
Abstract
Background
Alzheimer's disease (AD) is an incurable condition that places primary caregivers in the challenging position of providing long-term care.
Objective
To characterize quality of life (QOL) and caregiving burden among primary caregivers of patients with AD, identify the correlates of these outcomes, and evaluate the relationship between disease-specific knowledge levels and their QOL and burden profiles.
Methods
A cross-sectional survey was conducted with 120 pairs of patients with AD who were hospitalized between April and September 2023 and their primary caregivers. Sociodemographic and clinical information of patients and caregivers was obtained. Caregivers were assessed using the Chinese versions of the Zarit Burden Interview, Dementia Knowledge Assessment Scale, and 12-Item Short Form Health Survey. Correlates of caregivers’ QOL and caregiving burden were analyzed using stepwise multiple linear regression.
Results
Primary caregivers had high caregiving burden, relatively low disease-related knowledge, and impaired QOL. Patients’ age, disease duration, and the frequency of wandering episodes resulting in missing incidents were identified as key potential risk factors for caregivers’ QOL. However, caregivers’ educational level, the absence of disease, and higher levels of disease knowledge were major protective factors. Core predictors of caregiver burden included compromised Physical and Mental Component Summary scores.
Conclusions
Enhancing caregiver education and improving the availability of community-based care resources for families facing AD in remote regions of Southwest China are urgently needed. Creating culturally sensitive and clinically applicable assessment frameworks is also critical to effectively address the impact of traditional cultural values that turn caregiving duties into a moral obligation.
Introduction
Alzheimer's disease (AD) is a common neurodegenerative disorder in older adults, mainly characterized by progressive cognitive decline, behavioral changes, and eventual disability. 1 The growing number of patients with AD is placing increasing pressure on the global economy and public healthcare systems. By 2050, the number of people living with AD is estimated to reach 131.5 million worldwide. 2 Currently, no cure exists for the disease, 3 placing primary caregivers in the challenging position of providing long-term care.
An epidemiological survey conducted in China in 2020 reported that approximately 9.83 million people aged ≥60 years were living with AD. 4 This trend poses serious health and economic challenges to the country. In 2019, dementia-related mortalities were the fifth leading cause of death in China, with a mortality rate of 22.5 per 100,000 individuals. 5 By 2030, the direct costs associated with the disease are expected to exceed 114.2 billion USD. 5 China currently employs a unique elder care system known as the “9073” model, in which 90% of older adults receive care at home, 7% receive community-based care, and 3% live in care institutions. 6 This makes family caregivers the main providers of care and support for patients with AD in China, a model that differs significantly from that in Western countries, where institutional care is more prevalent. 7 China also has the largest older adult population worldwide, 5 amplifying the burden of elder care.
Primary caregivers of patients with AD are usually those who provide daily care and support, which may include family members, friends, or professional care providers. 8 In China, caregiving for patients with AD relies heavily on family members. 9 Confucian filial piety, a foundational component of Chinese social culture for centuries, emphasizes caring for aging parents as a moral obligation. This traditional value intertwines family responsibilities with social virtues. However, modern society presents challenges to the practice of filial piety. 10 While filial piety requires that children care for and financially support their parents, modern fast-paced lifestyles, financial stress, and limited elder care resources make it increasingly difficult for adult children to meet these expectations. For example, many adult children work away from home and cannot provide regular companionship to their parents, while others cannot afford the high costs associated with elder care. Furthermore, filial piety can be overextended, transforming from a cultural virtue into social pressure. In some families, parents may leverage filial piety to interfere with their adult children's lives. Social expectations associated with filial piety can also create psychological stress in children and limit their personal freedom, particularly when the quality of care provided is unsatisfactory. In 2016, China piloted long-term care insurance and promoted the “integration of medical and elder care” policies. However, these policies face the dual challenge of fragmented services and the absence of family support systems in remote regions, 11 particularly in the frontier ethnic minority regions of China.
Primary caregivers of patients with AD usually experience significant physical strain while performing daily caregiving activities. Caregivers of patients with AD carry a heavier burden than those caring for individuals with other chronic diseases. 12 Kim et al. 13 found that cognitive decline and a reduced ability to perform daily activities in patients with AD can increase caregiver burden. Other studies have shown that caregiver burden is influenced by multiple factors, including their demographic characteristics, the patient's conditions, and other contextual variables. 14 For example, being unemployed or a female caregiver is associated with a higher level of burden. 12
Patients’ cognitive abilities gradually decline as dementia progresses, necessitating caregivers’ participation in decision-making and care planning. This requires caregivers to possess essential knowledge about dementia, including its causes, outcomes, progression, and treatment options, along with the appropriate methods for providing care. 15 Amado and Brucki 16 found that caregivers’ level of knowledge about AD is linked to the timing of diagnosis and treatment. Patients’ risk of hospital readmission can increase when caregivers lack proper preparation and understanding of the disease.9,17 Therefore, caregivers’ disease-related knowledge directly influences patient care and management. A deeper understanding of the disease can help caregivers better cope with patients’ behavioral and psychological symptoms 16 and potentially reduce their burden. 18
Studies have consistently shown that primary caregivers of patients with AD have a lower quality of life (QOL) compared with the general population.19,20 The well-being of caregivers is affected by the patient's core symptoms, the caregiving burden, and personal challenges such as psychological stress, social isolation, and financial strain. Poon 21 found that the heavier the caregiver burden, the poorer the QOL. A study in Egypt 12 found that female caregivers experienced more physical stress than did male caregivers. An international study involving the United Kingdom, Italy, Spain, Germany, and the United States 22 found that caregivers’ QOL worsens with disease severity. These findings highlight the diverse challenges faced by caregivers of patients with AD across different cultural contexts, as well as how they respond and how their QOL is affected. Therefore, conducting cross-cultural research among caregivers of patients with AD is vital.
Most Western studies have been based on institutional care or community support systems. However, such systems may be unsuitable in remote regions of Southwest China because of cultural differences. The relationships and pathways between the disease-related knowledge, caregiver burden, and QOL have not yet been fully validated in such settings. Therefore, this study aimed to explore the relationships between caregiving burden, disease-related knowledge, and QOL among primary caregivers of patients with AD. We also sought to examine how demographic and sociological factors are associated with caregivers’ QOL, providing a non-Western perspective for the aging global population.
Methods
Design and participants
This study employed a cross-sectional design and non-probability sampling. We included 120 pairs of patients with AD admitted to the Geriatrics Department at the Dali Second People's Hospital, Yunnan Province, between April and September 2023, along with their primary caregivers. The inclusion criteria for patients were as follows: (1) AD diagnosis according to the World Health Organization's 10th edition of the International Classification of Diseases 23 ; (2) brain magnetic resonance imaging performed within 6 months before enrollment, showing hippocampal atrophy consistent with an AD diagnosis; (3) relatively stable condition; and (4) informed consent obtained from the legal guardians. The exclusion criteria were as follows: (1) diagnosis of other forms of dementia, such as vascular, Lewy body, frontotemporal, or traumatic brain injury-induced dementia; (2) the presence of severe physical illness; (3) being in the acute stage of an infectious disease; and (4) history of drug or alcohol abuse. For primary caregivers, the inclusion criteria were (1) provision of care for at least 3 months and (2) the ability to communicate clearly, willingness to participate, and provision of informed consent. The exclusion criteria were (1) simultaneously caring for other patients and (2) withdrawal from the study midway.
