
Abstract
Background
Dementia is a major global public health challenge, and gaps in public knowledge and stigma impede timely diagnosis and inclusive care. The Dementia Friends program is a brief community intervention to improve dementia knowledge and attitudes, but its effectiveness outside the UK, including Israel, is under-evaluated.
Objective
This study examined whether participation in the Israeli Dementia Friends program was associated with changes in dementia-related knowledge and stigma. In addition, we assessed whether perceived susceptibility, familiarity with dementia, and self-perception as a change agent were linked to these changes.
Methods
A pre-post research design included 820 participants at baseline (Time 1) and 205 at a three-month follow-up (Time 2). Participants completed questionnaires on subjective and objective dementia knowledge, stigma (emotional reactions and discriminatory behavior), perceived susceptibility, and perceiving oneself as a change agent. Data was analyzed using t-tests, analyses of variance (ANOVA), and regression analyses.
Results
Significant increases were found in subjective (p = 0.005) and objective (p = 0.019) dementia knowledge, with improved positive emotional reactions (p = 0.012). Negative emotional reactions decreased (p = 0.05), but discriminatory behavior showed no significant change (p = 0.75). Higher education was most strongly associated with increases in knowledge, and reductions in perceived susceptibility were associated with decreases in negative emotional reactions and discriminatory behavior.
Conclusions
Program participation was associated with higher dementia knowledge and more positive emotional responses, though discriminatory behaviors persisted. More comprehensive strategies beyond education are needed to fully address stigma.
Keywords
Introduction
Dementia is a global public-health concern defined as a syndrome of chronic or progressive brain diseases impairing memory, comprehension, learning, and judgment. 1 It is the seventh leading cause of death globally and a significant contributor to disability in older adults. 2 Current estimates predict the number of people living with dementia will rise from 55 million in 2020 to 78 million by 2030 and 139 million by 2050. 3 Despite these alarming trends, dementia remains an insufficiently addressed public-health issue.
This gap is reflected in a widespread lack of knowledge and persistent stigma toward dementia. 4 Individuals with dementia often face negative stereotypes about unpredictability, communication difficulties, and changes in appearance,5,6 as well as misconceptions, such as viewing dementia as part of the normal aging process or thinking nothing can be done to avert it. These stigmatic beliefs can lead to discriminatory behaviors, such as social distancing, support for institutionalization, and biases in employment and health insurance, resulting in social isolation and loss of status.7,8
In light of this ongoing awareness gap, there is an urgent need for targeted educational initiatives that both increase understanding of dementia and reduce stigma, fostering inclusive, supportive environments for people living with the condition and their caregivers. In response to this need—and to help mitigate dementia's impact on patients, families, and society at large—the Alzheimer's Society in the UK launched the “Dementia Friends” program in 2013. 9 This scalable, community-based intervention has since been adapted globally to improve knowledge, attitudes, and behaviors toward dementia.
The British Dementia Friends program provides essential information on dementia, its symptoms, and effective communication techniques to foster understanding and reduce stigma. 10 The program reached about one million participants through a one-time session focusing on five key messages: dementia is caused by a disease of the brain, not aging; dementia is more than forgetfulness; individuals with dementia can lead fulfilling lives; and individuals with dementia are more than their symptoms. Lectures, exercises, scenarios, and videos were used in the sessions.11,12 Participants were encouraged to take social action such as sharing information or volunteering in this context.13,14
As the initiative has spread, more than 20 million people have participated in the program in many countries, including the U.S. (in 24 states), Canada, Australia, South Korea, Germany, Denmark, Scotland, Wales, and Northern Ireland.9,11 Further to this broad implementation of the program worldwide, the effectiveness of the program's informational sessions has been examined in studies conducted in various countries. Such studies have consistently shown positive results, with participants gaining knowledge about dementia and improving their attitudes toward individuals with the condition.9,10,15 Most participants have been students or adolescents.9,10,12,16,17 However, evidence of stigma reduction has been limited, with only one study showing a notable reduction in stigma among nursing students. 18 Following these important yet inconclusive results, a Dementia Friends program was developed and implemented in Israel.
The Israeli Dementia Friends program
In Israel, the Dementia Friends program was developed through a partnership between a partnership between governmental, non-profit, and community organizations. It became a central part of the national plan to address dementia, aiming to raise public knowledge, reduce stigma, and cultivate dementia-friendly communities that support individuals with dementia. 19
Similar to programs in other countries, the sessions in Israel provided information on the main types of dementia, symptoms, brain changes, and the role of communication in treatment, and included lectures, group exercises, scenario-based activities, and videos. Each session lasted about an hour and was held in various cities across Israel, from the northern regions to the central areas. Potential participants were recruited by the research coordinator in collaboration with EMDA (the Israel Alzheimer's and Dementia Association), a non-profit organization dedicated to raising awareness, providing support, and delivering services for people with dementia and their families. Recruitment took place through schools, community organizations, and elder-care groups across various regions of Israel.
