
Abstract
Background
Subjective cognitive complaints (SCC) have been identified as potentially prodromal to dementia and Alzheimer's disease but research in Latin American populations is lacking.
Objective
To analyze sociodemographic and clinical factors associated with incidence of SCC and cognitive decline in Chile.
Methods
A prospective population-based study in a central-south county of Chile: the MAUCO cohort. We included adults (38–74 years) with a SCC questionnaire and Mini-Mental State Examination (MMSE) test at baseline and follow-up, and normal baseline cognitive assessments. Multivariate Cox regression was used to assess associations between sociodemographic, clinical factors and incidence of SCC and cognitive decline.
Results
2136 participants had cognitive assessments at baseline and follow-up. Average age was 56 years (SD 9.13), 76% female, 25% had <6 years of education. Mean follow-up was 5.0 (SD 0.64) years. Among 1504 participants without baseline SCC, 254 (16.8%) reported SCC at follow-up. Older age (HR 1.02; 95% CI 1.01–1.03), use of benzodiazepines (HR 2.14; 95% CI 1.27–3.61), antidepressants (HR 1.88; 95% CI 1.07–3.30) or depressive symptoms (HR 1.60; 95% CI 1.19–2.15) were associated to SCC incidence. Of 1646 with a normal baseline MMSE, 208 (12.6%) developed cognitive decline. The number of medications (HR 1.11; 95% CI 1.03–1.20), and baseline SCC (HR 1.40; 95% CI 1.05–1.88) were associated with cognitive decline.
Conclusions
Use of benzodiazepines and antidepressants were the main factors associated with SCC, while SCC and MMSE score were the strongest predictors of cognitive decline. Both should be used to target preventive interventions.
Keywords
Introduction
Globally, over 51 million people live with dementia, 1 a number expected to rise by 166% by 2050. 2 Dementia is predicted to be among the 10 leading causes of disability-adjusted life years (DALYs) in 2050, 3 and yet no curative treatment exists. Dementia illness trajectory involves gradual cognitive decline, ranging from mild complaints to severe symptoms that impair independence and lead to death. 4 While many modifiable risk factors have been consistently reported, providing evidence about dementia prevention, 5 identifying early stages of the disease is key to develop interventions aiming at slowing down progression.
Subjective cognitive complaints (SCC), defined as a self-experienced worsening of cognitive capacities, independent of performance on cognitive tests, 6 represent an opportunity for early interventions.6,7 People with SCC are 2 times more likely to develop dementia than those without, and 19.8% progress to some level of cognitive decline in 10 years.7,8 Progression risk factors include older age onset, low education, depression, anxiety, smoking, impaired daily living activities, stable and informant-reported complaints.8,9 However, most of this evidence comes from Europe, Asia and North America, with limited studies from Latin America and few studies have investigated factors associated to the development of SCC in older adults.10,11
Chile is in an advanced demographic transition stage, 12 with an estimated prevalence of dementia around 0.93%, which increases to 13.13% among people 75 years and older. 13 By 2050, this prevalence is expected to double, 2 making dementia the sixth cause of DALYs in Chile. 14 Understanding factors associated with the progression to SCC and cognitive decline in this population is crucial. The aim of this study was to analyze the sociodemographic and clinical factors associated with progression of SCC and cognitive decline and the effect of age in the MAUCO cohort, a semirural population in Central Chile.
Methods
Study design and data sources
This is a population-based prospective cohort study in Molina, a semirural city located in the central-south region in Chile: the MAUCO cohort. 15 MAUCO participants were recruited between 2014 and 2019 using household census sampling. Adults aged 38 to 74 years old, living in Molina were included.15,16 Self-reported sociodemographic, health status, lifestyle, psychosocial and cognitive symptoms were collected at baseline, along with biometric measurements and laboratory tests. More information about the MAUCO cohort and participants’ characteristics can be found elsewhere.15,16
Population
This analysis included all participants in the MAUCO cohort with a cognitive test available at baseline and follow-up, and no SCC or cognitive impairment at baseline.
Assessment of subjective cognitive complaints and cognitive impairment
Participants completed a Mini-Mental State Examination (MMSE) test and a SCC questionnaire at baseline and follow-up. Questionnaires were applied by nurse technicians trained by an expert psychiatrist.
The MMSE test is widely used to assess cognitive function and as a screening test for cognitive impairment. It comprises assessments of seven cognitive domains, scores range from 0 to 30, 17 and has been validated in the Chilean population. 18 As the MMSE test score is highly affected by educational level, 19 we used three different cut-off points by education to define cognitive impairment (<=22 for less than 5 years; <=23 between 6 and 11 years and <=24 for more than 12 years of education), based on Kochhann study. 20 We excluded participants with less than two completed MMSE subsections at baseline or follow-up. Participants with a missing value on one of the MMSE subsections but a total score above the cut-off point were classified as with no cognitive impairment.
SCC were assessed through three questions: “Does your memory fail frequently?, “Do you notice being slower to think, plan or solve problems?”, “Do you have problems paying attention?”. Participants who answered at least one of these questions with “yes” were considered as having SCC. 21
Outcomes
The two outcomes used in this study were incidence of: (1) subjective cognitive complaint and (2) cognitive decline. Incidence of subjective cognitive complaint was defined as a participant without cognitive complaints at baseline who answered “yes” to any of the three questions at the follow-up. Incident Cognitive decline was defined as a cognitive impairment at follow-up based on the MMSE score cut-off point used, in subjects with a normal MMSE test score at baseline. Both outcomes were analyzed separately.
Sociodemographic factors
We included age, sex, marital status, years of education and income at baseline. Age (<60 and >=60 years old) and education (<6; 6–8, > 8 years) were categorized only for descriptive purposes but analyzed as continuous variable. Monthly earnings in Chilean pesos were categorized by terciles and then converted to American dollars and inflated to 2023.
Health status, comorbidities, and behavioral factors
Self-reported health status was assessed using the question ´Would you say your health is excellent, good, regular or bad?´, and was categorized as excellent-good and regular-bad. We used the questions ´Has any specialist advised you to use hearing aids?´ and ´How do you assess your vision?´ to identify participants with hearing and visual problems.