Data collection
General information. A self-administered questionnaire was used to collect clinical and sociodemographic data from patients with AD and their primary caregivers. For patients with AD, the information obtained included gender, age, ethnicity, occupation, marital status, educational level, disease duration, number of hospitalizations, frequency of wandering episodes leading to missing incidents from home, household economic status, and place of residence. Data collected from caregivers included gender, age, educational level, occupation, marital status, relationship to the patient, daily caregiving hours, whether they lived with the patient, personal medical history, and medication history.
QOL. Primary caregivers’ QOL was assessed using the 12-Item Short Form Health Survey (SF-12). 24 We applied the scoring algorithm for the Physical Component Summary (PCS) and Mental Component Summary (MCS) developed by John E. Ware in 1995, which has been widely used in China.25,26 The scores range from 0 to 100, with higher scores indicating a better QOL. In this study, the scale's Cronbach's alpha coefficient was 0.911.
Caregiver burden. The Zarit Burden Interview (ZBI), originally developed by Zarit et al. 27 in America, was translated into Chinese by Wang et al. 28 This scale assesses caregiver burden across various caregiving situations, such as those related to stroke, dementia, and schizophrenia. It consists of 22 items rated on a 5-point Likert scale (0–4), with total scores ranging from 0 to 88. Higher scores indicate a greater level of caregiving burden. The reliability and validity of the Chinese version of the ZBI are well established. 29 In this study, the scale's Cronbach's alpha coefficient was 0.897.
Dementia knowledge. The Dementia Knowledge Assessment Scale (DKAS) was developed in 2015 at the University of Tasmania. 30 It includes the following four subscales: causes and characteristics of dementia, communication and behavior, care considerations, and risks and health promotion. The scale contains 25 items and is suitable for assessing dementia-related knowledge among untrained healthcare workers and family caregivers. Specifically, the Chinese version of the DKAS (C-DKAS) was adapted by Zhang et al. 31 via three rounds of Delphi consultations with 19 international dementia experts. It uses a 3-point Likert scale (0–2), with a total score ranging from 0 to 50, and includes an additional “Do not know” option. This version reduces the ceiling effect observed in the DKAS and has demonstrated strong reliability and validity. The scale's Cronbach's alpha coefficient in this study was 0.814.
Procedures
All investigators received standardized and rigorous training before conducting the survey. The researchers provided written and verbal explanations of the study's purpose and procedures to the participants, and informed consent was obtained. Questionnaires were completed independently by the primary caregivers. For participants unable to complete the form independently, the researchers used the questionnaire items to conduct structured interviews and recorded their responses. This study adhered to the principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Medical Ethics Committee of the Second People's Hospital of Dali Bai Autonomous Prefecture (Approval No.: 2023-KY-01).
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, N.Y., USA). The marital status categories (“unmarried,” “divorced,” and “widowed”) were combined into the single category of “not currently married” for subsample analyses because of the limited sample size. Patient clinical and demographic characteristics, as well as caregivers’ demographic information, were analyzed using proportions and means ± standard deviations, as appropriate.
Descriptive statistics (including score ranges, maximum and minimum values, means, and standard deviations) were calculated for all scale scores (ZBI, C-DKAS, PCS, and MCS). Internal consistency was assessed using Cronbach's alpha for each scale's total score.
To explore the correlations between the total ZBI, C-DKAS, PCS, and MCS scores for family caregivers of patients with AD, Pearson correlation coefficients were used to examine bivariate relationships between these continuous variables. This analysis was preceded by normality assumption assessment through descriptive measures (skewness and kurtosis), the Shapiro–Wilk test, and visual inspection of Q-Q plots. Group differences in the SF-12 and ZBI scores were compared using independent-samples t-tests or one-way analysis of variance based on demographic characteristics. Independent-samples t-tests were applied for two-group comparisons, while one-way analysis of variance was used for three or more groups. Post-hoc comparisons were conducted using the least significant difference method.
To investigate factors associated with primary caregivers’ QOL scores, multiple stepwise linear regression analysis was performed to examine the relationships between disease characteristics, demographic factors, and scores on the ZBI, C-DKAS, and SF-12. Primary caregivers’ PCS and MCS scores served as the dependent variables for the first analysis. The independent variables were those showing statistical significance in the univariate analysis. Dummy variables were created for caregiver occupation (0 = employee, 1 = farmer, and 2 = retired), medical history (0 = yes and 1 = no), and place of residence (0 = urban and 1 = rural). Entry and removal probabilities were set at p < 0.05 and p > 0.10, respectively. For the second analysis, primary caregivers’ ZBI scores served as the dependent variable. Independent variables were those demonstrating statistical significance in univariate analyses. The C-DKAS score was included in the initial set of candidate models for the stepwise regression because of the conceptual importance of dementia-related knowledge in understanding caregiver burden, allowing the statistical procedure to evaluate its contribution alongside other covariates. Dummy variables were created for the caregiver–patient relationship (0 = spouse, 1 = child, and 2 = Others), co-residence with patient (0 = yes and 1 = no), and place of residence (0 = urban and 1 = rural). Statistical significance for all analyses was set at p < 0.05.
Results
Participants’ general characteristics
A total of 120 patients were included in the study. Among them, 48 (40%) and 72 (60%) were men and women, respectively. Their mean age was 71.64 ± 7.70 (range, 56–85) years. Of the participants, 68 (56.7%) were of Bai ethnicity, and the majority were farmers (80.8%). Regarding the frequency of wandering episodes leading to missing incidents from home, 36.7% of the patients had wandered four or more times. Most families reported their financial status as “adequate” (38.3%), and 52.5% lived in rural areas. Table 1 presents the detailed demographic and clinical data of the patients.
Patients’ baseline demographic and clinical characteristics.