The Israeli Dementia Friends program stood out due to adaptations tailored to Israeli society's needs. First, the sessions were accessible to all ages and educational backgrounds and were open to the public. Second, they included interactive group discussions alongside lectures to enable deeper understanding. Third, coordinators received specialized training to lead sessions for diverse populations. Finally, the program was sustained through local authorities across Israel, offered both in-person and online via a website and Facebook page. Finally, like similar programs elsewhere, it was also accompanied by evaluation research.
The evaluation study
The study's objective was to assess the Dementia Friends program's effectiveness within the Israeli context. Specifically, we aimed to explore whether the adaptation and implementation of the program markedly increased knowledge about dementia and decreased stigma within the Israeli population.
The theoretical framework guiding the evaluation study draws on several established models and theories related to health behavior change and stigma reduction. One such model is the Health Belief Model (HBM),20,21 which suggests that individuals’ perceptions of susceptibility to a health issue (in this case, dementia) can influence their behaviors and attitudes toward that issue. According to the HBM, perceived susceptibility, or the belief about one's risk of developing dementia, can increase motivation to engage in educational programs and adopt behaviors that reduce stigma. Additionally, the Theory of Planned Behavior (TPB)22,23 provided input especially in regards of how familiarity with dementia and perceiving oneself as a change agent may influence participants’ attitudes and behaviors. According to the TPB, individuals are more likely to engage in behaviors that they believe they have control over and that align with their intentions. Thus, in the context of the Dementia Friends program, increased familiarity with dementia may reduce stigma by improving attitudes, while perceiving oneself as a change agent could empower participants to act as advocates for people with dementia, further contributing to stigma reduction.
In accordance with these models, we hypothesized that we would find:
Changes in knowledge and stigma between Time 1 (before participating in the informational meeting) and Time 2 (three months after participating in the informational meeting); That changes in study variables (perceived susceptibility, familiarity with dementia, and perceiving oneself as a change agent) would contribute to an increase in knowledge about dementia and a decrease in stigma. Changes in study variables (e.g., perceived susceptibility, familiarity with dementia, and perceiving oneself as a change agent) will be associated with changes in dementia knowledge (both subjective and objective) and dementia stigma (positive emotional reactions, negative emotional reactions, and discriminatory behavior). Additionally, changes in knowledge (subjective and objective) will be associated with changes in dementia stigma.
Methods
Design and procedure
In the current study, approved by Bar-Ilan University's Ethics Committee (Approval No. 111703), a pre-post research design was used to evaluate the program's effectiveness. Potential participants were required to meet the following criteria to participate in the evaluation study. Inclusion criteria were age 18+, ability to understand and communicate in Hebrew, and no previous diagnosis of dementia. Exclusion criteria included: current diagnosis of dementia or other cognitive impairments, and participation in a similar program within the last 6 months. After signing an informed consent, eligible participants were asked to complete questionnaires in Hebrew at the beginning of the first session (Time 1) using pen and paper. Follow-up phone interviews were conducted three months later (Time 2) to assess both the immediate and lasting effects of the program on dementia knowledge and stigma. Program coordinators from EMDA organized the sessions, informing the research team of the times and locations. A research team member attended each session to distribute the questionnaires and collect them when completed. The study was not designed or powered for inferential subgroup comparisons by religion/ethnicity; analyses prioritized overall effects with demographic controls, and subgroup distributions are reported descriptively (Table 1).
Characteristics of all participants who filled out the questionnaire at Time 1 (n = 820).

Participant flow and follow-up
We prospectively tracked participation from Time 1 (T1) to Time 2 (T2) and report a detailed flow diagram in Supplemental Figure 1. The flow diagram includes available reasons for non-completion (e.g., unreachable, declined, scheduling conflict). Baseline comparisons of completers versus dropouts across sociodemographic characteristics and T1 study variables are shown in Supplemental Tables 1 and 2. At T1, questionnaires were self-administered on paper in-session. At T2, the same items and response scales were administered via standardized phone interviews (scripted protocol, interviewer training) to limit mode-related variance.
Measures
Knowledge about dementia
Subjective knowledge was assessed using a single item: “How much do you know about dementia?” Answers were rated on a 5-point Likert-type scale, ranging from 1 (not much at all) to 5 (very much). This single-item approach to assessing subjective knowledge has been used in previous studies and shown to yield meaningful data in public health and dementia research contexts.6,24 Objective knowledge was assessed using a list of four symptoms (e.g., being disoriented), and participants indicated whether they associated these symptoms with dementia. An overall index was calculated by summing the number of correct symptoms rated as being related to dementia (0 = wrong answer; 1 = correct answer), with higher scores indicating a higher objective knowledge. Previous studies using the knowledge questionnaire showed an alpha of 0.71 and above,24–26 suggesting acceptable internal consistency.
Dementia stigma was assessed on the basis of previous studies 26 and included three aspects of public stigma— positive emotional reactions, negative emotional reactions, and discriminatory behavior—using two items for each stigma type. Each item was rated on a 5-point Likert-type scale, ranging from 1 (strongly disagree) to 5 (strongly agree). Correlation between the two items of positive stigma at T1 was r = 0.54 (p < 0.001); of negative stigma r = 0.14 (p < 0.001); and of discriminatory behavior r = 0.15 (p < 0.001). Overall indices were calculated by averaging the items in each type of stigma, with higher scores indicating higher dementia stigma.
