
Abstract
Dementia is a progressive neurodegenerative disorder characterized by cognitive decline that interferes with daily functioning, particularly in the elderly. As one of the leading causes of disability among older adults, dementia remains a significant public health concern. Emerging evidence suggests that certain vitamins may play a crucial role in the prevention and management of cognitive impairment. This review explores the potential impact of key micronutrients specifically water-soluble vitamins such as vitamin C and B-complex (B1, B2, B3, B5, B6, B9, B12), and fat-soluble vitamins A, D, E, and K on dementia pathogenesis and cognitive function. Vitamin B deficiencies have been associated with brain atrophy, an early indicator of cognitive decline, and supplementation has shown promise in enhancing memory and slowing brain shrinkage. Similarly, vitamin C exhibits antioxidative properties that may protect against neurodegeneration. While nutritional support, particularly through micronutrient intake, is increasingly considered a viable strategy for cognitive preservation, findings from epidemiological and clinical studies remain mixed. These inconsistencies highlight the need for further research to determine optimal dosing, efficacy, and long-term impact of vitamin supplementation in dementia prevention. A well-balanced diet rich in essential vitamins may support brain health, but individual variability suggests the importance of personalized nutritional interventions. This review underscores the potential role of vitamins in maintaining cognitive health and calls for continued investigation into their therapeutic utility in delaying or preventing dementia.
Introduction
Dementia refers to a deterioration in cognitive functions that affects everyday activities. Alzheimer's disease (AD) is one of its leading causes. 1 In medical and psychiatric terms, dementia is a chronic (and occasionally acute) impairment of mental processes resulting from brain disease, leading to altered personality, diminished situational awareness, and disruptions in memory, judgment, and reasoning.2,3 The most prevalent form is senile dementia, also known as AD. Additional causes include strokes, drug- or psychedelic-induced delirium, and rare conditions like mad cow disease. 4 Dementia involves the gradual decline of cognitive abilities while consciousness remains intact (unless influenced by specific factors like delirium. 5 Rather than being a single disease, dementia encompasses a variety of symptoms, including impaired memory, reasoning, and social skills, which hinder daily life. 6 While memory loss is a common feature, it does not alone confirm dementia, as it can stem from various factors. 7 AD remains the primary cause of progressive dementia in older adults. 8 Although the displays of this condition vary widely, dementia primarily affects key cognitive functions, including memory, communication and language skills, concentration and attention span, reasoning and judgment, and visual perception. 9 Individuals with dementia often fight with short-term memory, leading to difficulties in tasks like locating personal items, managing finances, organizing, cooking, keeping track of appointments, or navigating familiar routes. Most forms of dementia are progressive, 10 meaning symptoms develop slowly and intensify over time. Depending on the underlying causes, dementia symptoms can vary. Memory loss, difficulty speaking or recalling words, disorientation, lack of concentration, anxiety, paranoia, melancholy, inappropriate behavior, delirium and impatience are some typical signs, though.11–13 The deterioration of brain cells hinders their communication, and when this normal interaction is disrupted, it impacts cognition, behavior, and emotional regulation. 14 AD, vascular dementia, and temporal lobe cell damage are examples of definitive forms of dementia that deteriorate over time and are irreversible.15,16 Among individuals aged 65 and older, AD is the leading cause of dementia. 17 This condition involves the accumulation of amyloid-β (Aβ) protein clusters, known as plaques, and may also be influenced by genetic factors. 18 Vascular dementia, another common type, results from impaired blood flow to the brain due to injured blood vessels, often caused by strokes or other circulatory issues.19,20 Micronutrients such as vitamins C, B-complex (including B6, B9, and B12) and fat-soluble vitamins A, D, E, and K play a key role in cognitive health.21–23 They may impact the risk and progression of dementia. 23 Vitamin C and E act as antioxidants to decrease oxidative stress connected to neurodegeneration, while B vitamins (mainly B12 and folate) help lessen homocysteine levels, a known risk factor for dementia. 24 Vitamin D deficiency has been linked with an increased risk of AD, possibly due to its neuroprotective and anti-inflammatory effects. 25 Vitamins A and K contribute to brain health by supportive neuronal function and reducing amyloid plaque formation, though additional research is needed. 26 Overall, adequate intake of these micronutrients through diet or supplementation may help mitigate dementia risk, though clinical evidence remains mixed and context-dependent. 27
Vitamins are categorized into two key groups: water-soluble vitamins (like most B vitamins and vitamin C), fat-soluble vitamins (such as vitamins A, D, E and K, which do not dissolve in water); The human body acquires vitamins primarily through dietary intake, as these vital micronutrients are not synthesized in sufficient quantities to meet physiological needs.28,29 For adults, vitamins are obtained from a varied diet including fruits, vegetables, whole grains, dairy, and lean proteins.30–33 Vitamins and minerals play crucial roles in maintaining optimal brain function in neurotransmitter synthesis, neuronal signaling, synaptic plasticity, and protection against oxidative stress.34–36 This is particularly crucial in early childhood, when the brain is rapidly developing, and in later life, when it undergoes significant structural and functional changes. 37 Efficient nerve signal transmission is essential, and vitamins significantly influence brain function and neural communication. 