diagnosed AD and non-AD cases. Optimal cutoff values were determined through receiver operating characteristic (ROC) curve analysis, with detailed results presented in Table 3.
Cutoffs of different methods in separating clinically diagnosed AD and non-AD.
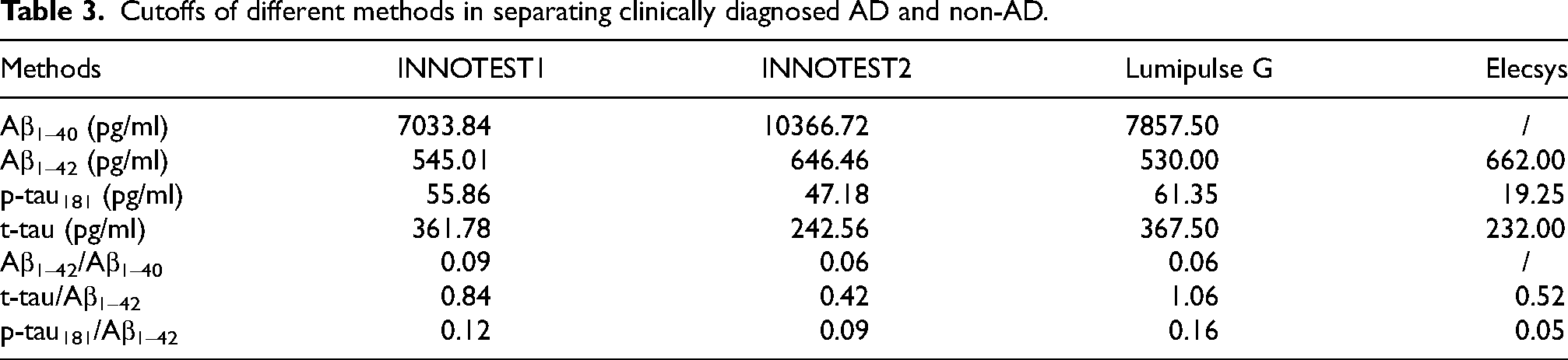
The highest accuracy when measuring Aβ1–42 was achieved by Elecsys (0.909). While the highest accuracy when measuring t-tau (0.776), p-tau181 (0.821) and the three ratios (Aβ1–42/Aβ1–400.881, t-tau/Aβ1–42 0.866 and p-tau181/Aβ1–42 0.836) was achieved by Lumipulse.
Detailed diagnostic performance metrics, including area under the curve (AUC) values accuracy measures, sensitivity and specificity, are provided in Supplemental Table 1. Corresponding ROC curves illustrating the discriminatory capacity of each assay are displayed in Figure 1.
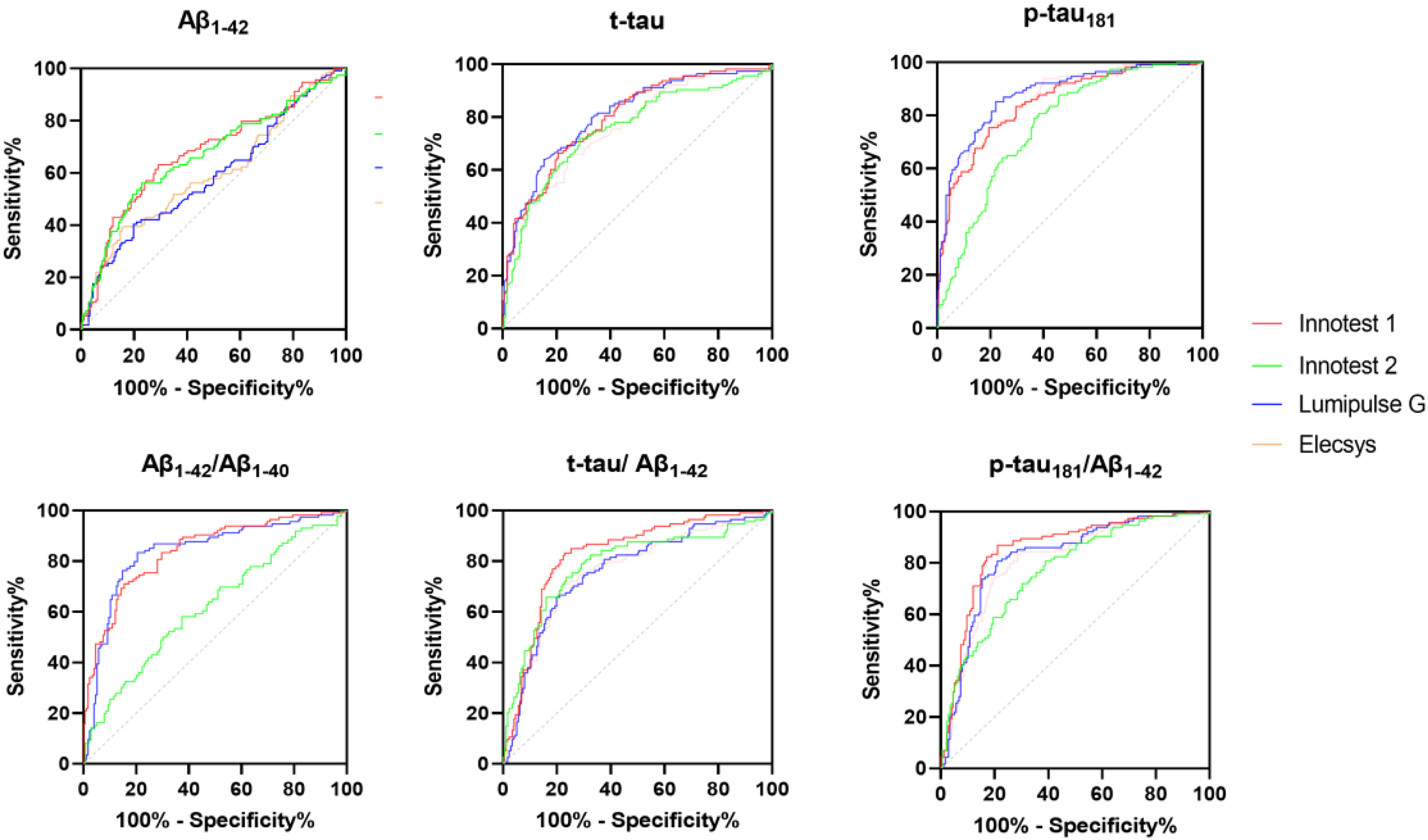
ROC curve of different methods for differentiating AD and non-AD.
To further explore the consistency between the AT(N) biomarker classification and clinical diagnosis, we generated a table comparing AT(N) profiles derived from four different platform-specific cutoffs (INNOTEST 1, INNOTEST 2, Lumipulse G, and Elecsys) across the same clinical cohort. By applying ROC-derived cutoff values for t-tau/Aβ1–42, p-tau181based on clinically diagnosed AD and non-AD, we classified each individual according to the AT(N) framework. The resulting consistency between clinical diagnosis and AT(N) biomarker classification was showed in Supplemental Table 2. This allowed us to assess whether the use of different biomarker platforms impacts AT(N) classification, and how closely these classifications align with the clinical diagnosis.
Cutoffs of CSF biomarkers between PET+ and PET−
We evaluated and compared the diagnostic accuracy of four CSF assay platforms (INNOTEST®1 and 2, Lumipulse® G, and Elecsys®) for discriminating between PET+ and PET− cases. Optimal cutoff values were determined through ROC curve analysis, with detailed results presented in Table 4.
Cutoffs of different methods in separating PET+ and PET−.