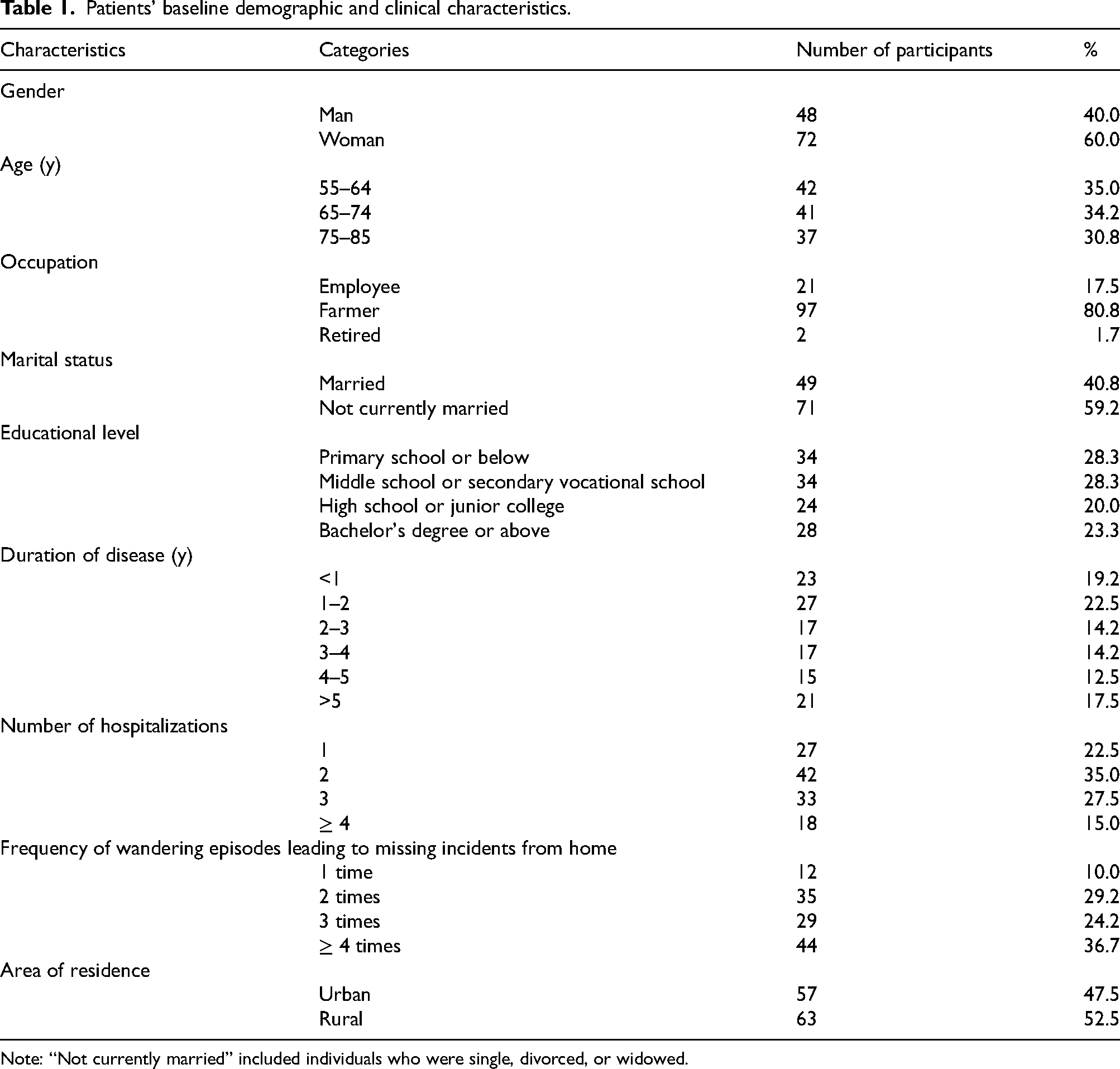
Note: “Not currently married” included individuals who were single, divorced, or widowed.
Overall, 120 primary caregivers participated in the study. Among them, 36 (30%) and 84 (70%) were men and women, respectively. Their mean age was 44.77 ± 20.04 (range, 21–84) years. The majority of caregivers had a middle school educational level (30.8%), and most of them were farmers (55.8%). Furthermore, 66.7% were married. Regarding their relationship to the patient, 40.8% and 35.8% were spouses and children, respectively. Most caregivers spent 7–12 h daily providing care (35.8%). A total of 59.2% of the primary caregivers had a history of illness. Table 2 presents the baseline sociodemographic characteristics of the caregivers.
Caregivers’ baseline sociodemographic characteristics.
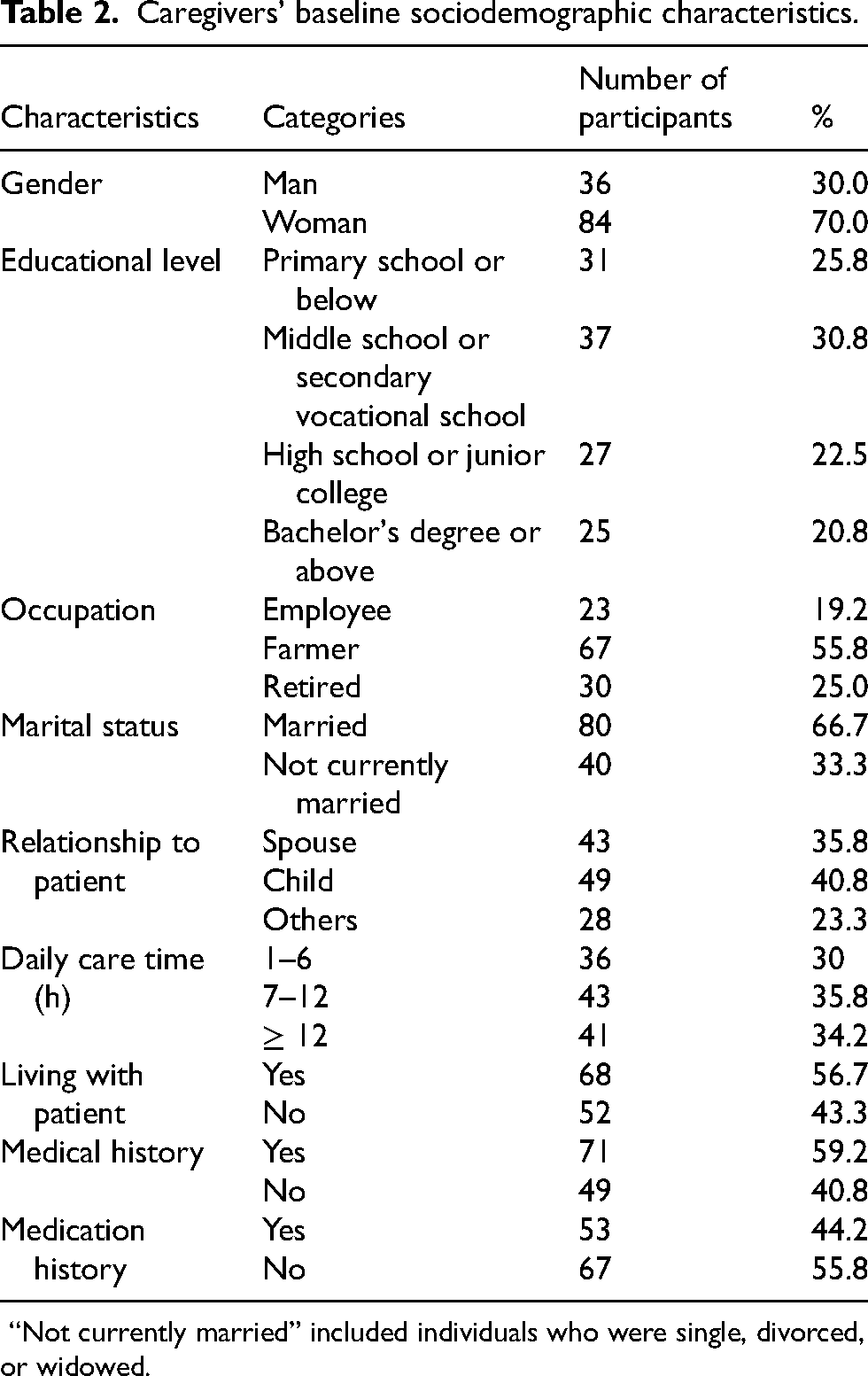
“Not currently married” included individuals who were single, divorced, or widowed.