Perceived susceptibility, was assessed with two items: “How worried are you about developing dementia during your lifetime?” and “To what extent do you assess your chances of developing dementia during your lifetime?”. 27 Answers were rated on a 5-point Likert-type scale, ranging from 1 (a very low extent) to 5 (a very high extent). Correlation between the two items at T1 was r = 0.44 (p < 0.001). An overall index was calculated by averaging both items.
Familiarity with dementia was assessed at baseline (T1) using two binary items: (1) “Do you have a family member diagnosed with dementia?” and (2) “Do you have an acquaintance diagnosed with dementia?” (yes = 1 / no = 0). 27 Responses were combined into a binary indicator (0 = no familiarity; 1 = familiarity with a family member and/or an acquaintance diagnosed with dementia). No imputation was applied for this variable; blank responses were coded as 0.
Perceiving oneself as a change agent, which refers to the belief that one can effect positive changes for the benefit of others, was assessed using a single item composed for the present study: “To what extent do you perceive yourself as a person who makes changes for the sake of others?” Answers were rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (to a very high extent).
Sociodemographic characteristics included gender, age, marital status, number of children, years of education, place of birth, religion, volunteer (yes/no).
Data analysis
Data were analyzed with SPSS ver. 29. Background variables were described using means and standard deviations for continuous variables, and frequencies and percentages for categorical ones. Demographic differences between participants who were available at T2 versus participants who were no longer participating in the study were calculated with t-tests, chi squares, and Z ratios for the comparison of independent proportions. Missing values, for participants who were available at T2, were replaced with the expectation-maximization method, using maximum likelihood estimation.
Analysis of missing data revealed, that for the 205 participants who were available at T2, there were 1.5% to 18% of missing data in the study variables before the informational meeting. There were zero to 3.4% of missing data in their responses after the informational meeting (see Supplemental Material). Missing was not at random in T1 (Little's MCAR test: χ2(92) = 143.90, p < 0.001), and was not at random in T2 (Little's MCAR test: χ2(25) = 64.64, p < 0.001). Analyses for T1 showed that gender (female) was associated with a higher percentage of missing values for T1 subjective knowledge (r = -0.24), and T1 negative emotional stigma (r = -0.22). Age was negatively associated with missing values for T1 objective knowledge (r = -0.29), and years of education were positively associated with T1 subjective and objective knowledge (r = 0.33 and r = 0.32, respectively). Analyses for T2 showed that age was positively associated with missing values for T2 negative emotional stigma (r = 0.21), and years of education were positively associated with T2 subjective and objective knowledge (r = 0.33 and r = 0.27, respectively).
The relationships between the background variables and the study variables at T1 were examined with Pearson correlations and t-tests. Longitudinal differences in the study variables were evaluated with analyses of covariance (ANCOVA), controlling for gender, age, and years of education. For the purpose of the third hypothesis, change in the study variables was defined with adjusted (standardized) residual gains, controlling for the Time 1 values. Change indices: We computed standardized residual gains (SRG) by regressing Time 2 (T2) scores on Time 1 (T1) scores and saving the standardized residuals. Multiple regressions were calculated for change in knowledge and in the three types of stigma. Control variables were gender, age, and years of education. Independent variables were familiarity with a person with dementia, change in subjective and objective knowledge, change in perceived susceptibility, and change in perceiving oneself as a change agent.
Results
Key findings
From T1 to T2, subjective and objective knowledge increased, positive emotional reactions increased, and negative emotional reactions decreased, whereas discriminatory behavior did not change (small effects; η2 ≈ 0.02–0.04). In the regression models, a higher education level was associated with greater increases in both subjective and objective knowledge. Further, an increase in subjective knowledge was associated with decrease in negative emotions, decrease in perceived susceptibility was associated with reductions in negative emotions and discriminatory behavior, and a positive change in self perception as a change agent was associated with an increase in positive emotions.
Participant characteristics
Table 1 includes the characteristics of the participants who completed the questionnaire at T1 (n = 820). Most were women over 60 years of age, married, with an average of two-to-three children, and with more than 13 years of education. In addition, most were Jewish, and over half were born in Israel and reported knowing a person with dementia. About half had previously volunteered in the field of dementia care. Given the small cell sizes for several non-Jewish subgroups (e.g., Muslim n = 22; Christian n = 11; Druze n = 24), we did not conduct inferential subgroup comparisons; distributions are reported descriptively in Table 1.
No statistically significant differences were found between participants who completed the questionnaire at both times (n = 205) and participants who participated only at T1 (n = 615) in either their demographic characteristics or in the study variables: subjective knowledge, objective knowledge, perceived susceptibility, familiarity with dementia, perceiving oneself as a change agent, and dementia stigma (see Supplemental Material).
