
Abstract
Background
Lower childhood socioeconomic status (cSES) has been linked to a higher risk of Alzheimer's disease and related dementia (ADRD). Yet, the mechanisms underlying this association remain unclear.
Objective
This study examined whether poorer health behaviors in adulthood mediate the association between lower cSES and ADRD risk. We further explored whether the mediating effects of health behaviors vary by gender or race/ethnicity.
Methods
Data were drawn from 26,631 participants in the Health and Retirement Study (Mage = 61.18 years). Cox proportional hazard models were used to estimate the association between cSES and ADRD risk, as well as the mediating effects of health behaviors, including smoking, heavy drinking, physical activity, and influenza vaccination.
Results
Lower cSES was associated with a higher risk of ADRD (hazard ratio = 1.06, [1.02, 1.09]). Lower physical activity mediated this association, accounting for 17.1% of the total effect of cSES on ADRD risk. Subgroup analyses revealed that this mediation was consistent across all gender and racial/ethnic groups, except for foreign-born Hispanics. Smoking mediated the association only for men, explaining 4.2% of the total effect.
Conclusions
These findings suggest that lower cSES may be a risk factor for ADRD partially through lower physical activity across most demographic groups. Interventions promoting physical activity in adulthood could help mitigate the adverse effect of low cSES on ADRD risk. Furthermore, smoking prevention programs may be particularly beneficial for men from lower socioeconomic backgrounds.
Introduction
Lower childhood socioeconomic status (cSES) has been linked to a higher risk of Alzheimer's disease and related dementia (ADRD).1–4 However, the specific pathways linking cSES to ADRD risk in later life remain largely elusive. Whalley et al. (2006) applied a life-course perspective to explore pathways from early-life environmental factors to ADRD risk, proposing that poorer health behaviors in adulthood may partly explain the association between lower cSES and higher ADRD risk. 5 Building on this framework, we examined the association between cSES and later-life ADRD risk, focusing on whether this association is mediated by adulthood health behaviors, such as smoking, heavy drinking, physical activity, and influenza vaccination.
Furthermore, there is limited understanding of whether the underlying mechanisms differ by sociodemographic characteristics such as gender or race/ethnicity. Individuals may engage in unhealthy behaviors that are more socially acceptable for their gender: men tend to smoke and consume excessive alcohol; women are more likely to be physically inactive.6,7 Thus, the mechanisms linking cSES and ADRD risk may differ by gender. Furthermore, the health behaviors and cognitive function of racial/ethnic minorities may be more negatively affected by lower cSES than White adults due to additional stressors, such as discrimination.8,9 This study explored whether the mediating role of health behaviors vary by gender and race/ethnicity.
Childhood SES and ADRD risk: health behaviors as underlying mechanisms
cSES is a multidimensional construct that includes factors such as parental education and subjective perceptions of a family's financial status. 10 Research consistently shows that lower cSES is associated with a higher risk of ADRD in later life, even after adjusting for adulthood SES.1,2,4 Notably, Korhonen et al. (2023) found that adulthood SES partly mediated the effect of lower cSES on ADRD risk. 2 This suggests that cSES may independently contribute to ADRD risk in later life, beyond the influence of adulthood SES.
Several mechanisms, such as adulthood cardiovascular health and personality traits, have been found to partially explain the association between cSES and ADRD risk.2,4 Still, the underlying mechanism linking cSES to ADRD risk remains largely unclear. According to a life-course perspective on ADRD onset, 5 poorer health behaviors in adulthood are one mechanism that explains how lower cSES contributes to higher ADRD risk. This perspective suggests that exposure to a risk factor (e.g., lower cSES) may increase the likelihood of subsequent exposure to other risk factors (e.g., poorer health behaviors), which could contribute to a higher risk of disease and potentially ADRD. Studies have found that lower cSES is linked to higher rates of smoking,11,12 heavy drinking, 13 and less physical activity14,15 in adulthood. Given that lower adulthood SES is linked to lower influenza vaccination rates, 16 lower cSES is likely associated with lower rates of influenza vaccination in adulthood as well given the cumulative model set forth by previous research. 5
Poorer health behaviors are well-documented factors that are associated with a higher risk of ADRD. Specifically, smoking has been consistently linked to an increased risk of ADRD. 17 While light-to-moderate alcohol consumption is either associated with a reduced risk of ADRD or unrelated, heavy drinking has been shown to increase the risk of ADRD. 18 In addition, lower levels of physical activity, particularly less engagement in moderate or vigorous physical activity, are associated with a higher risk of ADRD.19,20 Research also suggests that lower rates of influenza vaccination are linked to higher ADRD risk. 21 Together, poorer health behaviors in adulthood may serve as a long-term mechanism that partly explains the association between lower cSES and a higher risk of ADRD in later life.
Gender and racial/ethnic differences in the mediating effects of health behaviors
The underlying mechanisms between cSES and ADRD risk may vary by gender. While sex is a biological construct, gender reflects one's psychosocial identity which is often linked to people's behavior and the protective or risk factors that accompany this identity. 22 In this study, we use women and men to refer to participants’ self-identified gender. Social norms shape expectations for appropriate behavior based on gender. For instance, men are more likely to smoke and drink heavily than women,23,24 while women tend to engage in lower levels of physical activity than men. 7 Therefore, smoking and heavy drinking may be stronger underlying mechanisms (i.e., mediators) for men, while physical activity may be a stronger underlying mechanism for women.
Existing literature, while mixed, suggests some racial and ethnic differences in health behaviors. The prevalence of smoking is generally higher for non-Hispanic White (NHW) adults compared to Black and Hispanic adults. 25 In contrast, heavy drinking is more frequently reported among Hispanic adults compared to Black and NHW adults. 26 Furthermore, racial and ethnic minorities are likely to encounter additional stressors, such as discrimination, 27 which has been linked to a higher likelihood of smoking and heavy drinking.8,28 In addition, lower levels of physical activity and influenza vaccination rates are more consistently reported in adults from Black and Hispanic groups compared to NHW adults.26,29
Given these differences, greater smoking and heavy drinking, along with lower physical activity and vaccination rates, may serve as stronger underlying mechanisms among racial and ethnic minorities than among NHW adults. Furthermore, existing research suggests heterogeneity within Hispanic population based on nativity. Specifically, foreign-born Hispanic adults have lower rates of smoking30,31 and alcohol misuse 32 but engage in less moderate-to-vigorous physical activity 33 compared to U.S.-born Hispanic adults. Based on these differences, we examined whether the mediating effects of health behaviors vary across NHW, Black, U.S.-born Hispanic, and foreign-born Hispanic adults.