Overall evaluation results of the caregivers’ ZBI, C-DKAS, and SF-12 scores
The mean ZBI score was 53.31 ± 24.25 points, significantly exceeding the established threshold for moderate-to-severe burden (≥ 41). 32 Moreover, the mean C-DKAS score was 23.27 ± 8.52 points, representing only 46.5% of the maximum achievable score (50 points). Scores on the SF-12 subscales indicated substantial impairment; the PCS and MCS scores were 38.70 ± 11.96 and 40.64 ± 15.06, respectively, with the mean values markedly falling below the theoretical scale midpoint (50 points). Notably, the PCS score was lower than the MCS score. Table 3 shows the primary caregivers’ ZBI, C-DKAS, and SF-12 scores.
Primary caregivers’ ZBI, C-DKAS, and SF-12 scores.
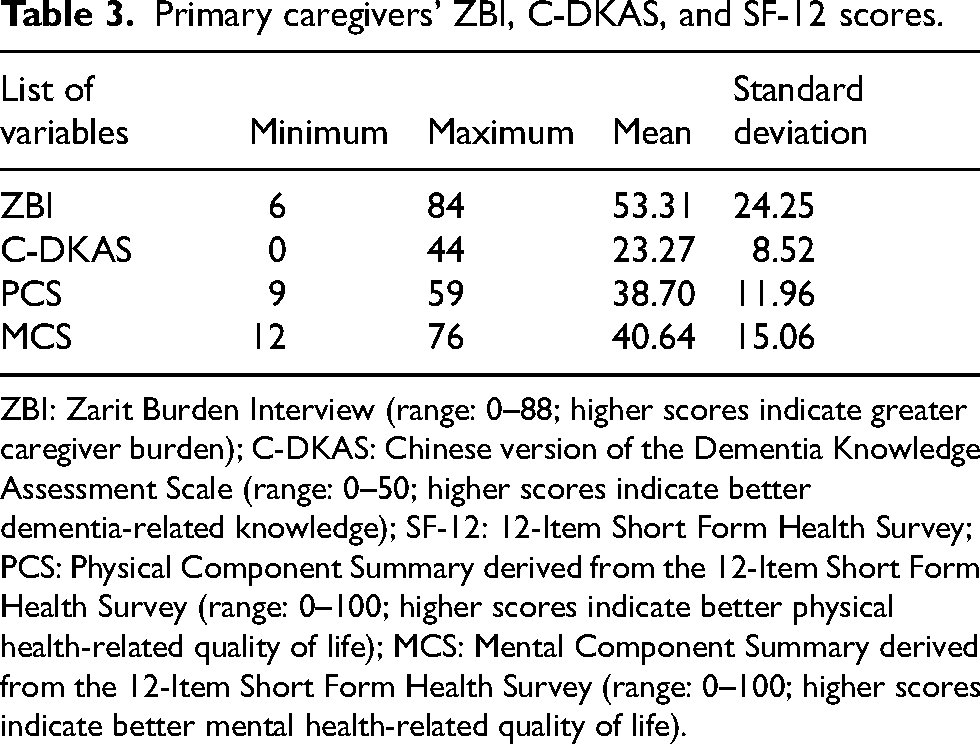
ZBI: Zarit Burden Interview (range: 0–88; higher scores indicate greater caregiver burden); C-DKAS: Chinese version of the Dementia Knowledge Assessment Scale (range: 0–50; higher scores indicate better dementia-related knowledge); SF-12: 12-Item Short Form Health Survey; PCS: Physical Component Summary derived from the 12-Item Short Form Health Survey (range: 0–100; higher scores indicate better physical health-related quality of life); MCS: Mental Component Summary derived from the 12-Item Short Form Health Survey (range: 0–100; higher scores indicate better mental health-related quality of life).
Bivariate analysis
The ZBI score was negatively correlated with both PCS (r = −0.393, p < 0.001) and MCS (r = −0.436, p < 0.001) scores. Conversely, the C-DKAS score was positively correlated with PCS (r = 0.350, p < 0.001) and MCS (r = 0.403, p < 0.001) scores. No significant correlation was observed between ZBI and C-DKAS scores. Table 4 and Supplemental Figure 1 present all correlation coefficients.
Correlation analysis of caregivers’ SF-12, ZBI, and C-DKAS scores.
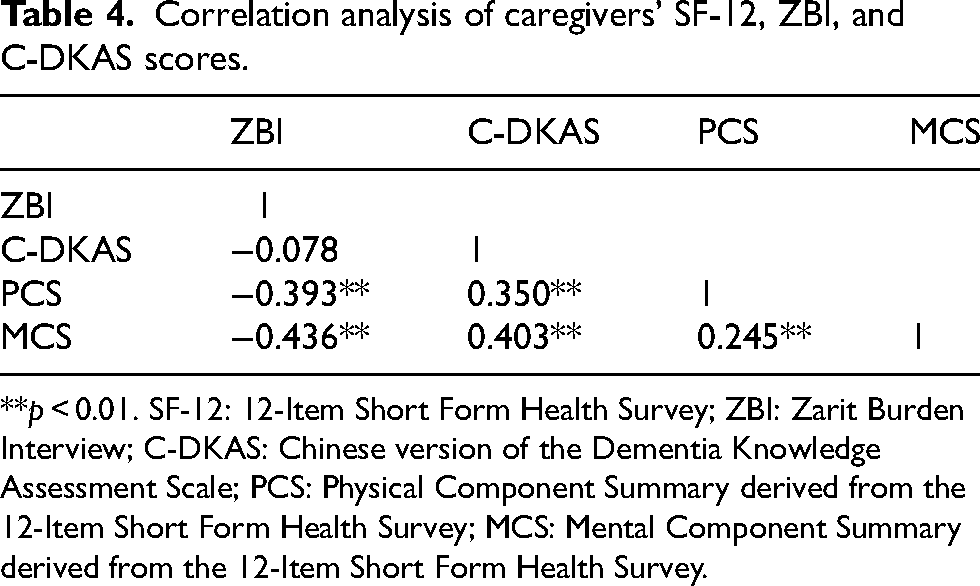
**p < 0.01. SF-12: 12-Item Short Form Health Survey; ZBI: Zarit Burden Interview; C-DKAS: Chinese version of the Dementia Knowledge Assessment Scale; PCS: Physical Component Summary derived from the 12-Item Short Form Health Survey; MCS: Mental Component Summary derived from the 12-Item Short Form Health Survey.