Associations between outcome variables and demographic characteristics
Relationships between the study's variables and demographic characteristics were examined at T1. Regarding gender, women evaluated their subjective knowledge (mean=3.14, SD = 1.06) higher than did men (mean=2.60, SD = 0.87) (t(169) = 3.11, p = 0.002). No differences were found in objective knowledge. The level of positive emotional reactions was higher for women (mean=4.07, SD = 0.98) than for men (mean=3.72, SD = 1.09) (t(179) = 2.13, p = 0.034), as was the level of negative emotional reactions (mean=1.76, SD = 0.88 versus mean=1.34, SD = 0.56, t(143.46) = 3.63, p < 0.001). Age was significantly and negatively associated with objective knowledge (r = -0.28, p < 0.001), but not with subjective knowledge. Age was further significantly and positively associated with negative emotional reactions (r = 0.16, p = 0.042). Years of education was positively associated with subjective knowledge (r = 0.28, p < 0.001), as well as with objective knowledge (r = 0.30, p < 0.001). Years of education was further positively associated with perceived susceptibility (r = 0.18, p = 0.013). Other demographic variables were unrelated to the study variables or had low variance. Thus, the study hypotheses were examined while controlling for gender (men-1, women-0), age, and years of education.
Differences across time
Lead-in
From T1 to T2, knowledge and positive emotional reactions increased, negative emotional reactions decreased, while discriminatory behavior, perceived susceptibility, and perceiving oneself as a change agent showed no change; effects were small (η2 ≈ 0.02–0.04).
Table 2 shows the differences between T1 and T2 meetings in the study variables. Significant increases were found in subjective and objective knowledge, as well as in positive emotional reactions. A significant decrease was noted in negative emotional reactions. No change was observed in discriminatory behavior, perceived susceptibility, and perceiving oneself as a change agent. Given attrition from 820 at baseline to 205 at follow-up, these pre–post differences should be interpreted with caution. Although baseline comparisons indicated no significant differences between completers and dropouts across sociodemographic characteristics and T1 study variables (Supplemental Tables 1 and 2), differential retention, due to variables not measured here, may still have affected the estimates of change.
Differences between Time 1 and Time 2 in the study variables (n = 205), with effect sizes (η2). a
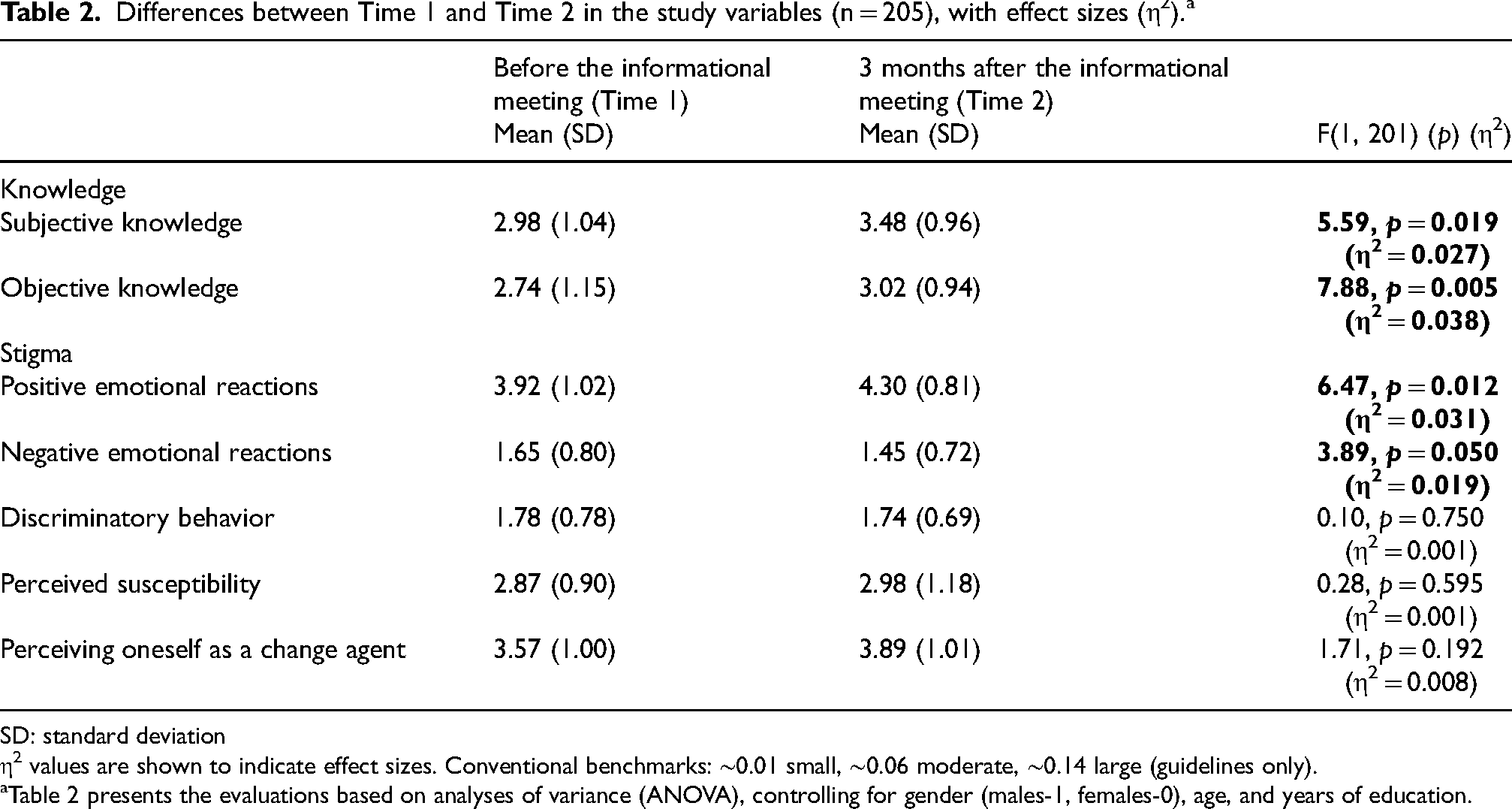
SD: standard deviation
η2 values are shown to indicate effect sizes. Conventional benchmarks: ∼0.01 small, ∼0.06 moderate, ∼0.14 large (guidelines only).