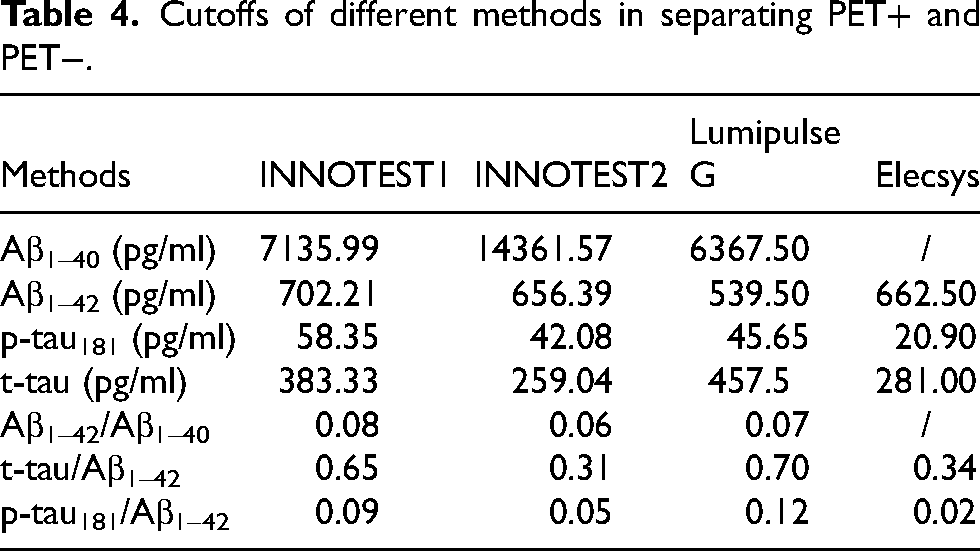
The highest accuracy when measuring Aβ1–42 (0.942) and t-tau (0.783) was achieved by INNOTEST1. The highest accuracy when measuring p-tau181 (0.873) and the three ratios (Aβ1–42/ Aβ1–400.958, t-tau/ Aβ1–420.944 and p-tau181/ Aβ1–420.944) was achieved by Lumipulse G.
Detailed diagnostic performance metrics, including AUC values, accuracy measures, sensitivity and specificity, are provided in Supplemental Table 1. Corresponding ROC curves illustrating the discriminatory capacity of each assay are displayed in Figure 2.