Correlation analysis between the general characteristics of patients and primary caregivers and SF-12 scores
Table 5 presents the associations between the general characteristics of patients/caregivers and SF-12 scores. After adjusting for multiple comparisons, significant group differences were observed in caregivers’ PCS and MCS scores according to patient educational level. Specifically, the scores increased with higher patient educational levels. Patient disease duration was negatively correlated with caregivers’ PCS scores. For MCS scores, significant differences emerged primarily between the short (<2 years) and long (>4 years) duration groups. Increased frequency of wandering episodes leading to missing incidents from home was associated with declining MCS scores among caregivers, although no significant differences were observed for PCS scores. Caregiver educational level was significantly associated with PCS and MCS scores. Spouses exhibited lower PCS scores than children or other caregivers, whereas MCS scores showed no significant group differences. ZBI scores demonstrated a hierarchical burden pattern: spouses exhibited the highest burden (59.49 ± 21.16), followed by children (51.22 ± 25.82) and Others (47.46 ± 24.61; F = 4.645, p = 0.033), demonstrating that caregiver burden significantly decreased as the kinship relationship became more distant. Supplementary Table 1 presents the complete statistics.
SF-12 component scores of caregivers as stratified by patient and caregiver characteristics.
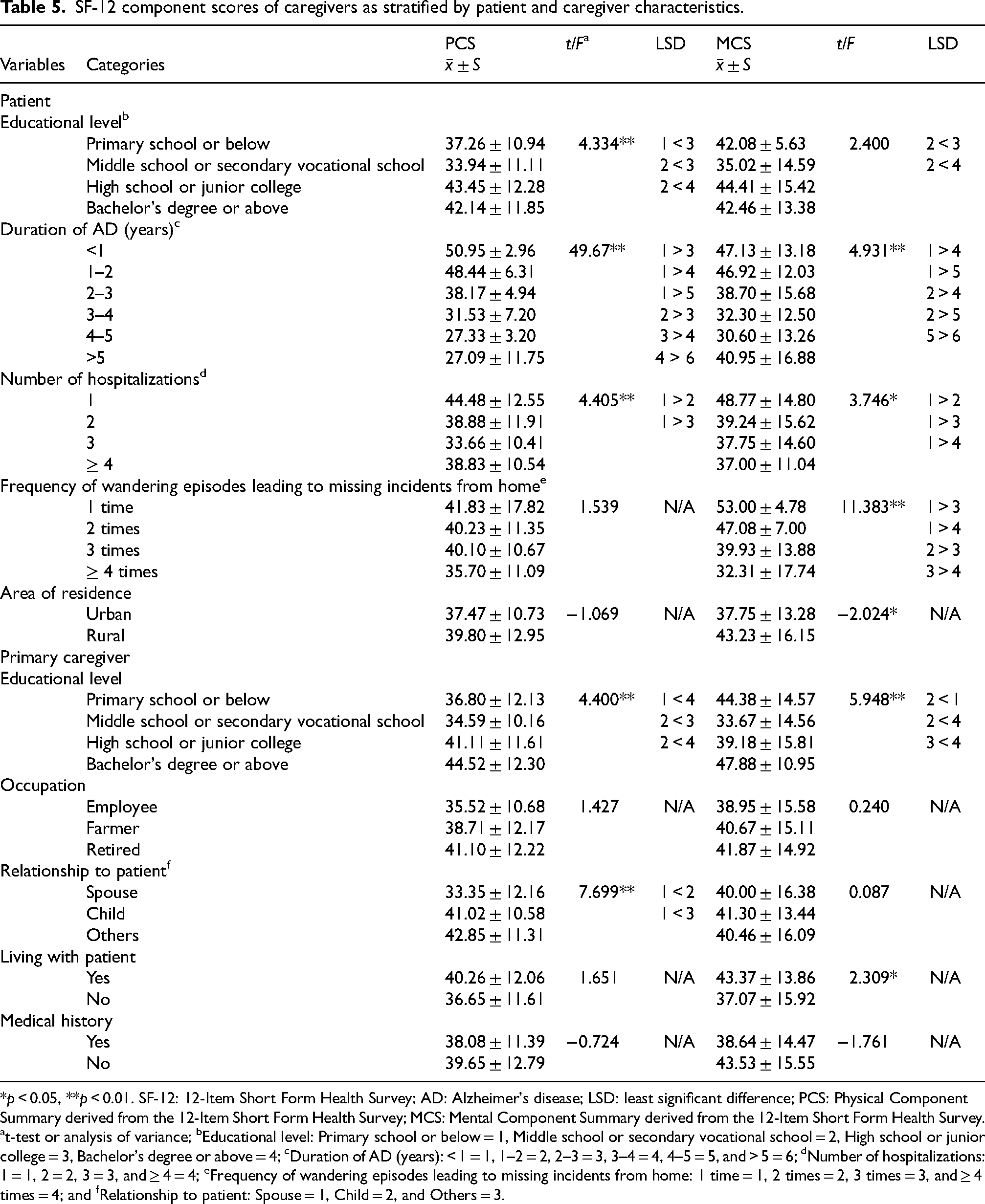
*p < 0.05, **p < 0.01. SF-12: 12-Item Short Form Health Survey; AD: Alzheimer's disease; LSD: least significant difference; PCS: Physical Component Summary derived from the 12-Item Short Form Health Survey; MCS: Mental Component Summary derived from the 12-Item Short Form Health Survey. at-test or analysis of variance; bEducational level: Primary school or below = 1, Middle school or secondary vocational school = 2, High school or junior college = 3, Bachelor's degree or above = 4; cDuration of AD (years): < 1 = 1, 1–2 = 2, 2–3 = 3, 3–4 = 4, 4–5 = 5, and > 5 = 6; dNumber of hospitalizations: 1 = 1, 2 = 2, 3 = 3, and ≥ 4 = 4; eFrequency of wandering episodes leading to missing incidents from home: 1 time = 1, 2 times = 2, 3 times = 3, and ≥ 4 times = 4; and fRelationship to patient: Spouse = 1, Child = 2, and Others = 3.
Multivariate analysis of the SF-12 scores among primary caregivers
Table 6 presents the results of the multiple linear regression analyses. A longer duration of the patient's illness (β = −0.638, p < 0.001) and older patient age (β = −0.152, p < 0.001) were significantly associated with lower PCS scores. Conversely, a higher educational level among caregivers (β = 0.142, p = 0.006) and greater C-DKAS scores (β = 0.115, p = 0.022) were associated with higher PCS scores. Retired caregivers reported significantly higher PCS scores compared with those in other occupations (β = 0.101, p = 0.037). This model accounted for 74.0% of the variance in PCS scores (adjusted R² = 0.740).
Factors associated with caregivers’ PCS and MCS scores.