Medicines reported by participants at the time of the baseline interview were converted to Anatomical Therapeutic Chemical (ATC) codes by a trained pharmacist. We counted the number of unique ATC codes reported for each participant, after excluding homeopathic medicines and wrong codes. We identified participants who used benzodiazepines through ATC codes N05B, N05CD, N05CE, N05CF, N03AE01, and N05AH.
Self-reported lifestyle behaviors were extracted from the baseline questionnaire. Smoking behavior was categorized as current, former, or never smoked. Alcohol consumption was assessed through an adapted version of the AUDIT questionnaire, 22 and people were classified as having a risky alcohol intake behavior if they drank >20 g for women or >30 g for men of alcohol per week. 15 Physical activity was assessed through the question ´In the last month, did you play sports or do physical activity outside of your work schedule, for 30 min or more at a time?´ and answers were classified as ´low physical activitý if less than three times a week of exercise was reported. 15
Grip strength was measured in kilograms using a dynamometer (Takei Physical Fitness Test). We recorded the average grip strength of tree measures for the dominant hand and categorized the level of grip strength as low for values <27 kg in men and <16 kg in women.23–25
We used the self-applicable Mediterranean Dietary Index (IDM-Chile), 26 to evaluate the adherence to a Mediterranean diet. The IDM-Chile score was categorized as high (14–9), medium (8.5–5) and low (<5).26–28
Cardiovascular risk factors
Cardiovascular risk factors were assessed through self-report, biometrics and laboratory results. People with hypertension were identified through self-reported diagnosis or antihypertensive medication use, or an average blood pressure >=140/90 mmHg at baseline. People with diabetes mellitus were identified through self-reported diagnosis or hypoglycemic drug use, a blood glucose >=126 mg/dl, or a glycated hemoglobin >=6.5%. People with dyslipidemia were identified through self-report diagnosis or self-report lipid-lowering drug use, a total cholesterol level >=200 mg/dL, LDL cholesterol >=130 mg/dL, a triglyceride >=150 mg/dL or HDL cholesterol <40 mg/dL. Body mass index (BMI) was calculated from height and weight measurements taken at baseline and classified as normal (BMI <25), overweight (BMI 25 to 29), and obese (BMI >30).
Depression symptoms
The Patient Health Questionnaire (PHQ-2), a validated brief version of the PHQ-9 for early detection of depressive disorders, was applied at baseline. 29 We used the recommended cut-off point of >=3 in the PHQ-2 score to define people at risk of depression disorders. 30
Hospital admissions
We calculated the number of hospital admissions (except pregnancy-related admissions) before the last cognitive assessment identified in hospital records from all public hospitals in the region and available for all MAUCO participants since baseline and updated until January 2024.
Analysis
The probability of progression of subjective cognitive complaint and cognitive decline was analyzed using Kaplan–Meier estimation. A Kaplan-Meier curve was also used to assess the risk of cognitive decline by group of age (<60 and >=60 years old) and SCC at baseline.
Univariate and multivariate Cox proportional hazards regression models were fit to assess the association between sociodemographic, clinical factors and progression of SCC and cognitive decline separately. The follow-up started from the date when baseline data was collected and ended on the date the follow-up cognitive test was performed. We tested the Proportional Hazards assumptions using the function cox.zph that correlates the corresponding set of scaled Schoenfeld residuals with time. Results from this analysis are available in Supplemental Tables 2 and 3. As some co-variables did not satisfy the proportional hazard assumption, a Cox model with time-dependent covariables was fitted using the tt command from the survival package in R based on Zhang et al. (2018). 31 To understand the effect of age, we explored interactions between covariables and age at baseline. The variables to be included in the models were selected as follows: (1) first we fitted a univariate model for each independent variable (univariate model), (2) then we fitted a model for each independent variable adjusted by age, sex, marital status and level of education (model 1); (3) then we fitted a model including co-variables based on the literature, and considering those statistically significantly associated with the outcome (p < 0.05) in model 1 (model 2).
As both subjective cognitive complaint questions and items of the MMSE test had missing values, we performed Multiple imputation with Predictive Mean Matching and 50 imputed datasets using the mice package in R. We also used the Multiple imputation models for missing values in covariates.
To better describe the effect of age on cognitive decline, we performed a subgroup analysis stratifying model 2 by group of age (<60 years old and >=60 years old). We ran model 2 for the variables without imputation to understand the effect of Multiple imputations of missing values. As the use of benzodiazepines and antidepressants might be correlated with depressive symptoms, we performed a sensitivity analysis of model 2, excluding participants with depressive symptoms at baseline. All analyses were performed with RStudio.
Results
Sample characteristics
Of all participants in the MAUCO cohort, 2136 had a cognitive assessment at baseline and follow-up. Among them, 622 had subjective complaints at baseline and therefore were not included in the final analysis, and 10 participants had a missing value in one of the three SCC questions. 357 had a cognitive impairment at baseline and were not included in the final analysis and 133 had a missing value in the baseline MMSE and those values were imputed in the final analysis. Figure 1 describes how each sample for the final analysis was derived and Supplemental Table 1 characterizes participants' SCC and impairment assessments at baseline and follow-up.