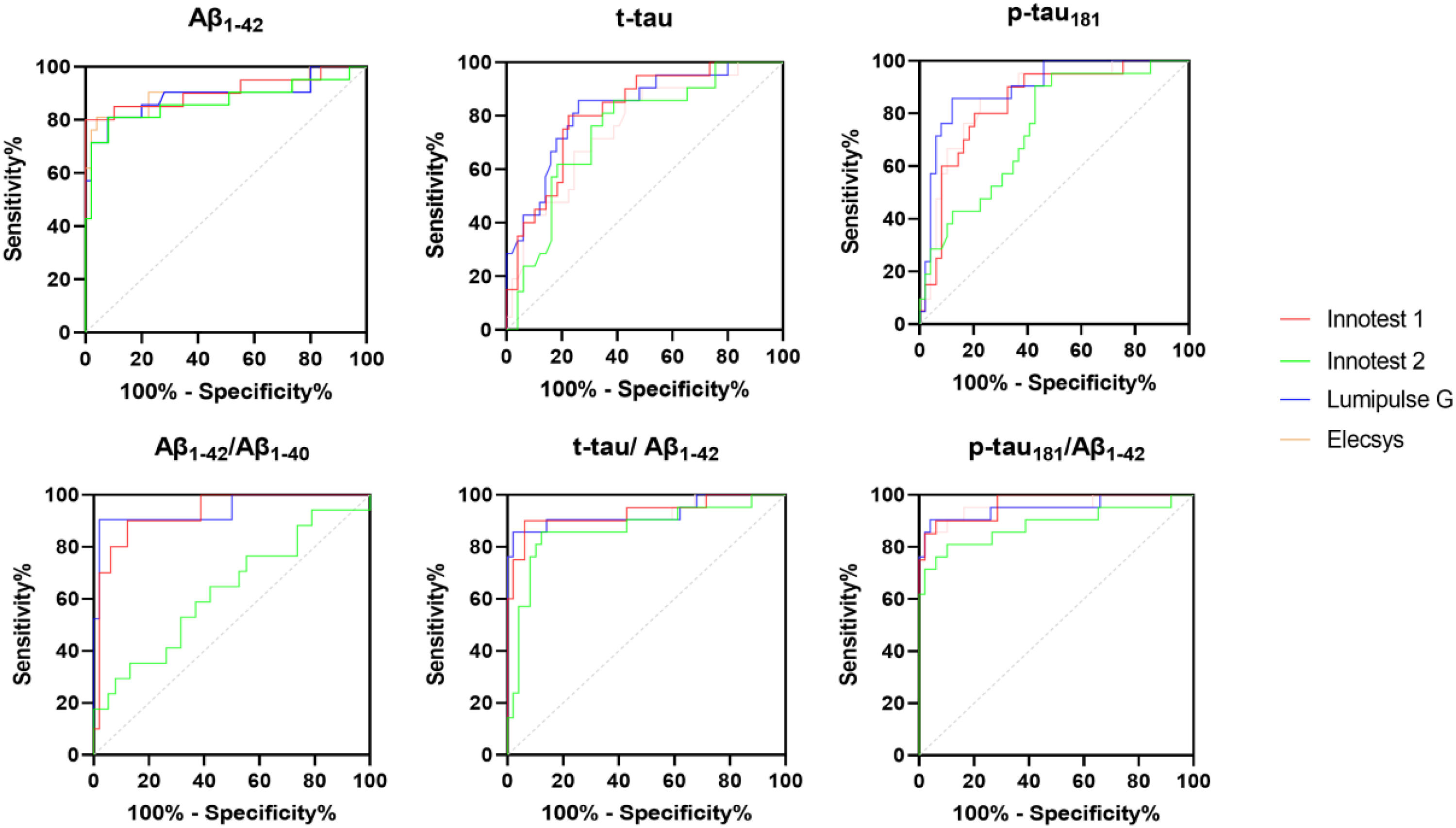
ROC curve of different methods for differentiating PET+ and PET−.
Cutoffs of CSF biomarkers between PET + and CN
We evaluated and compared the diagnostic accuracy of four CSF assay platforms (INNOTEST®1 and 2, Lumipulse® G, and Elecsys®) for discriminating between PET + and CN cases. Optimal cutoff values were determined through ROC curve analysis, with detailed results presented in Table 5.
Cutoffs of different methods in separating PET + and CN.