The current study
This study examined the association between cSES and ADRD risk, with a particular focus on testing the mediating effects of health behaviors. Specifically, we investigated smoking, heavy drinking, physical activity, and influenza vaccination, as these behaviors have been linked to ADRD risk. We further explored whether the mediating effects of health behaviors vary by gender or race/ethnicity. The following hypotheses were tested:
Methods
Participants
We used the Health and Retirement Study (HRS), a nationally representative and longitudinal survey of U.S. adults over age 50 and their spouses of any age. 34 Since 1992, HRS investigators have collected detailed information on the social, economic, and health characteristics of participants every two years. For the current study, we used data from 11 waves (2000–2020) of the HRS, as consistent cognitive information has been collected for both community-dwelling and nursing home residents since 2000. The HRS is sponsored by the National Institute on Aging (NIA U01AG009740) and is conducted by the University of Michigan. 35 We also used data from the Childhood Family and Childhood Health Aggregated Data, which is affiliated with the HRS and funded by the National Institute on Aging (NIA R01AG051142). 36
Our analytic sample was comprised of adults aged 51 years and older who did not have ADRD at baseline and had at least one follow-up wave of data (see Figure 1). Participants’ baseline wave for this study were between the 2000 and 2018 HRS Core assessments, ensuring that all participants had at least one follow-up wave of data. A total of 28,738 participants met these eligibility criteria for the current study. Of these, we excluded 2107 (7.3%) who had missing data on at least one study variable, primarily the physical activity measure (Nmissing = 1847). Compared to participants with complete data, those with missing data were older, had lower cSES, and were more likely to develop ADRD (ps < 0.001). No significant differences were observed regarding gender or adulthood wealth (ps > 0.28). The final analytic sample included 26,631 participants with complete data.
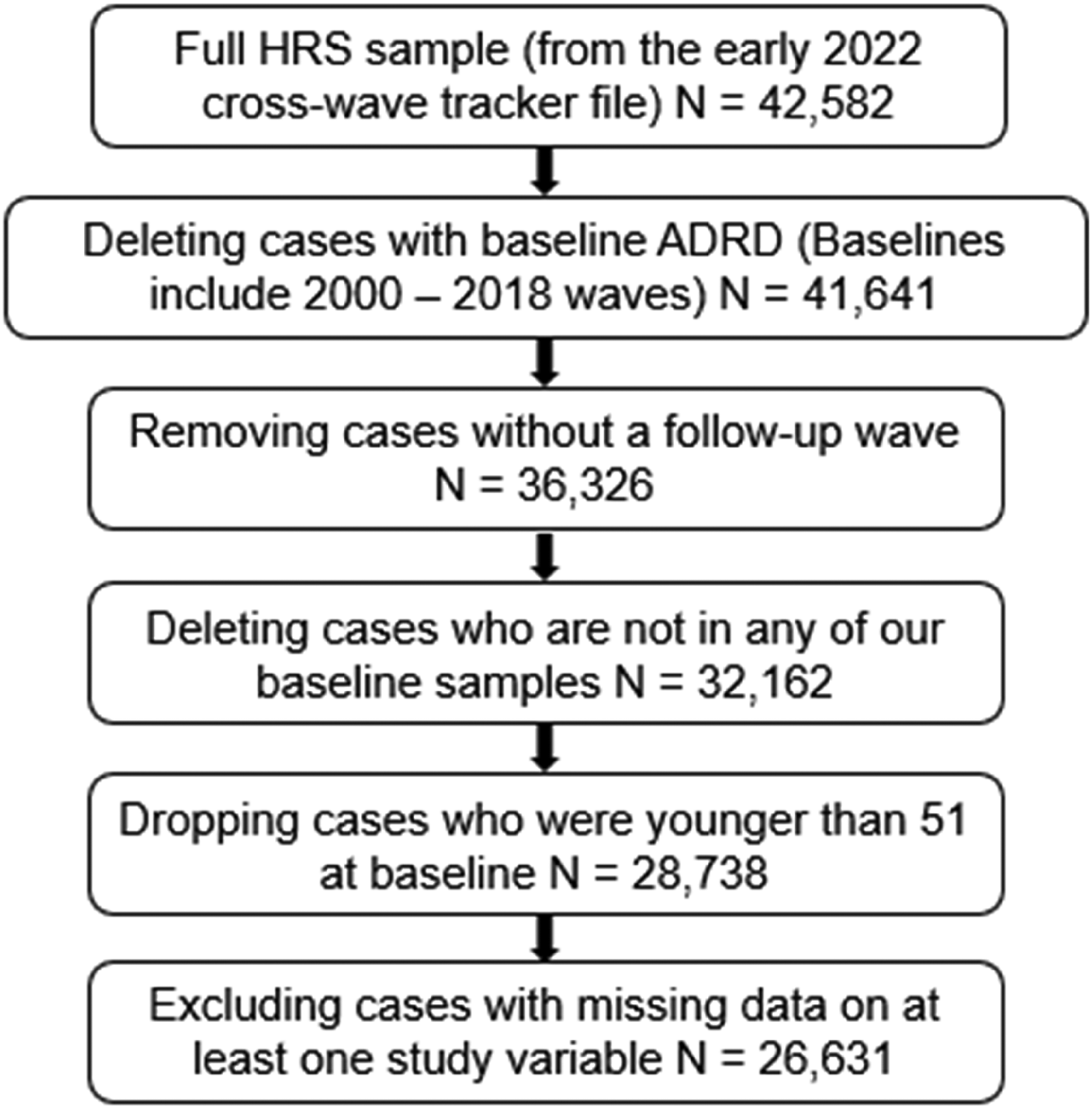
Sampling flowchart of the current study. ADRD: Alzheimer's disease and related dementia.