38 The speed of these signals largely depends on myelin function, which is supported by Vitamins. The possible neuroprotective effects of water-soluble vitamins, especially vitamin C and the B-complex group (which includes B1, B2, B3, B5, B6, B9, and B12), in dementia have been thoroughly investigated.39–41 By neutralizing free radicals and lowering neuroinflammation, vitamin C, a strong antioxidant, may help prevent oxidative stress, a major cause of dementia, and thus slow down cognitive deterioration.42,43 The metabolism of homocysteine depends on B vitamins, particularly B12, and folate; high homocysteine levels are associated with a higher risk of vascular dementia and AD.44,45 Although the results are still mixed, some research indicates that consuming enough B vitamins may maintain brain capacity and enhance cognitive function.46,47 Although deficits in these vitamins are linked to cognitive impairment, more longitudinal and mechanistic study is needed to prove causation and determine their therapeutic usefulness in managing or preventing dementia.48,49 Fat-soluble vitamins (A, D, E, and K) may affect dementia risk through diverse pathways, including neuroprotection, vascular health, and anti-inflammatory effects.50–52 Vitamin D, with its neurosteroid properties, is hypothesized to decrease Aβ growth and tau phosphorylation, while its deficiency is related to higher dementia incidence.53–55 Vitamin E's antioxidant properties may defend neuronal membranes from oxidative damage, with some indications suggesting slower progression in mild cognitive loss.42,56,57 Vitamin K is implicated in sphingolipid metabolism and is critical for brain cell integrity, and observational studies associate higher vitamin K intake with improved cognition.58–61 Vitamin A, though less studied, may support synaptic plasticity.62,63 However, excessive intake of fat-soluble vitamins poses toxicity risks, and clinical trials have yielded mixed consequences, highlighting the need for precise dosing and further study into their roles in dementia pathophysiology.64,65
Methods
In this systematic review of the role of vitamins in the prevention of dementia and the maintenance of cognitive function, a systematic search and analysis of literature was conducted. A comprehensive literature search was performed in PubMed, Scopus, and Web of Science, including articles dated from 2000 to 2025. The search involved using vitamins in combination with dementia, AD, and cognitive decline as keywords. Only studies that investigated the impact of vitamins on cognitive decline or dementia were included (i.e., observational studies, clinical trials, meta-analyses). The exclusion criteria were studies not involving vitamins and dementia, animal models irrelevant to human health, and articles without obvious description of cognitive impairment. Study design, sample size, the specific type of vitamin and dosage, cognitive outcomes, and results were extracted from the included studies and tabulated. This was a literature review, so a direct ethical consent was not required; however, all the studies included in this review respected ethical considerations. The results were systematically reported for each vitamin based on the existing literature. The review was concluded with recommendations for future research, particularly emphasizing the need for clinical trials to determine the optimal dosages and combinations of vitamins in dementia prevention. This approach ensured a comprehensive examination of the current evidence on the role of vitamins in cognitive health.
Impact of vitamin c on dementia
Vitamin C, a potent antioxidant, is crucial for lowering oxidative stress, a primary cause of dementia, including AD.66,67 Oxidative damage causes neuronal degeneration, and vitamin C helps fight off free radicals, which reduces inflammation and the formation of Aβ plaques, two traits of AD.67,68 Research has exhibited that higher levels of vitamin C in plasma are related to better cognitive function and a decreased chance of cognitive decline. 69 Furthermore, vitamin C stimulates the synthesis of neurotransmitters, including dopamine and norepinephrine, which are essential for memory and cognitive function. 70 Vitamins E and C are commonly used to prevent dementia because of their antioxidant properties.71,72 A study examined vitamin C's role in preventing neurodegeneration and assessed its ability to prevent dementia. 66 Supplementing with vitamins E and C has been related to better cognitive function in later life. 73 Because of its antioxidant qualities, vitamin C may help prevent dementia. 74 Vitamin C levels were found to be low in dementia patients. 75 Several beneficial effects on neurodegeneration over time, particularly in connection to AD, have been shown to be supported by L-ascorbic acid. 76 There is growing evidence that L-ascorbic acid may help improve certain aspects linked with the pathophysiology of AD. 77 Definitely, the scavenging action against reactive oxygen species, the control of neuroinflammation, the reduction of Aβ fibrillation, and the chelation of copper, iron, and zinc are the primary processes linked to AA neuroprotection. 78 High dosages of ascorbic acid supplementation reduced the impact of amyloid plaque in a mouse model of AD with a 5 familial AD mutation (5XFAD).79,80 To better understand the pathogenetic importance of AA in an AD mouse model, 5XFAD mice were mated with gulono-gamma-lactone oxidase (Gulo) knockout mice (KO-Tg mice).67,81 Increased AA supplementation in KO-Tg mice improved mitochondrial modification and BBB disruption while significantly lowering the burden of amyloid plaques. 79 The APPSWE/PSEN1deltaE9 animal model of AD was created by crossing APP/PSEN1(+) bigenic mice with SVCT2(+/−) heterozygous knockout mice, which also yielded interesting results. 80 By 14 months of age, compared to wild-type controls, there was a decrease in total glutathione and an increase in oxidative stress (F2-isoprostanes, protein carbonyls, and malondialdehyde). 80 Additionally, higher amounts of soluble and insoluble Aβ1–42, a higher Aβ1–42/1–40 ratio, and increased hippocampal and cortical Aβ plaque formations were seen in comparison to APP/PSEN1(+) mice with normal AA brains.80,82 AA deficiency accelerates the accumulation of amyloid, particularly in the early stages of the disease, and these effects are likely influenced by oxidative stress pathways.83–85 Huang et al. demonstrated showed ascorbate preloading dramatically lowered basal rates of endogenous Aβ production and stopped SH-SY5Y cells from dying through apoptosis. 