
Abstract
Background
Alzheimer's disease (AD) is a progressive neurodegenerative disorder where early diagnosis is essential for effective care.
Objective
This paper is set to compare the diagnostic performance of cognitive tests (Mini-Mental State Examination and Montreal Cognitive Assessment), serum biomarkers, EEG, and MRI separately and in combination with PET-CT results in the early diagnosis of AD.
Methods
The cognitive assessment was made in 384 individuals. blood sampling (biomarker tests), EEG monitoring, MRI, and PET-CT scans. Sensitivity, specificity, positive predictive value, and negative predictive value were used to determine diagnostic performance. The additional rule of probability and the product rule of probability were used to determine combined diagnostic power. ROC curves were plotted to visualize the performance of any modality.
Results
Among 384 participants, PET-CT confirmed AD in 192 cases (50%). Serum biomarkers showed the highest individual sensitivity (77.60%), followed by MRI (69.79%), EEG (66.67%), and cognitive tests (62.50%). All modalities had a specificity of 84.90%. When combined using the addition rule of probability, diagnostic sensitivity increased to 99.15% and specificity to 99.95%. ROC curve analysis showed serum biomarkers and MRI had the highest diagnostic accuracy. The multi-modal approach significantly improved early diagnostic performance compared to single modalities.
Conclusions
Serum biomarkers and MRI showed the best individual performance, though accuracy was only moderate. Combining modalities with the addition rule improved sensitivity and specificity markedly, while the product rule yielded low sensitivity and moderate specificity. Multimodal strategies may enhance early detection of AD but require further validation
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disorder characterized by progressive cognitive decline, including memory loss and changes in behavior and other mental functions.1–3 The aging of the world population is steadily increasing the prevalence of AD in the population, and therefore it is of utmost importance to clinical practice and research to diagnose this condition as early and as precisely as possible.4,5 Timely diagnosis can help to provide early treatment and planning of care and improve the potency of evolving curing approaches, which strive to drastically reduce the speed of the disease process. 6
Clinical assessment as well as neuropsychological testing has long been a major element of diagnosing AD, 7 the current revolution in biomedical technology has already presented various diagnostic tools with significant insight into the structural, functional, and molecular changes involved in the disease. 8 Positron emission tomography–computed tomography (PET-CT) has been identified as the gold standard in confirmation of pathology of AD, especially with visualization of amyloid plaques and tau tangles.9–12 PET-CT, although it has high specificity, is costly and not accessible, and radioactive tracers are used, and these factors present limitations to PET-CT being used as a routine procedure in most clinical practices. 13
To overcome these shortcomings, the idea of a multi-modal diagnostic system has been popularized, which consists of combining different non-invasive and inexpensive tools to increase diagnostic sensitivity. Simple mental status examinations, including the Mini-Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA), are also needed to assess the cognitive status and hamper the onset of changes. 14 Serum biomarkers, such as amyloid-β (Aβ), tau proteins, and so on, are viewed as a window to the biochemical process of the disease and are gaining broader acceptance in terms of early detection. 15 Electroencephalography (EEG) can give real-time data about brain activity and neural associations such that functional disruptions are easily uncovered before structural damage becomes apparent.16,17 Magnetic resonance imaging (MRI), on the other hand, helps in the visualization of brain atrophy and other structural abnormalities linked to AD.18–20
All these modalities add complementary and unique information. Cognitive tests record the existence of the lesser behavioral and functional performance, serum biomarkers indicate underlying disease pathology, EEG electrophysiologic abnormalities, and MRI anatomical abnormalities. In combination, the use of these tools can make a significant difference in the precision of diagnosis, especially during the early phase of the disease, where the cost of intervention is highest.
This research study is aimed at comparing the diagnostic performance of cognitive tests, serum biomarkers, EEG, and MRI—alone and in combination with PET-CT findings—as potential alternatives to PET-CT for the early diagnosis of AD. The proposed research will attempt to establish an evidence-based framework by comparing the sensitivity, specificity, and predictive value of each single modality and by combining the performance levels of each modality using both probabilistic addition and probabilistic product rules. An effective and practical multi-modal diagnosis of AD can be established.