Measures
Childhood socioeconomic status (cSES)
cSES was assessed using three items: (1) maternal and (2) paternal education levels, and (3) self-rated childhood financial situation. Participants reported the highest grade of school completed by their mother and father, ranging from zero to 17, respectively. These responses were reverse-coded so that higher scores represented lower parental educational attainment. Participants also rated their family's financial situation during childhood using the options “pretty well off financially”, “about average”, “poor”, and “it varied.” Based on the recommendation of previous research, 37 “it varied” was recoded as “about average.” Then, the responses were recoded, with higher scores representing a poorer subjective financial situation (1 = pretty well off financially; 3 = poor). Finally, the three items were normalized for comparability and averaged, with higher scores indicating lower cSES, ranging from 0 to 1 (M = 0.51, SD = 0.21). If a participant had missing data on one or more items, the score was created by averaging the available items.
Alzheimer's disease and related dementia (ADRD)
ADRD status was assessed using the Langa-Weir classification approach, which is widely employed to assess ADRD at the population level. 38 According to this approach, we used a 27-point scale that included immediate word recall (0–10), delayed word recall (0–10), serial subtraction of 7 s (0–5), and backward counting from 20 (0–2). The total score ranged from 0 to 27. Participants who scored from 0 to 6 were classified as having ADRD (as higher scores on these measures corresponded to better cognitive performance).
For participants represented by a proxy, a 11-point scale was developed 38 using the proxy's assessment of the participant's memory from excellent to poor (0–4), the proxy's assessment of whether the participant had limitations in five instrumental activities of daily living including using the phone, managing money, taking a medication, preparing hot meals, and shopping for groceries (0–5), and the survey interviewer's assessment of difficulty in completing the interview due to cognitive limitation (0–2). For participants represented by a proxy, those with scores between 6 and 11 were classified as having ADRD (as higher scores on these measures corresponded to worse cognitive performance).
In this study, ADRD onset was defined as meeting the ADRD classification in two consecutive waves. This approach was adopted to reduce the potential misclassification of ADRD, particularly for participants from underrepresented groups who are more likely to be misclassified as having ADRD. 39 It also prevents inclusion (or exclusion) of participants who may waffle back and forth along the threshold line for the ADRD classification. Time-to-event for ADRD was defined as the period from baseline to the onset of ADRD.
Health behaviors
We assessed four health behaviors: smoking, heavy drinking, physical activity, and influenza vaccination. For participants who developed ADRD during follow-up, we used their responses from waves prior to ADRD onset to avoid the reverse causality, where ADRD might have an effect on health behaviors. Smoking was measured based on whether participants had ever smoked in their lifetime. In each wave of HRS, participants reported whether they had ever smoked more than 100 cigarettes in their life time. Those who answered “yes” at baseline or follow-up assessments were classified as “ever smokers” (1), while those who answered “no” were classified as “never smokers” (0). In this study, 55.7% of participants were ever smokers.
Heavy drinking was assessed based on participants’ heavy drinking status throughout the study period. In each wave of HRS, participants were asked whether they had ever consumed an alcoholic beverage. Those who responded “yes” were then asked how many days per week they consumed alcohol, and how many drinks they consumed on the days they drank in the last three months. We calculated the average weekly alcohol use by multiplying the number of drinking days by the number of alcoholic drinks on those days. According to the National Institute on Alcohol Abuse and Alcoholism (2024), 40 participants were coded as heavy drinkers if they consumed 15 or more drinks per week for men, and drank 8 or more drinks per week for women. Each wave's heavy drinking status (0 = non-drinker or light drinker, 1 = heavy drinker) was averaged, with higher scores indicating more years of heavy drinking during the study period, ranging from 0 to 1 (M = 0.06, SD = 0.19).
Physical activity was measured based on participants’ engagement in vigorous and moderate physical activities throughout the study period. In each wave of HRS, participants were asked how frequently they participated in vigorous activities, such as jogging, swimming, or gym workout, using the following options: “everyday”, “more than one a week”, “once a week”, “one to three times a month”, or “hardly ever or never”. They were also asked how frequently they participated in moderate activities, such as walking at a moderate pace, or cleaning the car, using the same response options. Responses were recoded, with higher scores indicating greater physical activity (1 = hardly or never to 5 = everyday). The responses to vigorous and moderate physical activities at each wave were averaged, with higher scores indicating greater physical activities, ranging from 1 to 5 (M = 2.47, SD = 0.91).
Influenza vaccination was assessed based on participants’ vaccination status throughout the study period. In each wave of HRS, participants were asked whether they had an influenza vaccination since the last survey. The influenza vaccination status (0 = no, 1 = yes) at each wave was averaged, with higher scores indicating more consistent influenza vaccinations during the study period, ranging from 0 to 1 (M = 0.63, SD = 0.40).
Covariates
We adjusted for several sociodemographic characteristics associated with ADRD risk: age at baseline (in years), self-identified gender (0 = men, 1 = women), race/ethnicity, education, and wealth at baseline. Participants reported their race as White/Caucasian, Black/African American, or Other. They also indicated whether they identified as Hispanic/Latino. We created dummy variables for Non-Hispanic Black (hereafter referred to as Black), Hispanic, and other race category, with NHW as the reference category. Hispanic participants were classified as U.S.-born if they reported being born in one of the 50 U.S. states, and as foreign-born if they were born outside the United States, including its territories. Education was measured as the total number of years of schooling completed (0–17). Wealth was calculated as the sum of all assets, including real estates, vehicles, and savings, minus debt.
Statistical analyses
Cox proportional hazard (CPH) models were used to examine the association between cSES and the risk of developing ADRD (Hypothesis 1). Since the analytic sample was restricted to participants without ADRD at baseline, the estimates reflect the effects of cSES on the onset of ADRD during follow-up. The assumptions for the CPH models were validated using Schoenfeld's residual test. 41 Analyses included both unadjusted and adjusted models (including sociodemographic covariates), implemented using the survival R package. 42 In all models, continuous variables were standardized to facilitate interpretation.