86 Using an in vitro model, Cheng et al. showed that a lack of AA could lead to a higher production of harmful Aβ oligomers. In the absence of AA, neurotoxic fibrillogenesis is more strongly induced, and the Aβ domain briefly comes into touch. Inhibited is the little NO-catalyzed release of oligosaccharides that include anhydromannose (anMan). 87 Vitamin C, which is known as a powerful antioxidant, could have a protective role in dementia through its anti-oxidative and anti-inflammatory properties that are thought to be involved in the pathogenesis of cognitive impairment.88,89 Higher level of vitamin C intake found to be related to a lower risk of AD and other dementias, possibly contributing to its ability to quench free radicals and to maintain the integrity of the nerve cells.67,90 Clinical trials have produced conflicting findings despite observational research suggesting that vitamin C may have a preventive effect against dementia.90,91 Supplementing with vitamin C, especially when combined with vitamin E, may reduce cognitive deterioration in early-stage dementia, according to some research. 92 Other studies, however, found no appreciable benefit, suggesting that the effects of vitamin C may depend on the disease's progression or the beginning nutritional status. 93 Maintaining sufficient vitamin C levels by diet or supplementation is still a potential way to support brain function in older populations despite discrepancies.48,90
Impact of vitamin b on dementia
The water-soluble vitamin group known as B vitamins is crucial to the process of cellular metabolism. 94 Group B vitamins increase the body's metabolism and encourage cell division and growth because they frequently participate in the cycle of cell metabolism.. 95 Vitamin B supplements significantly reduce the incidence of dementia in older persons without dementia, according to a systematic review and meta-analysis. 96 Aside from proteins, minerals, fats, and carbs, vitamins are essential dietary components for life.97,98 The methylation cycle, the synthesis of monoamine oxidase, DNA, RNA, protein, and phospholipids, as well as cell repair, are all impacted by the vitamin B complex.99,100 As part of the body's detoxification process, the methylation cycle maintains DNA, provides energy, controls mood and behavior, and ensures a healthy immunological and inflammatory balance. 101 Only a byproduct of the methylation cycle, homocysteine serves as a sensitive indicator of vitamin B deficiency. 102 Vitamin B3 (niacin) is essential for energy metabolism, DNA repair, and cellular signaling, with deficiency leading to pellagra, characterized by dermatitis, diarrhea, and dementia41,103 In actuality, low levels of vitamins B1, B2, B6, B9, and B12 predict high homocysteine levels and cognitive decline. 104
Vitamin B1
Thiamine, a water-soluble vitamin B, is vital to the healthy process of the neurological system and helps cells convert carbohydrates into energy.105,106 The connection between thiamine deficiency and neurological issues, such as cognitive deficiencies, was among the first instances of nutritional insufficiency.107,108 In actuality, thiamine deficiency is very common in older persons, especially those who are hospitalized or institutionalized, and is linked to greater rates of AD and depression. 109 Given its benefits for neurological conditions like encephalopathy and cognitive impairments, diet, and dementia are related. 110 In rats, repeated thiamine shortage results in brain damage and diminished cognition. 111 Although there is promising evidence that thiamine deficiency is associated with the risk of cognitive decline, further research is needed to determine whether thiamine supplementation will be beneficial as a preventative treatment for cognitive decline110,112 . Specifically, it is unclear if a high dietary thiamine intake improves mental performance, according to recent cross-sectional and case-control studies. 113 In a study examining the connection between vitamin B1 and dementia, Zhu et al. examined 47 healthy controls and 91 dementia patients. 114 They discovered that the vitamin B1 levels of dementia patients were lower than those of the healthy control group. According to their findings, the B1 vitamin is a dementia marker. 114 Thiamine was evaluated as a protective factor for preventing dementia progression in people with alcohol use disorder, and vitamin B1 was recommended in the treatment plan and health policies to prevent dementia development and/or advancement. 115 Dementia may, therefore, be related to vitamin B1 insufficiency.114,116
Vitamin B2
Riboflavin, or vitamin B2, is the precursor of flavin adenine dinucleotide (FAD). In the intermediate metabolism of lipids, amino acids, and carbohydrates, riboflavin is essential.117,118 Skin and epithelium are examples of tissues with high cell turnover where riboflavin deficiency first manifests because it can be involved in both one- and two-electron transfer pathways.117,119 The lips, skin, eyes, and digestive system membranes become inflamed as a result. In a meta-analysis systemic review study on the micronutrient consumption of older adults, deficiencies in riboflavin and thiamin were linked to poor cognitive results. 120 Interestingly, riboflavin and vitamin D metabolism are related, and a deficiency in riboflavin and an imbalance in FAD result in a discernible alteration in the skeleton and central nervous system's structure. 121 Methylenetetrahydrofolate reductase (MTHFR) has FAD as a cofactor. As a methyl donor, MTHFR facilitates the synthesis of 5-methylenetetrahydrofolate, which aids in the remethylation of homocysteine.122,123 Folate and riboflavin work together to help reduce plasma homocysteine levels. 124 Indeed, in a group of 126 healthy people who took folate supplements, it was seen that riboflavin and folate worked together to lower plasma homocysteine levels, most likely via boosting MTHFR's catalytic activity. 124 Moreover, patients with the mutation MTHFR 677T allele, a mutant form of the MTHFR gene that hinders the conversion of dietary folate into the active form, have higher homocysteine levels because of riboflavin deficiency regardless of folate status.