Methods
The aim of this prospective diagnostic accuracy study was to determine the sensitivity of the four diagnostic modalities—cognitive tests (MMSE and MoCA), serum biomarkers, EEG and MRI—in identifying AD against the results of PET-CT, which was the gold standard. 21 The study was approved by the institutional ethics committee, and all participants provided informed consent. Suspected cases of early-stage AD were recruited, and their clinical and demographic information, such as age, gender, and symptoms related to thinking, was documented in a systematic manner.
The cognitive assessment was carried out using the MMSE and the MoCA. MoCA has more executive function-related and abstraction tasks than MMSE and supports orientation, attention, memory, language, and visuospatial abilities. Each of the tests was administered by certified neuropsychologists in a standardized clinical environment. The MMSE was scored out of 30, with cutoffs of 24–30 indicating no impairment, 18–23 mild impairment, and 0–17 severe impairment. 14 The MoCA was also scored out of 30, with scores below 26 indicating cognitive impairment and 26–30 considered normal cognitive function. 22
For the purposes of diagnostic accuracy analysis and receiver operating characteristic (ROC) curve generation, MMSE and MoCA results were considered together as a single cognitive screening category. A participant was classified as “cognitive test positive” if either MMSE or MoCA fell below the established cutoff for impairment, and “negative” if both were above cutoff. This approach was chosen to maximize sensitivity and reflect how cognitive screening is often applied in practice.
Venous blood was collected aseptically and analyzed using immunoassays for Aβ42, total tau (t-tau), and phosphorylated tau (p-tau). A reduced Aβ42/Aβ40 ratio and elevated tau levels were considered markers of AD pathology.
For ROC analysis, the serum biomarker panel (Aβ42, Aβ40, total tau, and phosphorylated tau) was combined into a single diagnostic variable. This composite classification was based on a reduced Aβ42/Aβ40 ratio together with elevated tau levels (t-tau and/or p-tau). The resulting biomarker index was then used in contingency tables and ROC curve analysis against PET-CT as the gold standard.
EEGs in a resting state were recorded according to the international 10–20 electrode montage. Participants were instructed to remain comfortably seated with their eyes closed during the recording. EEG analysis focused on AD-specific patterns, including increased theta and delta activity and decreased alpha and beta activity. Where available, event-related potentials, like delayed P300 responses, were also assessed.
To determine structural brain changes, high-resolution T1-weighted MRI scans were carried out. The emphasis was made on hippocampal atrophy and cortical thinning. Other images (T2-weighted and FLAIR) were taken to identify white matter hyperintensities. Radiologists who read all of the scans were blinded to the PET-CT results.
PET-CT was used as the benchmark. The presence of amyloid plaque was observed applying amyloid PET tracers. There was radiotracer injection of the participants and capture via hybrid PET-CT scanner. It was established that AD is positive after the presence of amyloid plaques or tau tangles.
The individual modalities were evaluated with respect to their objective performance in the study sample using standard statistical terms: sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Sensitivity was established to be the ratio of the true positive earlier recognized by the test, and specificity had been termed as the ratio of true negative earlier recognized by the test. PPV showed the true likelihood that a positive test was an indication of the disease, and NPV showed the true likelihood that a negative test indicated a lack of disease. Such measures were computed with the help of 2 × 2 contingency tables, and the results of PET-CT provided the gold standard. Also, the ROC curves were calculated to account for how well each modality could perform diagnoses, and the area under the curve (AUC) was taken as an aggregate of precision. With IBM SPSS version 27, all statistical calculations were done.
To assess the diagnostic strength of using multiple modalities, it would follow that the addition rule of probability and the product rule of probability will be utilized as probabilistic models. These designs can be used to aid in estimation of the accuracy of tests that improve the overall accuracy of testing compared to using the single tests individually.