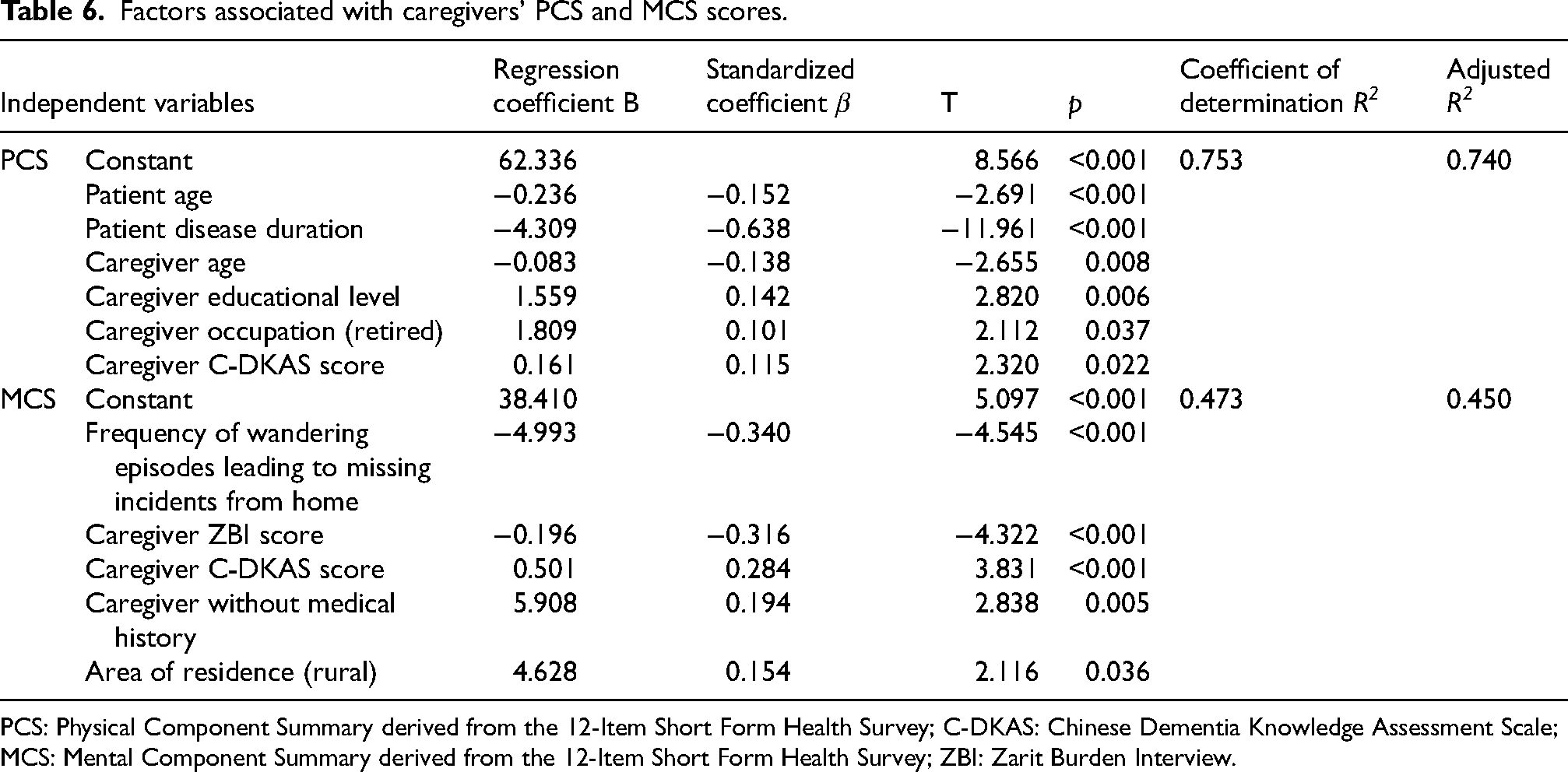
PCS: Physical Component Summary derived from the 12-Item Short Form Health Survey; C-DKAS: Chinese Dementia Knowledge Assessment Scale; MCS: Mental Component Summary derived from the 12-Item Short Form Health Survey; ZBI: Zarit Burden Interview.
Regarding the MCS dimension among caregivers, higher frequency of wandering episodes leading to missing incidents from home (β = −0.340, p < 0.001) and ZBI scores (β = −0.316, p < 0.001) were significantly associated with poorer mental health status. Better C-DKAS scores (β = 0.284, p < 0.001), rural residence (β = 0.154, p = 0.036), and the absence of a history of medical conditions among caregivers (β = 0.194, p = 0.005) emerged as protective factors. This model explained 45.0% of the variance in the MCS scores (adjusted R² = 0.450).
Multivariable analysis of the ZBI scores showed that rural residence was associated with reduced caregiver burden (β = −0.153, p = 0.050). Lower caregiver MCS (β = −0.371, p < 0.001) and PCS (β = −0.197, p = 0.026) scores were associated with higher burden levels. Unexpectedly, higher caregiver C-DKAS scores were associated with increased burden (β = 0.200, p = 0.019). This model accounted for 39.1% of the variance in ZBI scores (adjusted R² = 0.391). Supplemental Table 2 presents the complete statistics.
Discussion
In this study, we examined 120 pairs of patients with AD and their primary caregivers in a remote region of Southwest China. The findings highlight the complex relationship between caregivers’ multidimensional burden, disease-related knowledge level, and QOL. Additionally, the results revealed that primary caregivers experienced a high caregiving burden level, had limited knowledge about the disease, and reported poor QOL. Caregivers’ QOL was associated with both the patients’ and their own sociodemographic characteristics, along with the patients’ clinical features. These findings provide important evidence for a better understanding of the challenges associated with AD caregiving in non-Western settings.
The primary caregivers’ C-DKAS scores were similar to those reported by Zhang et al. 31 but lower than those in Western countries.15,33 Dementia education is incorporated into routine health management in Western countries. However, community health services in the study region still lack standardized training programs. AD symptoms, such as aggressive behavior, influenced by Confucian cultural beliefs, are sometimes viewed as moral failures rather than medical symptoms. 9 This leads to the stigma surrounding the disease, 34 which may cause delays in diagnosis and intervention. Fundamentally, this reflects a lack of public knowledge about the disease, limiting the ability to recognize and anticipate AD symptoms and progression. The delay in seeking medical attention reflects a gap in public health education about AD in this region.
Primary caregivers’ total ZBI score was higher than that reported by Li et al., 11 who found a mean ZBI score of 26.91 ± 15.88 among AD caregivers. This discrepancy may be attributed to geographical differences in the study samples. The participants in the study by Li et al. 11 were from Beijing, an international metropolitan city influenced by modern cultural values. In such settings, caregiving responsibilities are more openly shared, with a greater emphasis on caregivers’ personal development and physical and mental health. Community support and healthcare resources are also more readily available. However, the present study's participants were from ethnic minority communities in the remote border regions of China, and we observed a clear gradient of burden intensity (spouses > children > Others). This phenomenon may stem from multiple factors. First, China has long been deeply influenced by Confucian culture, and the “differential mode of association” theory 35 may provide a pertinent analytical lens for understanding this phenomenon, as it prioritizes care obligations that decrease with relational distance. Spouses, being part of the innermost relational circle, usually assume lifelong care commitments, 36 whereas children internalize caregiving as an inescapable moral duty under filial piety ethics. 9 These clearly defined hierarchies of responsibility may cause the closest kin to take on excessive caregiving duties while neglecting their own needs, leading to increased burden. Second, structural disparities between developed and border regions—including economic development, healthcare accessibility, and social security systems—may directly intensify burden experiences. Caregivers demonstrated limited knowledge of AD, typically mistaking its symptoms for normal aging and fear of social stigma. Consequently, patients were frequently diagnosed only in the middle or late stages of AD, when the demands of caregiving had significantly increased. However, community-based and professional care resources have not kept pace with these growing needs, resulting in an intense “family-based” care model. 37 Overall, caregivers may endure compounded burdens arising from cultural expectations, further amplified by resource scarcity, cognitive gaps, and high care demands—all within a context of limited access to effective support. Besides these contextual factors, the disease-specific progression of AD is a key driver of burden. In our study, multiple comparisons of ZBI scores revealed that the severity of caregiver burden was significantly associated with disease progression indicators, such as longer patient disease duration and increased number of hospitalizations. This pattern in AD may markedly differ from other dementia subtypes.38,39 A previous cohort study with an 18-month follow-up found that caregiver burden in AD was lower than that associated with frontotemporal and Lewy body dementia. 38 Caregivers of patients with frontotemporal dementia experience greater burden and psychological strain due to early-onset behavioral disinhibition and personality changes, 39 while those caring for individuals with Lewy body dementia must continually manage visual hallucinations, Parkinsonian symptoms, and fluctuating cognition, all contributing to elevated burden.38,39 Therefore, disease heterogeneity is an important factor contributing to differences in caregiver burden, underscoring the necessity of developing precise support strategies tailored to specific dementia subtypes. This study highlights that < 5% of care for older adults is supported by community services under China's “9073” elder care model. Caregivers in remote and ethnic minority regions face the patient's irreversible progressive decline and lack systematic support due to geographically constrained resources, leaving them isolated and unsure of how to seek help. Therefore, developing culturally adapted, long-term support systems consistent with the trajectory of AD is urgently needed.