Homocysteine was unaffected by normal or elevated vitamin B12 (cobalamin) levels, highlighting the importance of preserving equilibrium in total vitamin B status. 125 Additionally, the Halstead-Reitan categories test, a nonverbal assessment of abstract thinking skills, revealed that 260 adults over 60 who consumed less riboflavin in their diet had worse cognitive outcomes. 126
Vitamin B3
Vitamin B3, also known as niacin, has been studied for its potential impact on dementia in adults, particularly due to its role in brain health and cellular metabolism.41,127 Studies indicate that maintaining sufficient levels of niacin may help alleviate oxidative stress and inflammation, both of which are significant contributors to neurodegenerative diseases such as AD.127,128 Higher total niacin intake was associated with a reduced risk of AD and age-related cognitive decline. 129 Moreover, niacin is used for the synthesis of nicotinamide adenine dinucleotide (NAD) coenzyme that plays a crucial role in mitochondrial function; also there is possible use in explaining the slow rate of cognitive decline in dementia patient.127,130 But despite some supporting evidence for the neuroprotective action by niacin, the results have been conflicting.127,131 While niacin supplementation did improve cognitive function in some instances, flushing and liver toxicity are potential problems for those consuming too much.129,132 In addition, results from clinical trials so far still do not provide conclusive evidence that niacin prevents dementia, and therefore they call for further research. 95 Nonetheless, ensuring have enough niacin through a healthy diet including foods such as fish, nuts and whole grains could be a reasonable strategy for preserving brain health in older adults.133,134
Vitamin B5
Pantothenic acid (vitamin B5) is an important water-soluble vitamin, which is required for the body to function, and is necessary for numerous biological activities, such as energy metabolism and neurotransmitter synthesis.40,135 It is increasingly believed that vitamin B5 could have potential effects on cognitive health, and also reduce risk of dementia. 136 Research has also shown that optimal vitamin B5 enables the body to manufacture acetylcholine, a neurotransmitter involved in both memory and learning that is deficient in the brains of those suffering with AD and other forms of dementia.136,137 In addition, its contribution to energy metabolism might be hoped to preserve neuronal integrity and activity and thereby retard neurodegenerative processes.39,138 While there is limited direct scientific proof that B5 supplementation can prevent dementia, its role in brain health overall attests to the fact that it is an important part of a diet.136,139 Studying of such diseases of the nervous system demonstrates the necessity for investigation of the prospect of salvaging the memory loss or its prophylaxis by means, among other things, of micronutrients like vitamin B5.40,140 Precision medicine techniques can also demonstrate personalized vitamin B5 responses and offer a potential direction for personalized interventions in dementia care.141–143
Vitamin B6
Pyridoxine, pyridoxal, and pyridoxamine are the three chemically separate components that makeup vitamin B6, which is essential for controlling brain function and for homocysteine re-methylation.144,145 It has an impact on the neurotransmitters that control depression, anxiety, and pain perception. 146 Its shortage has been linked to seizures, migraines, AD, cognitive decline, and other forms of dementia, in addition to increasing homocysteine levels.147,148 Pyridoxine levels, depression, and cognitive function were clearly correlated in 140 people assessed using the major depression diagnostic scale. 149 Supplementing with vitamin B6 improves mood, cognitive function, long-term memory, and psychotic symptoms in schizophrenia while lowering blood homocysteine levels.150,151 Similarly, high doses of vitamins B6, B9, and B12 reduced up to seven times the amount of cerebral atrophy in the grey matter of the brain (important areas linked to AD and dementia) in older people with a higher risk of dementia (mild cognitive impairment according to the Petersen scale), especially in those with elevated homocysteine levels, slowing cognitive decline. 152 However, vitamin B6, B9, and B12 supplements do not affect atherosclerotic lesions in individuals with hyperhomocysteinemia. 153 Despite the fact that they lower homocysteine levels. It's interesting to note that while low serum pyridoxine levels are associated with poorer motor skills, pyridoxine supplementation does not enhance learning or cognitive outcomes in animal studies. 151
Vitamin B9
Folate, also known as vitamin B9, is important for several biological processes and is required for DNA synthesis, repair, and methylation.154,155 Foods naturally contain folate; however, folic acid is a synthetic, oxidized version of folate that was chemically synthesized in 1943 and is frequently used for dietary fortification (it was made necessary in 1998). There is worry that folic acid may have detrimental consequences on the incidence of colon cancer, even though it is essential for lowering neural tube abnormalities and homocysteine serum levels. 156 Similarly, enriched flour leads to an imbalance and adversely impacts methylation reactions due to its elevated folic acid levels relative to typical natural folate levels. 157 On the other hand, low folate levels are positively correlated with cognitive deterioration.158,159 A study of 166 people with AD or dementia found that folate levels were consistently and significantly higher in the control group than in patients who already had a cognitive illness. This implies that older people using folate supplements may be essential for preventing prevalent types of dementia. 160