The likelihood of stating that at least one of the tests will identify AD accurately was estimated using the addition rule of probability. This strategy is more applicable where the settings are clinical, where a high level of sensitivity is required to avoid missing diagnoses. The formula for combined sensitivity using the additional rule is: 1 – (1 – S_Cognitive) (1 – S_Biomarker)(1 – S_EEG)(1 – S_MRI). 23 Similarly, the combined specificity using the addition rule is 1 – (1 – Sp_Cognitive)(1 – Sp_Biomarker)(1 – Sp_EEG) (1 – Sp_MRI). 23 These formulas assume that the tests are statistically independent and provide a more inclusive estimate of diagnostic capability.
In contrast, the product rule of probability was applied to estimate the likelihood that all tests would simultaneously agree on the diagnosis. This method is more conservative and is typically used when high specificity is required, such as in confirmatory testing where false positives must be minimized. The formulas for combined sensitivity and specificity using the product rule are S_Cognitive × S_Biomarker × S_EEG × S_MRI and Sp_Cognitive × Sp_Biomarker × Sp_EEG × Sp_MRI. These calculations provide a comprehensive understanding of how combining diagnostic tools can enhance or limit diagnostic accuracy depending on the clinical context.
Results
A total of 384 participants with suspected early-stage AD were enrolled in the study, comprising 193 males (50.26%) and 191 females (49.74%). The mean age was 74.56 ± 8.60 years. PET-CT findings revealed that 192 participants (50.00%) were positive for AD, while the remaining 192 were classified as normal individuals (Table 1).
Descriptive statistics of variables.