Table 2 presents the evaluations based on analyses of variance (ANOVA), controlling for gender (males-1, females-0), age, and years of education.
Takeaway: Knowledge↑; negative emotions↓; discriminatory behavior = ns; perceived susceptibility = ns; change-agency = ns (η2 ≈ 0.02–0.04).
Correlates of change in knowledge and stigma
Lead-in
Greater familiarity was associated with larger knowledge gains; increases in subjective knowledge were associated with lower negative emotions; decreases in perceived susceptibility were associated with reductions in both negative emotions and discriminatory behavior; and women and increases in change-agency were associated with higher positive emotions.
Change indices
Change analyses used standardized residual gains (SRG)- T2 regressed on T1 per outcome- providing baseline-adjusted indices of within-person change.
Pearson correlations were calculated for the associations among the change variables. Several correlations were found significant, although low in magnitude. Increase in knowledge (both subjective and objective) was higher for participants who knew a person with dementia. Change in subjective knowledge was positively associated with a change in objective knowledge. An increase in positive emotional reactions was higher among women. This increase was also associated with an increased perception of oneself as a change agent. A decrease in negative emotional reactions was associated with an increase in subjective knowledge, and with a decrease in perceived susceptibility. Finally, a decrease in discriminatory behavior was associated with a decrease in perceived susceptibility.
Summary (regression models)
In multiple regressions, a higher education level was associated with greater change in knowledge. Further, increase in subjective knowledge was associated with decrease in negative emotions, decrease in perceived susceptibility was associated with reductions in negative emotions and discriminatory behavior, and a positive change in self perception as a change agent was associated with an increase in positive emotions. Explained variance was modest (R2 ≈ 0.08–0.09).
Multiple regressions were calculated to assess the relative contribution of change in the study variables to change in knowledge. Control variables were gender, age, and years of education. The independent variables were familiarity with a person with dementia, change in perceived susceptibility, and change in perceiving oneself as a change agent. Neither regression model was significant (change in subjective knowledge: R2 = 0.05, F(6, 198) = 1.71, p = 0.119; change in objective knowledge: R2 = 0.04, F(6, 198) = 1.33, p = 0.246), and in both models, only years of education showed a significant association with knowledge (change in subjective knowledge: β=0.20, p = 0.007; change in objective knowledge: β=0.16, p = 0.025), such that higher education level was associated with greater change in knowledge.
Next, multiple regressions were calculated to assess the relative contribution of change in the study variables to change in stigma. Similar control and independent variables were used, with the addition of change in subjective and objective knowledge as independent variables. The three regression models are presented in Table 3.
Regression models for change in stigma (n = 205).