Additionally, folic acid consumption, along with pyridoxine and vitamin B12 supplementation, showed reduced rates of brain atrophy in those over 70 with mild cognitive impairment. 161 It enhanced global cognition, verbal delayed memory, and the clinical dementia diagnostic scale in patients with higher serum omega-3 fatty acid levels. 162 This highlights the importance of including both B vitamins and omega-3 fatty acids in the diet for the prevention of cognitive decline, even though a clinical trial involving these nutrients is required to determine whether the combination can slow the progression from mild cognitive impairment to AD.162,163 It was recently revealed that a nutraceutical formulation containing folate and vitamin B12, among other substances, significantly improved the cognitive function of 24 AD patients as well as their behavioral and psychological symptoms of dementia. 164 Similarly, in the 4166-person HAPIEE (Health, Alcohol and Psychosocial Factors in Eastern Europe) study, performance (verbal fluency, immediate memory) was favorably connected with folate and vitamin B12. 165
Furthermore, among 7030 postmenopausal women who were observed for more than five years and did not have memory cognitive impairment or likely dementia, those whose folate consumption was less than the daily recommended allowance were linked to a higher risk of probable dementia and mild cognitive impairment. 166 On the other hand, a two-year investigation of vitamin B12 and folic acid supplementation in 2919 adults over 65 with elevated homocysteine levels revealed no positive effects on performance across four cognitive domains, but there was a little improvement in global cognition.167,168 An elevated risk of cognitive decline was found to be substantially correlated with low vitamin B12 status. Additionally, it was said that there is no connection between vitamin B12 and dementia prevention. 44 The significance of vitamin B12 in dementia has been the subject of conflicting research, making it difficult to draw firm conclusions.168,169
Vitamin B12
According to a systematic review and meta-analysis, vitamin B12 may help prevent dementia, and Clarke (2008) claims that vitamin B12 is in charge of preventing cognitive decline. 96 Changes in homocysteine, vitamin B12, and folate are strongly linked to dementia. 170 A study that evaluated the relationship between plasma vitamin B12 levels and dementia risk found no link between B12 levels and dementia progression. 171 An elevated risk of cognitive decline was found to be substantially correlated with low vitamin B12 status. 168 Cobalamin, often known as vitamin B12, is crucial for the brain and neurological system to function normally.157,172 It contributes to myelin synthesis, the normal physiology of the nervous system, and the cellular metabolism of proteins, lipids, and carbohydrates. 172 A lack of vitamin B12 causes severe symptoms of depression, mania, psychosis, suicidal thoughts and actions, and cognitive deterioration.173,174 Low cobalamin levels increase the risk of cognitive decline, dementia, and AD and are linked to a five-fold acceleration of brain atrophy.168,175 Actually, elevated vitamin B12 levels offer protection, preventing cognitive impairment and brain atrophy linked to AD. 176 Vitamin B12 methylation mechanisms affect homocysteine levels, and vitamin B12 deficiency is one of the most common causes of hyperhomocysteinemia, which has been associated with a higher risk of dementia, particularly AD.177,178 The incapacity of the gastric system to absorb B12 is the most frequent cause of B12 insufficiency in older adults. 179 Research has shown that there is a significant relationship between vitamin B12 sufficiency and brain growth in individuals between the ages of 61 and 87. 176 There is a correlation between high homocysteine concentrations and the onset of dementia, according to a literature search of all published data from 2012 to 2019.180,181 Eleven observational studies and seven systematic reviews on the connection between vitamin B12, homocysteine levels, and cognitive decline were found using this search (poor quality evidence).182,183 Low-to-moderate quality data suggests that vitamin B12 (and folate) supplementation may slow the rate of brain atrophy, which is a prelude to dementia and AD. 182 Folate and vitamin B12 are essential to the function of the brain, particularly in the elderly, and deficiencies have been associated with impaired cognitive performance and higher risk of dementia.168,184–186 Vitamin B12 is important for neuronal health and myelin formation, while folate participates in the metabolism of homocysteine; high levels of homocysteine have been linked to neurodegeneration. 187 A number of studies indicate that an adequate status of folate and, but there are inconsistent findings with some randomized controlled trials reporting no beneficial effect on preventing dementia by supplementation.188,189 Deficiencies especially in elderly individuals whose diet is poor or who have malabsorption, continues to be of great interest in relation to neurological health. 190 The water-soluble vitamins B- complex play a key role on brain, deficiencies cause neurodegenerative disease (Figure 1).

The graphical illustration compares healthy and neurodegenerative brains lacking vitamin C and B complexes, resulting in neuroinflammation, tau phosphorylation, cognitive and synaptic dysfunction.