*PET-CT findings used as the diagnostic gold standard.
The diagnostic accuracy of individual modalities showed that Serum Biomarkers had the highest sensitivity at 77.60%, followed by MRI at 69.79%, EEG at 66.67%, and Cognitive Tests at 62.50%. All four modalities demonstrated the same specificity of 84.90%. Positive predictive values ranged from 80.54% for Cognitive Tests to 83.71% for Serum Biomarkers, while negative predictive values ranged from 69.36% to 79.13% (Table 2).
Cognitive tests, EEG, serum biomarkers, and MRI compared with PET-CT findings.
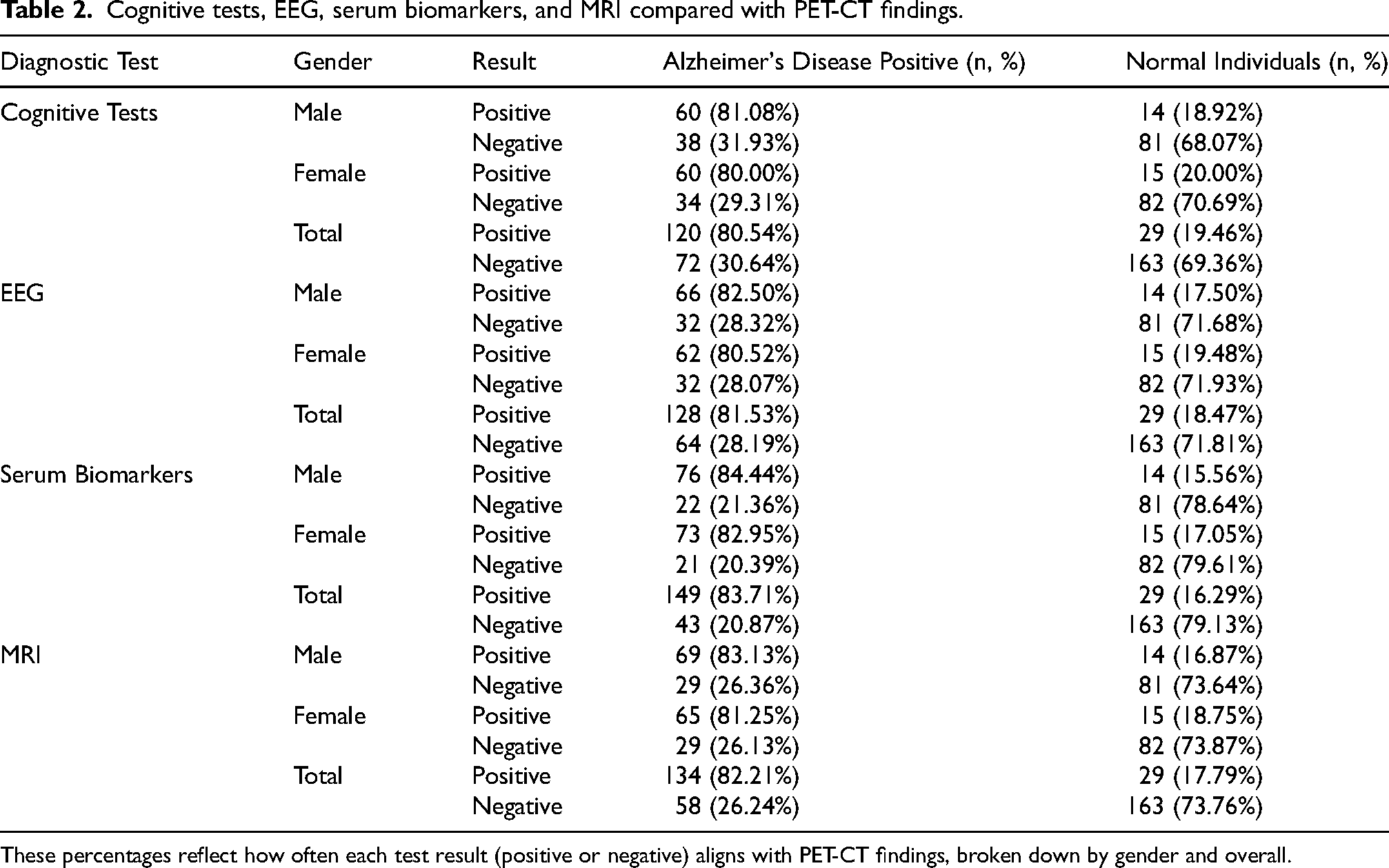
These percentages reflect how often each test result (positive or negative) aligns with PET-CT findings, broken down by gender and overall.
When combining diagnostic modalities, the addition rule of probability significantly improved sensitivity. The combination of Serum Biomarkers and Cognitive Tests yielded a combined sensitivity of 91.60%, which increased to 97.20% when EEG was added, and further to 99.15% with the inclusion of MRI. Conversely, the product rule, which requires all tests to be positive, resulted in lower combined sensitivities: 48.50% for Serum Biomarkers and Cognitive Tests, 32.33% with EEG added, and 22.57% when MRI was also included (Table 3).
Combined specificity, calculated using the product rule decreased as more tests were added: 72.08% for two tests, 61.20% for three, and 51.96% for all four. However, when using the additional rule, combined specificity increased dramatically, reaching 99.95% for the full combination of all four modalities (Table 4).
Diagnostic accuracy of cognitive tests, EEG, serum biomarkers, and MRI.

Combined statistics of cognitive tests, EEG, serum biomarkers, and MRI.