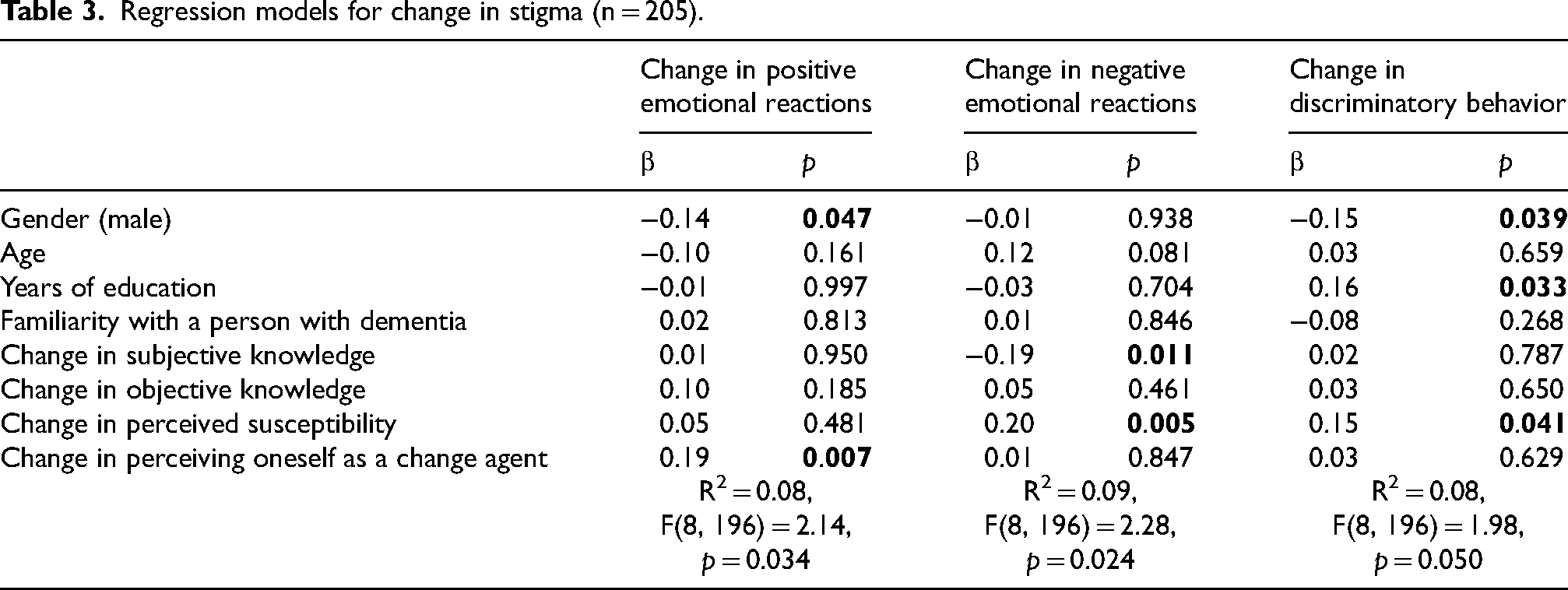
Takeaway: Familiarity → knowledge↑; ↑subjective knowledge & ↓perceived susceptibility → negative emotions↓; ↓perceived susceptibility → discriminatory behavior↓; education → knowledge gains; overall effects small.
The three models were significant, yet the explained variance in them was low. Change in positive emotional reactions was significantly related to gender and change in perceiving oneself as a change agent, such that among women, and among those who had a greater increase in perceiving themselves as a change agent, there was a greater increase in positive emotional reactions. Change in negative emotional reactions was significantly related to change in subjective knowledge and change in perceived susceptibility, such that a greater increase in subjective knowledge and a greater decrease in perceived susceptibility were associated with a greater decrease in negative emotional reactions. Change in discriminatory behavior was significantly related to gender and years of education, as well as to change in perceived susceptibility, such that for men, and for those with a lower education level and a greater decrease in perceived susceptibility, there was a greater decrease in discriminatory behavior.
Discussion
The study's findings align with previous research, demonstrating the effectiveness of the Dementia Friends program in significantly increasing knowledge about dementia. Studies from the UK, the U.S., and other countries have shown that participants’ knowledge about dementia improves after attending short, structured sessions that deliver key messages about the disease.9,11,28 Similarly, in the Israeli context, we observed increases in both subjective and objective knowledge from T1 to T2. The program's success in boosting knowledge can be attributed to the accessible format, which simplifies complex information about dementia. Moreover, the use of interactive group activities combined with factual presentations has been reported to engage participants, which may be associated with improved immediate comprehension and retention of key concepts. 10
In terms of the time between pre-and post-program measurements, most studies conducted on the program have employed short follow-up periods, ranging from immediately post-session to one month later.9,28 In the current study, the follow-up period was three months, providing valuable insights into the sustainability of knowledge gains. Although continued retention of knowledge was demonstrated over this three-month period, longer follow-up intervals (e.g., six months or a year) would be beneficial, as has been suggested by previous studies. 11 Researchers should also explore how repeated or ongoing educational interventions could reinforce this knowledge, potentially enhancing the program's overall effectiveness.
Regarding the three dimensions of dementia-related stigma—positive emotional reactions, negative emotional reactions, and discriminatory behavior—a mixed picture was revealed of the intervention's effects. On the one hand, the assessments conducted post-intervention showed an increase in participants’ positive emotional reactions toward individuals with dementia, a crucial factor in creating a more supportive and inclusive environment for those living with dementia. 29 Additionally, there was a significant decrease in negative emotional reactions, suggesting that the post-session assessments were associated with lower levels of discomfort and/or fear toward people with dementia. Although the literature on the role of Dementia Friends in reducing stigma is limited, our findings are consistent with broader research on knowledge and attitudes toward dementia.30,31 For instance, a study by Chang and Hsu (2020) in Taiwan revealed a link between increased knowledge and more positive attitudes toward dementia among 347 adults. The focus of that study 30 was on attitudes such as discomfort, shame, and unfriendliness, whereas we also examined positive emotional reactions and discriminatory behavior. As such, the current study provides a broader understanding of how educational interventions can influence different aspects of stigma.