The mediating effects of health behaviors on the association between cSES and ADRD onset (Hypothesis 2) were estimated with a counterfactual approach. 43 Specifically, this approach allows for the decomposition of a total effect into direct and indirect effects, as well as the percentage of the total effect mediated by the indirect effect, even in nonlinear models such as CPH models. Specifically, continuous mediators (heavy drinking, physical activity, and influenza vaccination) were modeled via a linear regression, while the binary mediator (smoking status) were modeled via a logistic regression. All models accounted for the covariates listed above. These mediation analyses were conducted using the regmedint R package. 44
Subgroup analyses were conducted to examine gender (Hypothesis 3) and racial/ethnic differences (Hypothesis 4) in the mediating effects of health behaviors, with subgroups (e.g., men or women) specified using the regmedint package.44,45 Survey weights were not applied due to the complexity of the modeling approach and limitations of the regmedint package.
Results
Participant characteristics
Descriptive statistics for the study participants are presented in Table 1. Approximately 16.4% of participants developed ADRD over the follow-up period. Those who developed ADRD tended to have lower cSES. In addition, participants who developed ADRD, on average, reported lower physical activity, more heavy drinking, and higher rates of influenza vaccination. There was no significant difference in the percentage of individuals who had ever smoked between those who developed ADRD and those who did not. Further, those who developed ADRD were also more likely to be women, older, less educated, and to identify as Black or Hispanic.
Characteristics of participants by ADRD onset (N = 26,631).
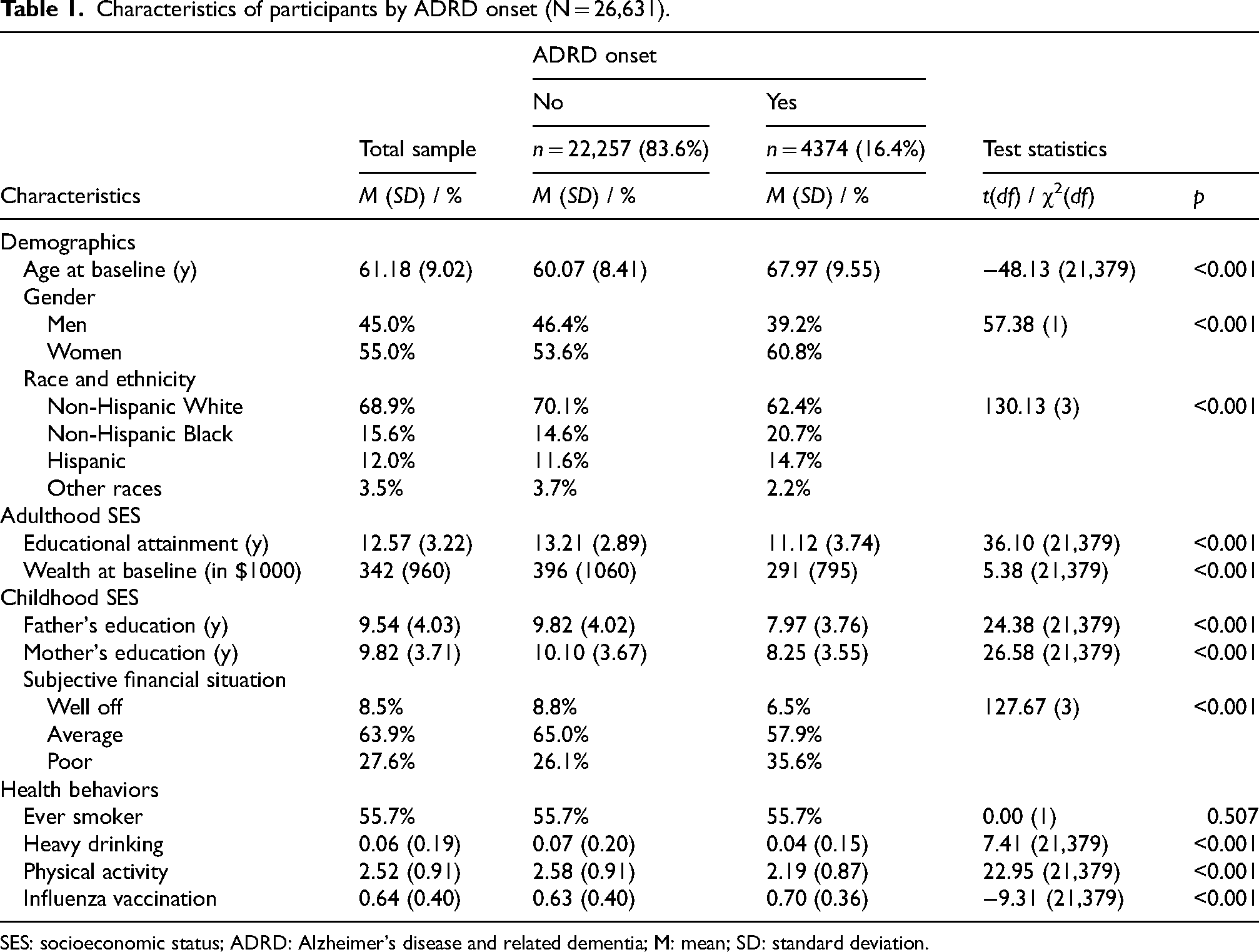
SES: socioeconomic status; ADRD: Alzheimer's disease and related dementia; M: mean; SD: standard deviation.
Women were more likely to develop ADRD and report lower cSES than men (see Supplemental Table 1). Women reported less smoking, less heavy drinking, and higher rates of influenza vaccination, but engaged in less physical activity. By race/ethnicity, Black adults were most likely to develop ADRD, followed by Hispanic, NHW, and other racial/ethnic groups (see Supplemental Table 2). Black and Hispanic adults reported lower cSES compared to NHW adults. NHW adults were most likely to smoke, engage in heavy drinking, and be vaccinated for influenza than other groups. The “other” racial/ethnic group reported the highest levels of physical activity, while Black adults reported the lowest.
The association between childhood SES on ADRD risk
Results from CPH analyses examining the association between cSES and ADRD risk are presented in Table 2. In both unadjusted and adjusted models, lower cSES is associated with a higher risk of developing ADRD. In the unadjusted model, lower cSES was associated with a 47% higher risk of developing ADRD (Model 1; HR = 1.47 [1.44–1.51, p < 0.001). After adjusting for sociodemographic covariates, including adulthood SES (i.e., education and wealth), lower cSES was associated with a 6% higher risk of ADRD (Model 2; HR = 1.06 [1.02–1.09], p = 0.001).
Cox proportional hazard models estimating the association between childhood SES and ADRD risk.