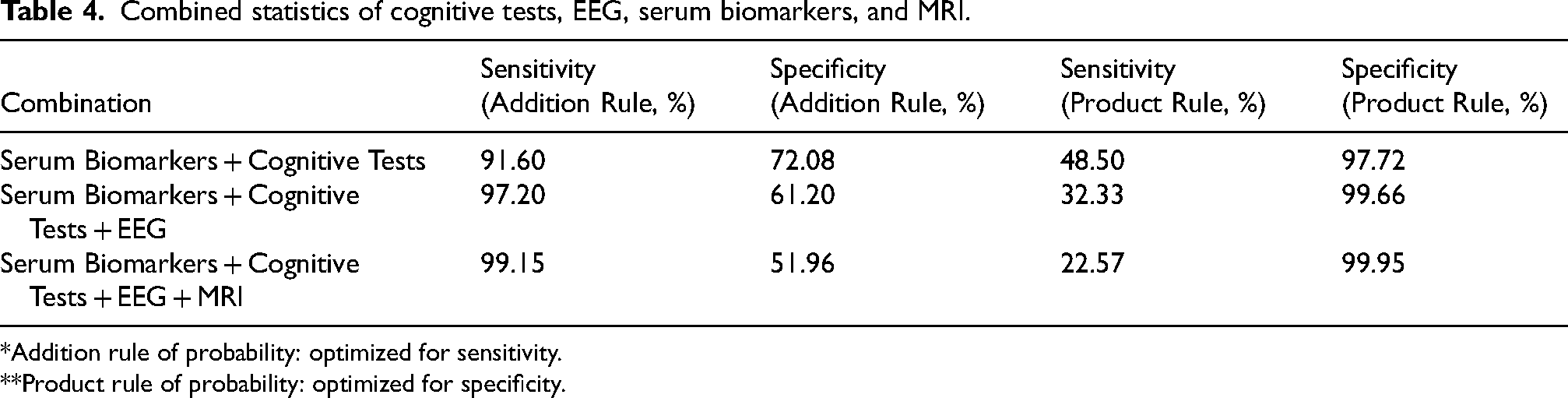
*Addition rule of probability: optimized for sensitivity.
**Product rule of probability: optimized for specificity.
ROC curve analysis (Figure 1) visually confirmed the diagnostic performance of each modality. Serum Biomarkers and MRI demonstrated the highest AUC, indicating strong diagnostic capabilities. EEG and Cognitive Tests, while slightly lower in AUC, provided valuable complementary information, especially when used in combination with other modalities.
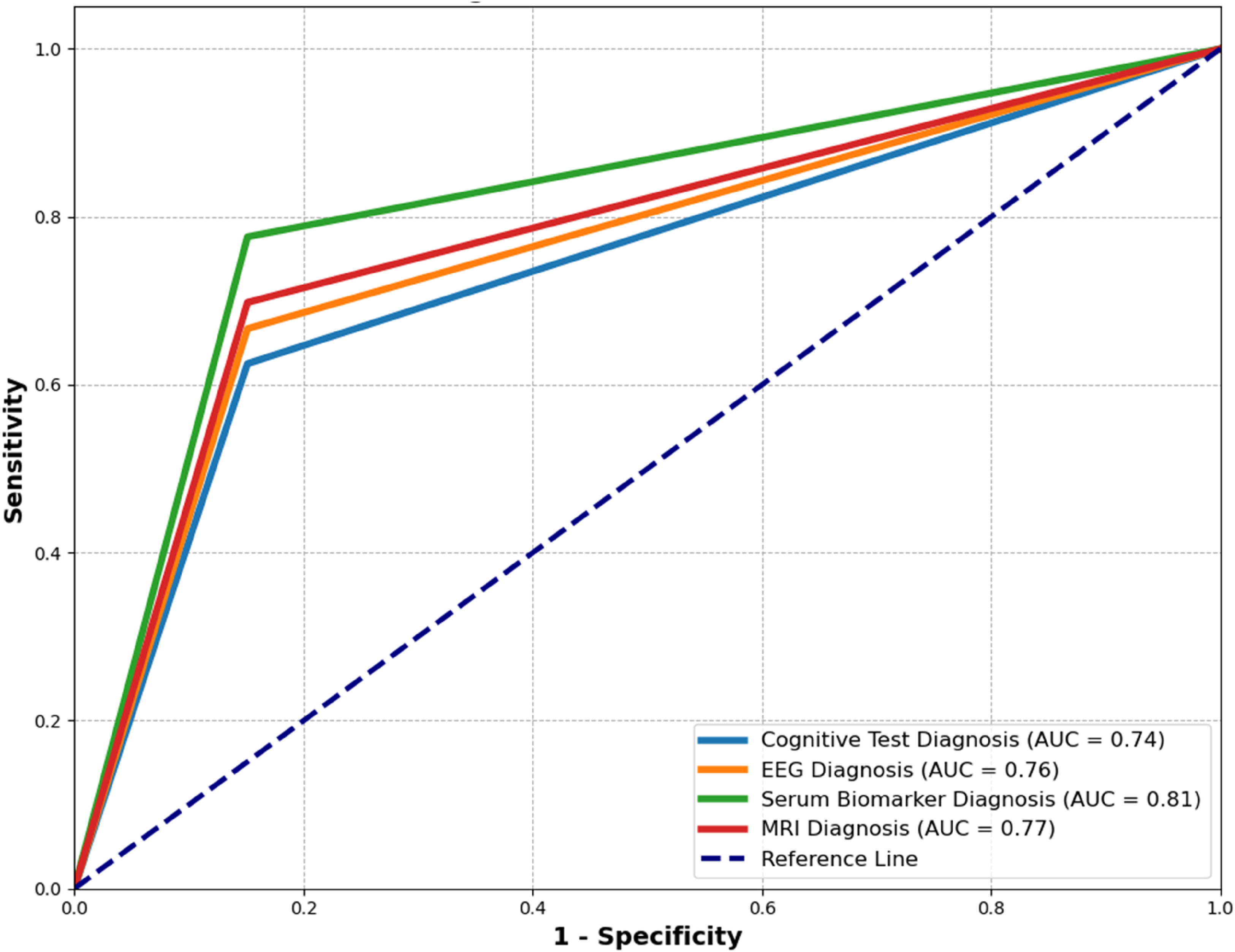
ROC curve for the diagnostic modalities—MRI, EEG, serum biomarkers, and cognitive tests—evaluated against the PET-CT gold standard.
These findings support the use of a multi-modal diagnostic approach for AD, where combining cognitive, biochemical, functional, and structural assessments significantly enhances diagnostic accuracy compared to any single modality alone.
Discussion
This study evaluated the diagnostic accuracy of cognitive tests, serum biomarkers, EEG, and MRI—individually and in combination—against PET-CT findings in the early detection of AD. Our findings support the growing body of literature advocating for a multi-modal diagnostic approach to improve sensitivity and specificity in clinical settings.