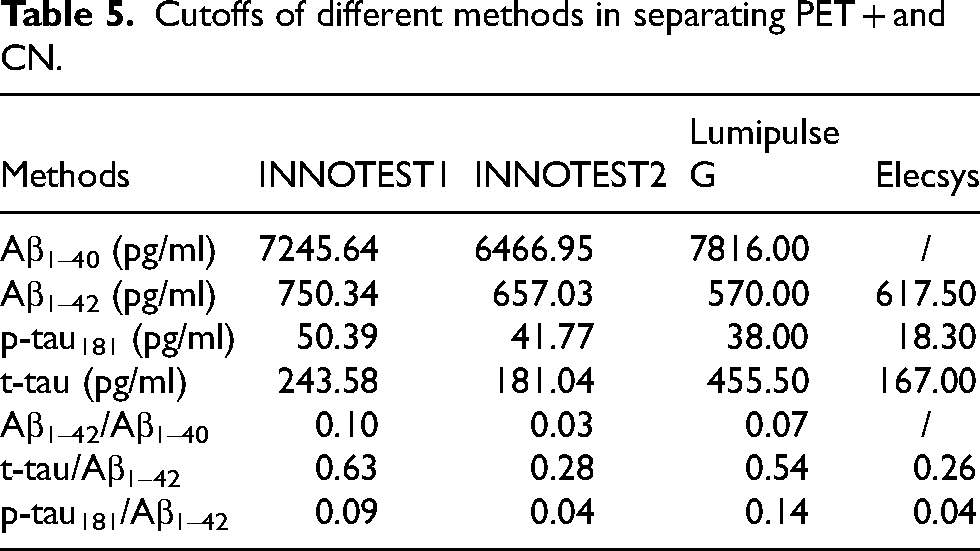
The highest accuracy when measuring Aβ1–42 (0.942) and t-tau (0.783) was achieved by INNOTEST1. The highest accuracy when measuring p-tau181(0.928) and the two ratios (Aβ1–42/Aβ1–400.986 and t-tau/Aβ1–42 0.942) was achieved by Lumipulse G. The highest accuracy when measuring p-tau181/Aβ1–42 was achieved by Elecsys (0.956).
Detailed diagnostic performance metrics, including AUC values, accuracy measures, sensitivity and specificity, are provided in Supplemental Table 1. Corresponding ROC curves illustrating the discriminatory capacity of each assay are displayed in Figure 3.
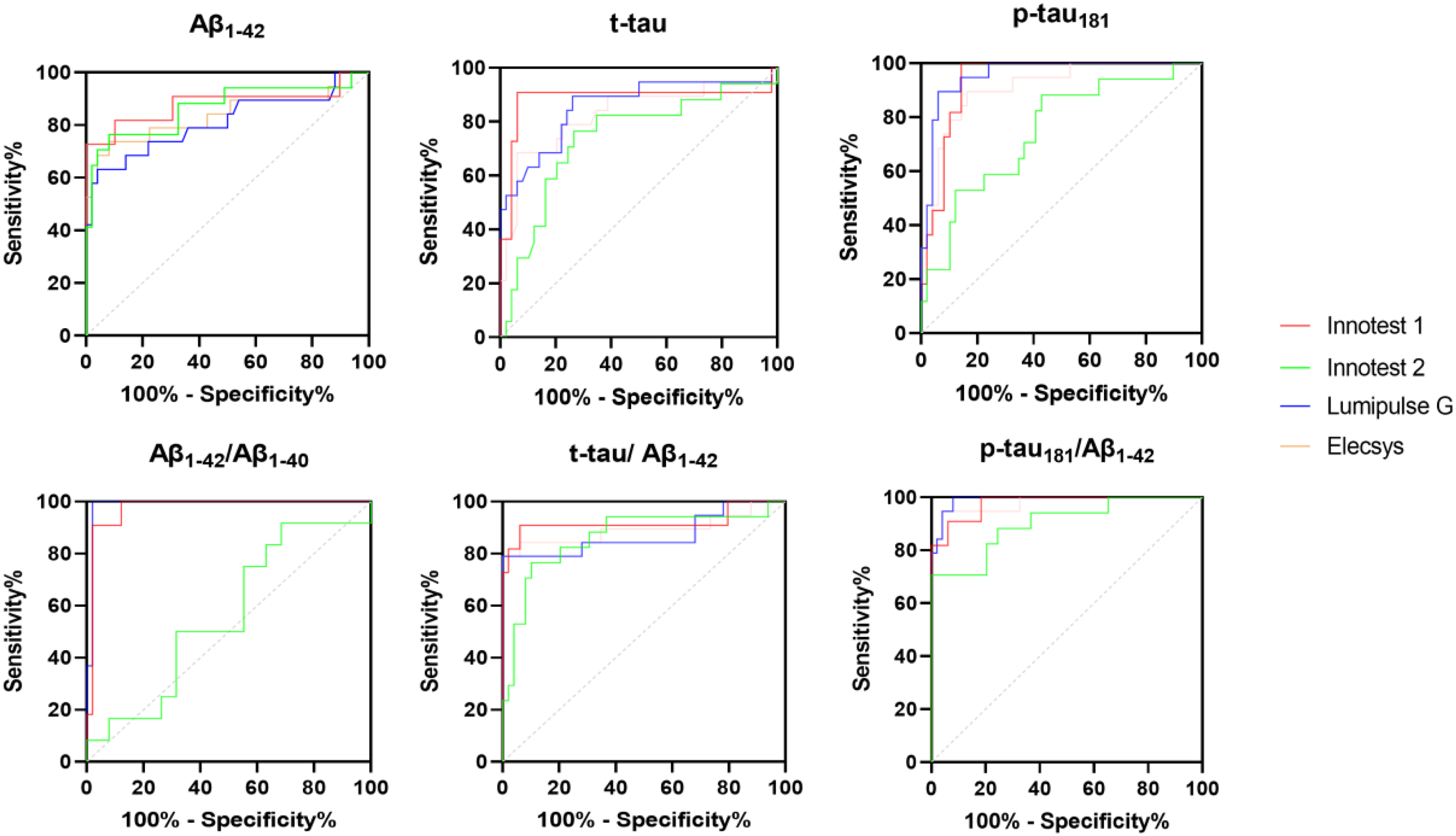
ROC curve of different methods for differentiating PET+ and CN.
Discussion
In this study, we assessed the diagnostic performance of four core AD biomarkers (Aβ1–40, Aβ1–42, t-tau, and p-tau181) and their ratios (Aβ1–42/Aβ1–40, t-tau/Aβ1–42, and p-tau181/Aβ1–42) using three immunoassays (INNOTEST, Lumipulse G, and Roche Elecsys) in a Chinese cohort. Our findings demonstrated higher accuracy in measuring most biomarkers by automated assays (Lumipulse G and Elecsys) over manual assays (INNOTEST). Notably, INNOTEST exhibited significant inter-laboratory variability (difference of accuracy between INNOTEST1 and INNOTEST2), underscoring the importance of standardized protocols and experienced personnel to ensure result accuracy. Biomarker ratios(Aβ1–42/Aβ1–40, t-tau/Aβ1–42, and p-tau181/Aβ1–42) consistently showed higher diagnostic accuracy than absolute values. However, established cutoffs were not directly comparable across different methods or clinical contexts, such as distinguishing AD from non-AD cases or cognitively normal controls. It should also be noted that the cutoff values for distinguishing amyloid PET status were derived from a subset of participants with available PET data, rather than from the entire cohort of 176 AD, 114 non-AD dementia cases, and 19 cognitively normal controls. Therefore, further validation in larger PET-confirmed cohorts is necessary to generalize these thresholds to broader clinical diagnostic populations.