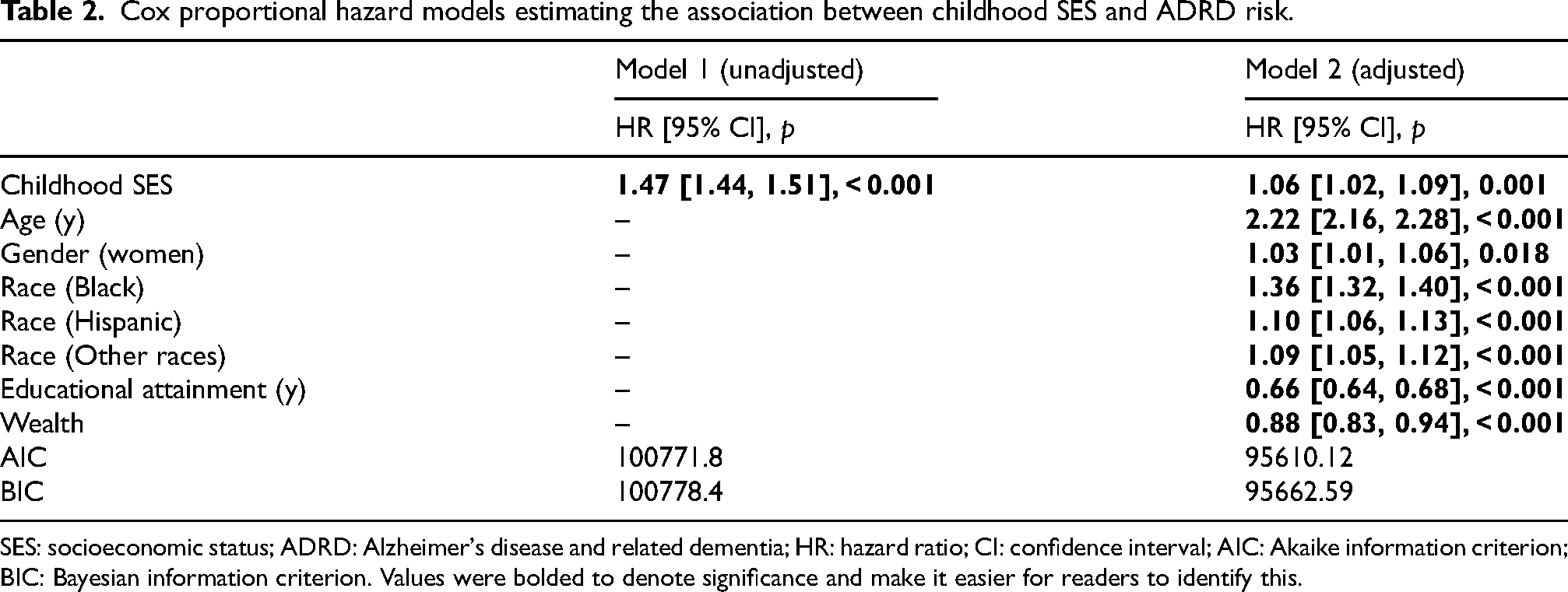
SES: socioeconomic status; ADRD: Alzheimer's disease and related dementia; HR: hazard ratio; CI: confidence interval; AIC: Akaike information criterion; BIC: Bayesian information criterion. Values were bolded to denote significance and make it easier for readers to identify this.
The mediating effects of health behaviors
As presented in Table 3, physical activity significantly mediated the association between cSES and ADRD risk, accounting for 17.1% of the total effect of cSES on ADRD risk (HR = 1.01 [1.01, 1.01], p < 0.001). As illustrated in Figure 2, lower cSES was associated with less physical activity (β = −0.06, p < 0.001). More physical activity was associated with a lower risk of developing ADRD (HR = 0.87 [0.84, 0.91], p < 0.001), suggesting that less physical activity is linked to a higher ADRD risk. The direct effect of cSES on ADRD remained significant (HR = 1.06 [1.02, 1.10], p = 0.004), indicating that physical activity partially mediated the association between cSES and ADRD risk.
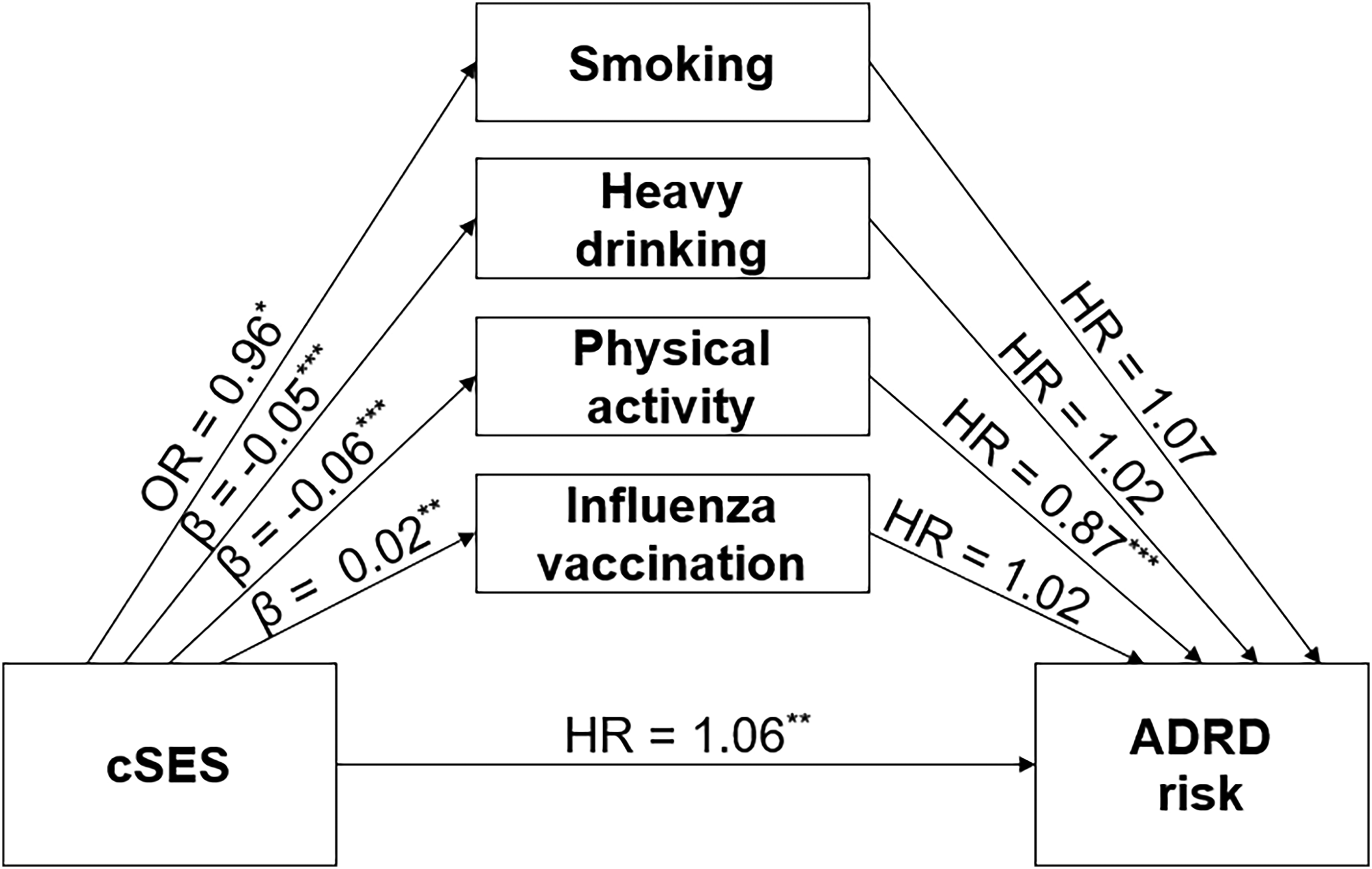
Mediation model path diagram for childhood SES, health behaviors, and ADRD risk. cSES: childhood socioeconomic status; ADRD: Alzheimer's disease and related dementia; OR: odds ratio; HR: hazard ratio. *p < 0.01; **p < 0.05; ***p < 0.001.
Mediating effects of health behaviors on the association between childhood SES and ADRD risk.
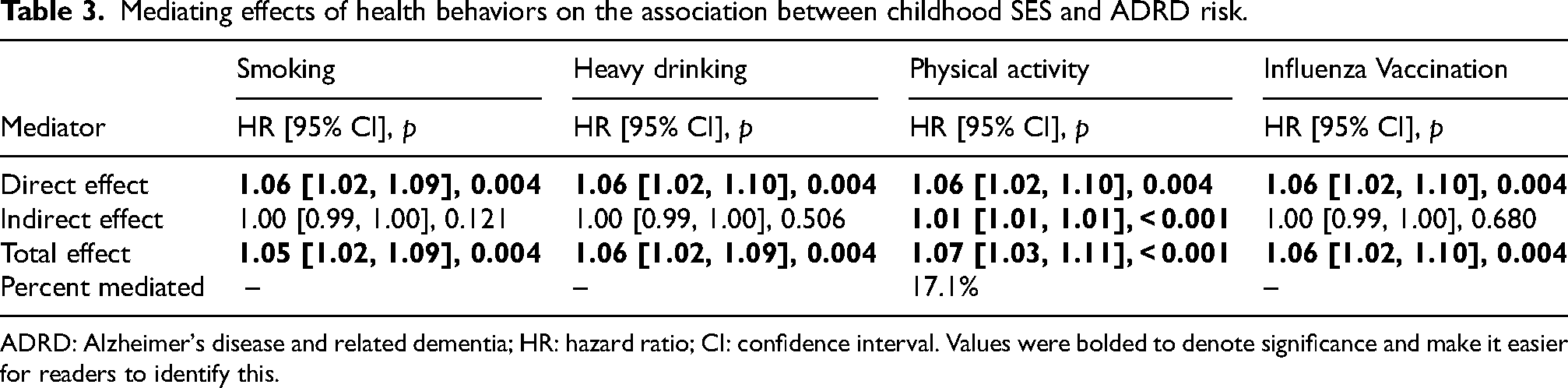
ADRD: Alzheimer's disease and related dementia; HR: hazard ratio; CI: confidence interval. Values were bolded to denote significance and make it easier for readers to identify this.