In our research, the sensitivity and specificity of cognitive tests were also similar to recent meta-analyses (62.50% and 84.90%, respectively). In a 2023 Bayesian study of the ADNI data set, the MoCA presented a sensitivity of 91.2% with a specificity of 90.1% in detecting AD, whereas, compared to the sensitivity, the MMSE reported almost similar values of sensitivity with a higher specificity of 92.2%. 24 Likewise, the 2022 systematic review results revealed pooled sensitivity and specificity of MMSE as 73 and 83, respectively. 25 These results confirm the usefulness of cognitive tests as easily performed and sensitive screening measures, but the diagnostic sensitivity can be enhanced when administered in conjunction with objective biomarkers.
Serum biomarkers proved to have the highest individual sensitivity in our research (77.60%), as it corresponds to current progress in blood-based diagnostics. A post-2024 NIH-funded study discussed how plasma p-tau217 and the Aβ42/Aβ40 ratio attained diagnostic accuracy in more than 90% contingent upon contrasting with PET and CSF results. 26 Such findings reinforce the ongoing promise of blood biomarkers as a non-invasive, blood-based alternative to the CSF test, especially in early diagnosis.
EEG, which has a sensitivity of 66.67% and specificity of 84.90% in our study, has also become promising in the recent literature. In a 2025 systematic review, EEG was shown to pick up early changes in the functioning of the mind in AD as a result of elevated theta and reduced alpha activity. 27 These electrophysiological changes correlate with ours and make a case for EEG as a relatively inexpensive tool that can help in real-time diagnostics.