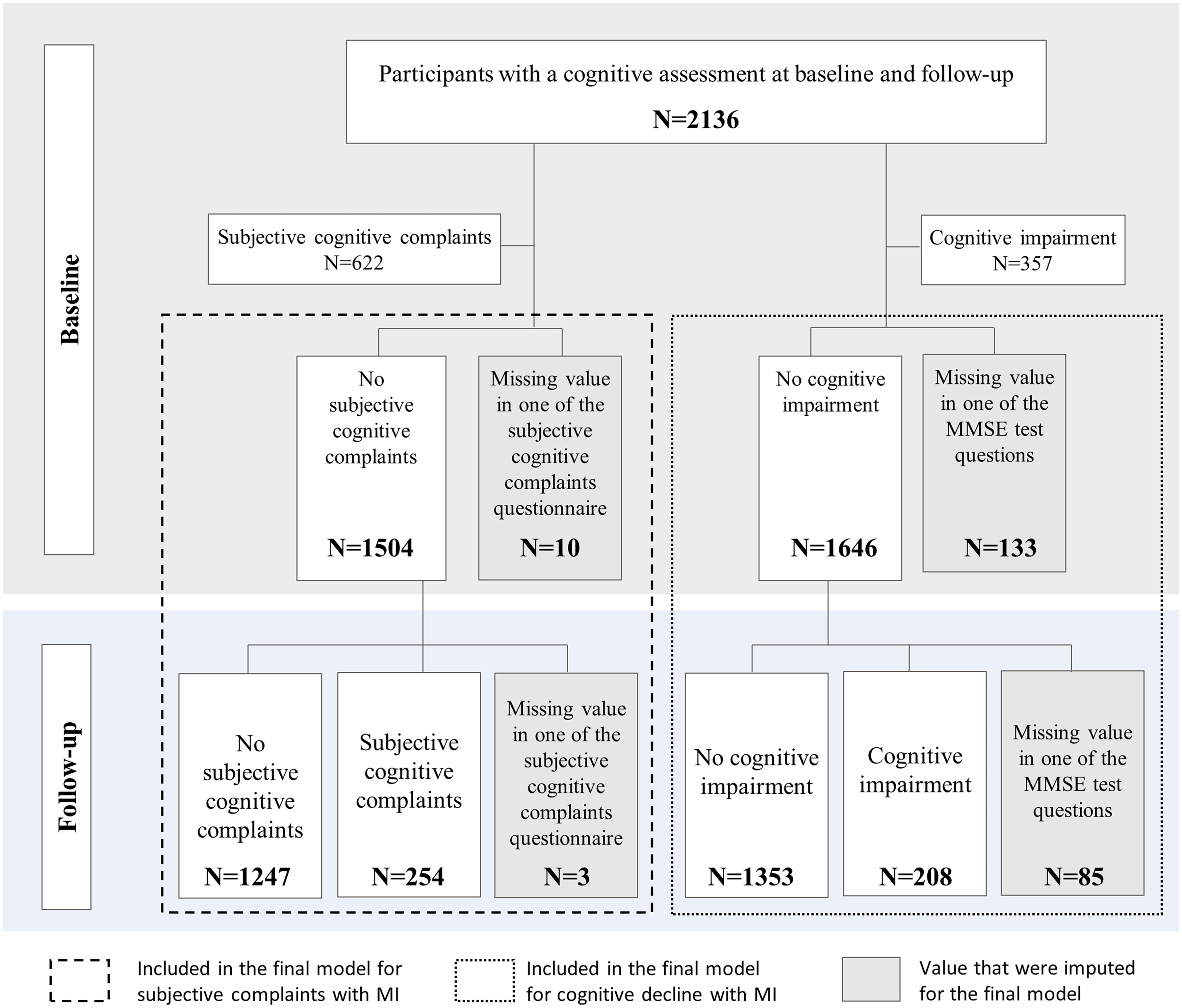
Flowchart describing how each sample for the final analysis was derived.
The 1504 participants without subjective complaints at baseline had an average age of 54.9 (SD 9.34), 34.7% were older than 60 years old, 73.9% female, 21.8% had less than 6 years of education and 36.5% reported a monthly income of less than US$ 194.9 (Table 1). The average follow-up was 5.0 (SD 0.64).
Baseline characteristics of the sample.
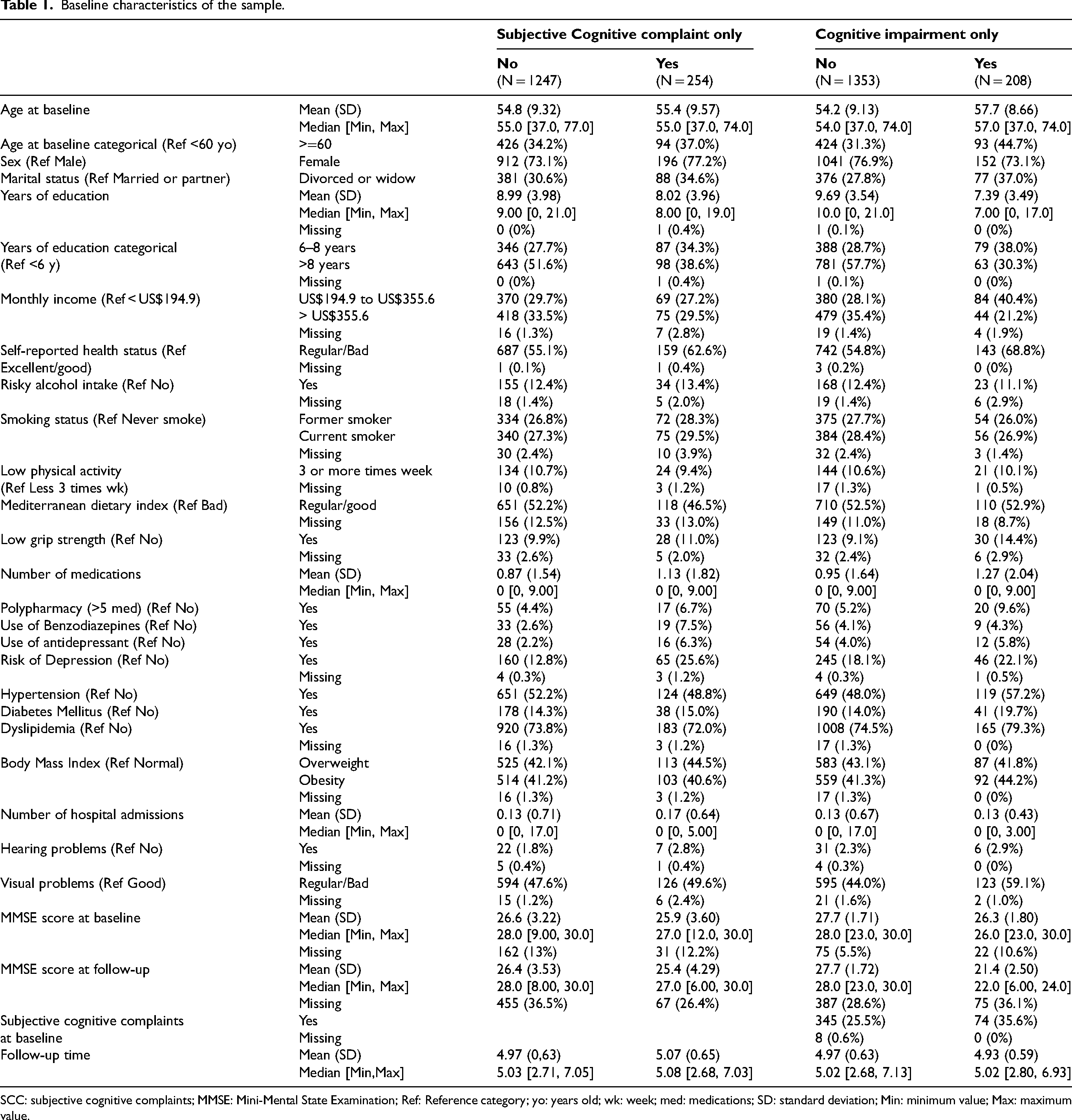
SCC: subjective cognitive complaints; MMSE: Mini-Mental State Examination; Ref: Reference category; yo: years old; wk: week; med: medications; SD: standard deviation; Min: minimum value; Max: maximum value.