There were no significant mediating effects of smoking, heavy drinking, or influenza vaccination on the association between cSES and ADRD risk (Table 3; ps > 0.120). As presented in Figure 2, lower cSES was associated with the lower odds of smoking (OR = 0.96, p = 0.020), less heavy drinking (β = −0.05, p < 0.001), and greater influenza vaccination (β = 0.02, p = 0.003). However, none of these health behaviors–smoking, heavy drinking, and influenza vaccination–were associated with ADRD risk (ps > 0.05).
Gender and racial/ethnic differences in the mediating effects of health behaviors
As shown in Table 4, we conducted subgroup analyses to examine whether the mediating effects of health behaviors differed by gender or race/ethnicity. Among both men and women, lower cSES was associated with a higher risk of ADRD through less physical activity (ps < 0.001), accounting for 11.2% of the effect in men and 21.8% in women. Similarly, lower cSES was linked to a higher risk of ADRD through lower levels of physical activity across all racial/ethnic groups, except for foreign-born Hispanics. Specifically, lower physical activity accounted for 26.5% of the cSES-ADRD association in NHW adults, 19.2% in Black adults, 13.2% in U.S.-born Hispanic adults, and 17.5% in adults from the “other” racial/ethnic groups. In contrast, among foreign-born Hispanics, lower cSES was directly associated with a higher risk of ADRD (HR = 1.06 [1.02, 1.10], p = 0.004) but indirectly associated with a lower risk of ADRD via more physical activity (HR = 0.99 [0.98, 0.99], p < 0.001).
Mediating effects of health behaviors on the association between childhood SES and ADRD risk by subgroups.