MRI, which obtained 69.79% and 84.90% sensitivity and specificity, respectively, in our study, is one of the pillars of structural imaging in AD. A 2024 study utilizing machine learning on MRI characteristics (including hippocampus volume and cortical thickness) found that 95% of the participants could be successfully classified based on the AD diagnosis and normal aging by utilizing the MRI tools. 28 In another review of 2021, the authors stressed that although MRI without other tests is not a reliable method to reveal amyloid pathology, it still helps to find structural atrophy and exclude other dementia-related diseases. 29
The most important result of our work was an improvement in the diagnostic performance with the help of multi-modal combinations. With the addition rule of probability, the combination of serum parameters, cognitive tests, EEG, and MRI provided a sensitivity of 99.15% and a specificity of 99.95%. These findings matched a 2025 systematic review of AI-based multimodal diagnostics, which found that biomarker-enhanced multimodal diagnostics combining imaging and biomarker and cognitive data exposed substantially better classification performance and clinical value. 30 A study published in 2024, which was based on SeaLM and used a Transformer-based model to fuse MRI and PET imaging data, reached an accuracy of 98.19% when classifying people with AD, while healthy people were classified at 99.43%. 31
The former, though, had a sensitivity of only 22.57%, as opposed to that of the latter, whereas the specificity was high. This can be more suited under confirming circumstances when it is necessary to reduce the false positives. A more recently published multimodal study based on longitudinal data alluded to the same trade-off between sensitivity and specificity in fusion models by arguing in favor of diagnostic thresholds set on contextual grounds. 32
Our results are consistent with the existing trend of AD research that significantly incorporates multi-modal, data-driven modalities. Using an assembly of cognitive, biochemical, electrophysiological, and structural information, clinicians will be able to make more appropriate and earlier diagnoses, which will lead to better patient outcomes and allow more specific interventions to be made.
Limitations and practical considerations
In this study, some limitations should be mentioned. First, its cross-sectional nature limits the findings made on predictive validity over time and longitudinal studies will be needed to ascertain whether the multimodal approaches remain diagnostic over the disease course. Second, there might be potential selection bias because subjects were selected by specialty clinics, which might be representative of populations with a higher pretest likelihood of having AD than would be seen in community or primary care environments. Third, the results were not stratified by age, sex, ethnicity, and education, which may affect cognitive tests and biomarker patterns and, in subsequent studies, should be considered to increase generalizability.
Clinically, a multimodal framework may not be equally applicable in primary and specialty care. Brief cognitive screening along with blood-based biomarkers could be used as a viable first approach to the condition in primary care, whereas more detailed protocols, including both MRI and EEG, and confirmatory PET-CT, could be more suitable in the specialty clinics. Lastly, issues of cost, access and equity are important to implementation. Serum biomarkers and cognitive tests are relatively cheap and reproducible in low-resource settings whereas advanced neuroimaging and PET-CT are relatively expensive and limited. It will be necessary to ensure that diagnostic innovations are accessible to all people to avoid the growing disparities in the treatment of AD.
Conclusion
This paper demonstrates that cognitive tests, serum biomarkers, EEG, and MRI each show moderate diagnostic accuracy for early AD (AUCs 0.74–0.81), with serum biomarkers and MRI performing best among individual modalities. None of the tests proved accurate enough to be regarded as superior on their own. Sensitivity and specificity improved substantially (up to 99%) when modalities were combined using the addition rule of probability, highlighting the potential of a multimodal diagnostic approach. However, this approach assumes statistical independence between tests, which may overestimate performance in real-world settings. By contrast, the product rule yielded low sensitivity (22–48%) and moderate specificity (51–72%), making it unsuitable for screening and of limited value for confirmatory diagnosis. Overall, our results suggest that multimodal strategies may enhance early detection of AD, but findings should be interpreted with caution and validated in larger, more diverse cohorts before integration into routine clinical practice.
Footnotes
Acknowledgements
We thank all participants and clinical staff for their support in this study.
Ethical considerations
The study was approved by the Bolan Medical Complex Ethics Committee (Approval No: 1950). All procedures complied with the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants prior to enrollment.
Consent for publication
Participants consented to the publication of anonymized data.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.