Multiple regression analysis of ZBI scores showed that lower MCS and PCS scores were major determinants of higher ZBI scores. This finding aligns with those of previous studies. 32 Although univariate analysis showed that spouses bore the heaviest burden, neither the relationship to patient nor co-residence status remained significant in the final model after controlling for MCS, PCS, and place of residence. A possible explanation is that PCS and MCS, being stronger predictor variables, masked the independent contribution of kinship. Alternatively, this could be because spouses experience less visible strains or greater conflicts in role expectations, 40 pressures not captured by the generic SF-12 items but directly impacting ZBI items. Furthermore, the protective effect of rural residence on ZBI scores may be associated with the extended family structures prevalent in rural areas, where daily care responsibilities are shared among members through division of labor. 20 These factors may buffer the stress experienced by primary caregivers. Moreover, future longitudinal studies merit investigation of these dynamics.
We also found that caregivers experienced a high physical burden and relatively low psychological burden, with an overall poor QOL. These results align with the findings of Ibrahim et al. 12 and were worse than those reported by Okuda et al. 41 in Japan. This “relatively low” psychological burden score may have multifaceted origins. First, in-depth analysis revealed an urban–rural disparity in caregivers’ MCS scores, with rural caregivers scoring higher than their urban counterparts. This may be attributed to the study area's status as an ethnic minority region, where rural families usually live in multigenerational households. Such family structures may provide emotional support and help reduce psychological stress. Close kinship and neighborhood ties in rural areas may also promote mutual assistance and help share caregiving burden, 19 suggesting that informal support systems play a key role in maintaining mental health. Second, the observed low psychological burden does not necessarily indicate good mental health among caregivers; rather, it may reflect the limitations of the measurement tool (SF-12 MCS) in capturing psychological distress within specific cultural contexts. Third, it could stem from social desirability bias inherent in self-administered questionnaires, 42 which may suppress caregivers’ truthful reporting of negative psychological states. This highlights the urgent need to develop specific assessment tools that integrate cultural context, emotional expression patterns, and social support dimensions. However, no significant difference was observed in PCS scores between urban and rural caregivers, suggesting that future research is needed to understand the physiological adaptation mechanisms among rural populations engaged in physical labor. We also found that retired caregivers exhibited a physical advantage (higher PCS score), possibly due to being relieved from occupational physical demands and the benefits of regular routines for self-health management. This indicates that relief from the dual burden of occupation and caregiving is a key protective factor.
Multiple regression analysis revealed that patient age and disease duration were the main potential risk factors associated with lower PCS scores, while the frequency of wandering episodes leading to missing incidents from home was the main potential risk factor for lower MCS scores. Caregivers’ higher educational level and absence of medical history emerged as protective factors. These findings align with those of previous studies,11,20 confirming that caring for patients with advanced-stage AD has a cumulative negative effect on caregivers’ physical health. 43 In our sample, 30.8% of patients were aged ≥75 years. Older patients usually present with additional chronic conditions and are physically frail, requiring frequent assistance with turning in bed, toileting, and other basic tasks. As the disease progresses from mild to moderate or severe disability, caregiving responsibilities shift from simply supervising medication intake to fully assisting with activities such as eating and dressing. This significantly increases caregivers’ physical workload, contributing to a greater burden on their physical health (i.e., lower PCS scores). 44 More critically, wandering incidents demonstrated devastating impacts: the MCS scores in the group with four or more such incidents plummeted compared with those in the one-incident group (β = −0.340, p < 0.001). Patients with AD usually exhibit neuropsychiatric symptoms, such as wandering or going missing. Such episodes are associated with the risk of falls, injuries, and dehydration, elevating caregivers’ psychological stress and inducing feelings of fear and helplessness, 45 thereby reducing their MCS scores. Collectively, early diagnosis, active symptom control, delaying disease progression, and preventing wandering incidents constitute key intervention targets.
In the multiple regression analysis, higher ZBI scores were identified as a potential risk factor for lower MCS scores, aligning with previous studies’ findings.12,46 Caregivers typically experience physical fatigue while assisting patients with basic daily activities such as eating, drinking, and toileting—a burden that is more pronounced among female caregivers. 12 However, in our study, we did not observe a significant gender difference in MCS scores. This may be because 56.7% of our sample was from the Bai ethnic group, whose traditional culture values and empowers women in social and familial roles, 47 potentially buffering the influence of gender on the MCS outcomes. Unfortunately, we could not quantitatively assess the influence of Confucian filial piety values. Existing measurement tools for Confucian values and traditional cultural beliefs 48 have primarily been validated among Chinese students studying locally and abroad. However, their reliability and validity in the primary caregiver population have not been adequately tested. Although Confucian filial piety usually emerges as a salient cultural theme in qualitative analyses, suggesting its potential significance in shaping caregiving experiences (e.g., motivation or perceived obligation), its non-quantifiable nature in this study implies that these interpretations should only be regarded as evidence-based, plausible inferences. The absence of culturally validated instruments across regions, along with the disconnect between culturally specific values and disease-related variables, remains a long-standing challenge in cross-cultural research. Therefore, new interdisciplinary innovation is urgently required to address these methodological limitations. Future research could develop culturally sensitive and clinically applicable assessment tools by integrating approaches from cultural psychology, epidemiology, and psychometrics.