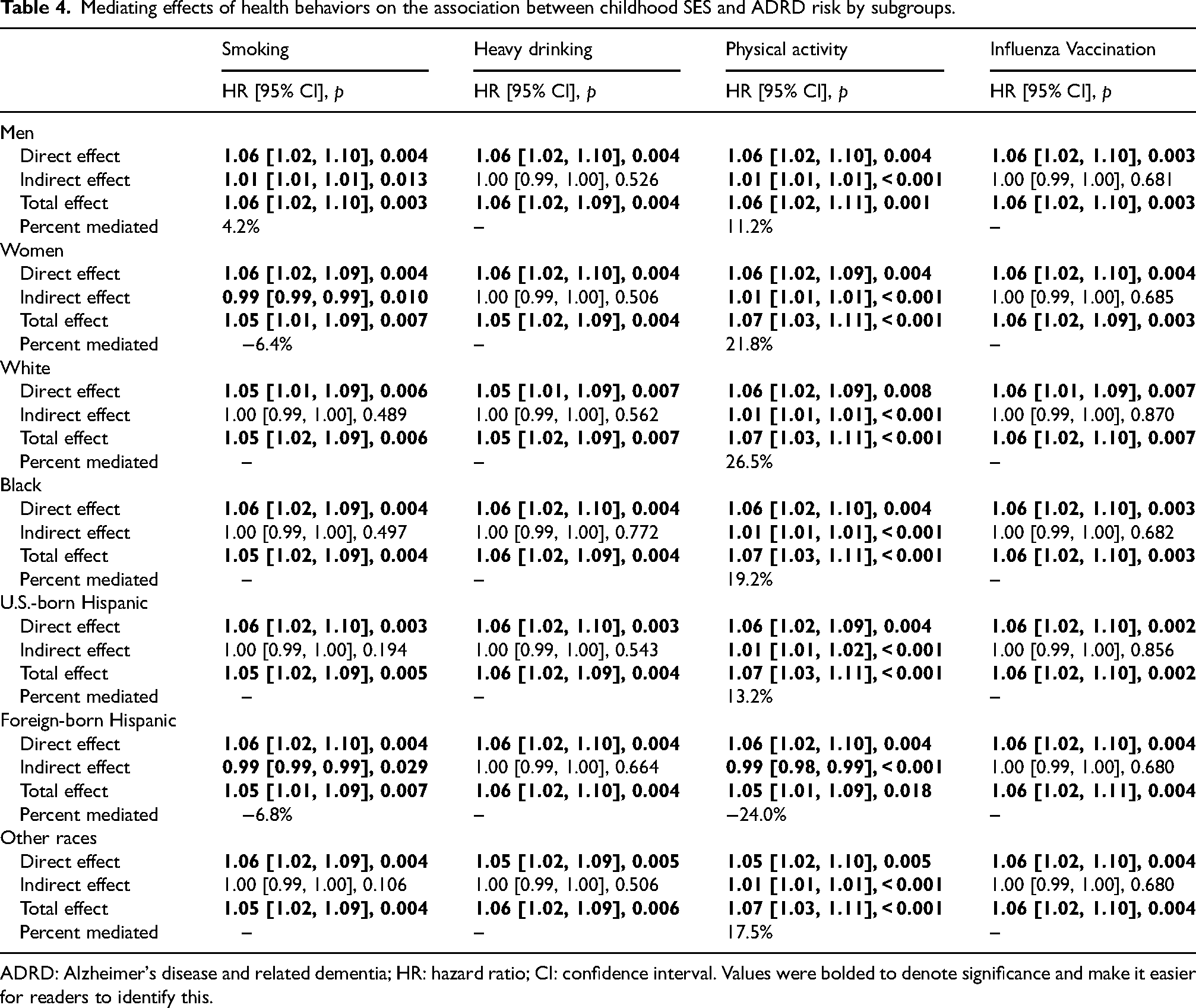
ADRD: Alzheimer's disease and related dementia; HR: hazard ratio; CI: confidence interval. Values were bolded to denote significance and make it easier for readers to identify this.
Subgroup analyses also revealed that smoking mediated the association between cSES and ADRD among men (HR = 1.01 [1.01, 1.01], p = 0.013), accounting for 4.2% of the total effect of cSES on ADRD risk. To our surprise, among women, lower cSES was directly associated with a higher risk of ADRD (HR = 1.06 [1.02, 1.09, p = 0.004), but indirectly associated with a lower risk of ADRD through lower odds of smoking (HR = 0.99 [0.99, 0.99], p = 0.010). A similar pattern emerged among foreign-born Hispanics: lower cSES was directly associated with a higher risk of ADRD (HR = 1.06 [1.02, 1.10], p = 0.004) but indirectly associated with a lower risk of ADRD through lower odds of smoking (HR = 0.99 [0.99, 0.99], p = 0.029).
Heavy drinking and influenza vaccination did not mediate the association between cSES and ADRD risk across gender or racial/ethnic groups (ps > 0.505).
Discussion
This study examined the association between cSES and the risk of ADRD in later life, as well as the mediating role of health behaviors in adulthood. We further explored whether the mediating effect of health behaviors varied by demographic characteristics, such as gender and race/ethnicity. Our findings indicate that lower cSES is associated with a higher risk of developing ADRD, even after adjusting for adulthood SES. These findings align with previous research linking lower SES in childhood to a greater risk of ADRD in later life.1–4 By demonstrating that the relationship between cSES and ADRD risk persists independent of adulthood SES, this study further strengthens the evidence that early-life socioeconomic conditions may have a lasting impact on cognitive health in later life.
Furthermore, our study extends prior research by showing that lower cSES is associated with a higher risk of ADRD in later life, partially through lower levels of physical activity during adulthood. This pattern holds across all genders and racial/ethnic groups, except for foreign-born Hispanics. Across all groups, less physical activity in adulthood was linked to a higher risk of ADRD, consistent with previous findings.19,20 On the other hand, the association between cSES and physical activity differed for foreign-born Hispanics. Among most racial/ethnic groups, lower cSES was associated with less physical activity in adulthood, aligning with existing research.14,15 Individuals from lower childhood socioeconomic backgrounds may have had fewer opportunities to live in neighborhoods with public parks or participate in organized sports in their childhood.46,47 This restricted access could lead to less physical activity in both childhood and subsequently adulthood, in turn conferring a greater risk of ADRD.
In contrast, among foreign-born Hispanics, lower cSES was associated with more physical activity in adulthood. A previous study reported that foreign-born Hispanics tend to work in physically demanding occupations, such as agriculture or construction. 48 Given this, foreign-born Hispanics with lower cSES are likely to engage in higher levels of non-leisure time physical activity. Since this study combined both non-leisure and leisure time physical activity into a single measure, greater non-leisure activity may explain the observed association between lower cSES and higher physical activity in adulthood among foreign-born Hispanics.