The 1646 participants without cognitive impairment at baseline had an average age of 54.9 (SD 9.13), 34.3% were older than 60 years old, 76.7% female, 18.5% had less than 6 years of education and 36.7% reported a monthly income of less than US$ 194.9. 26.7% of people without cognitive decline at baseline also referred SCC (Table 1).
Subjective cognitive complaints
Of the 1504 people without SCC at baseline, 254 (16.9%) reported SCC at follow-up (Table 1). The median survival rate was 6.7 (95% CI 6.0–6.9) and the cumulative probability of developing SCC at 5 years was 0.091 (95% CI 0.07–0.11) (Figure 2). Being older, lower monthly income, the number of medications, use benzodiazepines, antidepressants and had a high risk of depression disorder were more likely to developed SCC at the follow-up (Univariate model in Table 2).
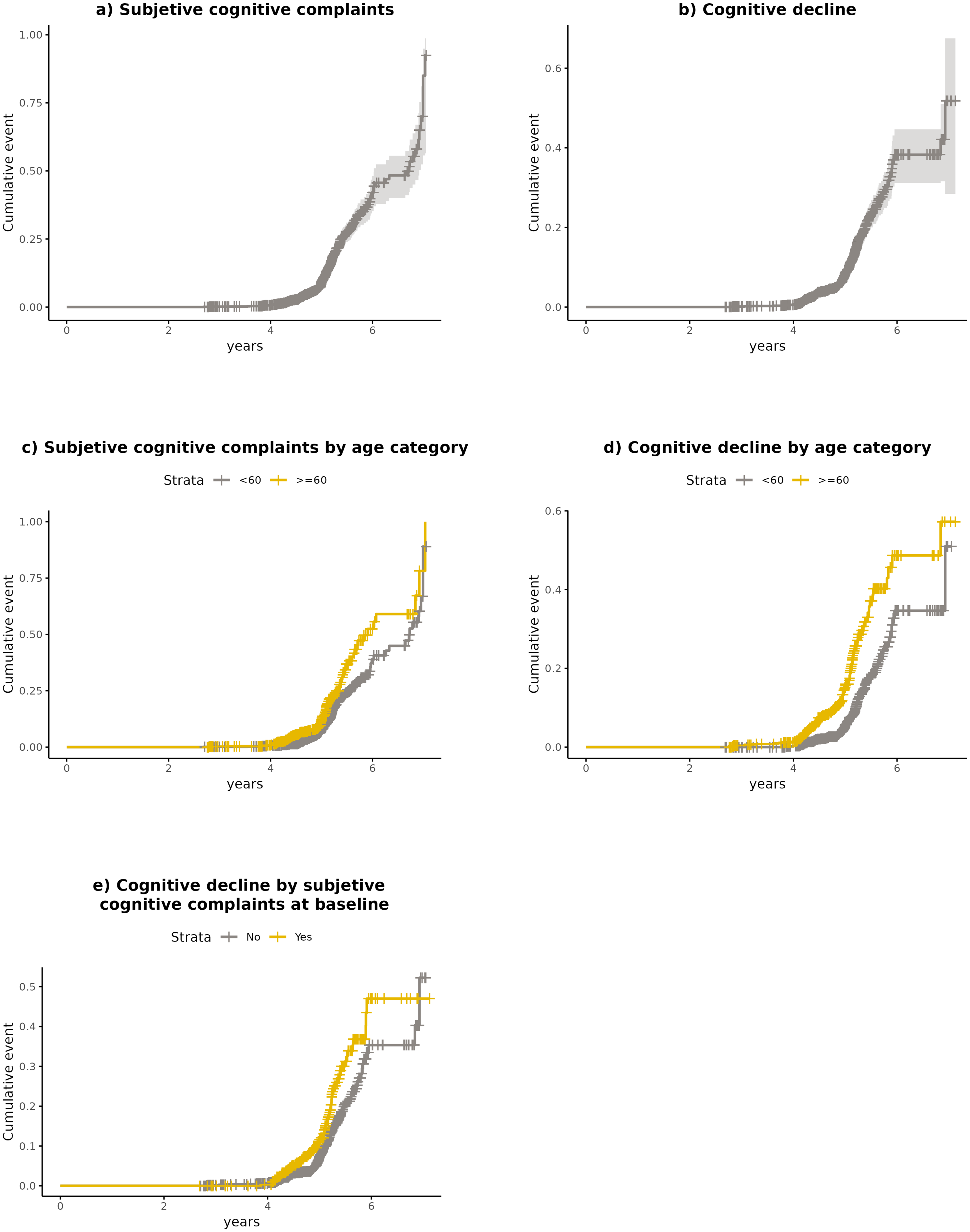
Kaplan–Meier curve for the cumulative probability of progress towards subjective complaints or cognitive decline. Kaplan-Meier curve for the (a) cumulative probability of progress towards SCC, (b) cumulative probability of progress towards cognitive decline, (c) cumulative probability of progress towards SCC by group of age, (d) cumulative probability of progress towards cognitive decline by group of age, and (e) cumulative probability of progress towards cognitive decline for participants with and without SCC at baseline.
Univariate and multivariate Cox-proportional hazard models for the risk of progression to subjective cognitive complaints.