The persistence of discriminatory behavior in both pre- and post-intervention highlights a significant challenge. Although educational programs can effectively alter knowledge and positive emotions, self-perceptions related to behavioral change are more complex, underscoring the need for more comprehensive approaches, including community engagement and policy initiatives. This notion resonates with broader research in stigma reduction, suggesting that a longer and multifaceted approach is essential to change all dimensions of stigma, including its perceived behavioral aspects.4,32,33 For example, a study regarding dementia stigma reduction, in which contact was created with people with dementia over 12 weeks, revealed a significant improvement in behavioral stigma and dementia-related stigma in general. 34 Although several η2 values were small, the program is brief, low-cost, and scalable. Modest but significant improvements in knowledge and emotional reactions, sustained over three months, can still have population-level relevance. At the same time, the lack of change in discriminatory behavior indicates that educational sessions alone are insufficient. Multi-component strategies may be required. Behavioral change is typically harder to achieve than shifts in knowledge or emotions because it depends not only on attitudes but also on opportunities, social norms, and perceived control (e.g., willingness versus ability to act in everyday settings).35,36
According to our multivariate analyses, higher education level was significantly associated with increased objective and subjective knowledge about dementia, even when controlling other variables such as age, gender, and familiarity with dementia. This finding suggests that individuals with a higher education level not only demonstrated a greater increase in their level of factual knowledge but also perceived themselves as being more knowledgeable about dementia. The relationship between education level and knowledge retention remained robust even in the presence of other factors. These findings align with previous research such as Crawley et al. (2022), which has demonstrated that higher levels of education contribute to greater dementia knowledge. 37 Education thus seems to be a key correlate in expanding both actual and perceived knowledge about dementia.
The lack of association between changes in knowledge and the independent variables—familiarity with dementia, perceived susceptibility, and perceiving oneself as a change agent—suggests that knowledge acquisition through educational programs may operate independently of personal experience or attitudes. Knowing a person with dementia may not lead to greater understanding, as personal experience alone does not provide comprehensive knowledge. 38 Similarly, perceived vulnerability to dementia often impacts emotional responses rather than increasing factual understanding (i.e., concern about the disease does not necessarily result in increased knowledge in the absence of targeted educational interventions). 4 Additionally, although believing in one's ability to effect change can motivate action, such belief is not inherently linked to acquiring new knowledge; formal education seems to play a more critical role. 39 These findings highlight the crucial role of structured education in effectively enhancing both objective and subjective knowledge about dementia.
Regarding the predictors of change in stigma, our findings showed that increased subjective knowledge was associated with reductions in negative emotional reactions. Namely, as participants gained a better understanding of dementia, their feelings of discomfort and/or fear toward individuals with dementia diminished, highlighting the role of knowledge in reducing stigmatizing attitudes. This finding aligns with a prior study conducted among 101 adults aged 18 and older from local universities in northern Minnesota, which revealed that taking part in Dementia Friends sessions increased knowledge about dementia and had a positive impact on participants’ attitudes toward dementia. 10 This pattern is consistent with theory-based accounts in which improved understanding reduces uncertainty and fear, thereby lowering affective stigma in the short term. 40
An association was found between a decrease in perceived susceptibility and a reduction in negative emotional reactions. This finding suggests that feeling less at risk of developing dementia and holding fewer ageist beliefs may be linked to lower levels of shame and fear toward the condition. At the same time, within HBM/TPB frameworks, reduced perceived risk could dampen prevention motivation unless paired with efficacy-enhancing elements (e.g., clear action options, skills, and perceived control). 41 Accordingly, brief information sessions should balance risk communication with concrete efficacy-building components to reduce fear-driven stigma while preserving engagement in preventive behaviors.