We also observed a gender difference in the mediating effect of smoking. Specifically, a higher odd of smoking partially mediated the adverse effect of lower cSES on ADRD risk only among men. In contrast, among women, lower cSES was associated with lower odds of smoking. This finding aligns with previous studies reporting that poorer neighborhoods increased the smoking of men but not of women, 49 and more for men than for women 50 —both suggesting that smoking might be a particularly salient pathway leading to ADRD for men from lower cSES backgrounds. This may be due to the social disapproval of smoking among women. 23 In addition, women from lower cSES may have limited financial resources to purchase cigarettes. 51
A similar pattern was observed among foreign-born Hispanics, such that lower cSES was linked to a lower odd of smoking. Previous research found that foreign-born Hispanics are less socially accepting of smoking than U.S.-born Hispanics. 52 Social norms discouraging smoking, along with financial limitations, may contribute to lower odds of smoking among foreign-born Hispanics from lower cSES backgrounds. Nonetheless, additional evidence is needed to fully establish these gender and nativity status differences in the mediating effect of smoking in the cSES-ADRD association.
Neither heavy drinking nor influenza vaccinations significantly mediated the effect of cSES on ADRD risk in this study. Contrary to our predictions, lower cSES was associated with less heavy drinking and higher rates of influenza vaccination. This finding appears to contradict a previous study of middle-aged men, which reported that lower cSES is associated with higher odds of binge drinking. 13 It is worth noting, however, that lower socioeconomic status is linked to a reduced risk of heavy drinking in women 53 and substance use tends to decline across the lifespan, particularly in older adulthood. 54 Thus, this discrepancy may be due to our inclusion of both men and women in the analysis and our exclusive focus on older adults.
Overall, the current findings suggest that lower cSES is associated with a higher risk of developing ADRD in later life, partially through physical activity, across all gender and racial/ethnic groups, except for foreign-born Hispanics. This indicates that promoting physical activity in adulthood could help mitigate some of the adverse effects of low cSES on ADRD risk across most demographic groups. Therefore, interventions designed to promote physical activity may be particularly beneficial for adults from low cSES backgrounds. For instance, behavioral interventions that involve goal setting and self-monitoring have been shown to produce long-term changes in physical activities among older adults. 55 In addition, our findings suggest that smoking prevention programs could further help reduce ADRD risk among men from lower cSES backgrounds. Finally, our findings on the differences in the mediating effects of health behaviors between U.S.-born and foreign-born Hispanics add to the growing evidence of heterogeneity within the Hispanic population. These results highlight the need for future research to consider both race/ethnicity and nativity when examining socioeconomic conditions, health behaviors, and cognitive health in later life.
Strengths and limitations
This study has several strengths. First, we used a large national sample of older adults and conducted mediated CPH analyses, which are well-suited for estimating the mediating effects of health behaviors on the association between cSES and ADRD risk. Second, the present study contributes to our better understanding of the mechanisms linking cSES to ADRD risk. Our findings indicate that less physical activity mediates the association for most demographic groups, suggesting the need for physical activity intervention for individuals from lower socioeconomic backgrounds. Lastly, to our knowledge, this is the first study to explore potential gender and racial/ethnic differences in the mechanisms underlying the cSES-ADRD association. Our results suggest that lower cSES may have a lasting impact on ADRD risk, both directly and indirectly through less physical activity in adulthood, across demographic groups. In addition, smoking was found to mediate the cSES-ADRD association only among men.
Nevertheless, we acknowledge several limitations in this study. First, our analyses were restricted to health behaviors in adulthood, particularly midlife and older adulthood. Unfortunately, complete data on such behaviors in childhood, adolescence, and young adulthood were not available, except for lifetime smoking status. Future research would benefit from incorporating measures of health behaviors across these earlier and later life stages, which may also play an important role in explaining how cSES contributes to ADRD risk in later life. Second, ADRD risk was determined based on cognitive tests and proxy reports rather than clinical diagnoses in the current study. Previous research using the HRS has shown that cognitive tests correctly classify 88% of participants, and proxy assessments classify 75% correctly, in determining whether participants have ADRD. 56 We adopted a conservative classification approach by requiring that a participant's cognitive performance fall below the threshold for two consecutive waves in order to reduce the likelihood of misclassification of ADRD status. However, some potential for misclassification remains. Replicating these findings using clinical diagnostic criteria for ADRD would be valuable.
Conclusions
Findings from the current study suggest that lower cSES may be a risk factor for ADRD in later life. This study highlights the mediating role of physical activity in the association between cSES and ADRD risk. Specifically, lower physical activity in adulthood mediated the association between lower cSES and higher ADRD risk across all gender and racial/ethnic groups, except for foreign-born Hispanics. These results suggest that interventions aimed at increasing physical activity may help reduce ADRD risk among most adults from low socioeconomic backgrounds. Furthermore, given that smoking may serve as an additional mechanism linking cSES and ADRD risk in men, smoking prevention programs could provide benefits for men from lower socioeconomic backgrounds.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251394317 - Supplemental material for Health behavior mechanisms linking childhood socioeconomic status to Alzheimer's disease and related dementia risk: Exploring gender and racial/ethnic differences
Supplemental material, sj-docx-1-alz-10.1177_13872877251394317 for Health behavior mechanisms linking childhood socioeconomic status to Alzheimer's disease and related dementia risk: Exploring gender and racial/ethnic differences by Suyoung Nah, Carmen JW Chek, Ana Montoya, Audrey Duarte, Lindsay H Ryan and William J Chopik in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
This study used data from the HRS and the Childhood Family and Childhood Health Aggregated Data, which is affiliated with the HRS. All research protocols for these contributing studies received ethical approval from the University of Michigan Institutional Review Board.
Consent to participate
Prior to each HRS interview, participants were provided with a written informed consent information document. At the start of each interview, all participants were read a confidentiality statement, and gave oral consent by agreeing to participate.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The HRS is sponsored by the National Institute on Aging (NIA U01AG009740) and is conducted by the University of Michigan. The Childhood Family and Childhood Health Aggregated Data is affiliated with the HRS and is funded by the National Institute on Aging (NIA R01AG051142). Also, this work was supported by Kyungpook National University Research Fund, 2025.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.