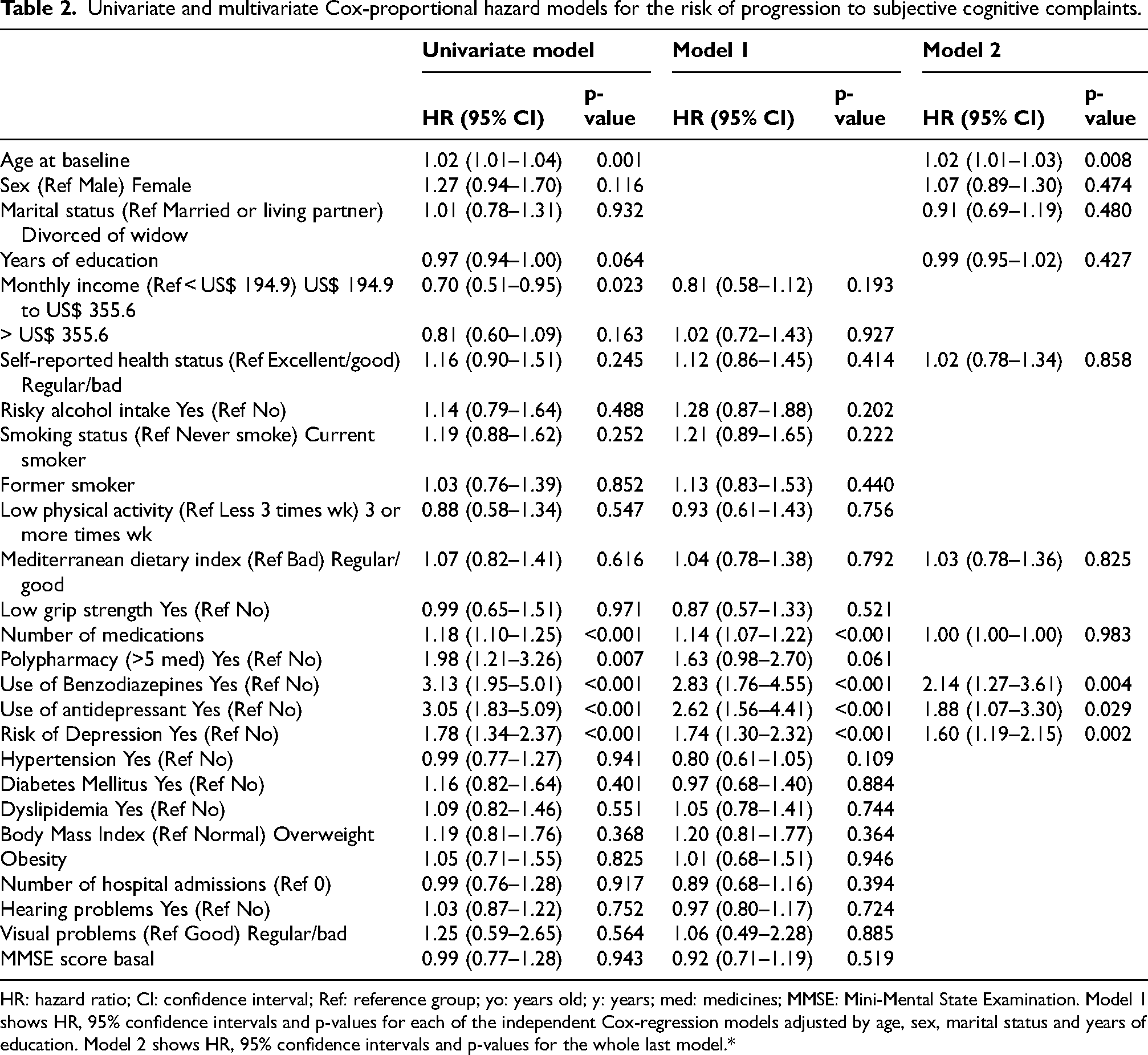
HR: hazard ratio; CI: confidence interval; Ref: reference group; yo: years old; y: years; med: medicines; MMSE: Mini-Mental State Examination. Model 1 shows HR, 95% confidence intervals and p-values for each of the independent Cox-regression models adjusted by age, sex, marital status and years of education. Model 2 shows HR, 95% confidence intervals and p-values for the whole last model.*
The number of medications, use of benzodiazepines, antidepressants and the risk of depressive disorder remained significantly associated with the incidence of SCC at follow-up after adjusting for age, sex, marital status and years of education (Model 1 in Table 2). The MMSE score, cardiovascular risk factors or self-reported health status at baseline were not associated to the development of SCC.
Older people (HR 1.02; 95% CI 1.01–1.03), and those who use benzodiazepines (HR 2.14; 95% CI 1.27–3.61), antidepressants (HR 1.88; 95% CI 1.07–3.30) or had depressive symptoms suggesting a depression (HR 1.60; 95% CI 1.19–2.15) were more likely to develop SCC during the follow-up (Model 2 in Table 2). People who used benzodiazepines or antidepressant at baseline were 2.14 and 1.88 times more likely to develop SCC respectively, independently of depressive symptoms.
Cognitive decline
Of the 1646 people without cognitive impairment at baseline, 208 (12.6%) had cognitive decline at follow-up (Table 1). The cumulative probability of developing cognitive decline at 5 years was 0.083 (95% CI 0.07–0.10) (Figure 2). Being old, with lower years of education, lower monthly income, regular or bad self-reported health status, low grip strength, higher number of medications, use antidepressants, hypertension, diabetes, visual problems and lower MMSE score at baseline were associated to a higher risk of cognitive decline (Univariate model in Table 3). People with SCC had a higher risk of developing cognitive impairment than those without SCC at baseline (Figure 2 and Table 3).
Univariate and multivariate Cox proportional hazard models for the risk of cognitive decline.