Impact of vitamin A on dementia
Research has been conducted on the potential role of vitamin A, a fat-soluble compound vital for immune function, cellular communication, and vision, in promoting cognitive health and preventing dementia.48,191 Research shows that vitamin A and its active metabolite, retinoic acid, greatly influence neurogenesis, synaptic plasticity, and memory formation. 192 Because oxidative stress and Aβ buildup are two vital clinical characteristics of AD, vitamin A deficiency has been linked to cognitive deficits. 193 Research on animals indicates that a deficiency in vitamin A exacerbates memory impairments, whereas supplementation may assist in decreasing neurodegeneration. 194 Nevertheless, hazards are associated with both inadequate and excessive intake of vitamin A, rendering the issue complex. According to specific epidemiological studies, moderate vitamin A consumption is associated with improved cognitive function; however, excessive intake may lead to toxicity and adverse neurological consequences. 195 Optimal serum retinol levels were related to a lower risk of cognitive decline, according to a long-term study by ref. 196 Nevertheless, excessive supplementation did not yield any further benefits. These observations suggest a reciprocal relationship in which neuroprotection depends on maintaining equilibrium. Further research is required to elucidate the impact of vitamin A on the risk and development of dementia. 197 Results from clinical trials examining vitamin A supplementation in older adults have been inconsistent, highlighting the need for personalized strategies tailored to each person's nutritional status.198–200 Maintaining appropriate yet not excessive levels of vitamin A could represent a viable strategy for preventing dementia, warranting further investigation due to its involvement in regulating brain homeostasis.197,201
Impact of vitamin D on dementia
According to the World Health Organization, 202 A growing public health problem is AD and associated neurodegenerative dementia illnesses. Older adults are being advised to adopt preventive steps against dementia because the current treatments only have a minimally helpful effect on these disorders. It is recommended that older persons maintain healthy lives and participate in regular, long-term exercise to reduce their risk of acquiring dementia, despite the fact that AD is a complicated condition with unknown underlying causes. 203 However, these recommendations require people to change long-standing, unhealthy habits, which some people can do, but many cannot do so over time. There have also been suggestions for dietary supplements.204,205 Vitamin D deficiency has been connected to dementia risk in numerous recent epidemiological studies. Based on observational study results,206,207 Some have concluded that a vitamin D deficiency causes AD, and some have even suggested that vitamin D supplements may offer neuroprotection against dementia.54,208 After all, supplemental vitamin D has been shown to prevent rickets, which have already been connected to vitamin D and/or calcium deficiencies in newborns and children. 209 Studies on adults have found that taking vitamin D does not improve overall health, unlike the benefits seen in children's bone growth. 210 Some people continue to believe that a safe, optimal dosage of vitamin D (1000–2000 IU) can be taken daily in order to achieve a suitable serum vitamin D level without suffering any significant side effects. 211 One may claim that the target demographic may have a connection between dementia and vitamin D levels. A study on elderly African American women found no significant correlation between vitamin D levels and dementia. 212 However, studies carried out in Asian countries have shown that vitamin D can be a helpful preventative measure for dementia. 213 Depending on the patient's age and geographic location, vitamin D appears to play a beneficial function in dementia prevention.
Impact of vitamin E on dementia
Vitamin E is a class of eight naturally occurring, fat-soluble chemical derivatives of tocopherol and tocotrienol.214,215 It is found naturally in many food items, including nuts and seeds like sunflower and almond seeds, as well as vegetable oils and fats.216,217 Alpha-tocopherol, the only form of vitamin E used in AD clinical trials, is the most studied ingredient.218,219 The Food and Nutrition Board (FNB) of the Institute of Medicine of the National Academies (US) recommends that adults over 14 should take 22.4 IU (15 mg) of alpha-tocopherol daily (National Academy of Sciences 2000). The structure of vitamin E affects a number of its biological activities.220,221 Its antioxidant capabilities allow it to scavenge free radicals. 222
High quantities of vitamin E (over 3000 IU/day) are considered harmful and have been involved with a variety of symptoms, including exhaustion, stomach cramps, and diarrhea.223,224 Furthermore, a growing amount of evidence suggests that vitamin E supplementation may have negative effects, even at lower concentrations. 225 Vitamin E, for example, can increase the risk of bleeding and exacerbate the effects of aspirin. 226 Because of its antioxidant qualities, which may reduce oxidative stress and prevent cognitive decline, vitamin E shows promise as a helpful supplement in the treatment of dementia, particularly AD.227,228 Although its efficacy varies based on dosage and personal health considerations, numerous studies indicate that vitamin E can aid people with mild to moderate dementia delay functional deterioration.229,230 However, while several research supports its neuroprotective effects, other studies show incomplete or no significant impact, importance a need for more research to control optimal usage and long-term benefits. Despite mixed evidence, vitamin E remains a hopeful area of study in dementia prevention and therapy, especially when combined with other medications.218,231 Patients and caregivers should consult healthcare professionals before supplementation, as high doses may pose health risks. Future studies should focus on standardized protocols, larger sample sizes, and longer follow-ups to clarify vitamin E's role in dementia care. Until then, maintaining a balanced diet rich in antioxidants, along with other indication-based interventions, remains the best approach for supporting cognitive health.
Impact of vitamin K on dementia
Emerging evidence suggests that vitamin K may play a significant role in brain health and in the prevention of dementia.59,60 Vitamin K, mainly in its K2 form (menaquinone), helps activate proteins that regulate calcium metabolism, which is crucial for preventing vascular calcification and maintaining brain blood flow.232,233 Because of its potential to cause oxidative stress and neurodegeneration, vitamin K deficiency has been linked in studies to cognitive impairment. 60 Additionally, vitamin K-dependent proteins like Additionally, vitamin K-dependent proteins such as Gas6 are involved in neuroprotection and inflammation regulation, which are key factors in the progression of dementia. factors in the progression of dementia.234,235 Vitamin K has also been linked to preventing neuronal damage caused by Aβ plaques, a hallmark of AD. 235 Research shows that vitamin K can reduce oxidative stress in brain cells and boost cognitive function by supporting sphingolipid metabolism, which is vital for maintaining neuronal membrane integrity. 236 Animal studies indicate that vitamin K supplementation enhances memory and reduces Aβ accumulation, pointing to a possible therapeutic role in preventing dementia.237,238 However, human clinical trials are still necessary to validate these findings. Dietary sources of vitamin K, such as leafy greens (rich in K1) and fermented foods (containing K2), may support long-term brain health. A longitudinal study found that higher dietary intake of vitamin K was associated with better cognitive performance in older adults.61,239 Given that vitamin K deficiency is common in aging populations, enhancing intake through diet or supplementation could be a promising strategy to alleviate dementia risk.240,241 However, consuming too much vitamin K might cause problems with blood thinners; therefore, clinical circumstances need to be carefully considered.242,243 In conclusion, vitamin K appears to have neuroprotective properties that may help delay or prevent dementia by improving vascular health, reducing oxidative stress, and preventing Aβ toxicity.60,235 While preclinical and observational studies support its potential benefits, additional randomized controlled trials are necessary to establish definitive recommendations. Given its safety and availability in everyday foods, vitamin K represents a promising path for dementia prevention strategies.60,240 Public health initiatives promoting vitamin K-rich diets could be a practical approach to support cognitive aging.61,244 Overall, fat-soluble vitamins and water-soluble vitamins play crucial roles in the body (Figure 2).