Nevertheless, these results are consistent with other studies examining links between negative feelings toward individuals with dementia, dementia-related anxiety, and false beliefs regarding dementia.42,43 For example, two online studies conducted among two different groups (295 university students between ages 18–58, and 352 adults between ages 18–81) revealed that negative attitudes and stigmatization toward older adults were associated with health-related concerns and anxiety about one's development of dementia in both groups. 43
Another finding was that a decrease in perceived susceptibility was linked to reduced discriminatory behavior toward individuals with dementia. Apparently, when people feel less at risk of developing dementia, their fear and anxiety decrease, leading to less discriminatory attitudes. As dementia cases are on the rise, it is important to reduce individuals’ personal fear; doing so can foster greater empathy and understanding. Furthermore, lowering perceived discrimination may help ensure that individuals with dementia receive compassionate care and feel more included. These findings align with reviews by Nguyen and Li (2020) and Bacsu et al. (2022), showing that reducing negative beliefs lowers discriminatory behaviors toward individuals with dementia and their caregivers.29,44
Lastly, we found that an increase in perceiving oneself as a change agent was linked to more positive emotional reactions. As individuals feel more capable of helping people with dementia, their positive feelings toward them seem to increase. The Dementia Friends intervention encouraged social engagement, likely boosting participants’ sense of involvement and impact. These findings align with previous studies showing that contact with people with dementia enhances a sense of competence and positive emotional reactions.34,45
The current study has several limitations. Our sample comprised adults (mean age = 60.79), limiting generalizability. Future studies should include participants of all ages, including adolescents. Program efficacy was assessed after a single session, without extended follow-up; as such, longer interventions should be used in future studies to address dementia stigma better. Measurement choices likely constrained reliability, validity, and construct coverage: subjective knowledge and perceived change-agency were single items, and each stigma domain comprised two items with weak inter-item correlations. Future evaluations should employ validated multi-item instruments with broader conceptual coverage and, where feasible, longer or repeated exposure. Observed effects were small (η2 ≈ 0.01–0.04), consistent with a brief, low-intensity intervention. Moreover, the study was not designed or powered for inferential subgroup comparisons by religion/ethnicity (see Table 1); future studies should oversample minority communities, ensure language/translation equivalence, and pre-specify subgroup analyses. Data-collection mode differed between timepoints (paper at T1 versus phone at T2), potentially introducing mode effects despite identical item wording and interviewer standardization; future work should harmonize modes or assess mode equivalence. Attrition was substantial (820→205), so selection bias cannot be ruled out even though baseline characteristics and outcomes did not differ significantly between completers and dropouts (Supplemental Table 1 and 2). As data were not missing at random and the sample was small, we chose the EM method for data imputation. Future studies are advised to use larger samples, which would enable multiple imputation (MI) and pre-specified sensitivity analyses. Finally, the single-arm pre–post design limits causal inference. Randomization was infeasible in this nationwide rollout, but policy-compatible alternatives (e.g., cluster stepped-wedge aligned with phased municipal implementation, matched comparison communities) could strengthen internal validity in future evaluations.
Despite these limitations, the current study offers several unique contributions to the existing literature on dementia education and stigma reduction. First, it represents one of the few national-scale evaluations of the Dementia Friends program implemented outside the UK, targeting a broad adult age range in a non-clinical, community setting. Second, unlike many previous studies that assessed outcomes immediately post-intervention,9,10,13–15,19 this study included a three-month follow-up, providing insight into the short-term retention of knowledge and emotional change. Third, the program was evaluated within Israel's complex sociocultural context—characterized by strong familial caregiving norms, ethnic and linguistic diversity, and varied beliefs about dementia.8,46 These adaptations demonstrate how dementia-awareness initiatives can be effectively tailored to pluralistic societies, offering a transferable model for global public health systems.
In light of these contributions, several practical implications emerge. First, further dementia awareness programs should be implemented. These programs, when funded and championed by national community-based authorities, can make a significant difference. Second, these interventions should also be extended in length and contain more knowledge regarding dementia and dementia stigma. Third, addressing discriminatory behavior requires comprehensive strategies that include not only education but also community engagement and policy initiatives. Fourth, ongoing support and follow-up are crucial to ensure the long-term effectiveness of these programs in reducing stigma, expanding knowledge, and promoting a more inclusive environment for individuals with dementia. Accordingly, implementations should combine brief education with structured contact, periodic boosters, community-norm efforts, and service-level supports, alongside culturally tailored delivery and targeted outreach within minority communities, to help translate observed improvements in knowledge and emotions into more inclusive day-to-day behaviors. Where phased adoption is planned, simple, policy-compatible evaluation designs (e.g., stepped-wedge or matched comparisons) can be embedded to strengthen causal interpretation without disrupting service delivery. Finally, beyond brief education, we recommend concrete components: (i) direct or structured contact with people living with dementia and family caregivers (e.g., co-facilitated sessions, service encounters, volunteering); (ii) repeated or booster sessions across weeks to consolidate skills and norms; (iii) community-level initiatives that make inclusive responses visible and normative (e.g., bystander cues, local campaigns); and (iv) organizational/policy supports that enable action (clear procedures, leadership endorsement, environmental accommodations). Together, such multi-component approaches are more likely to produce durable changes in discriminatory behavior.
Conclusion
Participation in Israel's Dementia Friends program was associated with higher dementia knowledge and with reductions in some stigma—particularly negative emotional reactions—over three months. The program's accessible format appears to help convey complex information. However, discriminatory behavior did not change, underscoring the need for more comprehensive, longer-term approaches. Overall, ongoing dementia-awareness efforts remain important to support empathy and a more inclusive society for people living with dementia.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251413784 - Supplemental material for Evaluating the effectiveness of the “Dementia Friends” program in Israel on increasing knowledge and reducing stigma about dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877251413784 for Evaluating the effectiveness of the “Dementia Friends” program in Israel on increasing knowledge and reducing stigma about dementia by Aviya Riabzev, Perla Werner and Shiri Shinan-Altman in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
Ethics approval was received from the Ethics Committee of Bar-Ilan University (approval No. 111703).
Consent to participate
Informed consent was obtained from all participants involved in the study, in accordance with the approved ethical guidelines.
Consent for publication
Not applicable
Author contribution(s)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by JDC Israel Eshel.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the authors upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.