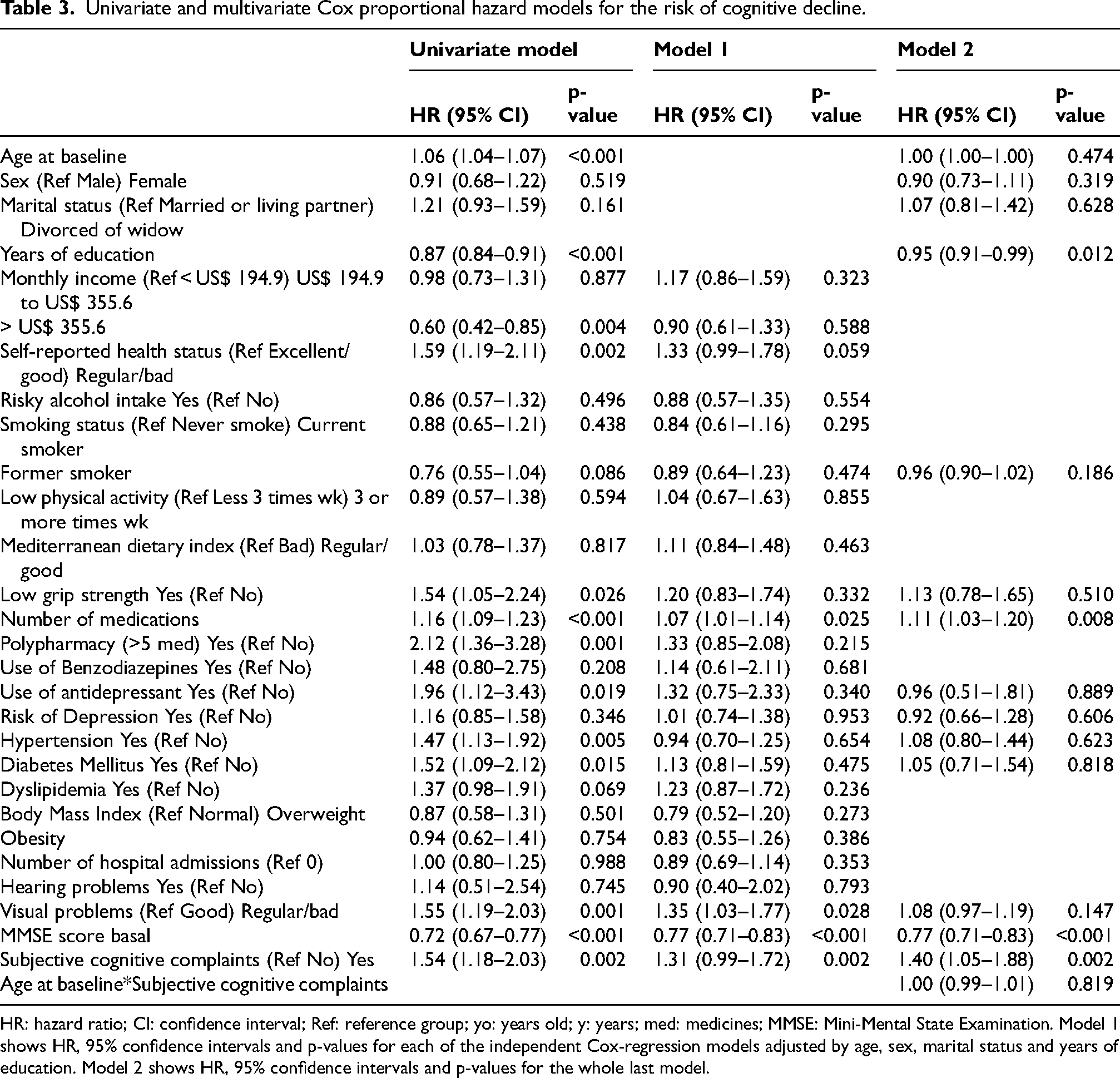
HR: hazard ratio; CI: confidence interval; Ref: reference group; yo: years old; y: years; med: medicines; MMSE: Mini-Mental State Examination. Model 1 shows HR, 95% confidence intervals and p-values for each of the independent Cox-regression models adjusted by age, sex, marital status and years of education. Model 2 shows HR, 95% confidence intervals and p-values for the whole last model.
After accounting by age, sex, marital status and education, people with a higher number of mediations, lower MMSE score and SCC at baseline were more likely to develop cognitive impairment during the follow-up (Model 2 in Table 3). People with SCC at baseline were 1.40 times more likely (HR 1.40; 95% CI 1.05–1.88) to have cognitive decline than people without SCC.
The effect of age
The interaction term for age and SCC in the model for cognitive decline was not significant (Table 3). However, HRs by age predicted from model 2 show that the HR is lower for those without SCC compared to those with subjective complaints when age is lower than 60 years old. From age 60 onward, this trend reverses, although confidence intervals overlap (Figure 3). Results from the subgroup analysis show that the effect of SCC was associated with cognitive decline in participants younger than 60 years old but not in the older group (Figure 4 and Supplemental Table 4).
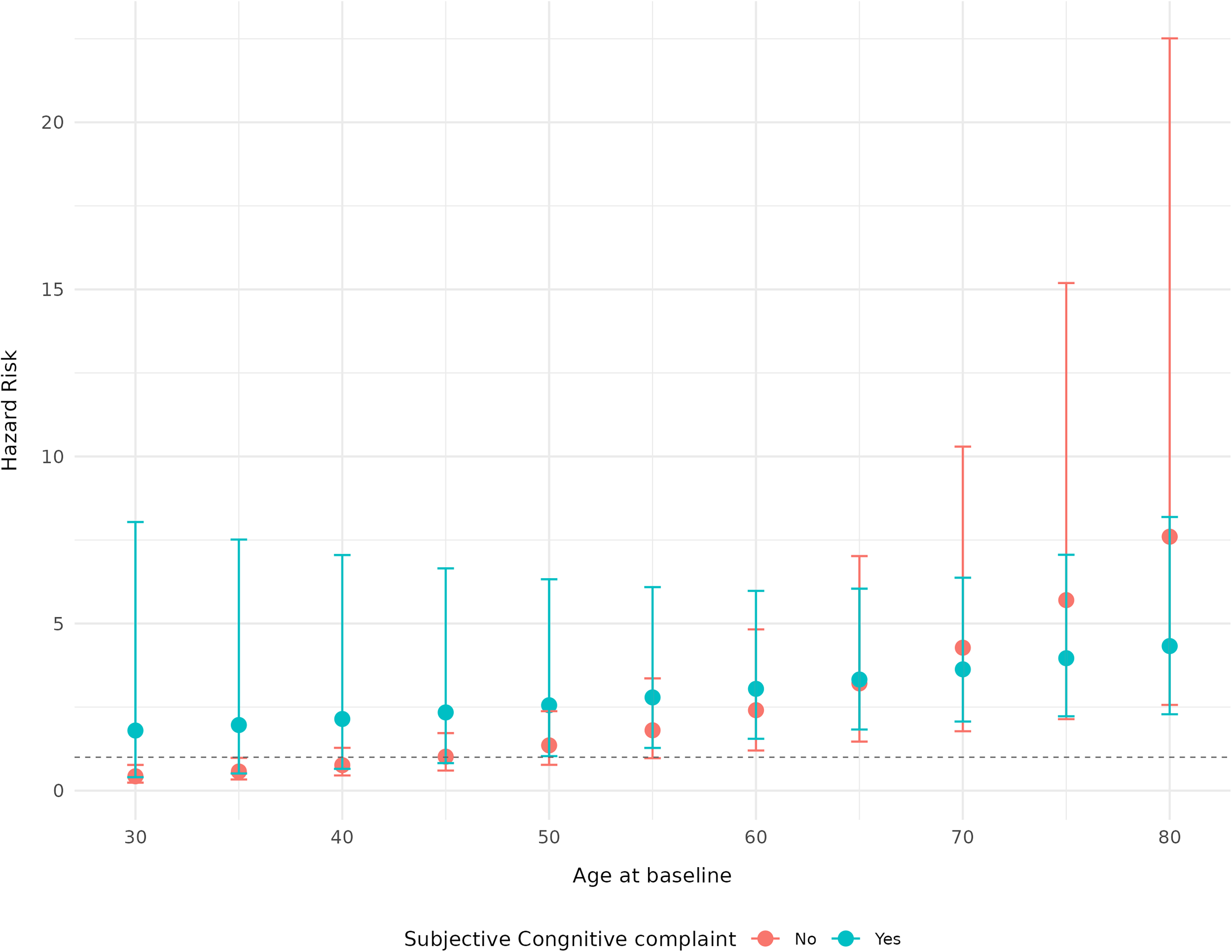
Predicted HR and 95% CI for the risk of cognitive decline by subjective cognitive decline and age.