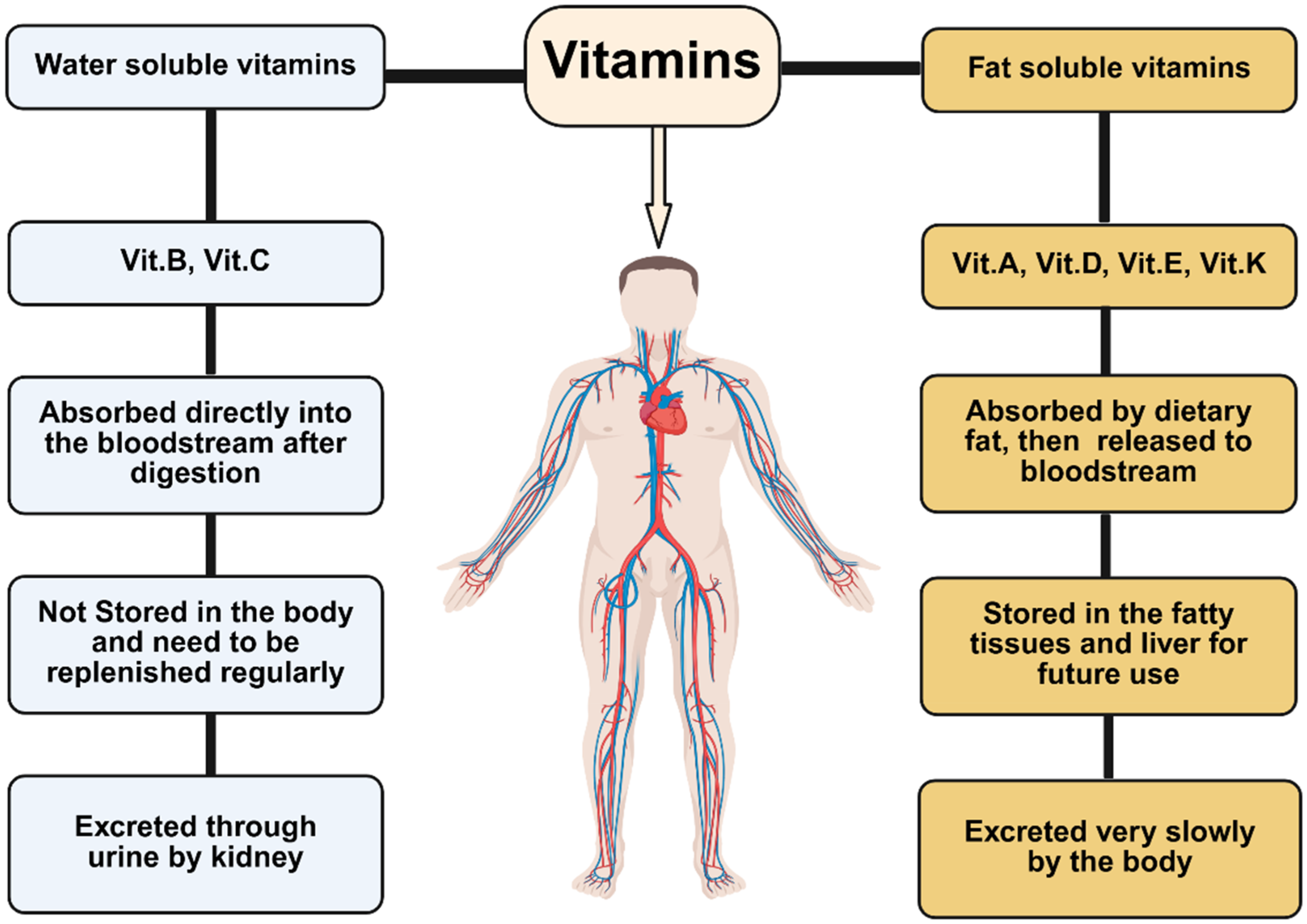
Shows the differences between water-soluble vitamins and fat-soluble vitamins.