Multiple regression analysis also showed that the C-DKAS score was positively correlated with QOL, particularly in the MCS domain, suggesting the potential for future interventions. This finding aligns with those of previous studies.15,49 Greater knowledge may enhance preparedness, which can consequently improve caregivers’ mental health. A caregiver's level of disease knowledge directly affects patient management. Understanding AD can help caregivers respond more effectively to behavioral and psychological symptoms, thereby improving patients’ overall QOL. 16 Interestingly, while univariate correlation analysis revealed no significant association between the C-DKAS and ZBI scores, multivariate regression analysis demonstrated that higher C-DKAS scores were associated with greater ZBI scores, which differs from previous conclusions. 50 This seemingly contradictory phenomenon is not statistically uncommon and may stem from a “suppression effect,” 51 where the underlying relationship between dementia-related knowledge and caregiving burden in univariate analysis was potentially masked by other variables correlated with both. When these variables were included and statistically controlled for in the multivariate model, the unique and directionally reversed association between dementia-related knowledge and caregiving burden became apparent. A potential explanation for the positive correlation between higher levels of disease knowledge and caregiving burden lies in the absence of systematic psychological support modules at local community/village clinics. While higher levels of disease knowledge may enhance caregivers’ awareness of AD's irreversible nature and long-term care demands, the lack of professional psychological support can trigger “anticipatory despair,” thereby exacerbating their perceived burden. 19 Goldberg's study 52 supports our perspective, suggesting that merely providing disease knowledge is insufficient for caregivers with high filial maturity. Providing long-term emotional support to help them cope with persistent grief and unresolved sorrow stemming from difficulty accepting parental illness is equally crucial for improving their mental health and well-being. Collectively, our data demonstrate that, while increased levels of disease knowledge improve the MCS scores, it concurrently elevates the ZBI scores. This challenges the presumption that “knowledge inherently empowers,” and may instead reveal its double-edged effect in resource-limited settings. The “more knowledge, deeper distress” phenomenon likely stems from systemic support deficiencies 53 rather than knowledge per se being detrimental, although further validation is warranted. This discovery underscores that didactic disease knowledge dissemination alone in resource-constrained communities with limited psychological support infrastructure may paradoxically exacerbate emotional burden. Consequently, integrating targeted psychosocial interventions becomes imperative.
In this study, conducted within a non-Western context with a distinct cultural background, we observed core features that differ significantly from those of Western person-centered dementia care models. 44 First, we identified a clear caregiving responsibility gradient (close relatives > Others), indicating that caregiving motivation stems primarily from duty-bound obligation rather than personal choice. This phenomenon may relate to China's current dementia care policy framework: although the government has piloted “long-term care insurance” and “integrated medical–nursing care demonstration sites” to alleviate care burdens, 11 these initiatives remain non-universal. Institutional care remains inaccessible in remote regions, compelling patients with AD and caregivers to opt for home-based care. Second, reliance on tight-knit family networks constitutes the primary support source—a sharp contrast to Western professional service systems. 44 This reflects fundamental differences in social welfare infrastructures. Furthermore, the relative scarcity of formal care resources in rural China (e.g., interdisciplinary teams and professional nursing facilities) likely necessitates heavy dependence on family informal care. These observed characteristics provide crucial non-Western perspectives and empirical evidence for understanding global diversity in AD care practices.
Limitations
This study had some limitations. Single-region sampling may have underestimated the variations in the more developed eastern regions of China. The participant cohort was comprised solely of an AD population. Additionally, the cross-sectional design limited the ability to draw causal inferences. Building on these limitations, future research should systematically compare caregiving experiences among different dementia subtypes and across China's diverse ethnic populations to elucidate the impact of disease heterogeneity on caregiving burden and identify cultural protective/risk factors. Moreover, the “filial maturity” framework should be incorporated to longitudinally track intergenerational role adaptation processes. Separately, future studies should evaluate differences within China's “9073” elder care model, focusing on using the institutionalized 3% subgroup as a reference. Although we aimed to explore the differences between Eastern and Western outcomes from a cultural perspective (such as the influence of Confucian values), cultural factors were not quantitatively measured. Therefore, future research should consider developing internationally applicable cross-cultural assessment tools to systematically evaluate cultural beliefs across global contexts, and establish multinational collaborations for comparative studies on dementia care disparities.
Conclusion
Primary caregivers of patients with AD in remote regions of Southwest China encounter many challenges, including a high caregiving burden, low levels of disease-related knowledge, and poor QOL across various aspects. Notably, a clear responsibility gradient was observed (spouses > children > Others). The most significant correlates of caregiver burden included compromised PCS and MCS scores. A higher level of disease knowledge was associated with improved MCS scores and increased caregiver burden. For PCS, patient age and disease duration were primary drivers. However, the most sensitive correlate for MCS was the frequency of wandering episodes leading to missing incidents from home, exacerbated by caregiver burden. The convergence of the responsibility gradient and resource scarcity may constitute a unique challenge in ethnic minority communities. Notably, the present findings provide valuable evidence to support the improvement of community-based care services within China's “9073” elder care model. They also highlight the urgent need to enhance caregiver education and expand community care services in remote, minority-populated regions. This study provides empirical support for the development of a culturally sensitive dementia care system in developing countries. More specifically, it emphasizes the need to establish a dynamic assessment framework that is culturally sensitive and clinically practical for addressing the influence of Confucian filial piety. Such efforts could pave the way for culturally tailored dementia care systems in developing countries.
Policy recommendations
We propose a tiered and implementable intervention framework beginning with low-education caregivers, for whom visual educational materials integrating local ethnic attire and lifescapes should be developed, such as Bai ethnic-themed illustrated AD booklets and dialect-narrated educational videos. These resources could be distributed through village clinicians, while leveraging village broadcast systems and traditional festival platforms for broader dissemination. Pilot “caregiver respite stations” should be established at township health centers or community clinics for high-burden caregivers to deliver the following three core services: respite care, foundational skill-building workshops, and psychological first aid with preliminary counseling and referral pathways. Concurrently, populations at high risk of AD require implementation of rapid dementia screening protocols to enable early detection, coupled with proactive symptom management for diagnosed patients using wearable tracking technology to mitigate wandering incidents. Finally, establishing a dementia care service network necessitates integrating caregiver burden and QOL metrics into annual health assessments to dynamically monitor high-risk subgroups, while advocating for policy reforms that formally incorporate AD caregiver support services—particularly respite care, competency training, and psychological support at community health facilities—into governmental budgeting systems. This should be operationalized through a three-tiered (province–prefecture–county) cost-sharing framework with prioritized fiscal allocation to resource-constrained ethnic minority regions.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251390494 - Supplemental material for Caregiving burden, disease-related knowledge, and quality of life among primary caregivers in Alzheimer's disease: A cross-sectional study
Supplemental material, sj-docx-1-alz-10.1177_13872877251390494 for Caregiving burden, disease-related knowledge, and quality of life among primary caregivers in Alzheimer's disease: A cross-sectional study by Yu Zhang, Xiaojiao Dong, Yunbin Yang, Xiuyun Wang and Tingting Zhao in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
Ethical considerations
This study protocol adhered to the principles outlined in the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Second People's Hospital of Dali Bai Autonomous Prefecture (Approval No.: 2023-KY-01).
We did not utilize any generative AI or AI-assisted technologies for content generation or data analysis. The only tools employed were basic grammar and spell-checking software.
Consent to participate
All participants provided verbal informed consent.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dali Science and Technology Bureau Key R&D Program (D2022NB1205) and the Yunnan Association for Science and Technology—Expert Workstation on Cognitive and Emotional Disorders in the Elderly, Dali Second People's Hospital (Document No. [2022]46).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.