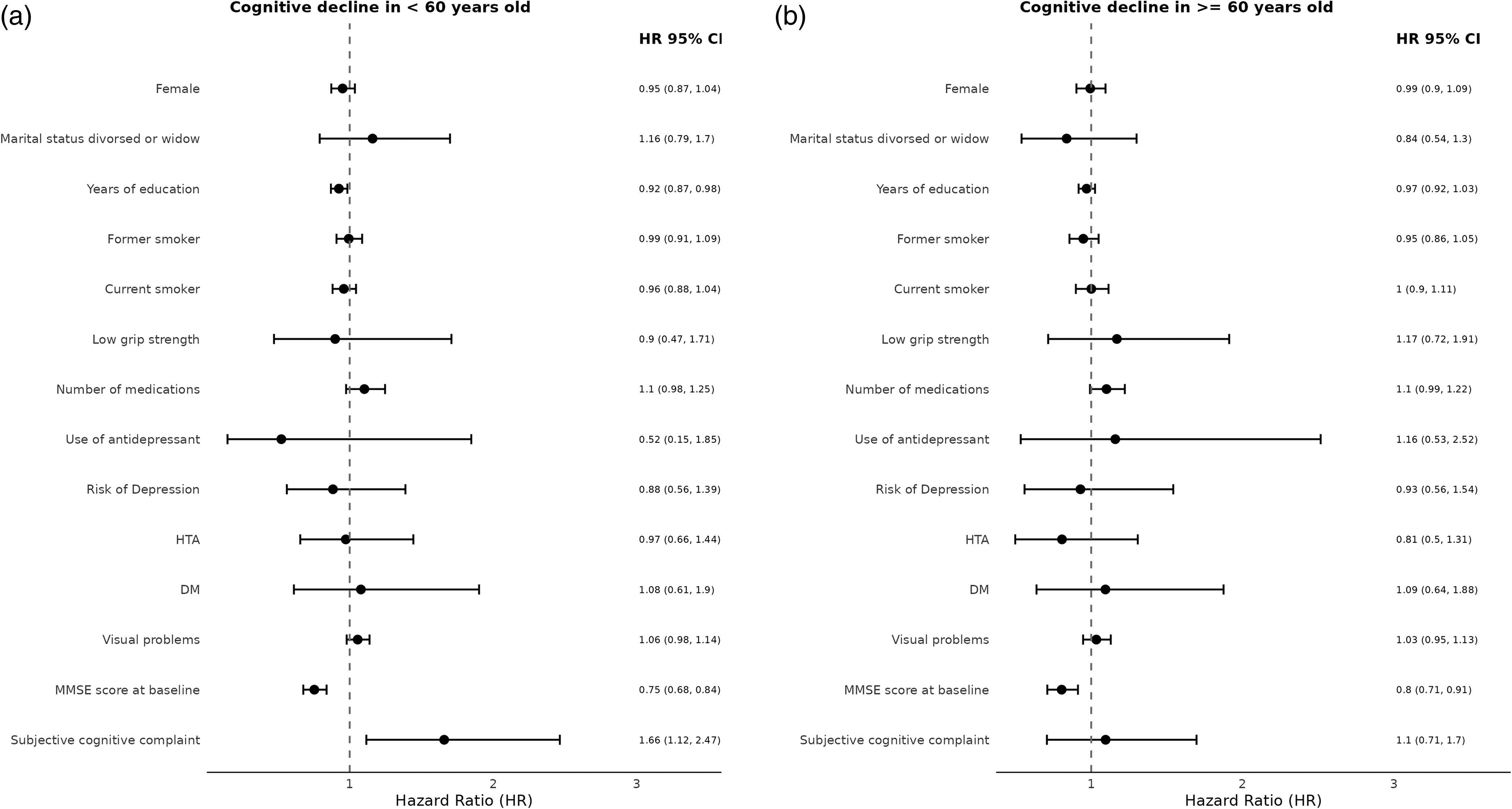
Multivariate Cox-proportional models for the risk of cognitive decline by age.
Figure 4 shows the hazard ratios (HR) and 95% confidence intervals (CI) from multivariate Cox Proportional Hazard Models fit (Model 2) after multiple imputation by group of age (<60 years old and >=60 years old). Figure a) shows the HR and 95% CI for models analyzing the risk of cognitive decline in < 60 years old and Figure b) for those 60 years and older.