Conclusion
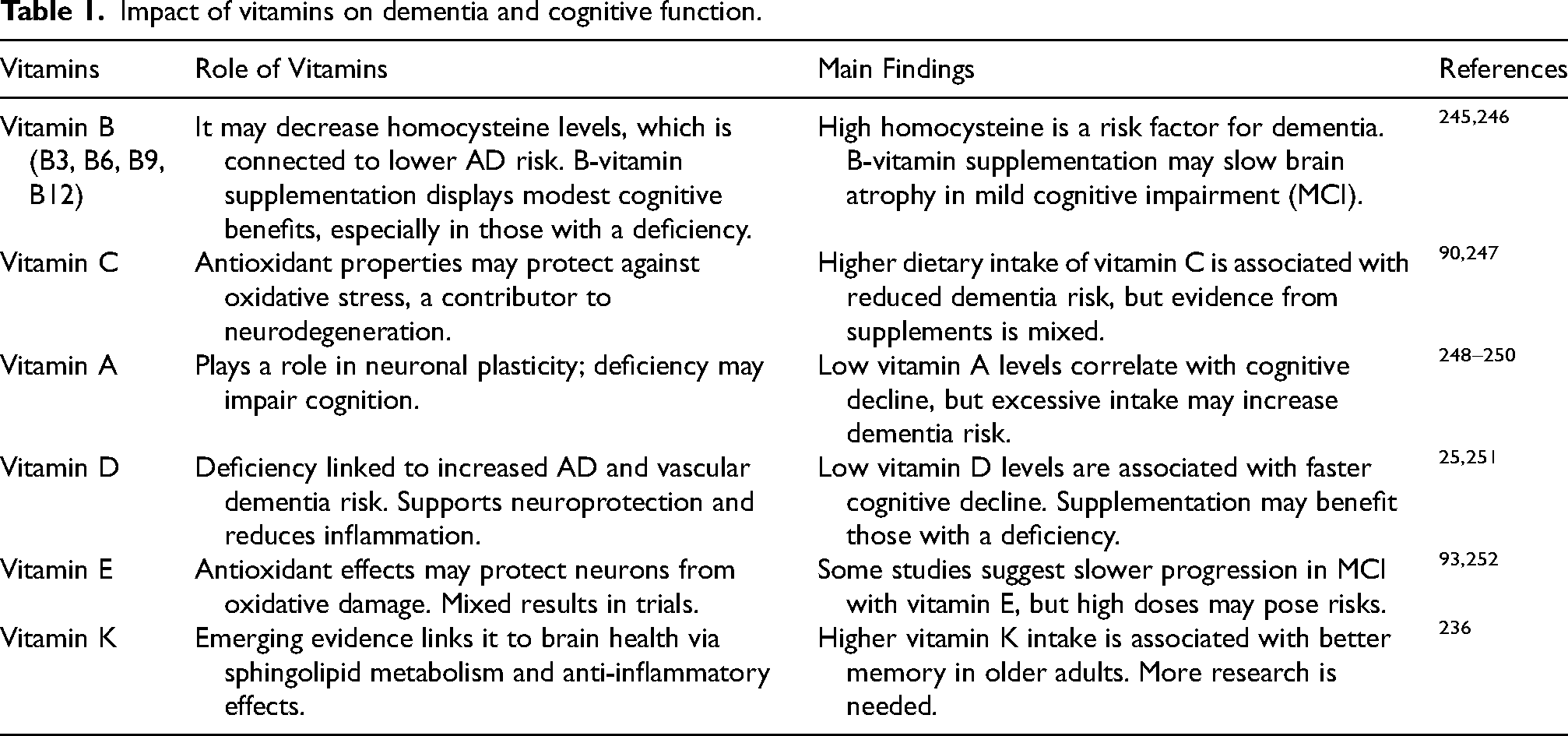
The impact of vitamins C, B, A, D, E, and K on dementia is complex, with each playing a distinct role in brain health. B vitamins, especially B6, B9 (folate), and B12, are vital for lowering homocysteine levels, which are linked to neurodegeneration, while antioxidants like vitamins C and E help fight oxidative stress, a key factor in the progression of dementia. Vitamin D promotes neuroprotection and reduces inflammation, whereas vitamin K supports sphingolipid metabolism, which is crucial for maintaining brain cell integrity. Although vitamin A's role is less clear, its derivatives may affect memory and learning. Collectively, these vitamins underscore the significance of a nutrient-rich diet in potentially delaying or reducing dementia symptoms. However, although evidence indicates their protective effects, excessive supplementation without medical supervision can be risky. Clinical studies show mixed results, highlighting that vitamins alone cannot prevent or cure dementia but may aid brain health as part of a comprehensive approach (Table 1).
Impact of vitamins on dementia and cognitive function.
Future directions and challenges
Research exploring the role of vitamins C, B, A, D, E, and K in dementia is increasingly advancing, with forthcoming studies emphasizing their neuroprotective mechanisms and potential applications in therapeutic interventions. Vitamin C, a potent antioxidant, may help reduce oxidative stress, a significant contributor to neurodegeneration. Concurrently, B vitamins, particularly B6, B9, and B12, are essential for the reduction of homocysteine levels, which are associated with cognitive decline. Future investigations should consider optimal dosages and the synergistic effects of these vitamins in therapies designed to slow or halt the progression of dementia. Vitamins A, D, and E also demonstrate potential in the prevention and management of dementia. Vitamin D's anti-inflammatory and neuroprotective properties may assist in regulating Aβ accumulation, whereas vitamin E's antioxidant effects could protect neuronal membranes from oxidative damage. Vitamin A, through its role in gene regulation and neuroplasticity, may support cognitive function. Subsequent research should incorporate long-term studies to establish causality and evaluate whether supplement intake during midlife can reduce the risk of dementia.
Additionally, personalized approaches considering genetic and lifestyle factors may enhance the efficacy of vitamin-based interventions. Emerging evidence suggests vitamin K, particularly in its K2 form, may play a role in brain health by supporting sphingolipid metabolism and reducing calcium-related neurodegeneration. Combined with vitamins C, B, A, D, and E, a multi-vitamin approach could offer comprehensive neuroprotection. Future directions include conducting clinical trials to test these vitamins in at-risk populations and investigating their interactions with existing dementia treatments. If proven effective, vitamin supplementation could become a cost-effective, accessible strategy for dementia prevention, complementing pharmacological and lifestyle interventions in global brain health initiatives.
Footnotes
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Shahid is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.