The clinical utility of CSF biomarkers for AD has been extensively studied and debated over the past decades. These biomarkers have proven valuable in several key applications: enhancing diagnostic accuracy in suspected AD cases, detecting AD at its earliest stages, differentiating AD from other neurodegenerative and cerebrovascular disorders, identifying AD in mixed-pathology scenarios, and diagnosing atypical AD presentations.20–22 Moreover, CSF biomarkers demonstrate high sensitivity and specificity in classifying the AD continuum and have shown utility in predicting disease progression. 23 CSF p-tau181/Aβ1–42ratio demonstrated strong predictive value for both cognitive decline and clinical conversion in cognitively unimpaired individuals and patients with mild cognitive impairment, achieving excellent diagnostic accuracy. 7 Besides, baseline CSF levels of p-tau181 were independently associated with subsequent disease progression, as reflected by hippocampal atrophy rate in AD. 24
INNOTEST has been one of the most widely used manual immunoassays in testing CSF biomarkers. INNOTEST assays including Aβ1–40, Aβ1–42, t-tau and p-tau181 have been validated to provide accurate and precise quantification in clinical trials and long-term clinical testing.25,26 However, Multisite studies have consistently demonstrated significant inter-laboratory variability in both measured levels and established cutoffs for the three CSF biomarkers (Aβ1–42, t-tau, and p-tau181) when using the INNOTEST platform. This variability primarily stems from site-specific differences in manual CSF processing techniques. Therefore, procedures have been harmonized to optimize the accuracy of CSF biomarkers in AD and use in clinical settings. 27 We also proved inter-laboratory variability of INNOTEST performed in two different laboratories, suggesting laboratory specific levels and cutoffs were necessary in clinical interpretation. Automated immunoassays had advantages to reduce variability caused by manual operation. Lumipulse G assays were validated to have good repeatability and reproducibility and was fit for purpose in clinical laboratory practice. 28 In several researches, Lumipulse G was proved to have good clinical concordance with INNOTEST assays and well-suited for CSF clinical routine measurements.29,30 Besides, CSF biomarkers measured with the Lumipulse G showed good agreement with amyloid imaging and could predict progression of cognitive decline.31–33 Roche Elecsys was another fully automated CSF assays and was proved to have well concordance with Aβ-PET measures or clinical diagnostic and prognostic variables.34–36 Also, a study based on pathology confirmed AD demonstrated high neuropathological validity of Elecsys-derived CSF biomarkers of AD. 37
Many pair wise comparisons have been conducted internationally among different CSF biomarker assays. Faull et al. concluded that the INNO-BIA AlzBio3 (Luminex) assay offered faster laboratory turnaround times and required lower sample volumes compared to the INNOTEST assay. 38 Monge-Argilés et al. demonstrated strong correlation between ELISA and xMAP platform results, but observed differences in absolute values, highlighting the importance of clearly specifying the analytical methodology used. 39 Schipke et al. confirmed that the INNOTEST, IBL and Meso Scale Discovery (MSD) assays all provide reliable results; however, they emphasized that absolute values must be interpreted within assay-specific diagnostic frameworks due to systematic variations between platforms. 40 Also, Keshavan et al. compared the Lumipulse, INNOTEST, and MSD assays and concluded that the Lumipulse platform demonstrates comparable sensitivity and specificity to established CSF immunoassays in detecting pre-symptomatic AD pathology. 41
Our results showed ratios (Aβ1–42/Aβ1–40, t-tau/Aβ1–42, and p-tau181/Aβ1–42) had better accuracy than absolute values. Research has shown that Aβ peptide concentration can be affected by pre-analytical factors especially surface exposure, which can be mitigated using biomarker ratios.42,43 Use of polypropylene transfer plates (PTPs) prior to INNOTEST Aβ1–42 analysis can lead to significant adsorption of Aβ1–42 (up to 69%), resulting in falsely low concentrations and potentially misleading diagnostic interpretations. 44 Although low-binding (LoB) tubes can reduce Aβ loss, studies have shown that even with LoB tubes, factors such as prolonged contact between CSF and tube surfaces (including the cap), low sample volume relative to tube surface area, and transfer between tubes can still lead to significant Aβ1–42 adsorption. These pre-analytical handling variables may explain the inter-laboratory variability observed in our results, highlighting the importance of standardized CSF processing protocols in biomarker assessment.45,46 The concentration ratio of Aβ1–42 to Aβ1–40 (Aβ1–42/1–40 Ratio) had been suggested to be superior to the concentration of Aβ1–42 alone when identifying patients with AD in many cohort studies and addition of the CSF Aβ1–42/1–40 ratio in the interpretation of the CSF profile of MCI patients would enhance their predictive value for underlying AD dementia.47,48 Besides, ratios of t-tau/Aβ1–42and p-tau181/Aβ1–42both improved the capacity of discriminating between AD and non-AD as well as AD and control groups.49,50 CSF Aβ1–42/Aβ1–40 or Aβ1–42/tau ratios were also found better correlating with Aβ-PET when using different immunoassays. 51 Therefore, we suggest using ratios as CSF biomarkers in clinical practice for diagnosing AD. However, it should be noted that the Aβ1–42/Aβ1–40 ratio is not available on the Elecsys platform, and thus cannot be compared across all three immunoassay methods in this study. For the Roche Elecsys platform, we recommend the use of alternative ratios such as p-tau181/Aβ1–42 or t-tau/Aβ1–42, which also demonstrated good discriminatory performance and are supported by this platform.