Sensitivity analysis
Results from the sensitivity analysis, without multiple imputation of missing values, show very similar results (Supplemental Tables 2 and 3). Excluding participants with depressive symptoms from the analysis does not change the main results. People without depressive symptoms but with benzodiazepine and antidepressant use have a higher risk of developing SCC at follow-up (Supplemental Table 5).
Discussion
In this population-based cohort study in adults from a rural community in Chile, we found that factors associated with the incidence of SCC and objective cognitive decline differ. People with SCC were 1.40 times more likely to develop objective cognitive decline than those without SCC. Factors associated with both outcomes in our study differ by age.
Our results reveal distinct factors associated with the incidence of subjective cognitive complaint and cognitive decline. Subjective complaints were associated with psychological symptoms and the use of antidepressants and benzodiazepines rather than cardiovascular or other physical factors associated with cognitive decline. It is possible that the measure of SCC used in this study might capture mental health symptoms as well as pre-clinical cognitive impairment. Whether the incidence of SCC represents a worsening of mental health issues or initial cognitive impairment needs further research.
We found that people with SCC had a 1.40 times higher cumulative probability of cognitive decline than those without. This association was driven by a higher risk of cognitive decline among people younger than 60 years old. These findings are consistent with the literature. Pike et al. reported a 1.9 hazard ratio risk for developing dementia and 1.73 for developing mild cognitive impairment. 32 An et al.'s review found that age at baseline influenced progression to dementia among people with subjective complaints. Progression rates followed a U-shaped curve, dropping between ages 50 and 60, and then rising again after age 70. This suggests that people under 60 might face a higher risk than those in their 60s, but risk increases again in older age. 9 It has been proposed that cognitive awareness might explain the higher risk of cognitive decline among younger people with SCC. 33 It is also possible that subjective complaints are less specific among adults between 60–70 due to the high prevalence of these symptoms. We did not observe a rise in the risk of progression to cognitive decline over 70 years old in our data, possibly due to a low proportion of older people in the cohort.
Our results support the notion of subjective complaints being a pre-clinical phase of dementia. However, 20% of older adults report SCC, 7 and 66% of people with subjective complaints in our sample did not report them again at follow-up. Predictors of cognitive decline among people with SCC include persistent complaints, self- and informant-reported complaints and biomarkers such as cerebral amyloid β-protein deposition and elevated cerebrospinal fluid tau levels, which could help identify high-risk groups for interventions.8,9 Further research is needed to better understand whether the age of subjective complaintś onset could be a predictor of cognitive decline.
Thirteen percent of our cohort developed cognitive decline over 5 years with an overall rate of progression of 19.6 per 1000 person-year. Similar results were reported in Pike et al., with a mean progression to mild cognitive impairment and dementia of 15% and 10% respectively. 32 The mean MMSE score at follow-up for those with cognitive decline in our study was 21.4 (SD 2.5), indicating mild-cognitive impairment. These findings are not surprising as our sample comprises a relatively young population.
We did not find an association between well-established risk factors of cognitive decline such as behavioral, cardiovascular risk factors and hearing problems when adjusting by age and education. 5 Differences in the duration, consistency, and timing of exposure to these risk factors might explain these findings. Most cardiovascular risk factors such as diabetes, smoking and physical activity are associated with dementia incidence when exposure occurs in midlife rather than late life.5,34,35 Additionally, studies evaluating risk factors of dementia often have an average follow-up of 10 years. 5 A more detailed characterization of risk and protective factors and a longer follow-up period might enable us to better identify subjects with a higher risk of dementia.
Strengths and limitations
To our knowledge, this is the first study that explores factors associated with the incidence of subjective and objective cognitive symptoms in Chile. We used a large population-based cohort, and validated instruments to measure our outcomes and covariables. The MAUCO population does not necessarily represent all the Chilean population. We found a high proportion of missing values for MMSE test both, at baseline and follow-up. Nevertheless, we were able to address this problem with Multiple Imputation and other techniques suggested in the literature, 36 and the sensitivity analysis comparing results with and without MI did not differ significantly. The MAUCO cohort represents a very low-educated population. The level of education is a well-known influencing factor of MMSE test scores. 17 While we used differential cut-off point based on educational level proposed in the literature to determine cognitive impairment, other objective cognitive tests that are not influenced by education might be useful to fully understand incidence of more objective cognitive impairment in this population.
Conclusions and implications
In this large population-based cohort, use of benzodiazepines and antidepressant were the main factors associated with progression of SCC while subjective complaint was the strongest factor associated to cognitive decline at younger ages. Both SCC and MMSE scores deteriorated with age. Either SCC or MMSE scores were predictors of further cognitive deterioration and should be used to target preventive interventions.
Supplemental Material
sj-pdf-1-alz-10.1177_13872877251406622 - Supplemental material for Subjective cognitive complaints and cognitive decline in the MAUCO population-based prospective cohort
Supplemental material, sj-pdf-1-alz-10.1177_13872877251406622 for Subjective cognitive complaints and cognitive decline in the MAUCO population-based prospective cohort by Javiera Leniz, Laura A. Huidobro, Sandra Cortés, Claudia Bambs, Catterina Ferreccio and Pablo Toro in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We would like to thank the MAUCO team and all participants for their time and assistance.
Ethical considerations
The MAUCO study protocol was approved by Ethics Committees at Pontificia Universidad Católica de Chile (N◦ 14–141) and the Maule Regional Service of the Chilean Ministry of Health.
Consent to participate
Informed consent was obtained from all participants in written.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The MAUCO cohort is supported by two grants from the Agencia Nacional de Investigación y Desarrollo (ANID), a Chilean governmental scientific research commission: Fondo de Financiamiento de Centros de Investigación en Areas Prioritarias (FONDAP) (grant number 15130011) and Fondo Nacional de Desarrollo Científico y Tecnológico (FONDECYT) (grant number 1170395). MAUCO also received material support from the Faculty of Medicine of Universidad Católica del Maule University, the School of Medicine of the Pontificia Universidad Católica de Chile University, the Ilustre Municipalidad de Molina (Molina's municipality) and the Molina and Curicó hospitals. Claudia Bambs also receives funding from the Center for cancer prevention and control, CECAN, FONDAP 152220002, Santiago, Chile.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the Advanced Center for chronic Diseases (ACCDiS) Directorate in accordance with the local institutional review board authorization, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.