A critical limitation in the clinical application of CSF biomarkers is the current lack of universally established cutoff values. 52 In an international systematic review of 40 centers involved in AD diagnosis worldwide, only 16% reported using cutoffs provided by the manufacturer, 4% used cutoffs based on the literature, and the remaining used in-house cutoffs. 53 There were several methods to define the cutoffs of CSF biomarkers. The most common method used to determine the threshold for CSF Aβ1–42 positivity was comparison with Aβ-PET. 54 Other methods included comparison between patients with AD and non-AD or normal control based on clinical criteria and/or postmortem neuropathological criteria. 55 However, most reported cutoffs were in-house cutoffs with limited extensive application.56–58
The study is not without limitations: (1) As a single-center study, our findings reflect center-specific cutoffs; future multi-center validation is warranted. (2) The absence of postmortem verification may introduce diagnostic confounding factors affecting both patient classification and cutoff determination. (3) Our analysis was limited to three common immunoassays; additional evaluation is needed as new assays and methodologies emerge for clinical use, such as mass spectrometry.
In this first comparative study of three immunoassays (INNOTEST, Lumipulse G, and Roche Elecsys) in a Chinese cohort, we demonstrated that all evaluated assays are suitable for routine CSF biomarker testing, with automated platforms exhibiting superior performance. Importantly, we established, for the first time, assay-specific cutoff values tailored to different clinical contexts in a Chinese population. To ensure result reliability, strict adherence to standardized protocols is essential, particularly for manual assays. We further recommend that all Chinese laboratories conducting AD CSF biomarker testing participate in the Alzheimer's Association quality control program.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251379084 - Supplemental material for Comparison of diagnostic accuracy of Alzheimer's disease cerebrospinal fluid core biomarkers using INNOTEST, Lumipulse G, and Elecsys assays: Insights from the PUMCH dementia cohort study
Supplemental material, sj-docx-1-alz-10.1177_13872877251379084 for Comparison of diagnostic accuracy of Alzheimer's disease cerebrospinal fluid core biomarkers using INNOTEST, Lumipulse G, and Elecsys assays: Insights from the PUMCH dementia cohort study by Chenhui Mao, Yutong Zou, Tianyi Wang, Longze Sha, Meiqi Wu, Shanshan Chu, Wei Jin, Bo Li, Yixuan Huang, Yuyue Qiu, Jialu Bao, Wenjun Wang, Yuhan Jiang, Liling Dong, Feng Feng, Li Huo, Charlotte Teunissen, Ling Qiu and Jing Gao in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors thank the study participants for their time and effort in participating in the trial.
Ethical considerations
The research protocol was conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki (1975) and its subsequent amendments. The Institutional Review Board (IRB) of Peking Union Medical College Hospital granted ethical approval for this study (Approval No. JS2810).
Consent to participate
Informed written consent was obtained from all participants and their caregivers.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (nos. 2020YFA0804500 and 2020YFA0804501), the CAMS Innovation fund for medical sciences (CIFMS) (nos. 2021-I2M-1-020 and 2020-I2M-C&T-B-010), National High Level Hospital Clinical Research Funding (nos. 2022-PUMCH-A-254).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Jing Gao is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Data availability statement
The data supporting the findings of this study are available within the article and/or its supplemental material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.